principles of endo access- max anteriors
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
goals of access include:
locate ________
__________ access to canals
removal of ________ and _________
conservation of _______
all canals
straight-line
chamber roof; coronal pulp tissue
tooth structure
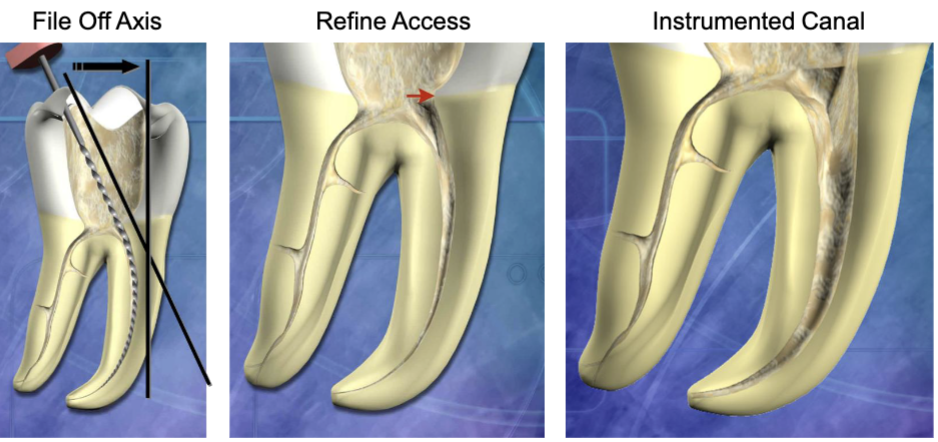
what is straight line access
unimpeded access of the instruments in the canals to the apical 1/3 of the canal or the first curve (if present)

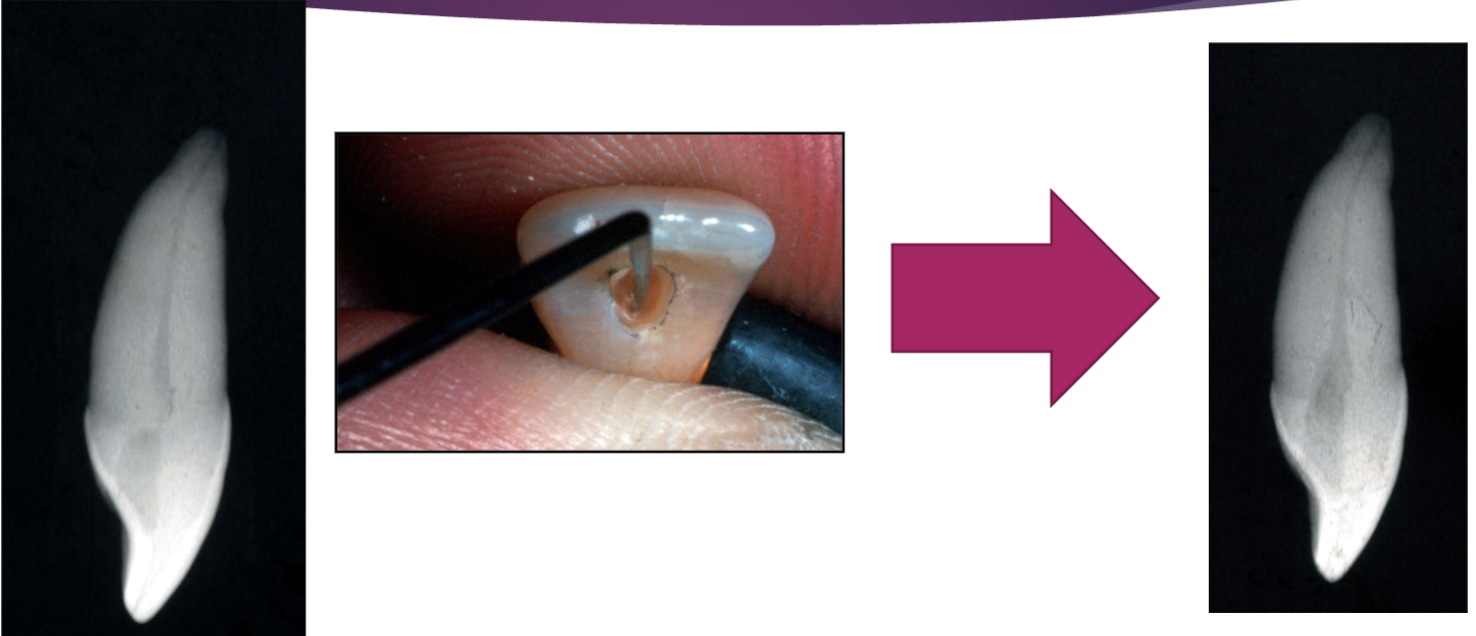
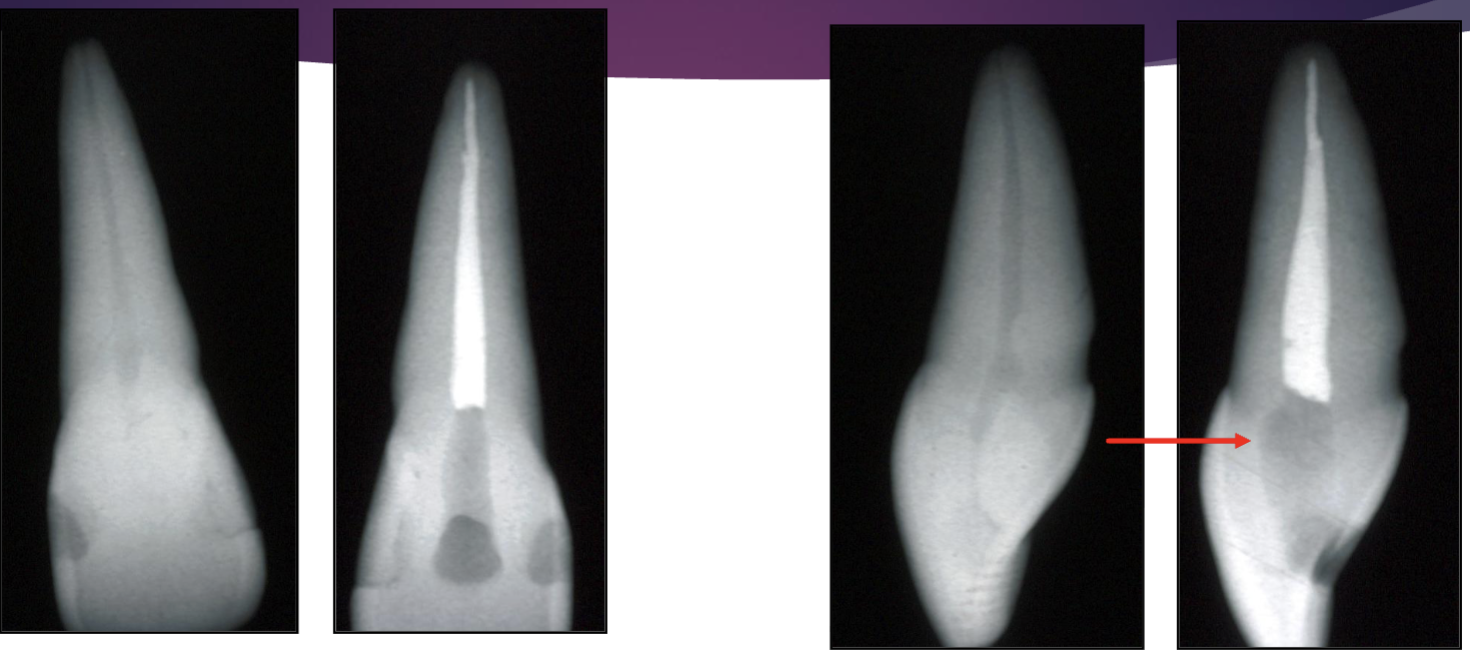
is this an example of straight line access
NO: need to open orifice (where red arrow is pointing) to be able to get straight line access
_______ dictates shape of access
pulp chamber
the access should be as _____ as possible but as ______ as necessary
small; large
