Operative One -- Pulp Protection and Therapy: Feitosa
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
Why dental pulp must be protected?
Why selective caries removal?
Preserve pulp vitality (patients seek care)
Avoid thermal sensitivity (pain) to the patient after restorative procedures
Avoid removal of sound/affected structure
Keep pulp mechanisms of reaction
Endo-treated teeth are more prone to fractures
Dentin-pulp complex
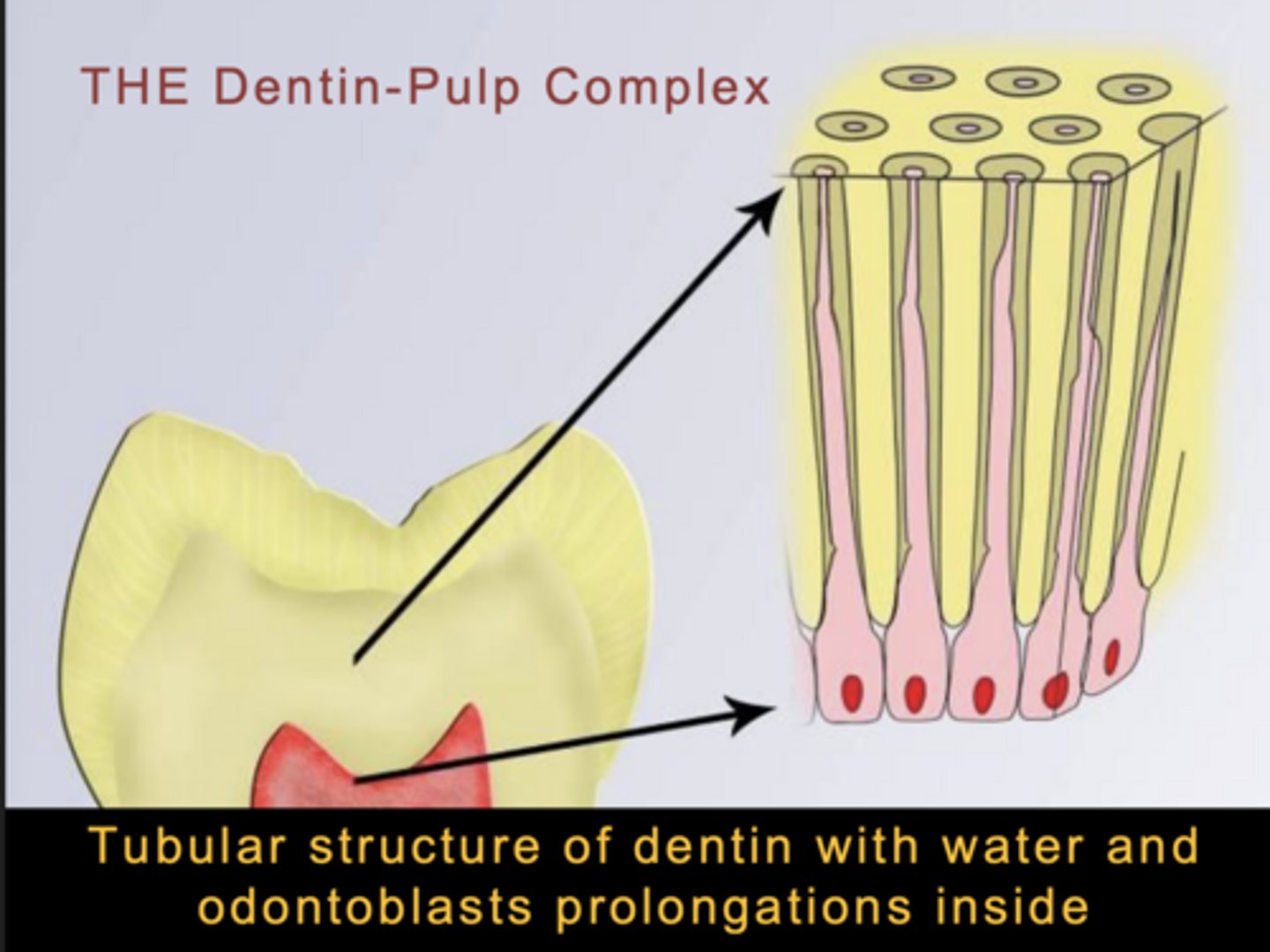
If you have any issue in the dentin the fluid inside the tubules will be felt by the odontoblast and can
present as sensitivity to the patient
- 1st pulp reaction = Pain
2nd reaction is called
Sclerotic Dentin
- If there is an enemy the odontoblasts can block the tubule and make it harder for the enemy (bacteria etc) can come
Is sclerotic dentin hard or softer than other dentin
harder
if you are restoring and the bottom is full of sclerotic dentin do you need to put a liner
No
3rd reaction
Rapid formation of tertiary dentin
- a reactionary formation of dentin
Causes of dental pulpal inflammation
Active caries
Cavity preparations (mild/severe)
