Functional Anatomy: Hip
1/101
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
102 Terms
Osteology for hips
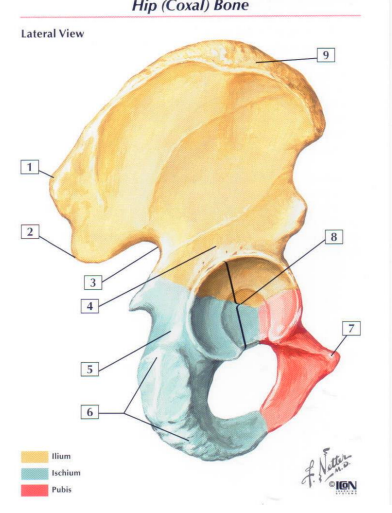
Innominate Ossification
full ossification occurs between 20-25 years of age
until ossification occurs, connected via cartilaginous union
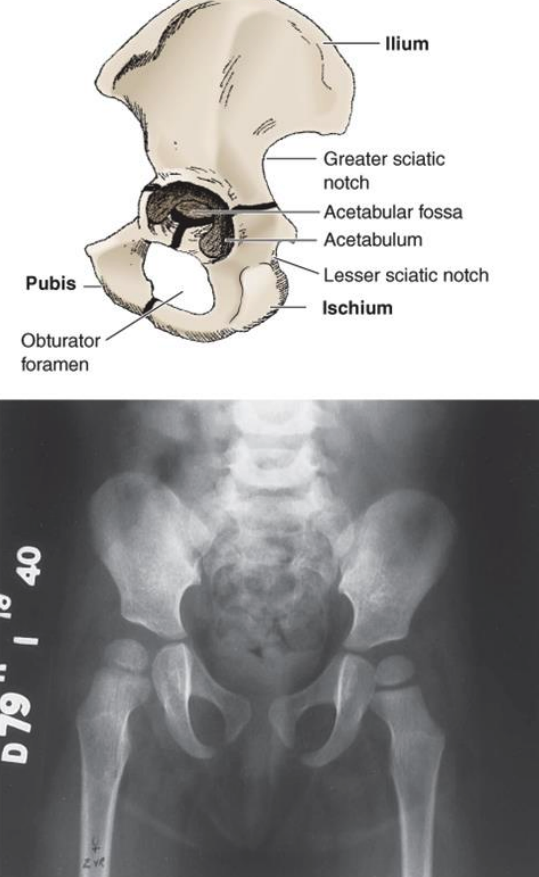
Pelvis → lateral view → acetabulum
acetabulum fossa
faces: lateral, anterior, and inferior
does not articulate with femoral head
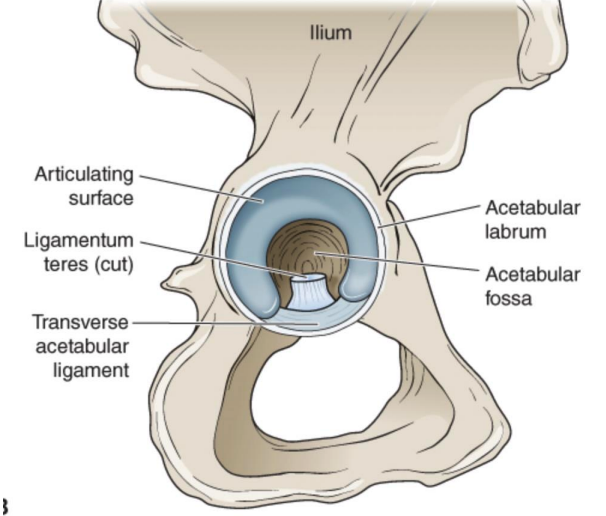
acetabulum articulating surface
horseshoe shape located anteriorly, superiorly, and posteriorly
articulates with femoral head
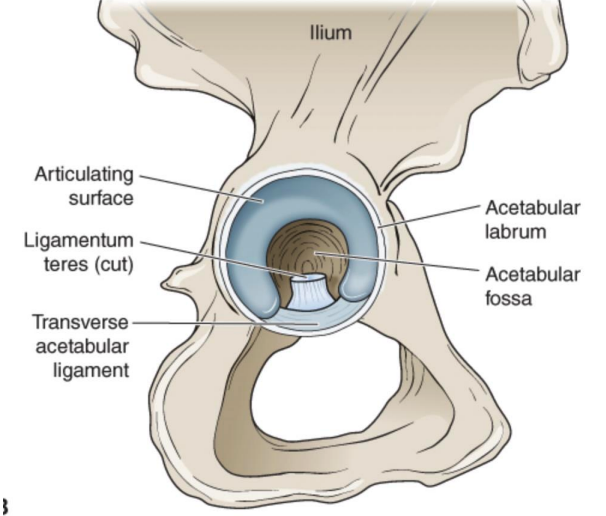
acetabular notch
located anterior-inferiorly
ligamentum teres origin
bridged by transverse acetabular ligament
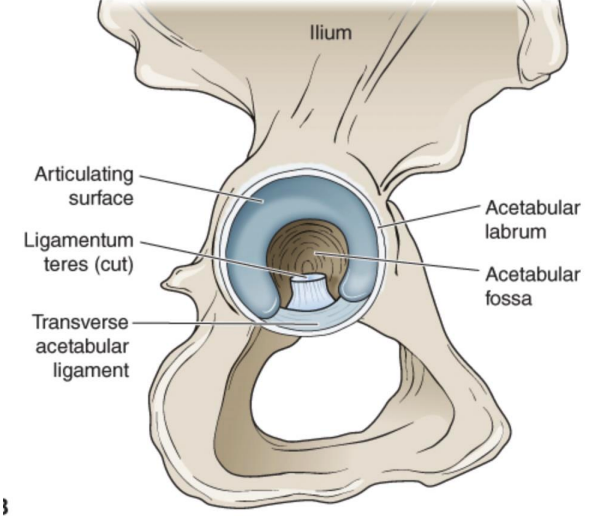
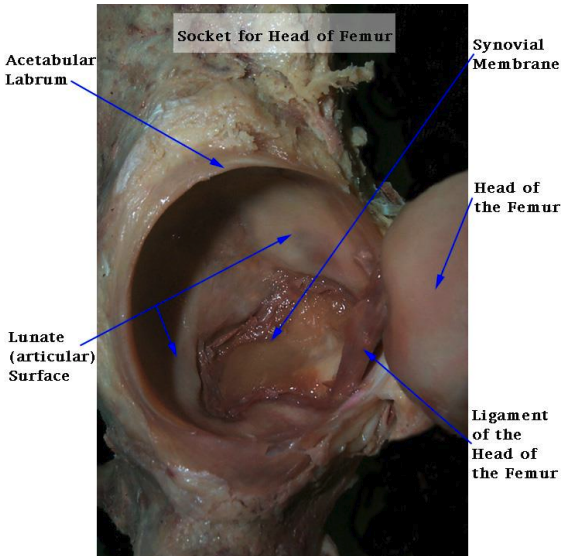
contents of acetabulum
lunate surface: hyaline cartilage, thick superior and anterior (based on WB)
fat pad
ligamentum teres
transverse acetabular ligament: spans acetabular notch and part of labrum, connects lunate surfaces
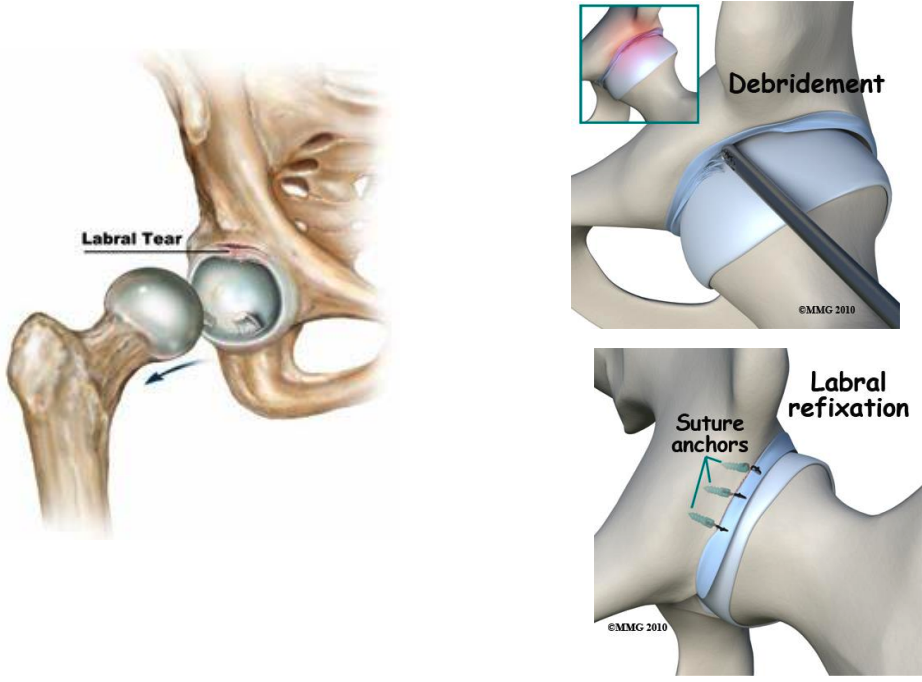
acetabular labrum
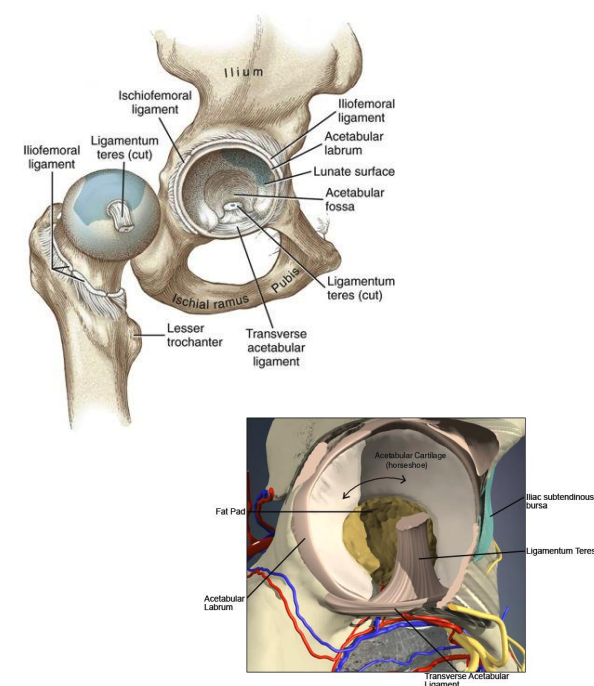
acetabular labrum
fibrocartilage
deepends socket and increase concavity
negative articular pressure
increases stability
nerve endings: proprioception (joint stability and balance) and pain
clinical relevance: labral tear
when labrum is compromised → friction stresses increases → articular cartilage deterioration → hip osteoarthritis
arthrology
diarthrodial ball and socket joint
primary function: support the weight of the head, arms, trunk in static erect posture and dynamic postures
primary functions are in weight bearing (compared to shoulder)
angle of the hip
acetabular angles: center edge angle and acetabular version
femoral angles: angle of inclination and femoral neck torsion
center edge angle
formed by a vertical line through the center of the femoral head and a line connecting the center of the femoral head and the bony edge of the acetabulum
definite dysplasia <16 degrees
possible (borderline) dysplasia 16-25 degrees
normal >25 degrees
excessive > 40 degrees