if access is too small, this can lead to… (3)
difficulty locating canals
missed canals
difficulty achieving straight-line access
if access hole is too big…(3)
unnecessary removal of tooth structure
inc risk of fracture
inc risk of perforation
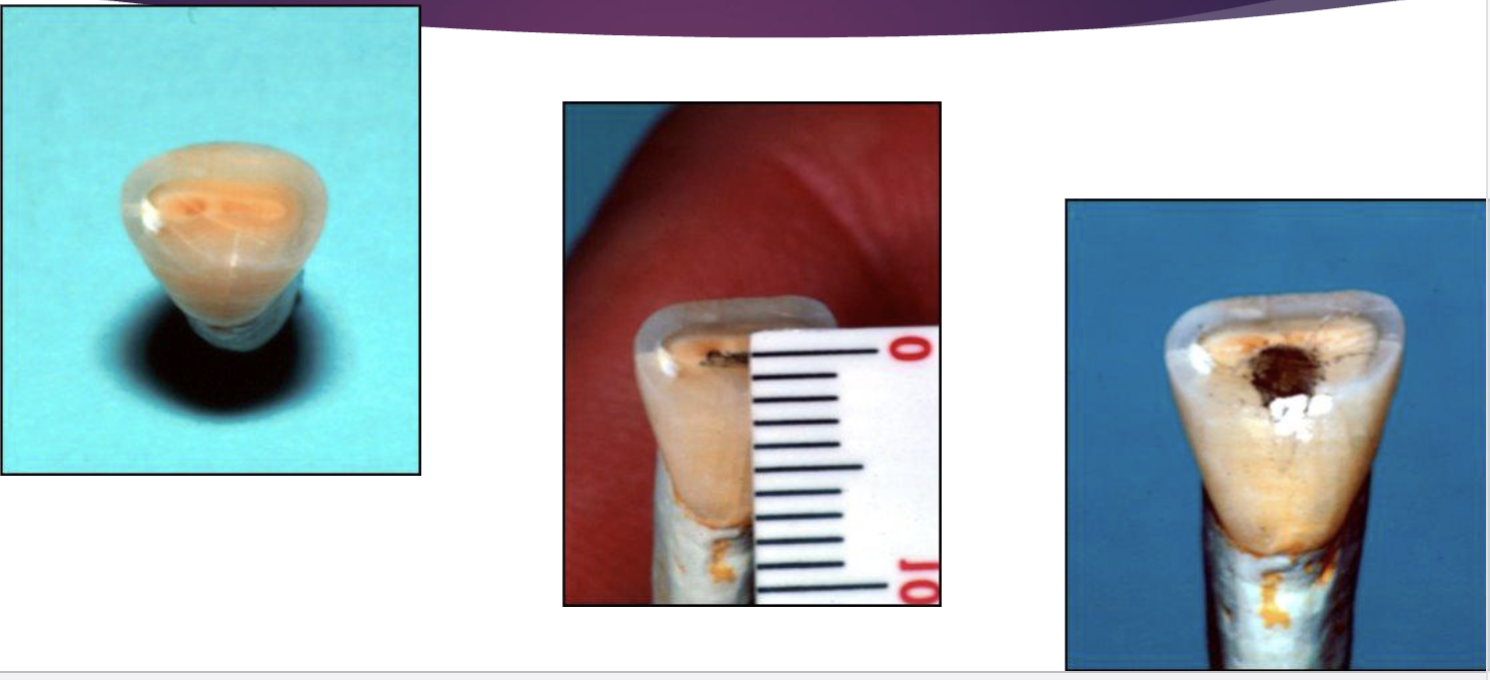
the removal of pulp materials from the pulp horns/crown is necessary to prevent…
coronal discoloration
4 principles of access
outline form
convenience form
caries removal
toilet of the cavity
what is the outline for of access
recommended shape of the access
projection of internal tooth anatomy onto external root structure
may change over time w calcification of chamber
what is convenience form for access
modification of ideal outline form to facilitate instrument placement and manipulation
reason for caries removal for access
prevent contamination of root canal system
