System physiology ch 10
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
Pacemaker cells
Start the heart beat
Contractile cells
Pump the blood
EKG
Records electrical activity
2 types of Cardiac cells
A. pacemaker cells (autorhythmic)- Do not contract, set the rhythm, found in the conduction system (~ 1% of cells): self-excitable (no nervous system needed)
B. Contractile cells- make up most of the heart, responsible for pumping blood
Analogy for 2 types of Cardiac cells
Pacemakers =”set” and Contractile = “squeeze”
Conduction pathway (very high yield)
SA node→ AV node→ AV bundle (Bundle of His)→ Bundle branches → Purkinje fibers
Analogy for Conduction pathway
SA→AV→Bundle→Branch→Purkinje or Start At A Very Big Bridge Path
SA node key function
main pacemaker (~75 bpm)
AV node key function
Delay (0.1 sec) → allows atria to contract first
Bundle/Purkinje key function
spread signal to ventricles; whole process takes ~0.22 sec
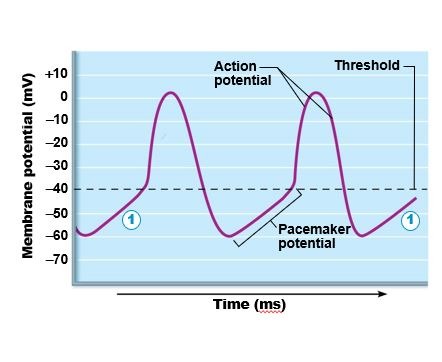
Pacemaker cells: Action Potential (3 steps)
Pacemaker potential- Na+ slowly enters→ K⁺ channels close→gradual rise
Depolarization - Ca2+ enters→spike
Repomarization - k+ leaves → back to negative
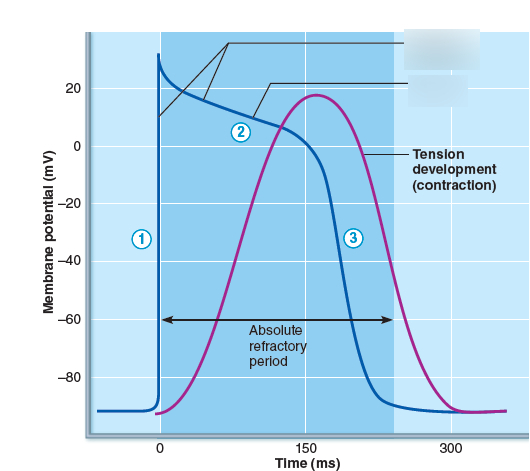
Contractile Cell Action Potential (Different)
Depolarization → Na+ IN (fast)
Plateau→ Ca2+ IN (keeps contraction going)
Repolarization → K+ OUT
Differences between Cardiac and skeletal AP
Cardiac AP lasts ~200 ms
Skeletal AP lasts 1–2 ms
Important because: Prevents tetany → ensures proper pumping
EKG Waves (critical)
P Wave - Atrial depolarization
QRS Complex - Ventricular depolarization (Atrial repolarization hidden)
T Wave - Ventricular repolarization
Important Intervals
P-R interval: atria → ventricles delay
S-T segment: ventricles fully depolarized
Q-T interval: total ventricular activity
Clinical connections (common Exam points)
Abnormalities:
Ectopic focus → abnormal pacemaker
Heart block → AV node fails
Extrasystole → premature beat (caffeine/nicotine)
EKG Clues:
Large R wave → enlarged ventricles
ST elevation/depression → ischemia
Long QT → arrhythmia risk
Pacemaker Problems (Rhythm Origin Issues)
A. Ectopic Focus
Mechanism: Abnormal region starts firing instead of SA node
Effect: Irregular or premature beats
B. Junctional Rhythm (AV node takeover)
Cause: SA node fails
Rate: 40–60 bpm (slower than normal)
EKG:
No P waves (atria not properly activated)
Conduction Problems (Signal Transmission Issues)
Heart Block (AV Node Dysfunction)
Mechanism:
Signal from atria → ventricles is delayed or blocked
Types:
Partial block: some signals pass
Complete block: no signals pass
Effect:
Atria and ventricles beat independently
Ventricles default to slow intrinsic rhythm (~30 bpm)
Treatment:
Artificial pacemaker
Premature Beats (Extrasystole)
Mechanism:
Early depolarization from ectopic focus
Causes:
Caffeine
Nicotine
Effect:
Skipped beat sensation
Next beat feels stronger (“thud”)
Why?
More filling time → stronger contraction
4. Dangerous Rhythm Disorder
Ventricular Fibrillation
Mechanism:
Chaotic, disorganized electrical activity
Effect:
No effective pumping → life-threatening
Causes:
Heart attack
Electrical shock
EKG:
Completely irregular, chaotic waves
EKG Clinical Interpretation
A. Enlarged Ventricles
Finding: Large R waves
Meaning: Hypertrophy
B. Ischemia (low oxygen)
Finding:
ST segment ↑ or ↓
“ST = Stress Trouble”
C. Long QT Interval
Problem: Delayed repolarization
Risk: Dangerous arrhythmias
“Long QT = Quivering Threat”
Homeostatic imbalance
Rhythm Problems:
Ectopic focus → abnormal beats
SA failure → AV takes over (no P waves)
Conduction Problems:
Heart block → atria & ventricles disconnected
Severe → needs pacemaker
EKG Red Flags:
Big R → enlarged heart
ST changes → ischemia
Long QT → arrhythmia risk
Emergency:
Ventricular fibrillation → no effective pumping