femoral neck coverage
acetabular dysplasia: shallow acetabulum that results in a lack of femoral head coverage = instability (less angle = less stability)
coxa profunda: acetabulum excessively covers the femoral head (excessive angle = impingment)
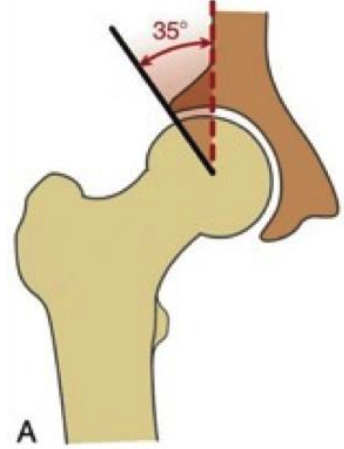
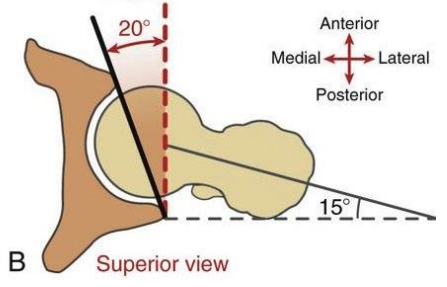
angle of acetabular version
known as the acetabular anteversion/retroversion angle
amount of anterior or posterior orientation in the transverse plane
Normal ~20 degrees anteversion
>20 degrees is anterversion, <20 is retroversion
femoral neck coverage acetabular anteversion
acetabulum is positioned excessively anteriorly in the transverse plane → can lead to instability
femoral neck coverage acetabular retroversion
acetabulum is positioned posteriorly in the transverse plane → can lead to over coverage of the femoral head/neck (impingement)
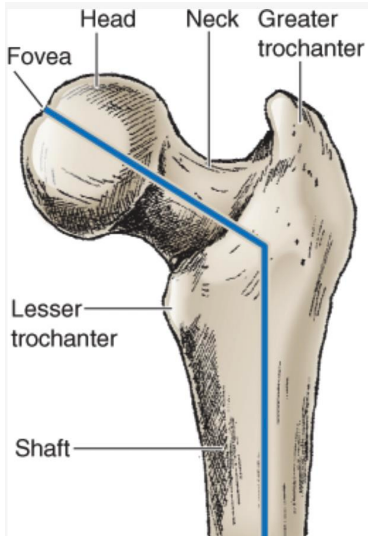
femur
head, neck, trochanters (greater/lesser), lateral epicondyle and medial epicondyle
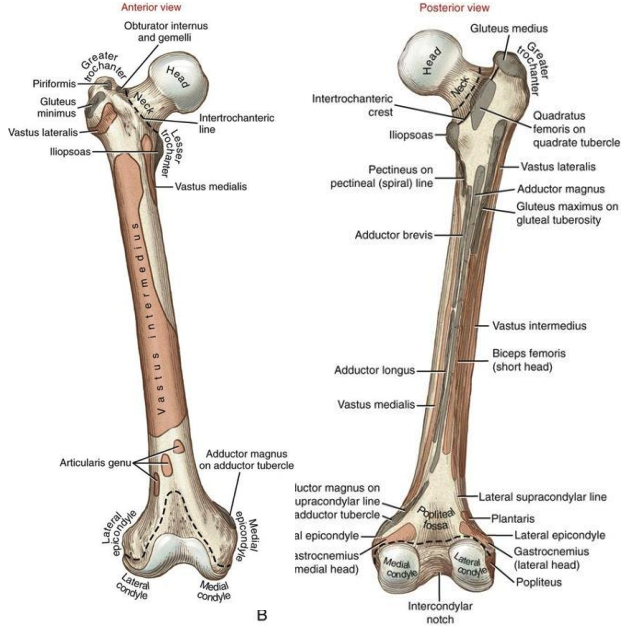
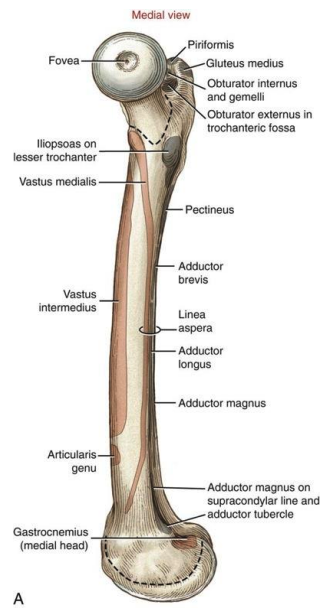
femur from medial view
fovea (ligementum teres attachment; not covered in hyaline cartilage) and anterior aspect of head exposed
femoral neck
angulated so that the femoral head faces medially, superiorly, and anteriorly with respect to the femoral shaft and condyles
angles of the femur
torsion of the femur:
twist between shaft and neck in the transverse plane
neck projects anterior to a M/L axis through the femoral condyles
birth 30=40 degrees
by skeletal maturity, normal angle: 15-18 degrees
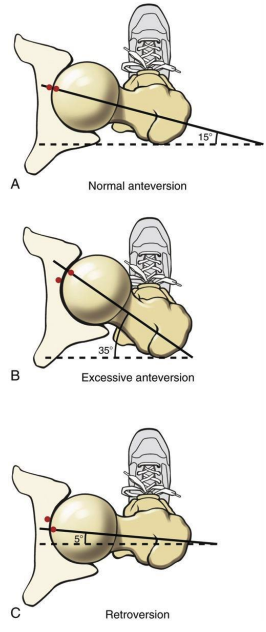
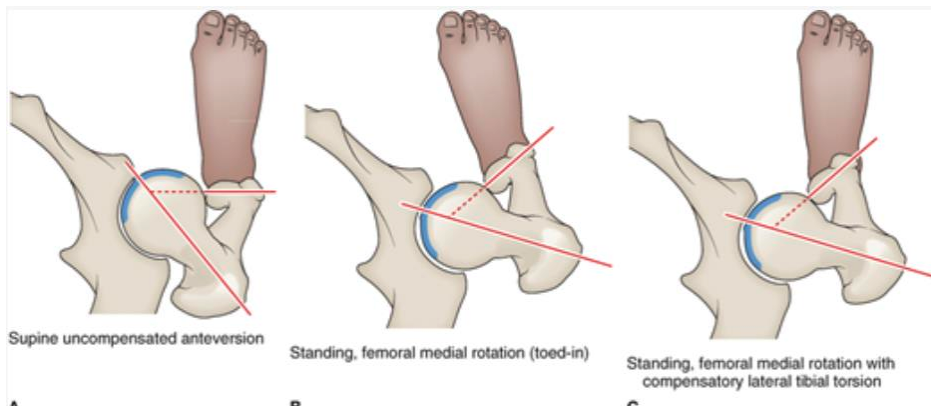
Femoral anterversion
-angle of torsion >15-20 degrees
-reduces hip joint stability
-more exposed anteriorly
-may lead to subsequent labral pathology
-to improve congruency → medial rotation of the femur
-alter knee biomechanics
-may lead to lateral tibial torsion
-hip ROM: increased medial rotation, decreased lateral rotation
-hip ER will be limited with hard end feel (DO NOT TRY AND STRETCH)
Femoral retroversion
-increases hip stability but can lead to impingement