assess restorability
provide sound tooth structure for temporization/restoration
what is toilet of the cavity for access
keep it clean → prevent debris from blocking canal by frequently irrigating
out of the 4 principles of access, which is done first
caries removal
7 steps for access opening procedures
study pre-op radiograph
estimate depth of access from RG
remove all caries, may/may not remove restorations
access: use 701 fissure bur w high speed
use DG-16 endo explorer to detect chamber/canal orifice
re-eval as needed during access w tactile sensation to make sure you create straight-line access and open orifice
expose RG if needed
what is an orifice
opening of the root canal inside the pulp chamber
between a maxillary lateral and central, which is more bulky
central
maxillary anterior teeth have ___ (#) canal
1
in mandibular canines, 30% have ____ canals. from this, __% have the 2 canals join, and __% exit separate
2; 20%; 10%
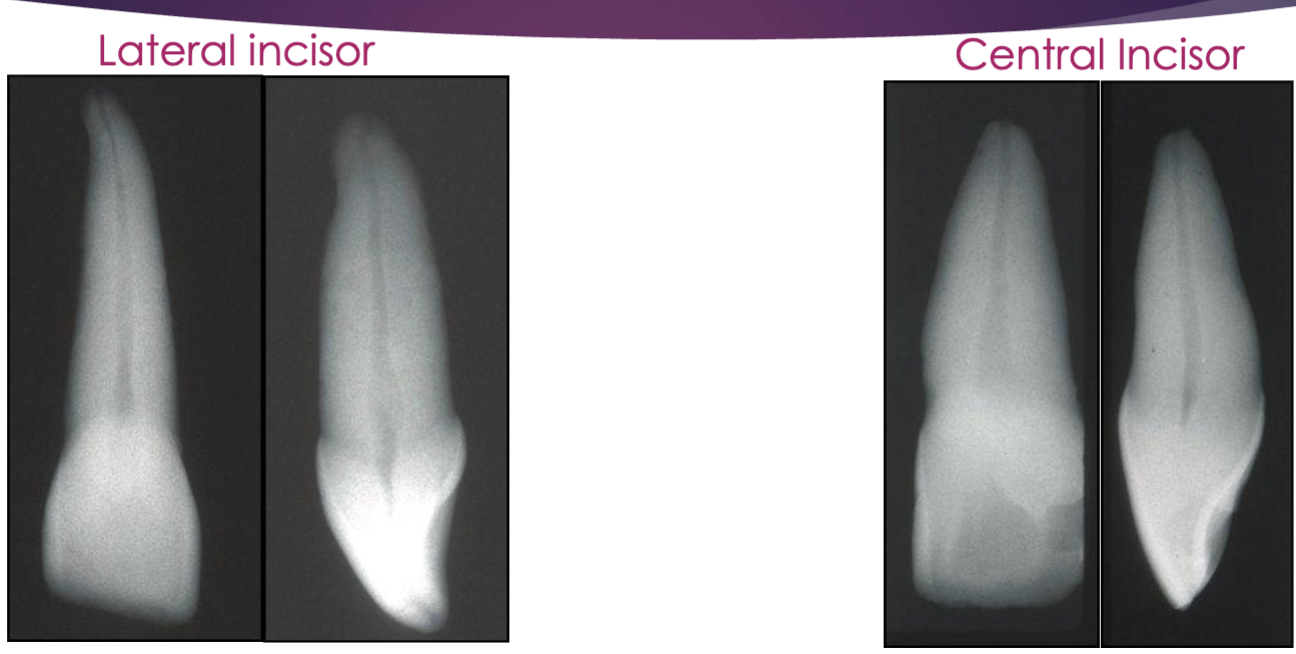
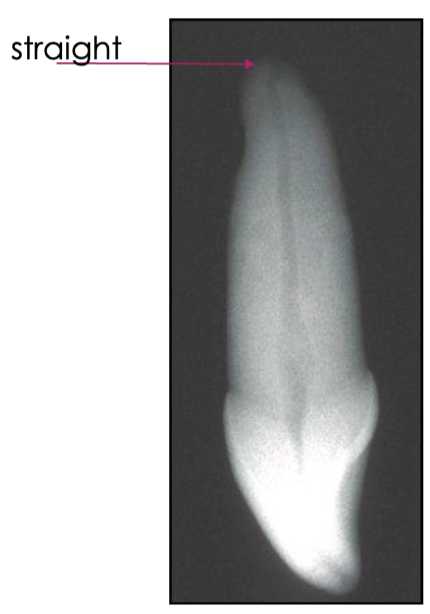
shape of the root of a central incisor
usually straight
shape of root of a lateral incisor
usually apical curvature to distal or palatal
shape of root of a canine
long, usual apical curvature
w canines, it can be difficult to radiographically interpret the apical portion due to…
a small root root tip
what does the canal shape look like in the mid root vs the apical third of a maxillary central incisor
both are round

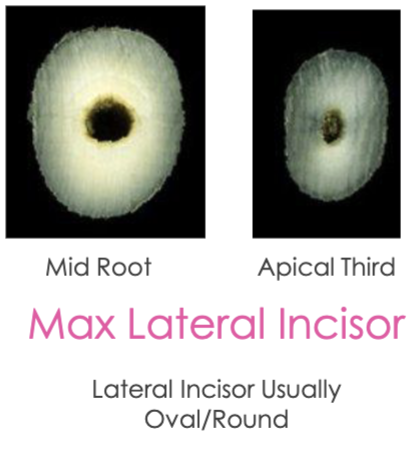
what does the canal shape look like in the mid root vs the apical third of a maxillary lateral incisor
can be round or ovoid
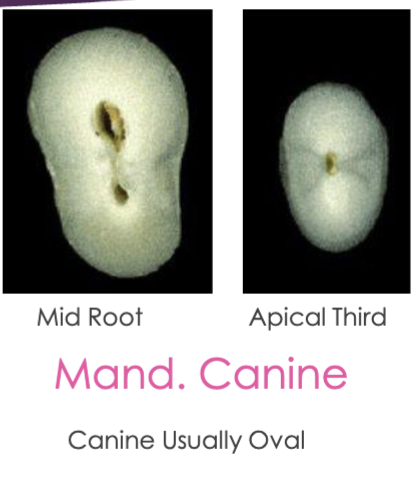