Dental materials (mild/transient)
Occlusal trauma
Pulpal pain
- intra-pulpal pressure on nerve endings secondary to an inflammation response
- Absence of inflammation - hydrodynamic inflammation
When does pulp need protection
After selective caries removal that have lead to deep cavity preparation
Full crown cavity preparations
Presence of mechanical pulp exposure
-- limited space for swelling
-- increase of pressure and cell death with severe inflammation
-- limited regeneration
Cervical dentin exposure due to erosion causing pain
How to protect the dental pulp
By proposing a preventive program to "eliminate" development and/or progression of carious lesions
By collecting appropriate information regarding pulp health prior to restorative procedures
By selecting/using appropriate cutting instruments, use water during preparation, no water during caries removal
By selecting/applying appropriate biological and mechanically resistant dental protective materials
Diagnosis of Pulpal Health:
Clinical Examination
- Anamnesis (spontaneuous pain?)
- Clinical inspection
- Palpation
- Percussion

Diagnosis of Pulpal Health:
Objective Tests
- Cold test
- Electric Pulp Test (EPT)
--- In case of lingering pain = endo
Decisions towards restoration
Diagnosis of vital pulp
Pulpitis is Reversible
No clinical or radiographic pulp exposure
Periapical radiolucency (lesion) in x-ray
(Need all four to = operative)

If a patient has spontaneous pain (Anamnesis)
Send them to endo don't even think twice bout that shit.
That shit is irreversible and send em packing to endo
Cavity Sealers
provide a protective coating to the walls of a prepared cavity and a barrier to leakage at the interface. All walls in their entirety are coated (Usual with Amalgam)
Cavity Liners
Cement coating of minimal thickness (less than 0.5mm) to provide a therapeutic effect (remineralization) or a physical barrier to bacteria (coat walls near the pulp only)
NOT TO BE PLACED ON ENAMEL/DEJ
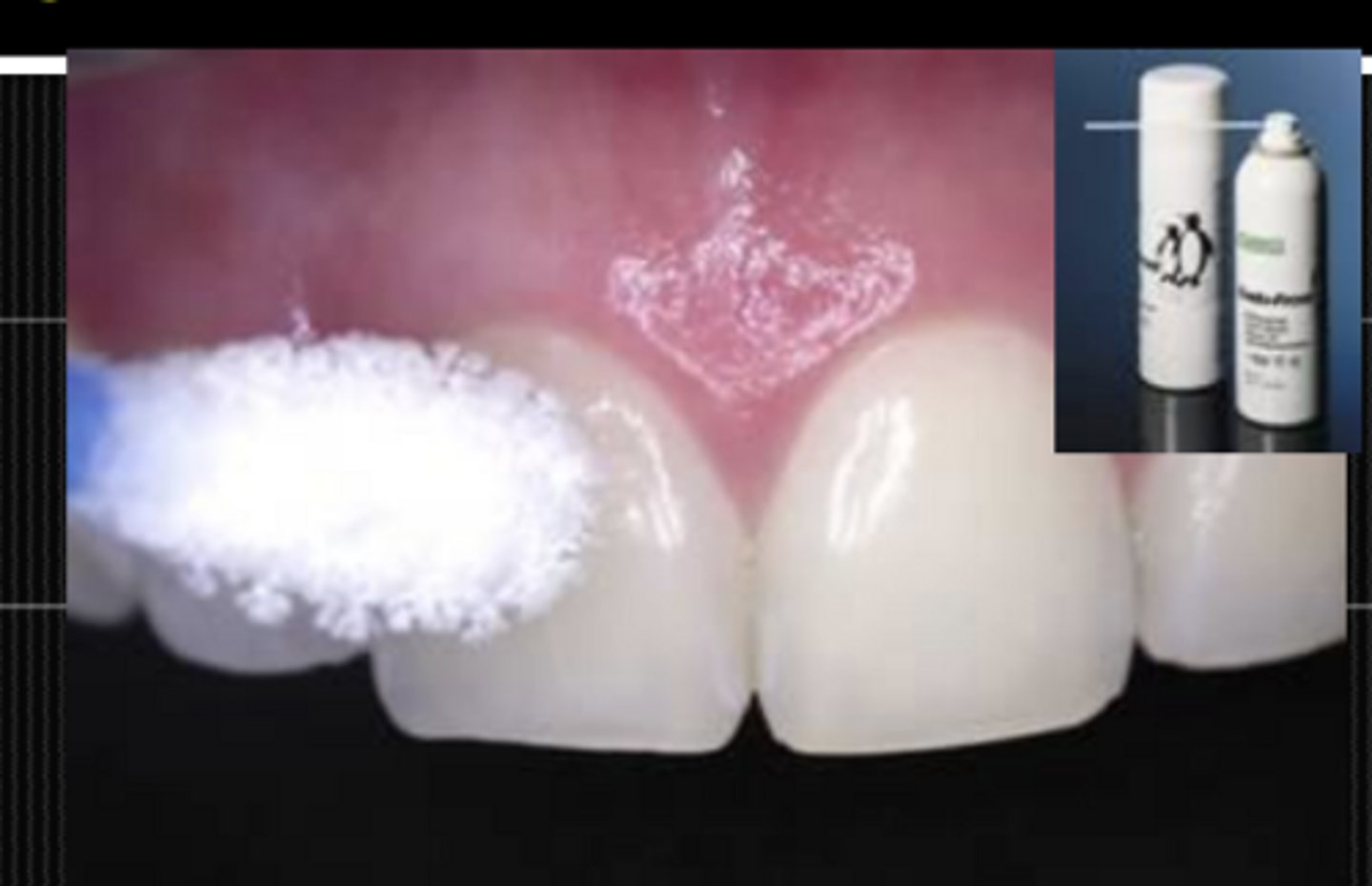
SuperSeal (Cavity Varnish)
Acidic nature- demineralizes the smear layer and the peritubular dentin
Reacts with the calcium hydroxyapatite to form a fine granular calcium oxalate precipitate
This precipitate occludes the dentinal tubules
Cavity liner RMGI