-impingement can lead to subsequent labral pathology
-to improve congruency → lateral rotation of the femur
-alter knee biomechanics
-hip ROM: excessive hip ER and limited IR
-hip IR will be limited with hard end feel (DO NOT TRY AND STRETCH)
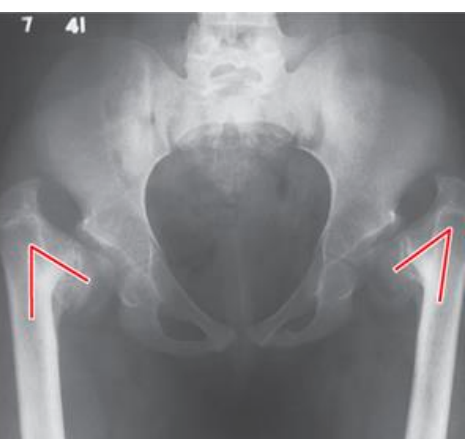
clinical implications of abnormal torsions

varus
an angulation of a distal segment towards the midline of the body relative to the normal ranges
valgus
an angulation of a distal segment away from the midline of the body relative to the normal ranges
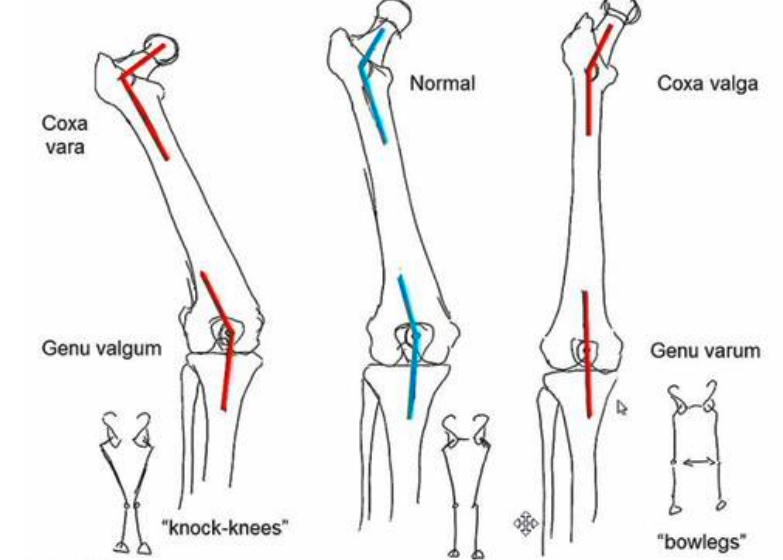
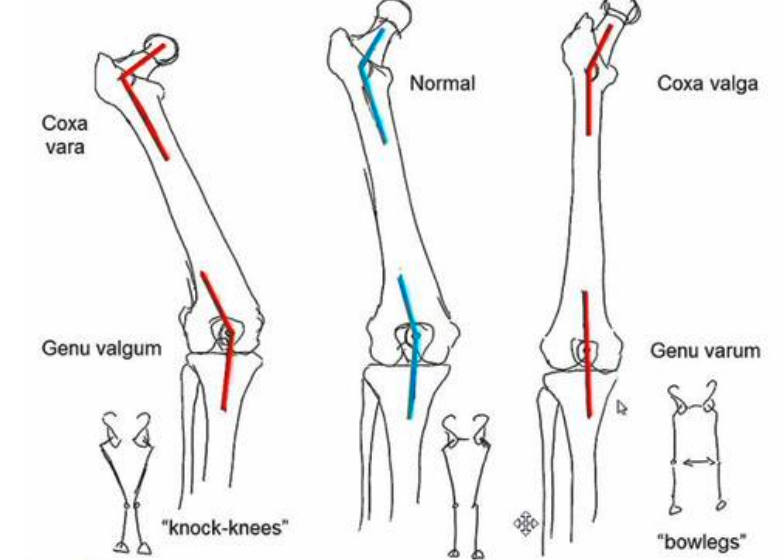
angle of inclination
-angle between the femoral neck and femoral shaft in the frontal plane
-adult normal ~125 degrees
-decreased angle = coxa vara <125
-increased angle = coxa valga >125 degrees

development and the angle of inclination
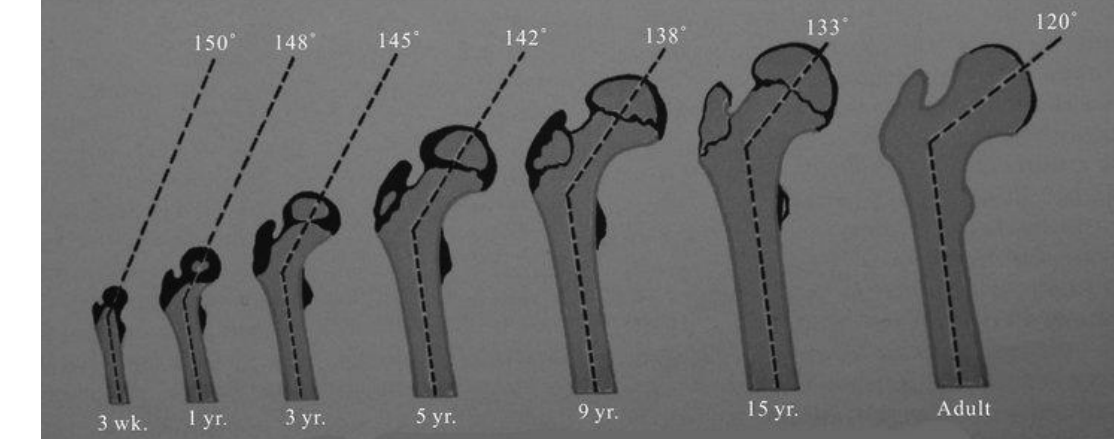
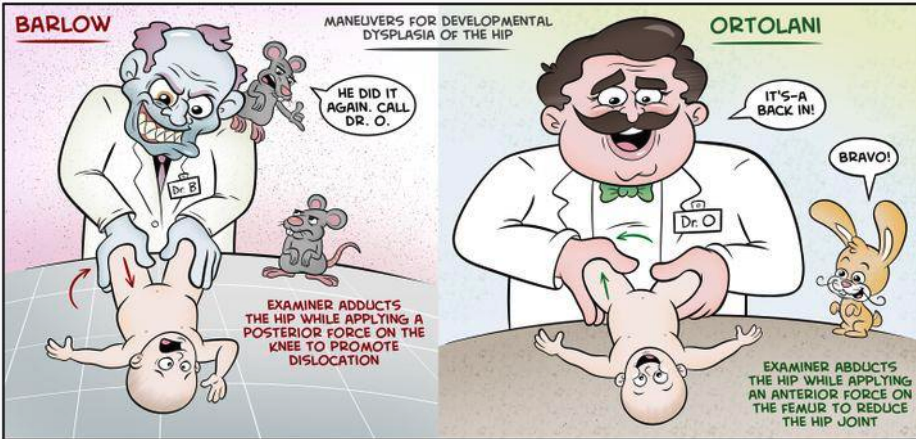
Clinical implications of coxa valga
-angle of inclination is > normal
-decreases abduction moment arm leading functionally weakened hip and increased joint reaction force
-decreased stability due to lessened coverage of the femoral articular surface with the acetabulum
-prediposes to hip dislocation

Barlow and Ortolani tests
LE chain effects of coxa valga
-less stability
-shallow acetabulum
-abducted hip
-genu varum at the knee
-supination of the foot
-longer limb
-normal at birth
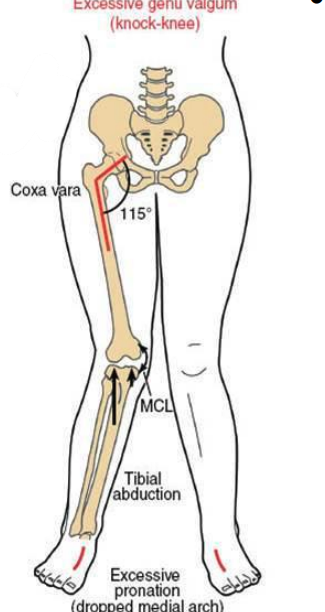
clinical implications of coxa vara
-increased hip joint stability
-increases moment arm of abductors (functionally stronger hip) reduces joint reaction force
-increase bending moment across femoral neck predisposition for (slipped capital femoral epiphysis or femoral neck fracture)
slipped capital femoral epiphysis
-typical demographics
male > female
obesity
african americans
northeast US
-associated with: hormonal abnormalities, specifically thyoid
LE Chain effect of Coxa Vara
increased shear force across the femoral neck, adducted hip, valgus knee, pronation at foot, shorter limb
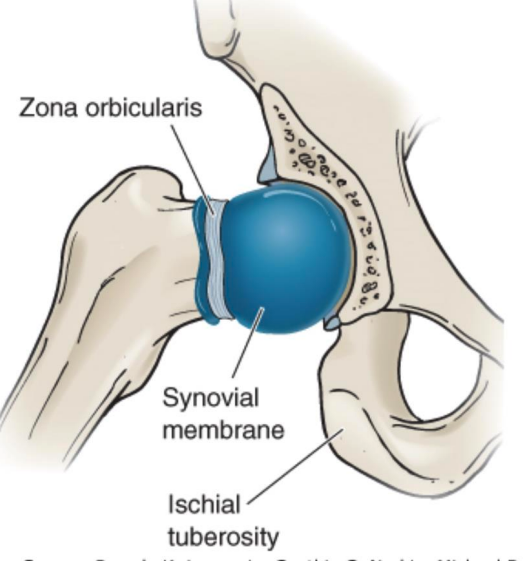
Hip capsule
thick and strong and reinforced by strong ligaments