what does the canal shape look like in the mid root vs the apical third of a mandibular canine
usually oval, mid root can start separate and then join in apical third
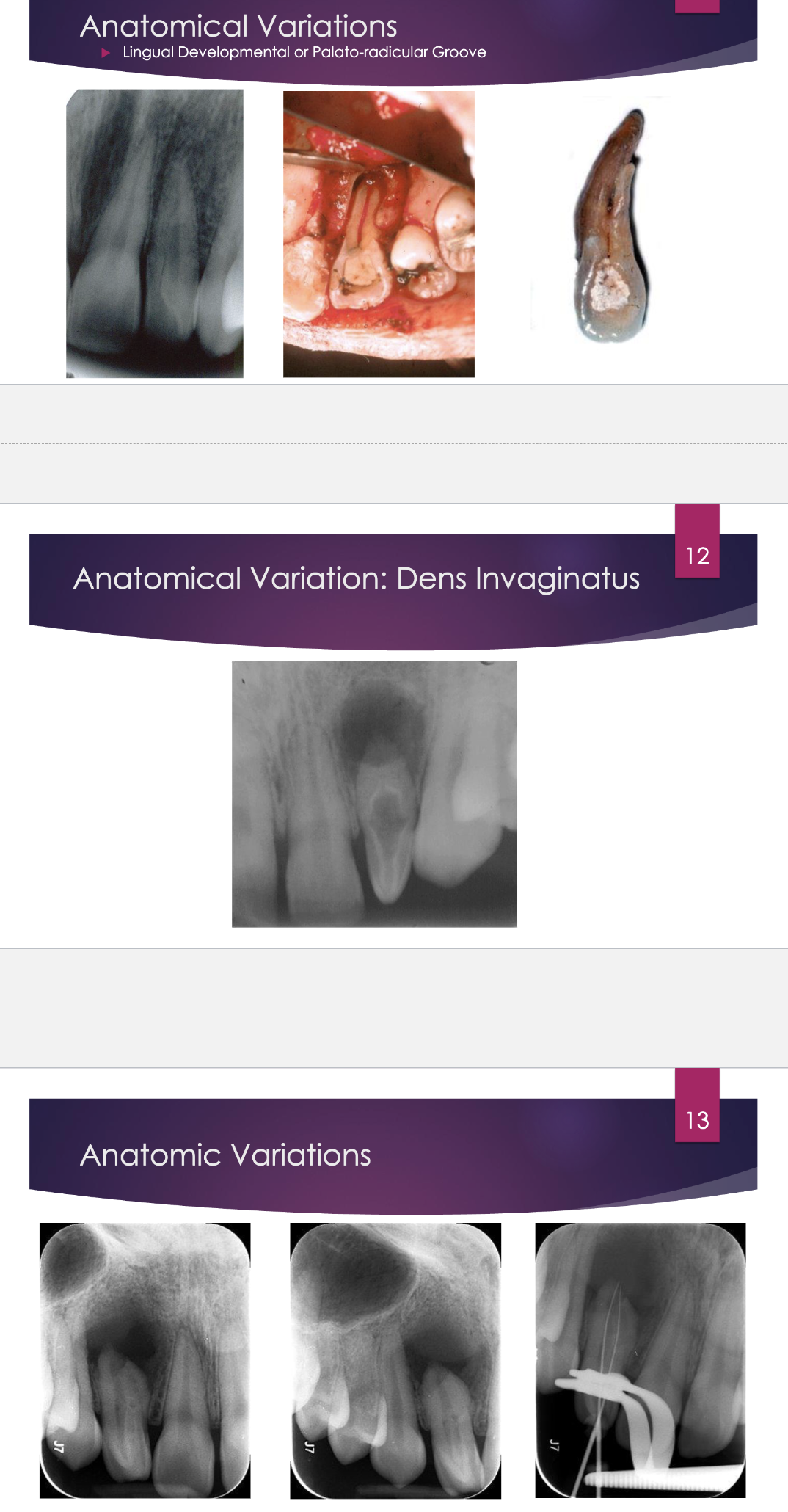
what are some anatomical variations you may see in maxillary anterior teeth (would NOT want to choice these as exercise teeth)
lingual developmental or palato-radicular groove
dens invaginatus
talon cups
the apical root of a maxillary central incisor may curve ____ or _____
distal; labially
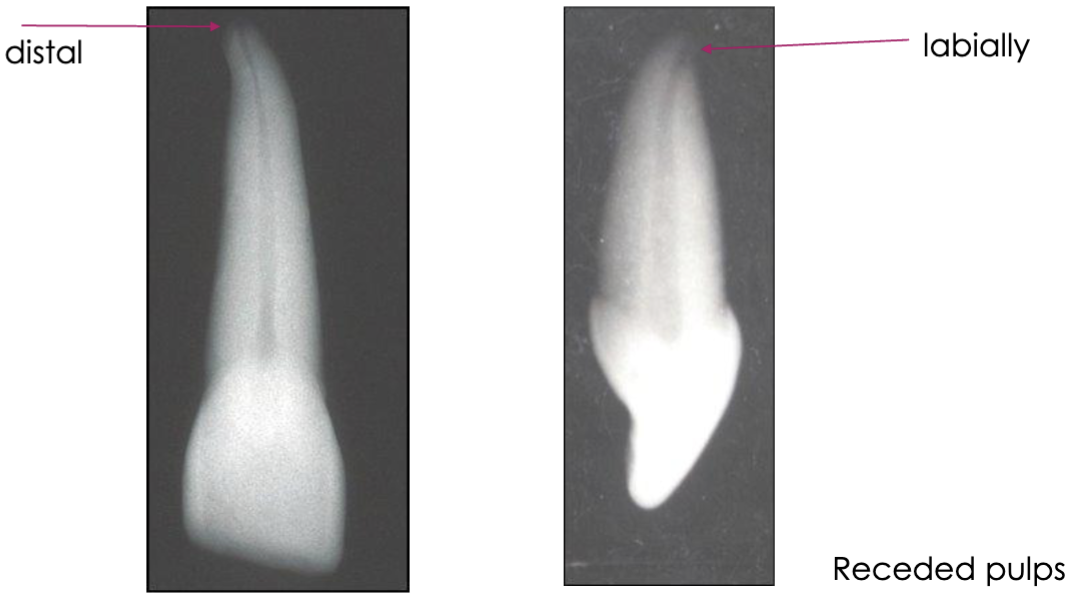
canals of maxillary central incisors are usually ________
straight
when determining the access outline for maxillary incisors, you want to know the incisal limit, what does this mean
determined by incisal edge and cavoangle of the lingual so that you get underneath the incisal edge to obtain straight-line access
