psyc 337 - suicide and non suicidal self injury
1/56
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
suicide
death resulting from intentional self injurious behavior, associated with any intent to die as a result of the behavior
suicide attempt
a nonfatal self directed potentially injurious behavior with any intent to die as a result of the behavior
interrupted attempt
a person takes steps toward making a suicide attempt but is stopped by another person prior to any injury or potential injury
self-interrupted/aborted attempt
a person takes steps to injure self but stops self prior to any injury or potential for injury
preparatory acts or behavior
acts or preparation toward making a suicide attempt
suicidal ideation
thoughts of suicide
items in questionnaire
I had thoughts of suicide. I thought that the world would be better off without me. I thought about my own death
Non-suicidal self-injurious behavior
behavior that is self directed and deliberately results in injury or the potential for injury to oneself
suicide stats for Canada
9th leading cause of death across all age groups in Canada, almost 4000 people. in Quebec, almost 900 people
how many deaths per 100,000 people for males
16.3
how many deaths per 100,000 people for females
5.7
suicidal thoughts stats
3.4 million. 11 million 18 to 34. 487500 males 18 to 34. 656700 females 18 to 34
3 key elements WHO
agency, intent, outcome
suicide and nssi in dsm prior to dsm5
listed as symptoms of depression and bpd
suicide and nssi in dsm 5
now includes conditions for further study- suicidal behavior disorder and nonsuicidal self injury disorder
research challenges in suicidality
rare, etiologically complex, difficult to study longitudinally, stigma/legal constraints, replication
common research methods
archival, psychological autopsy, big data
archival
data is obtained from preexisting records, databases, look at how variables relate to each other at any given moment
psychological autopsy
reconstruct what a person was like before the suicide through interviews with family, friends, co-workers, etc
big data
passively collect data from individuals (geolocation, social media, activity trackers, phone calls, purchasing history)
gender
women attempt suicide at significant higher rates than men in North America. but 77% of deaths by suicide are male. 4:4:1 to 3:6:1
proposed explanations for gender differences
base rates, lethal means, access, greater intent, mental health care, cultural acceptance, reactions from others
suicide - race and ethnicity
higher in American Indian, eskimo, Aleut, non-hispanic and white non hispanic
suicide and indigenous populations
Canadian indigenous people have among the highest rates of suicide in the world. not equally distributed across First Nation populations. Inuit people - 6.5 x higher risk than non indigenous. First Nations - 3.7x higher. Metis - 2.7X higher. Durkheim - language and community cohesion. higher community rates of a number of risk factors
most common methods used to attempt suicide
poisoning, cutting, stabbing
most common reason for death from suicide in US/canada
firearm suicides/hanging, suffocation, poisoning, fall/firearm
are risk factors warning signs
no
risk and protective factors
some are modifiable (depression, access to lethal means), and some are not (race, genetic predisposition, family history of suicide). reducing risk factors and increasing protective factors can help prevent suicide
risk factors for suicide
mood disorders, shizophrenia, anxiety, pds, EDs, conduct disorder, alcohol abuse, drug abuse, impulsivity, aggressive tendencies, perfectionism, history of trauma, physical abuse, sexual abuse, major physical illness, chronic pain, TBI, family history of suicide, suicidal friend, job/finincial loss, relationship loss, other stressful life event, lack of social support, barriers to health care, cultural/religious beliefs, problem solving skills deficits, non suicidal self injury, elevation, lgbtq, bullying, asthma, poor air quality, past attempt
proximal risk factors (proximal to attempt)
intoxication - approximately 25 to 50% of adults who die by suicide are intoxicated at the time of death. usually alcohol, but sometimes other substances as well. rates higher in younger people. access to means - people who have greater access to lethal means are more likely to die by suicide - treatment is means restriction
suicide contagion in the media
exposure to the suicide or suicidal behavior of one or more persons influences others to engage in these behaviors. exposure can occur via multiple channels. rates of suicide/suicidal behaviors appear to be influenced by frequency of media reporting (does dependent), content of media reporting (dramatic headlines, front page, explicit about suicide methods). positive/negative reporting biases (attitudes towards suicide, portrayal of suicide completes, consequences). unclear how suicide contagion occurs
protective factors
treatment (either psychosocial or pharmaceutical). lithium and clozapine (for bipolar and psychosis, respectively). preventative interventions like working to reduce aggressive behaviors in early elementary school seems to delay or prevent the onset of suicidal behaviors in young adulthood. culturally-influenced coping strategies, like values reflecting strong moral objections to suicide, and high family support = lower incidence of ideation and attempts among latinos
biological factors
evidence from win studies that suicidal behaviors are genetically influenced. adoptions studies - rates of suicide in bio relatives of adoptees who died by suicide higher than rates in adopted families. impulsivity and fearlessness is inherited
impulsivity and fearlessness
impulsivity has many dimensions - poor premeditation, sensation seeking, lack of perseverance, negative urgency. negative urgency higher in both ideates and attempters (compared to controls). poor remediation higher in SA. neither SI nor SA higher in sensation seeking or lack of perseverance. fearlessness, reduced pain sensitivity.