dense, inelastic and fibrous and encloses the entire joint
attaches to the periphery of the acetabulum blending with the labrum medially with multiple lateral attachments
thickest anterior & superior
thinnest posterior & inferior
-lined with synovial membrane
hip proximal capsule
attaches to periosteum proximal to acetabular rim and acetabular labrum
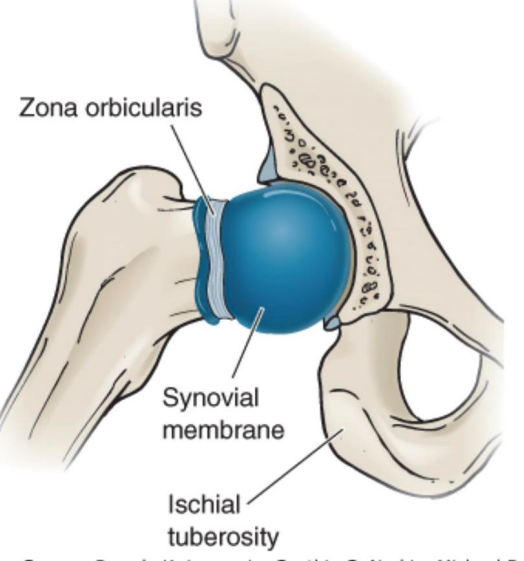
hip distal capsule
surrounds femoral neck (intra-capsular) but not the trochanters (extra-capsular)
-oblique fibers form collar-like structure around femoral neck known as zone orbicularis preventing distraction of the femoral head
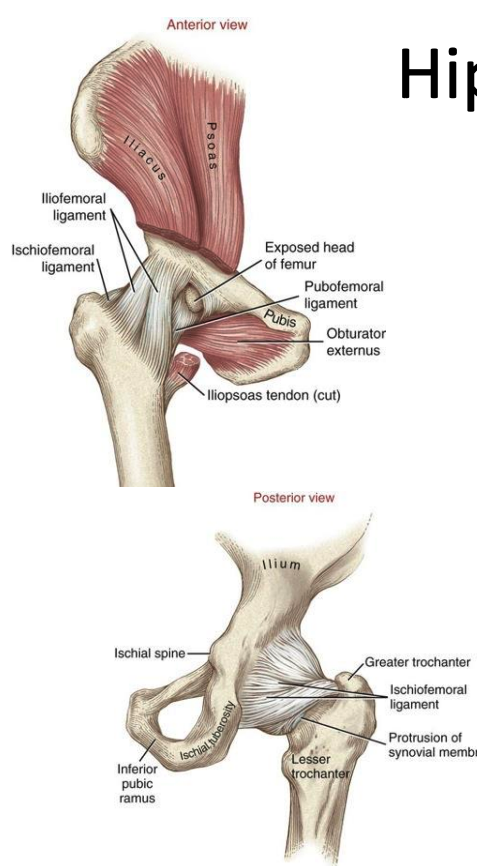
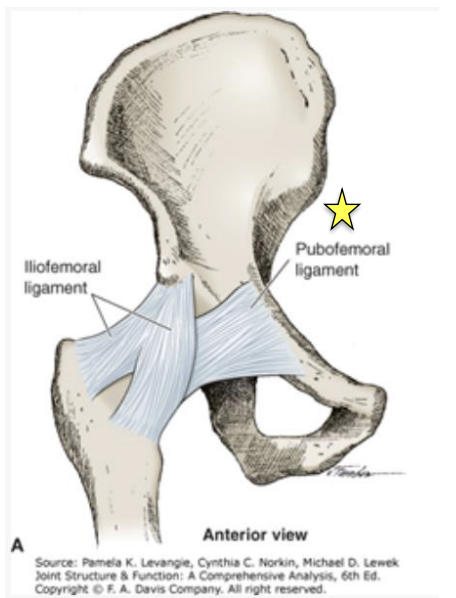
ligaments of the hip 2
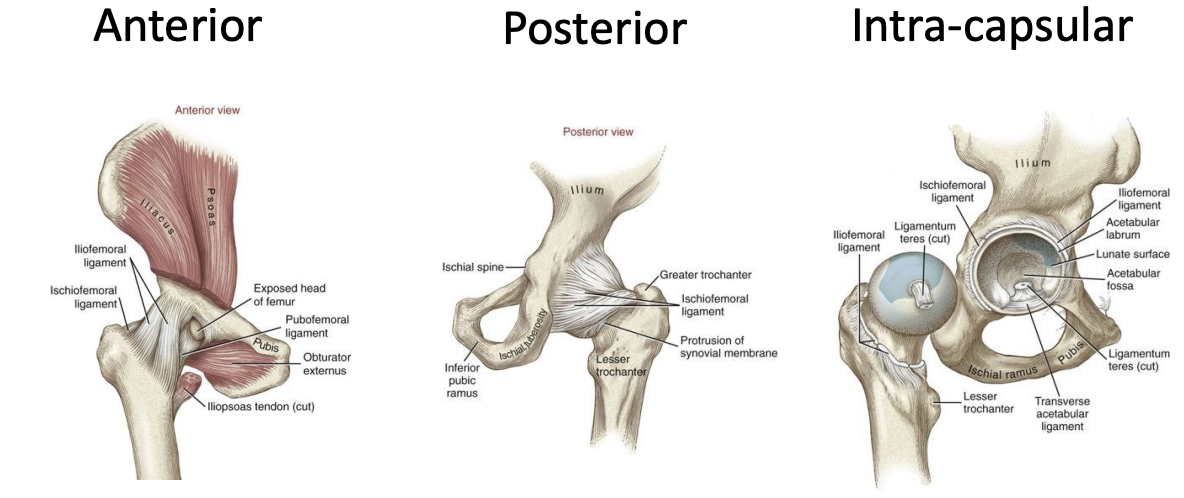
Hip joint capsule reinforcing ligaments:
anterior: iliofemoral ligament and pubofemoral ligament
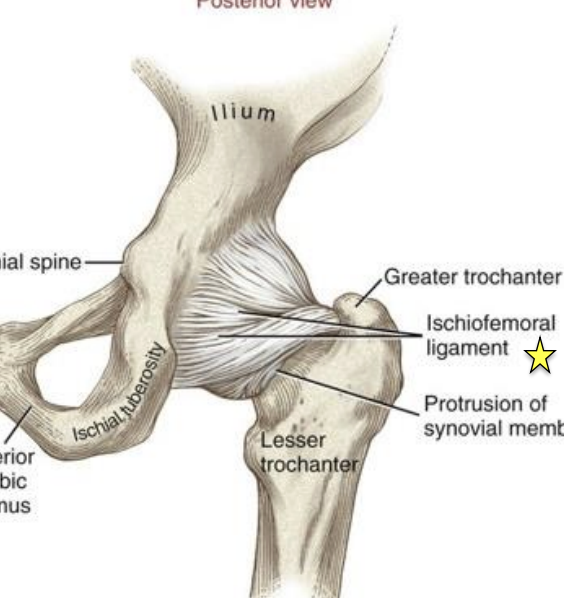
posterior: ischiofemoral ligament
ligamentum teres
iliofemoral ligament (Y ligament of bigelow)
O&I: AIIS to intertrochanteric line
superior band fibers are the strongest in the hip
limits hip extension, ER
superior fibers may be taut in adduction and inferior fibers taut in abduction
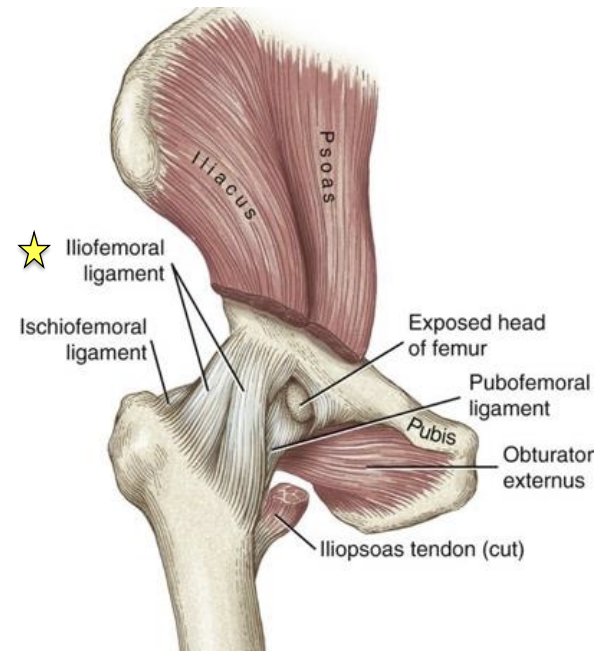
pubofemoral
O&I: anterior and inferior rim of the acetabulum and adjacent parts of the superior pubic ramus then cross joint to blend with medial band of iliofemoral ligament
-limits hip abduction, extension, ER
Ischiofemoral ligament
O&I: posterior acetabular rim to inner surface of the greater trochanter
-limits hip extension and IR
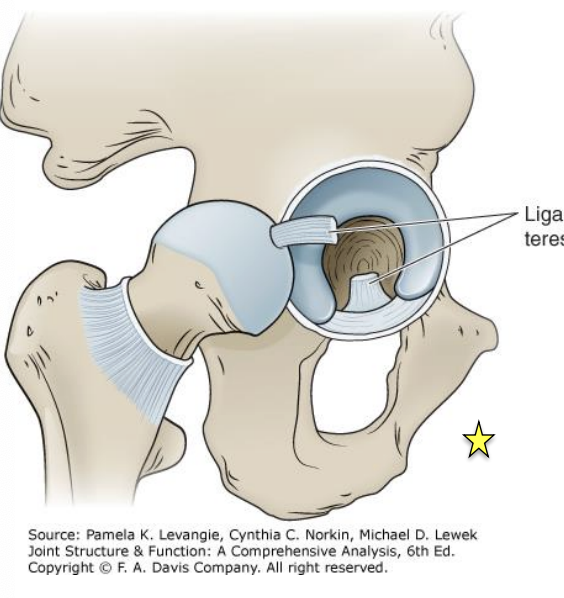
ligamentum teres
O&I: from acetabular notch to the fovea
intra-articular but extrasynovial
conduit for secondary blood supply to the femoral head
recent studies show it provides some stability
-limits hip IR and ER (when hip is >90 deg flexion)
ligaments of the hip
anterior, posterior, intra-capsular
general concept: ligaments LAX in flexion and TAUT in extension → capsular and ligamentous twist
femoral neck blood supply
femoral head is most commonly supplied by the medial femoral circumflex artery
minimal to no secondary arterial supply to femoral head