why is access always done on the lingual vs the incisal edge of anterior teeth
for esthetics
how would a worn maxillary incisors affect the incisal limit
incisal edge can be worn to or beyond the incisal limit
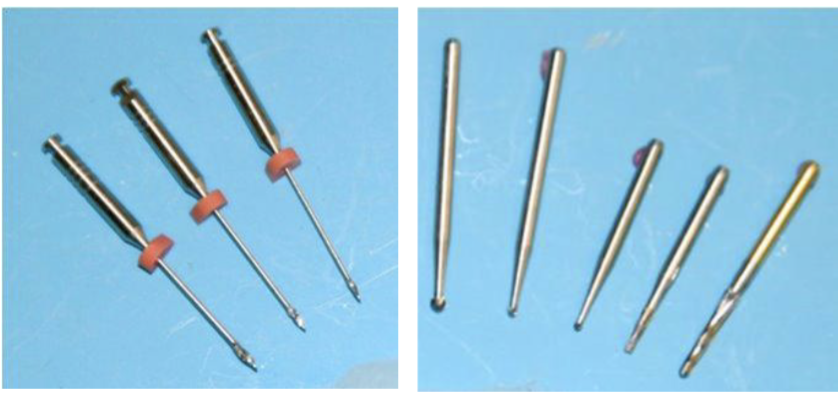
order of burs to complete access (but keep in mind the order is not definite)
initial access: 701/#1 round/ Endo Z
remove lingual shoulder/pulp horns/smooth: FG surgical length 2/4 bur
enlarge orifice/canal: slow speed w gates glidden #2/3/4
how to cut the cavo-surface outline
#701: about ~1.5 mm depth, hold perpendicular to tooth to get under incisal edge
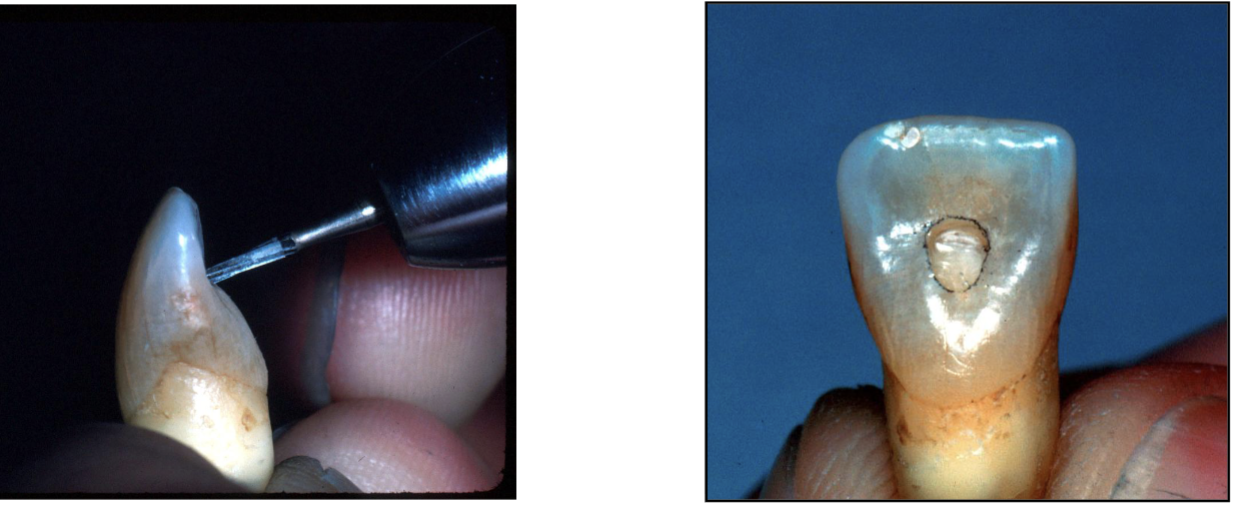
how to access prep into the pulp chamber after cavo-surface outline has been cut
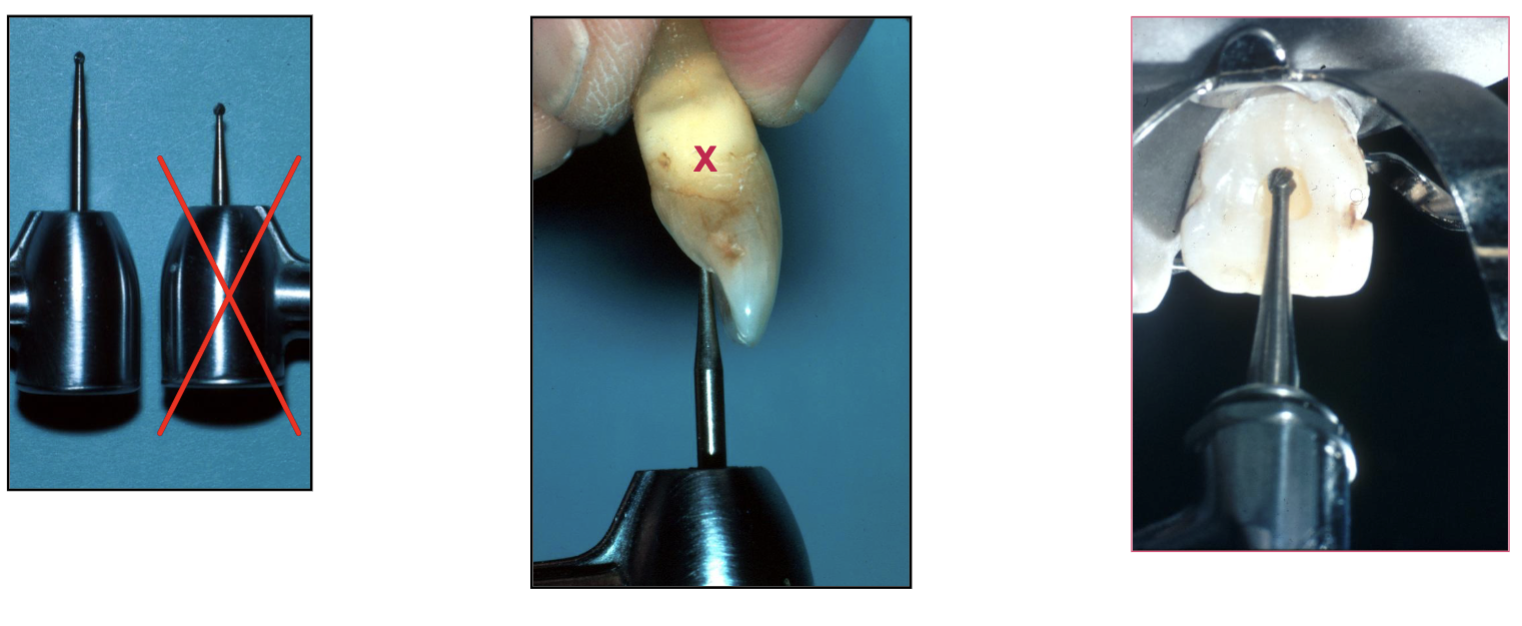
use surgical bur #2 (NOT short) to follow the long axis of the tooth