Cement or resin coating of minimal thickness- physical barrier to bacteria and their products
1-2 mm thickness for base
Cavity liner Resin Modified Calcium Silicates
Provided therapeutic benefit
- Fluoride release, dentinal seal, and antibacterial action promoting pulpal health

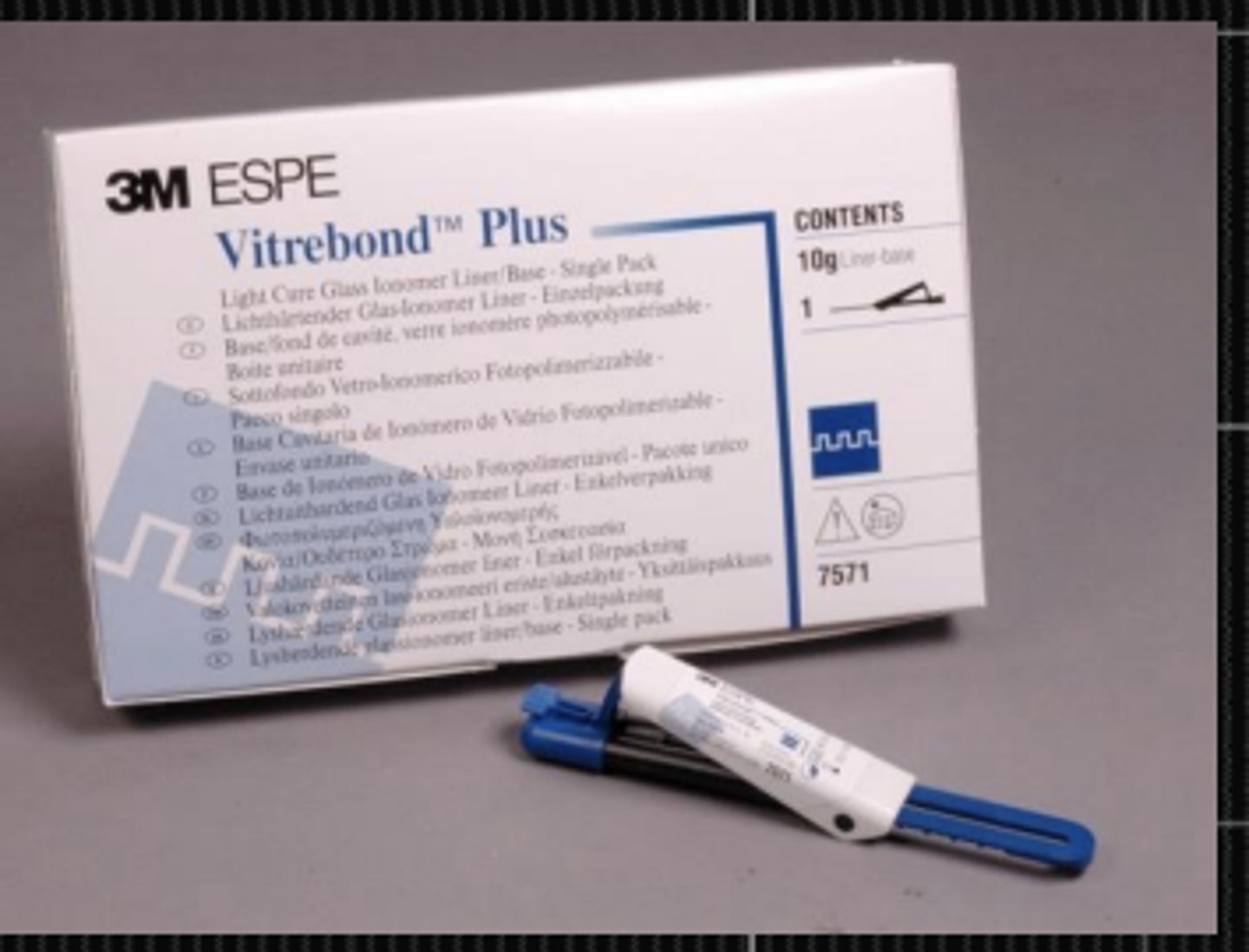
Vitrebond liner
Apply after partial caries removal
- is a RMGI
- Chemical bond to tooth structure
- Fluoride release
- Good mechanical properties
- Favorable pulpal response due to F release, initial low pH, physical barrier to bacteria penetration
Superficial cavity what kind of pulp protection
none silly
Moderate cavity what kind of pulp protection
Use Vitrebond some of the time
- depends on age of patient/ how clsoe to the pulp
Deep cavity what kind of pulp protection
Closed exposure
Use vitrebond always
Pulp exposure what kind of pulp protection
No vitrebond
can't put vitrabond on the pulp instead use Resin Modified Calcium Silicates
if you have sclerotic dentin
you do not need liner
Indirect pulp capping
When you put vitrebond layer down without exposure
Step-wise technique