increases femoral head risk of avascular necrosis
legg-calve-perthes disease
Legg-Calve-Perthes Disease
collapse of the femoral head due to loss of blood supply during childhood
Hip flexion ROM
~125 degrees
hip extension ROM
~10-30 deg
hip abduction ROM
~45 deg
hip adduction ROM
~20-30 deg
Hip IR ROM
~45 deg
Hip ER ROM
~45 deg
Closed Pack Position of the Hip
full extension of the hip with internal rotation and abduction
twist fibers within the capsular ligaments to most taut positon
not associated with the position of maximum joint congruency
most congruently in 90 degrees of flexion, abduction, and external rotation
Hip joint most congruent
90 degrees of flexion, abduction, and external rotation
Open pack position of the hip
30 degrees flexion, 30 degree abduction, and slight ER
open chain arthrokinematics
femur moving on the pelvis
convex on concave rule
roll and glide opposite
open chain hip arthrokinematics flexion
femoral head “SPINS”
-clinically: rolls anterior, glides post and rolls superior, glides inferior open chain hip arthrokinematics (sagittal plane)
open chain hip arthrokinematics extension
femoral head “SPINS”
-clinically: rolls posterior, glides anterior (sagittal plane)
open chain hip arthrokinematics abduction
rolls superior-lateral and glides inferior-medial (frontal plane)
open chain hip arthrokinematics external rotation
rolls posterior and glides anterior (horizontal plane)
open chain hip arthrokinematics internal rotation
rolls anterior and glides posterior (horizontal plane)
Closed chain Arthrokinematics
pelvis (acetabulum) moving on the fixed femur
Closed Chain sagittal plane motion
anterior tilt/rotation of the pelvic on the femur (hip joint goes into flexion)
posterior tilt/rotation of the pelvic on the femur (hip joint goes into extension)
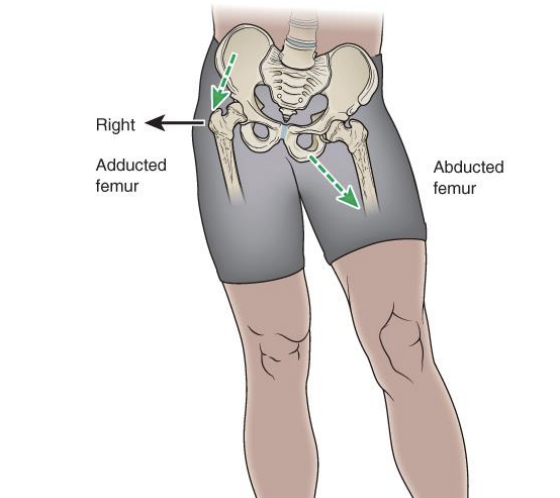
Closed chain frontal plane: unilateral stance
lateral pelvic tilt (named by what is happening on non weight-bearing side)
weight bearing hip is pivot point for axis of motion
pelvic hike, pelvic drop
pelvic hike
weight bearing hip abducts
pelvic drop
weight bearing hip adducts
closed chain lateral shift: bilateral stance