what you are feeling for when exploring the pulp chamber (w explorer)
what to find orifice, feel what you need to open more, if explorer doesn’t fit, need to open more
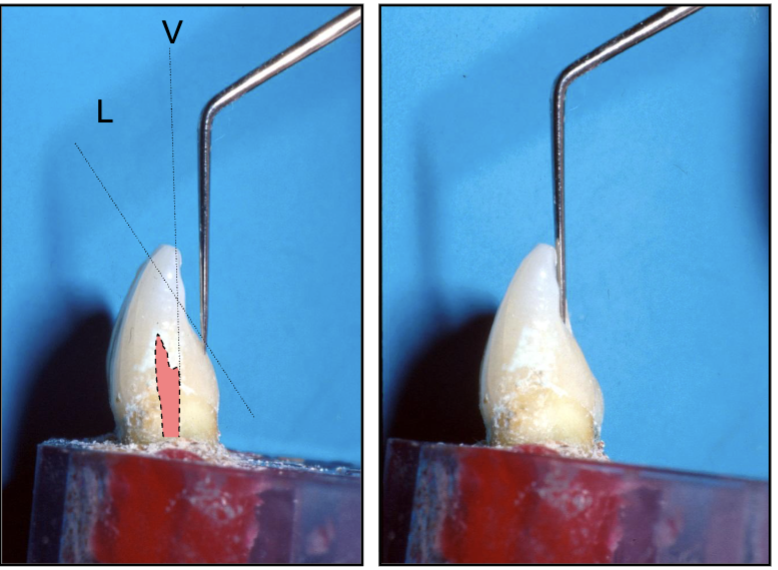
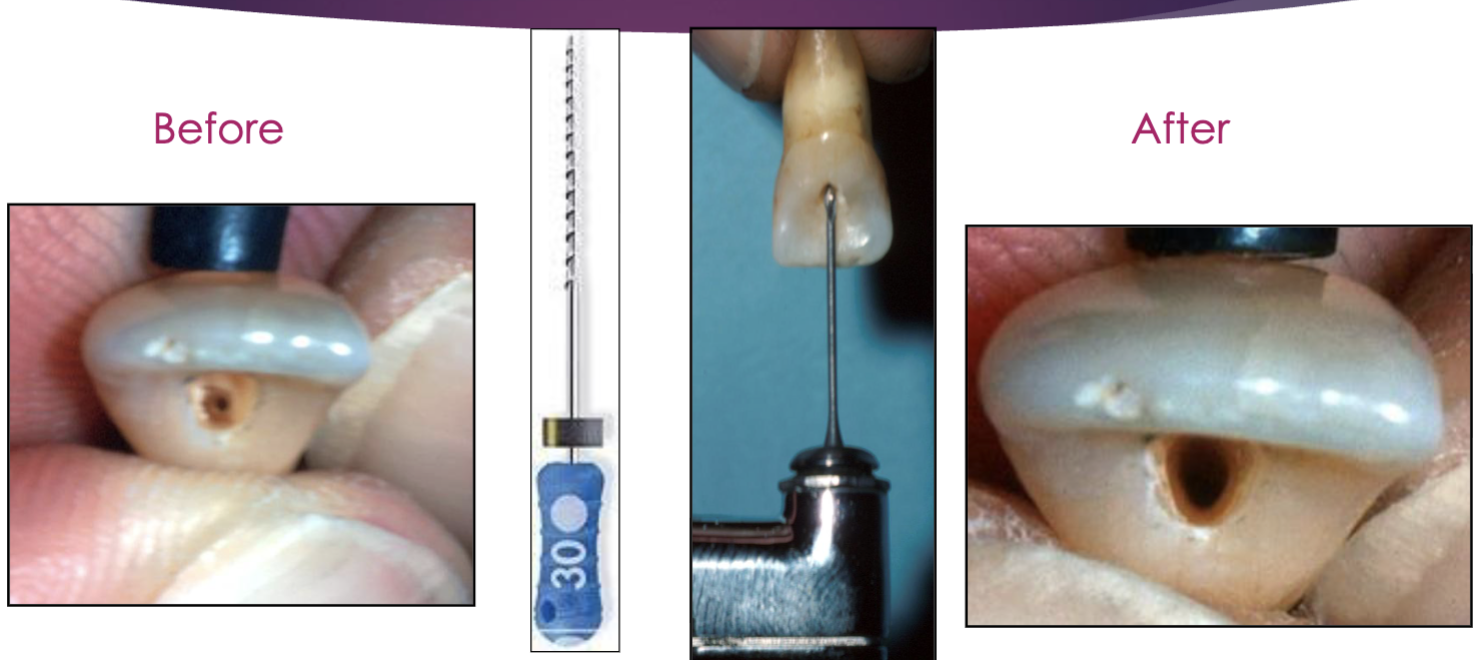
in maxillary incisors, it is important to remove the ____ (near the orifice) in order to get straight line access
lingual shoulder

what can you remove the lingual shoulder w
gates glidden #2/3/4 and hedstrom file
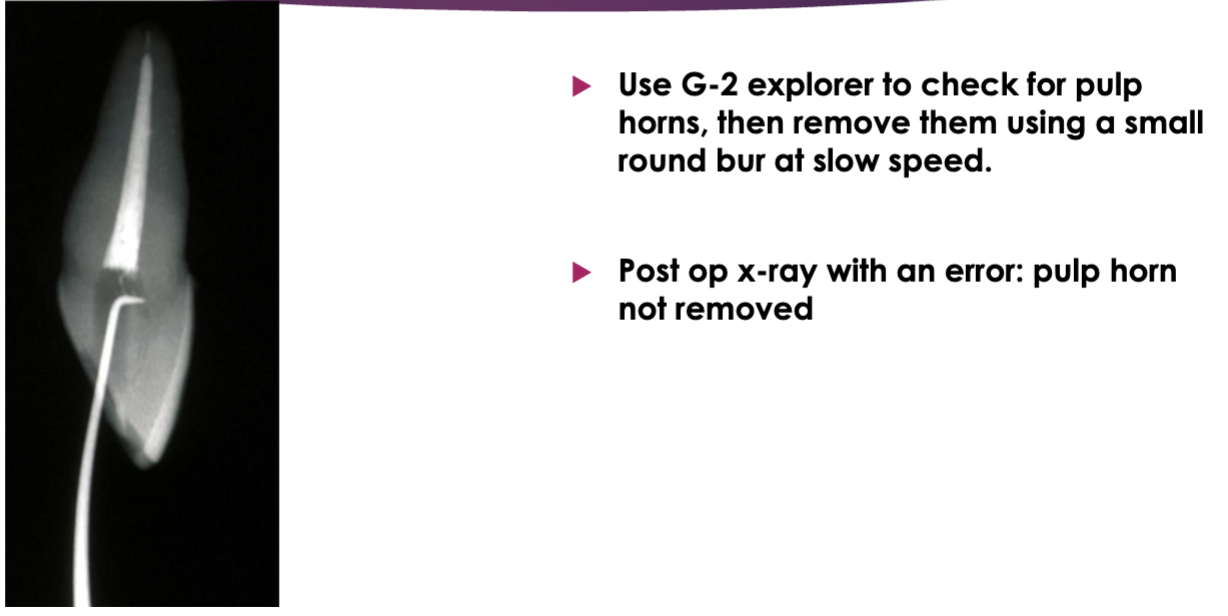
what should you be doing to check for pulp horns
use G2 explorer → if catching → use a small round bur at slow speed
if you’re having trouble opening the chamber and orifice, what questions can you ask yourself
how far are you in the pulp chamber?
are you under the incisal edge?
is your access large enough to have illumination to help locate the pulp space?