young patient with risk for pulp exposure even with selective caries removal
Deep lesions
Two appointments to wait for tertiary dentin formation
Direct pulp capping
- Direct pulp exposure
- Theracal onto pulp tissue
- vitrebond liner
- final restoration
Observe
- Extension of exposure
- Time until pulp capping done
- Bleeding control
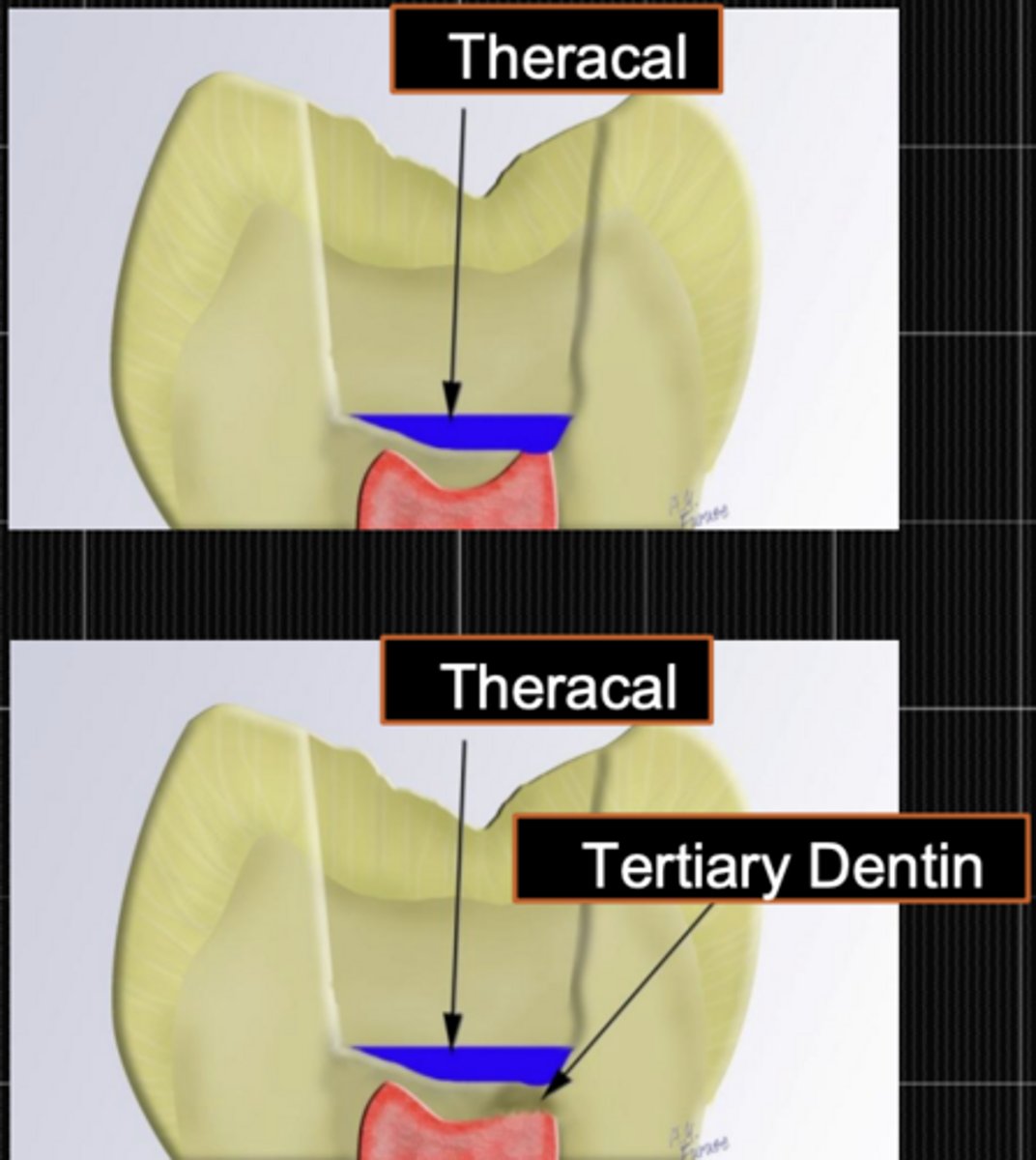
TheraCal LC
Resin-modified Calcium Silicate Pulp Protectant/liner
- Placement of a Ca[OH]2 liner in the deepest part of the preparation covering the pulp exposure
- Place liner on dentin only (pulpal and axial walls, away from all margins and enamel)
- Establish a tight seal to prevent bacterial invasion
- Stimulates apatite formation and the formation of tertiary dentin
- Maintain an antibacterial alkaline-related biological environment. It is an alkaline calcium silicate based on the chemistry of MTA
- After placement and curing follow with layer of Vitrebond and/or normal bonding procedures
Incomplete caries removal
only for very deep cavities
- Step Wise Technique may result in pulp exposure in 2nd visit
- Direct pulp capping has lower success rate tha SWT