pelvic cannot “hike”
both hips will move in frontal plane
if pelvis shifts to the right, right hip joint will be adducted and left hip will be abducted
closed chain transverse plane motion: unilateral stance
forward pelvic rotation:
reference side is side opposite to the rotating hip joint
right forward rotation: left stance leg, right pelvis translates anteriorly
weight bearing hip goes into internal rotation
backward pelvic rotation:
reference side is side opposite to the rotating hip joint
right backward rotation: left stance leg, right pelvis translates posteriorly
weight being hip goes into external rotation
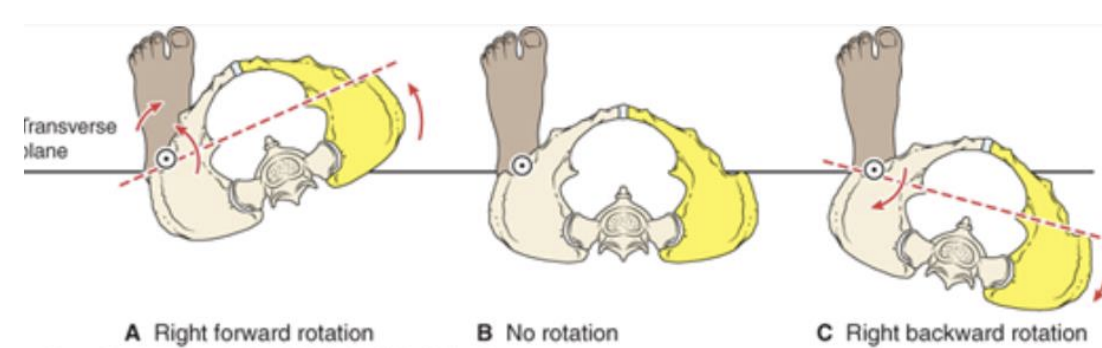
closed chain transverse plane motion: bilateral stance
forward rotation and backward rotation must reference a side
axis of motion occurs around a vertical axis through center of pelvis
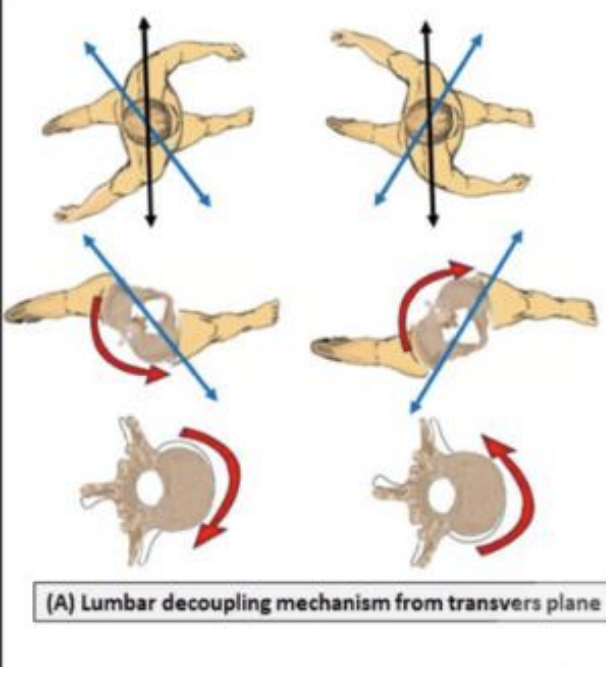
associated lumbar motions
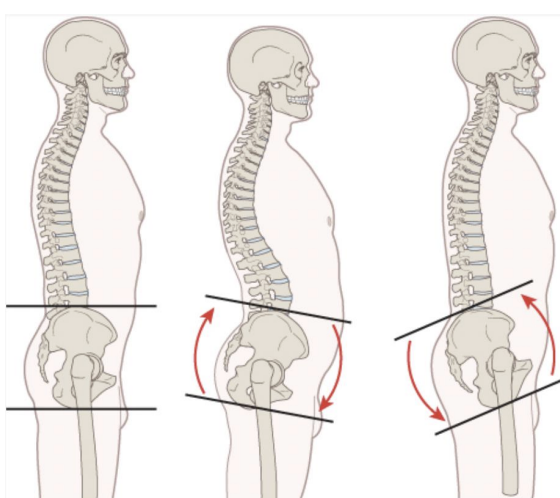
anterior pelvic tilt: hip flexion, lumbar extension
posterior pelvic tilt: hip extension, lumbar flexion
Coupled motion pattersn of the lumbar spine and pelvis
Hip flexion: pelvis on femur (anterior pelvic tilt)
-hip joint flexion
-increases lumbar lordosis
-produced by force-couple between the hip flexors and the erector spinae
hip extension: pelvis on femur (posterior pelvic tilt)
-hip joint extension
-decreases lumbar lordosis
-produced by force-couple between the hip extensors and the rectus abdominis
pelvic rotation during gait
the associated motion in the lumbar spine is in the opposite direction in the transverse plane
Lumbo-pelvic rhythm
ipsidrectional flexion
-lumbar flexion, anterior pelvic rotation, and hip flexion
-bending forward
-helps maximize motion
contradirectional
-lumbar spine extension
-anterior pelvic rotation
-hip flexion
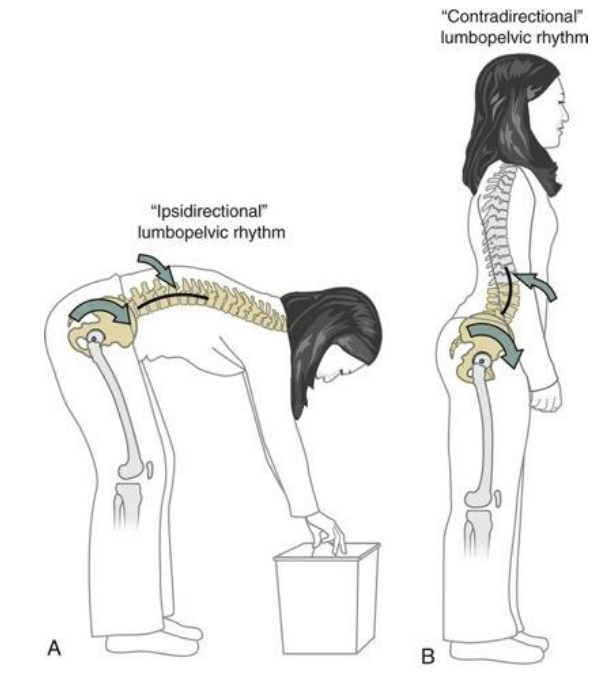
lumbopelvic rhythm: ipsidirectional
sum of motion of lumbar spine, pelvic, and hip
goal is to maximize motion
controlled by: hip extensors & erector spinae muscles eccentrically
contribution of each segment is dependent on (muscles length, joint mobility, neuromuscular control, and psychosocial factors)
