Week 2- airway and drug admin +procedures
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
Capnography/ETCO2
Measurement of partial pressure CO2 exhaled
normal 35-45mmHg
can be represented in waveform/capnogram
Change in shape —> disease
Change in number — pt deteriorating
What does capnography show information about
Ventilation— how effective CO2 being eliminated
Perfusion— how effective CO2 being tx through vascular system
Metabolism— how effective CO2 being produced by cellular metabolism
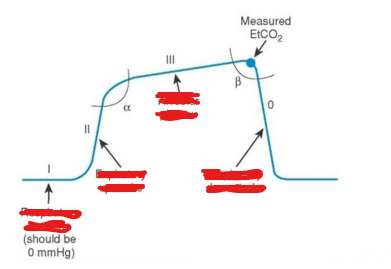
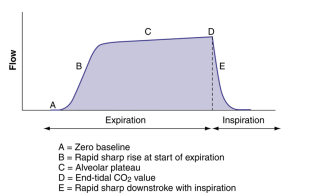
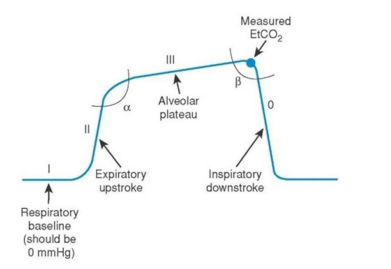
What is baseline, expiratory upstroke, alveolar plateau, inspiratory downstroke in Capnography?
Phase I – Baseline
• Flat line at the start of exhalation.
• Represents air from the anatomical dead space (trachea, bronchi, which don’t exchange CO2)
Phase II – Expiratory upstroke
• CO₂ air from alveoli begins to mix with dead space air.
• Steep upward slope.
Phase III – Alveolar Plateau
• Exhalation of pure alveoli gas
• Should be relatively flat in healthy lungs. • The end of this phase is where ETCO₂ is measured.
Phase IV – Inspiratory Downstroke
• Sharp drop as inhalation begins.
• Fresh air enters lungs, containing little CO2. Returns to baseline(<1% CO2 in air)
Compare pulse oximetry vs capnography
Oximetry pulse - O2
-Reflect oxygenation
-Lag in changes when hypoventilation or apnoeic
should be used with capnography
Capnography- CO2
-Reflect ventilation
-Hypoventilation apnoea detected immediately
-Should be used with oximetry pulse
Why does capnography detect hypoventilation/apnoeic instantly?
No breath —> no CO2 eliminated it flatlines instantly within 1 breath cycle
whereas oximetry pulse just measures how much O2 s circulating in blood which would remain high for minutes after
Values for CO2/Capnography
Normal 35-45mmHg
Elevated >45mmHg —> hypoventilation CO2 build-up
Decreased <35mmHg hyperventilation breathing too fast
Capnography waveform indications/contra/complic
Indic:
CPR
Sedation and procedural sedation
Ongoing monitoring of ventilation
Contra:
nil
Complic:
When performing effective CPR etCO2 must not be used to vary IPPV from recommended rate
10ml syringe markings
every large mark is 1ml
every small mark is 0.01ml
Vanish point 3ml syringe markings
every large mark is 0.5ml
every small mark is 0.1ml
Vanish point 1ml syringe markings
every large mark is 0.1ml
every small mark is 0.01ml
When drawing up 1ml of drug for injection, what syringe should you use? 10ml? 1ml? 3ml?
3 ml syringe, it would be hard to do 1ml into 1ml syringe
What are the contraindications for i-gel insertion?
• Conscious breathing patients
• Continuous use >4 hours
What are possible complications of i-gel insertion?
• Failure to ventilate adequately
• Patient intolerance
• Hypoxia
• Vomiting and aspiration
• Oropharyngeal trauma
What patient position is used for i-gel insertion?
Sniffing position to align:
• Oral axis
• Pharyngeal axis
• Laryngeal axis
Exceptions:
• Neutral position if C-spine injury
• Elevate head in obese patients
How should the i-gel be held during insertion?
• Hold along tubing/bite block
• Cuff outlet facing towards the chin
What should you do if early resistance is felt during i-gel insertion?
Perform a triple airway manoeuvre and continue gentle insertion.
How do you confirm correct placement of an i-gel?
• No air leaks when ventilating with BVM
• Incisors resting on bite block
• Chest rise and fall
• Fogging/misting in tube
• Breath sounds on auscultation
• ETCO₂ waveform
• Increasing SpO₂
What are the benefits of the gastric drainage port in an i-gel?
• Passive gastric drainage
• Active suctioning
• Reduces aspiration risk
• CPR
• IPPV ventilation
• Drowning
• Alcohol/food ingestion
• Obese or pregnant patients
How is the gastric tube length measured?
Measure from:
Nose → Earlobe → Xiphisternum
What does ETCO₂ measure?
The concentration of carbon dioxide at the end of exhalation.
What is the normal ETCO₂ range?
35–45 mmHg
What does ETCO₂ tell us about ventilation, perfusion, and metabolism?
Ventilation
→ Effectiveness of CO₂ elimination
Perfusion
→ Effectiveness of CO₂ transport through blood
Metabolism
→ Amount of CO₂ produced by cellular metabolism
What are contraindications for intranasal medication?