ideation to action
acquired capability? interpersonal psychological theory. 3 step theory. reduced fear of pain and death
Thomas Joiner: Interpersonal Psychological Theory
exposure to painful and fearsome stimuli reduces innate fears of pain and death. making it easier to approach the task of attempting suicide
3-Step Theory (Klonsky & May)
practical, dispositional, acquired.
Environmental Influences on Capability
capacity can arise through practice, habituation, and experience. playing more hours of violent video games correlated with greater capacity, even when controlling for previous painful life events. among vet students, greater exposure to euthanasia associated with increased fearlessness. among physicians, greater exposure to provocative work experiences (surgeries, treating trauma) associate with increased capacity
Distinguishing Attempters from Ideators
meta analysis of 27 studies comparing 12 sociodemographic and clinical variables between suicide attempters and ideates. depression severity, ptsd, depressive disorder for suicide
nssi course and prevalence rates
like suicide attempts, NSSI onset tends to peak during adolescence/young adulthood. rates of nssi may decrease with middle age
nssi age of onset
13
suicide attempts onset
16
nssi prevalence
lifetime prevalence of NSSI - 13 to 28 percent worldwide. in clinical samples as high as 80. prevalence fairly stable in all regions of the world that have been studied
methods, lethality, frequency
suicide attempts most highly lethal methods (hanging, ingestion of toxic substances). NSSI - low lethality behaviors that result in minimal damage (cutting, skin abrading, interfering with wound healing, banging/self hitting, burning). most people who endorse repeated NSSI use more than one method (average of 4). people endorsing suicide attempts often use the same method, but increase the lethality
sexual orientation and gender
gender diffs inconclusive. rates of NSSI higher in LGBTQ individuals than cis-het. risk of nssi (and suicide attempts) peaks during the coming out process. risk somewhat more pronounced for men than women
interpersonal functions of NSSI
autonomy, interpersonal boundaries and influence, peer bonding, revenge, sensation seeking, toughness
intrapersonal functions of NSSI
affect regulation, anti dissociation, anti suicide, marking distress, self punishment
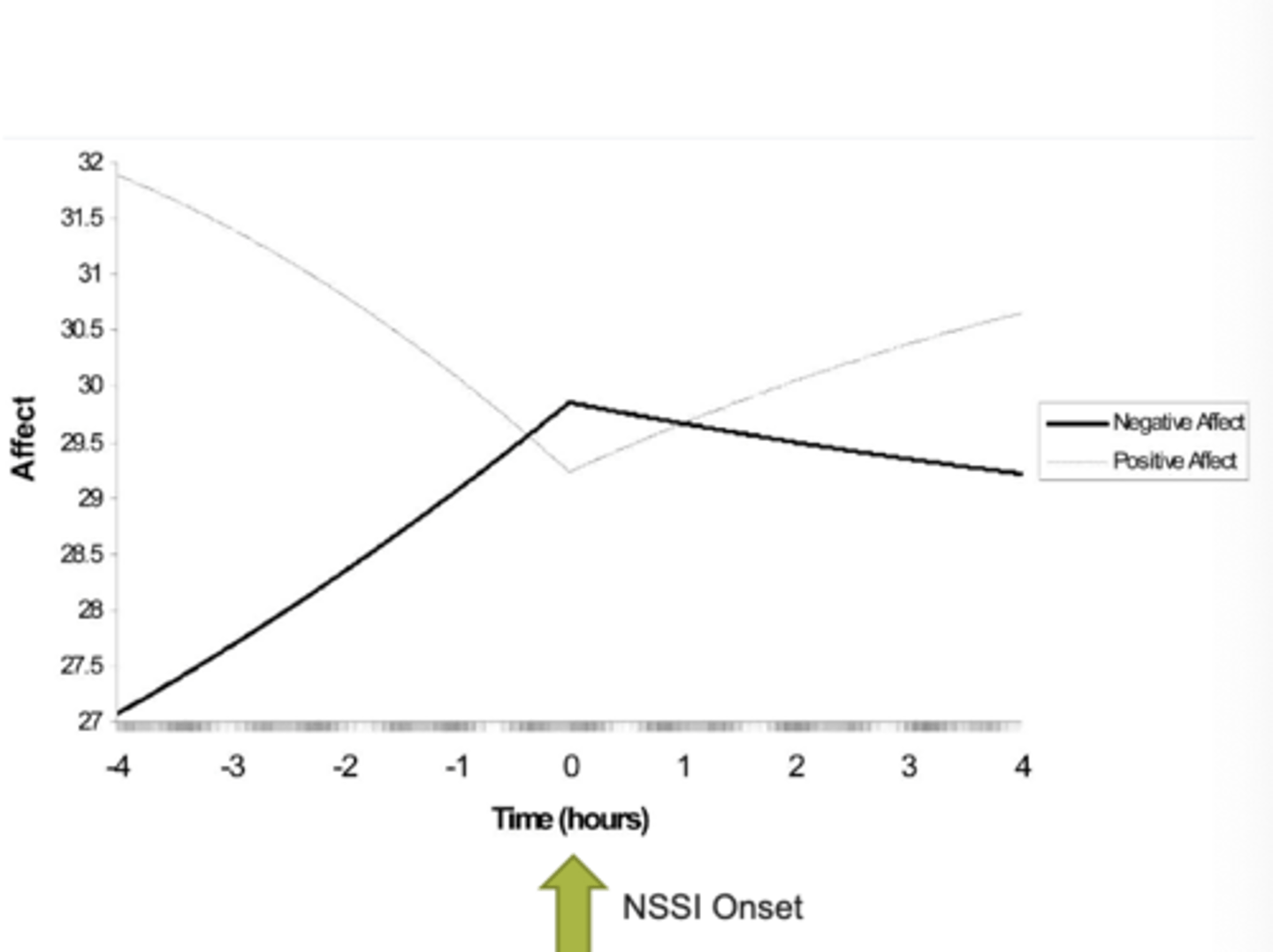