increased shear force across lumbar spine and increase disc pressure compared to contradirectional, decreased hip and knee flexion mobility required
lumbopelvic rhythm from a standing position (forward bending)
knees extended, forward bending is produced by forward bending of the lumbar spine ~40 degrees
during initial lumbar flexion the sacrum extends, then begins to flex and the pelvic anterior tilts
once all pelvic anterior tilt is taken up the hips flex
hips flexion = ~70 degrees
lumbopelvic rhythm: contradirectional
flexion is the sum of the motion of the pelvic and hips
goal: increase stability for lumbar spine and improved lifting mechanics
the lift: lumbar spine goes into extension maintaining the lumbar lordosis and pelvis (ilium and sacrum) anterior tilt and hips flex
decreased shear force across lumbar spine, decreased disc pressure, increased tension on hamstrings and increased knee flexion and hip flexion mobility required
anterior muscle innervation
femoral nerve
medial muscle innervation
obturator nerve
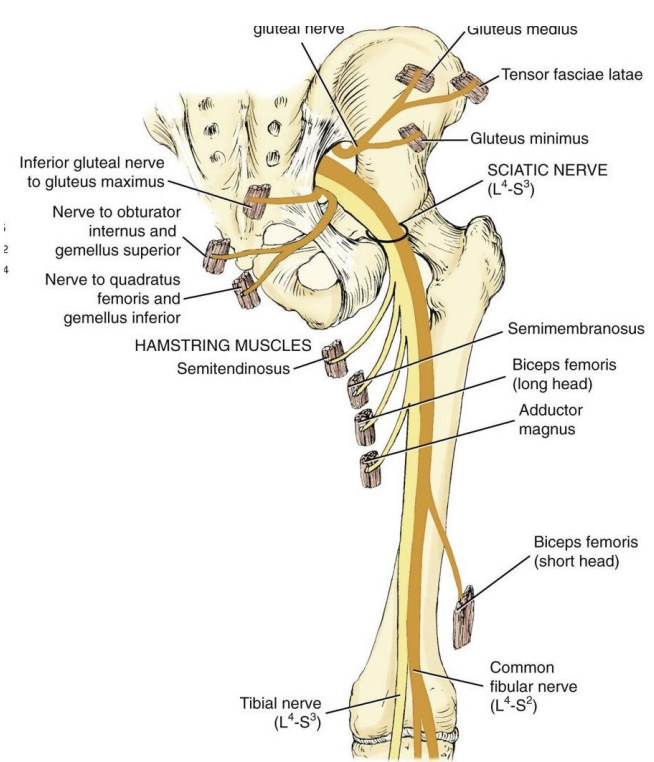
lateral muscle innervation
gluteal nerve (superior and inferior) p
posterior muscle innervation
sciatic nerve
-lateral: peroneal portion
-medial: tibial portion
Hip external rotators muscle innervation
ventral Rami S1 and S2 innervate the piriformis
nerve to the obturator internus and superior gemellus
nerve to the quadratus femoris and inferior gemellus
quadriceps muscle groups
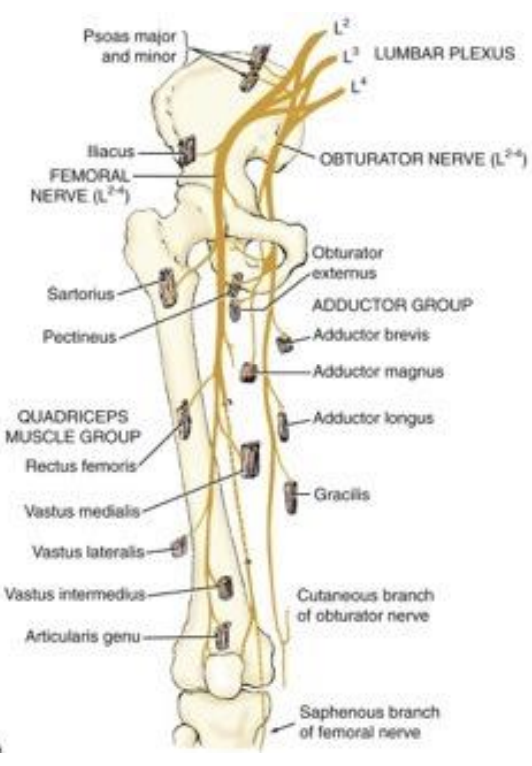
hamstrings muscle
Anterior peripheral nerve sensory distribution
lateral femoral cutaneous nerve, femoral nerve, obturator nerve, saphenous nerve, common fibular nerve, sural nerve, superficial fibular nerve, deep fibular nerve
posterior peripheral nerve sensory distribution
posterior femoral cutaneous nerve, sural nerve, tibial nerve
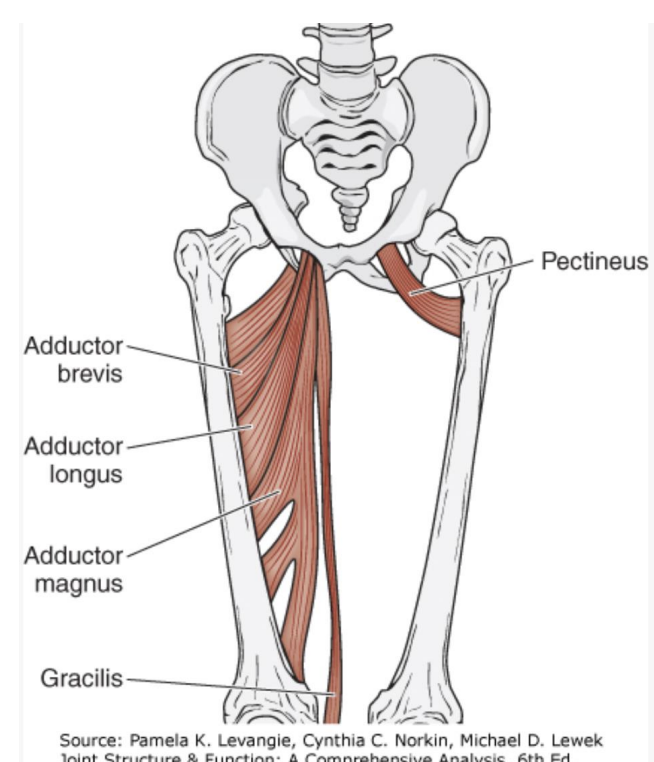
primary Hip flexors
iliopsoas, sartorius, tensor fasciae latae, rectus femoris, adductor longus, pectineusse
secondary hip flexors
adductor brevis, gracilis, anterior fibers gluteus minimus
hip flexors
impact of tight iliopsoas and rectus femoris on hip and lumbar spine