• Suspected nasal fractures
• Blood or mucus obstructing nasal passage
What is the dead space volume in intranasal devices?
0.1 mL
(Extra medication should be drawn up to account for this.)
When should intranasal medication be split between nostrils?
If >0.5 mL
Splitting improves surface area absorption.
When should you seek an alternate route instead of intranasal?
Back:
If dose >2.0 mL
What direction should the MAD nasal device be aimed?
Slightly upwards and outwards toward the ear.
How does IM drug absorption compare to oral and IV?
Faster than oral
Slower than IV
What is the maximum volume per IM injection site?
2 mL
If more → split between sites
What are common IM injection sites?
• Deltoid
• Vastus lateralis
What are possible complications of IM injections?
• Pain
• Minor haemorrhage
• Abscess
• Cellulitis
• Nerve damage
• Blood vessel damage
Where is the deltoid injection site located?
Inverted triangle:
• 1–3 finger widths below acromion
• Midpoint of lateral arm
Volume: 0.5–1 mL
Not suitable for <2 years old
Where is the vastus lateralis injection site?
Middle third between:
• Greater trochanter
• Lateral knee
Preferred for:
• Children
• Larger volumes
What is the Z-track technique?
• Pull skin laterally before injection
• Inject medication
• Release skin after needle removal
Prevents medication leakage back through track
What are the indications for IV cannulation?
• Medication administration
• Fluid resuscitation
• Blood product administration
Where should you avoid inserting an IV cannula?
• Burns
• Infection
• Trauma
• Significant oedema
What conditions make a limb contraindicated for IV access?
• Lymphoedema
• Arteriovenous fistula
• Post-mastectomy limb
What are complications of IV cannulation?
• Redness, swelling, pain
• Infection (commonly Staphylococcus aureus)
• Extravasation of drug/fluid
What are common breaks in aseptic technique during cannulation?
• Re-touching site after cleaning
• Assuming gloves are sterile
• Placing sterile equipment on dirty surfaces
• Touching sterile sheath
What is the preferred IV site in stable patients?
Dorsum of the hand
Advantages:
• Veins splinted by bones
• Good stability
What IV site is preferred for rapid fluid administration?
Antecubital fossa
What cannula sizes are commonly used in adults?
20G (Pink)
→ Standard drug administration
18G (Green)
→ Rapid fluids
16G
→ Major resuscitation
What is the purpose of priming a giving set?
To fill the IV line with fluid and remove air before connecting to the patient.
What is a major complication if IV lines are not primed properly?
Air embolism
What is Ruby’s Rule in IV fluid administration?
Never re-spike a bag of IV fluids.
(Associated with fatal infection in a 3-year-old.)
When considering IV cannulation in children, what question should you ask first?
Is there a more suitable route of administration?
Examples:
• Intranasal
• Intramuscular
• Oral
IV access may be more difficult and traumatic in paediatric patients.
What challenges affect IV cannulation in elderly patients?
Age-related changes include:
• Fragile skin
• Fragile veins
• Increased bleeding risk
• Medications (e.g. anticoagulants)
These increase the risk of vein rupture, bruising, and bleeding.
Why is IV cannulation contraindicated in a post-mastectomy limb?
Because lymph nodes may have been removed, leading to:
• Increased risk of lymphoedema
• Increased risk of infection
Why should you avoid IV cannulation in a dialysis fistula limb?
Dialysis fistulas alter vascular structure and are essential for dialysis.
Risks include:
• Damage to fistula
• Infection
• Reduced dialysis access
What determines the size of IV cannula you choose?
It depends on what you need the IV for.
Consider:
• Medication volume
• Fluid resuscitation
• Viscosity of solution
• Speed of administration
• Difficulty obtaining access
What cannula size is appropriate for small doses of medication?
20G cannula (pink) is commonly used.
Suitable for routine drug administration.
What cannula size is used for rapid fluid or large volume administration?
8G or larger
Examples:
• 18G (green)
• 16G (trauma/resuscitation)
Larger bore = faster flow rate.
Why might a larger cannula be needed for thick solutions?
Thicker solutions flow more slowly through small cannulas.
Larger bore allows easier flow and prevents blockage.
What is the priority in a peripherally shut-down patient?
Obtaining any IV access possible.
Cannula size may be less important than achieving vascular access.
Why is IV kit organisation important before cannulation?
It ensures:
• Efficiency
• Aseptic technique
• Reduced procedure time
• Better patient safety
Set yourself up before touching the patient.
What equipment should be prepared for IV cannulation?
Typical IV setup includes: T
• Tourniquet
• Antimicrobial swab
• Cannula
• Sharps container
• Dressing/bandage
• OpSite dressing
• Saline flush
What is the purpose of a tourniquet during cannulation?
It temporarily restricts venous return, causing veins to:
• Engorge
• Become easier to see and palpate
What is the purpose of a saline flush after cannulation?
To:
• Confirm patency of the cannula
• Ensure it is not infiltrated or extravasated
• Clear medication from the line
Why is the dorsum of the hand often preferred for IV cannulation?
Because:
• Veins are splinted by surrounding bones
• Reduced movement compared to joints
• Good stability for cannulas
What is a disadvantage of using the antecubital fossa for IV cannulation?
The cannula can become occluded when the arm bends.
However, it is useful for rapid fluid administration.