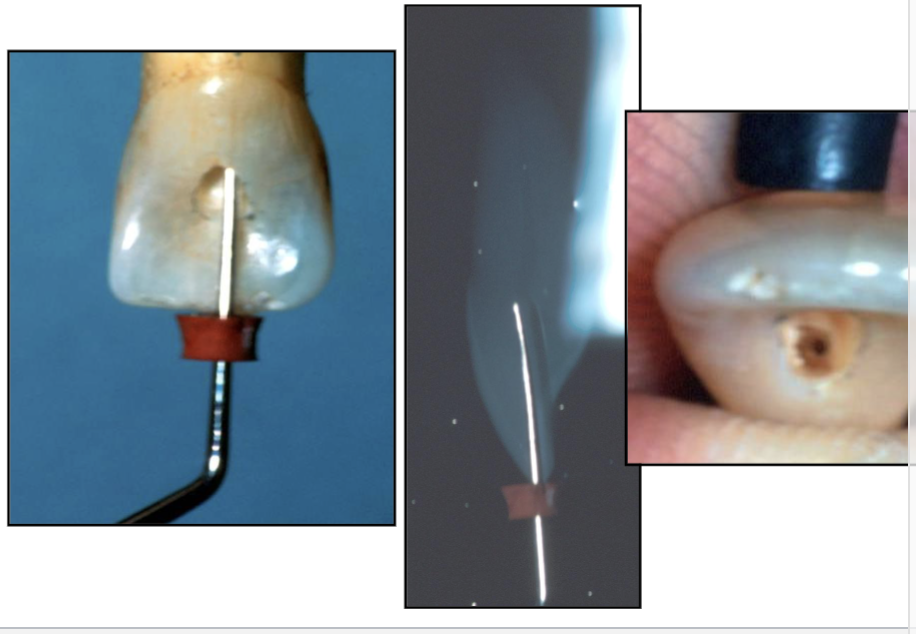
what error happen here
gouge towards the facial → opening too far
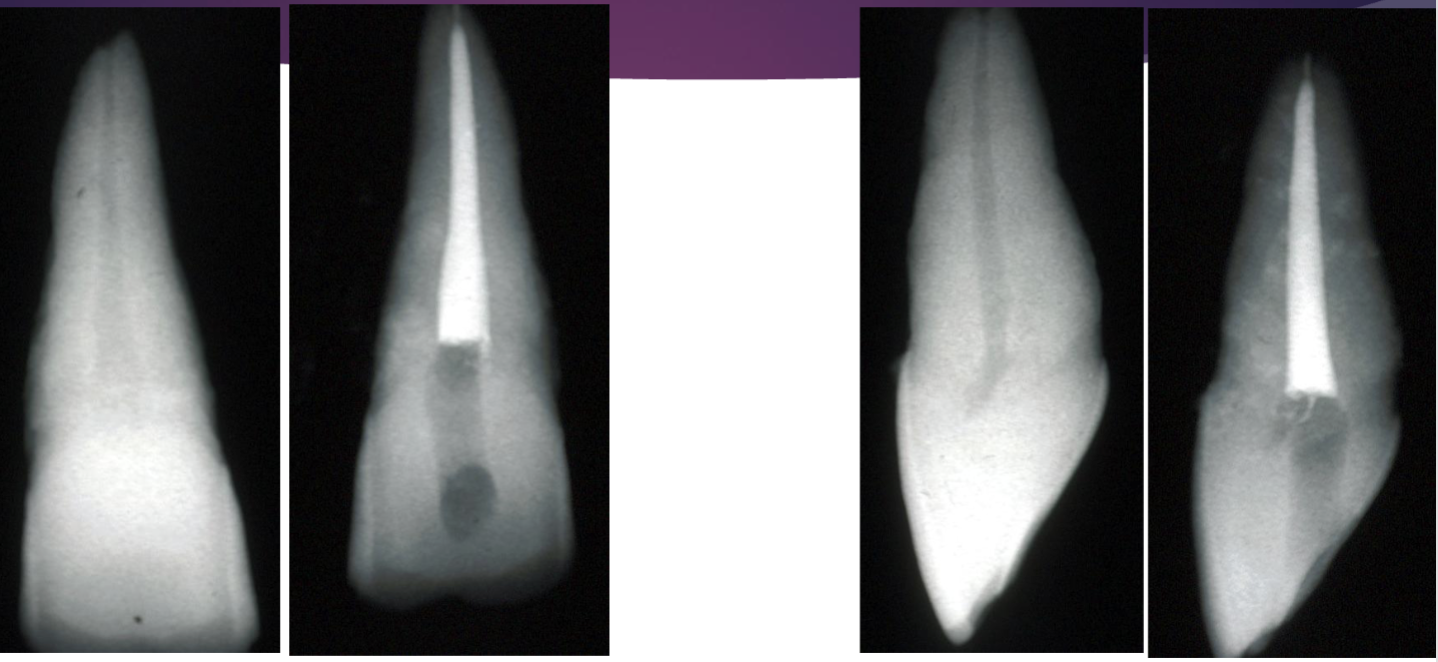
what error happened here
pulp horn not incorporated w access (was not removed)