primary hip extensors
gluteus maximus, hamstrings, adductor magnus
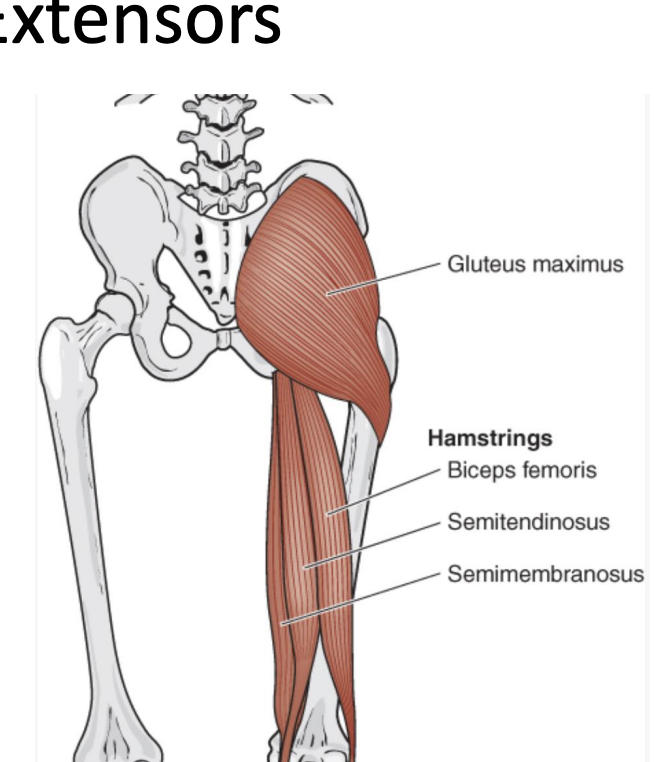
hamstring stretch
impact of tight hamstrings on the hip and lumbar spine
primary hip adductors
pectineus, adductor longus, gracilis, adductor brevis, adductor magnus
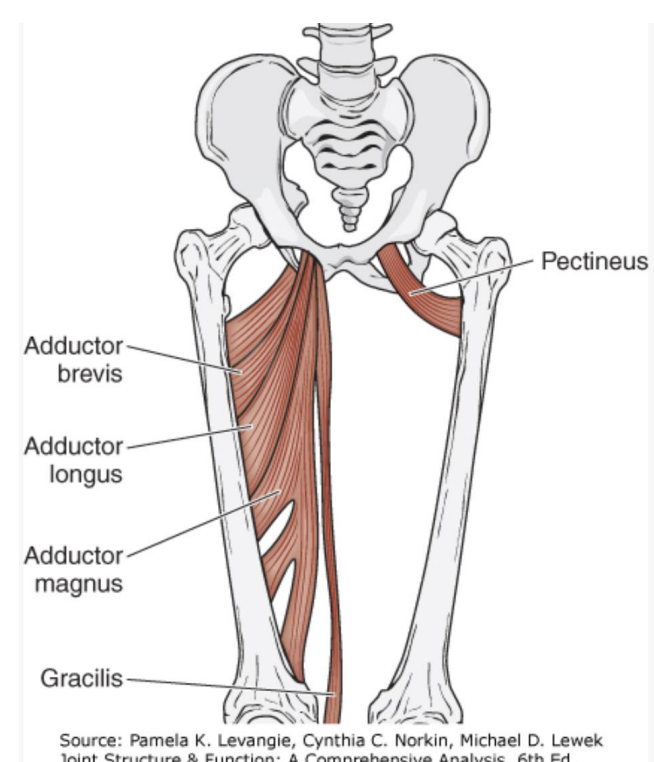
secondary hip adductors
biceps femoris (long head), gluteus maximus (lower fibers), quadratus femoris
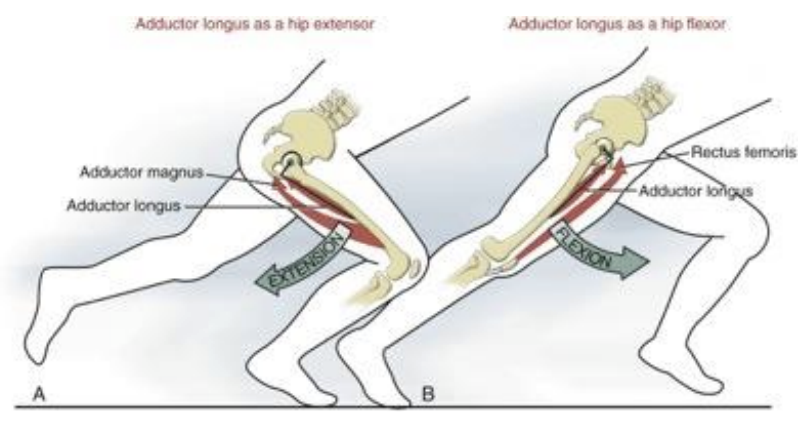
Dual action of adductor longus
dual sagittal plane action of the muscle demonstrated during sprinting
hip flexion, muscle is in position to extend the hip, along with the adductor magnus
hip extension, muscle is in position to flex the hip, along with the rectus femoris
actions are based on the change in line of force of the muscle
utilitarian function of the adductors may partially explain their high susceptibility to injury during running and jumping, especially while quickly changing directions
primary hip abductors
gluteus medius, gluteus minimus, tensor fascia latae
secondary hip abductors
piriformis and sartorius
primary hip external rotators
gluteus maximus, piriformis, gemellus superior, gemellus inferior, obturator externus, obturator internus, quadratus femoris
secondary external rotators
obturator externus, posterior fibers of the gluteus medius and minimus, sartorius, long head of the biceps femoris
hip internal rotators
NO PRIMARY IR because no muscle is oriented in the horizontal plane
adductors that possibly contribute to hip IR
adductor longus and brevis
pectineus
increased hip flexion, hip IR torque increase
secondary hip internal rotators
anterior fibers of the gluteus medius, gluteus minimus, tensor fasciae latae
pincer and CAM hip impingement
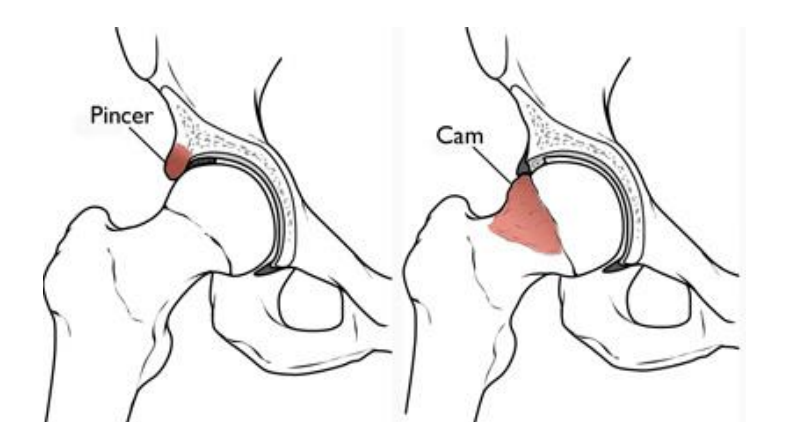
CAM hip impingement
excessive bony growth of the FEMORAL HEAD
leads to poor clearance of the femur specifically with flexion and abduction
can lead to labral pathology
pincer hip impingement
excessive bony growth of ACETABULUM
greater coverage of overhang of the acetabulum
causes compression of the superior labrum between rim and head of femur
can lead to labral pathology