NSSI in real time
131 females with bulimia, 19 with NSSI and 122 without NSSI. collected EMA over 2-week period. reported engagement in NSSI as well as positive and negative affect
nssi relationship to suicide
up to an 85 percent of people attempting suicide have a history of NSSI. college students with a history of NSSI 8 x more likely to have suicidal ideation, 25x more likely to have attempted suicide than students with no NSSI. but, many people with a history of NSSI do not go on to attempt suicide more than 60%. repetitive and.or severe NSSI seems to be a particularly strong predictor
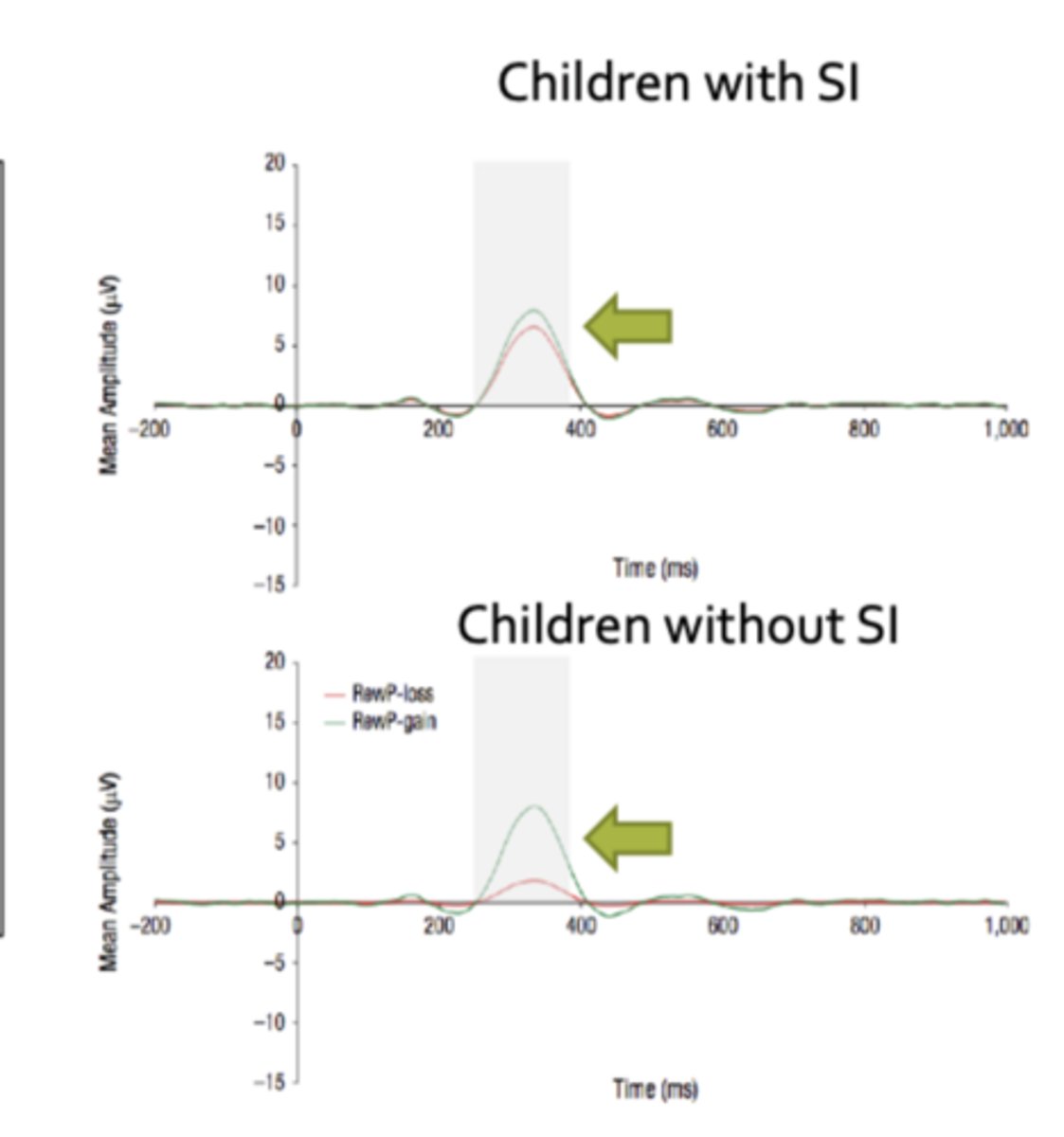
children with SI study
23 children with a history of recent suicidal ideation. 46 demographically and clinically matched children with no recent suicidal ideation. collected the RewP from participants as they completed a monetary reward task. control for current depression, anxiety and externalizing symptoms, as well as lifetime hx of mdd and anxiety disorders
experimental research methods
compare individuals responses to tasks, manipulations, etc
treatment studies research methods
randomly assign people to different conditions or treatments and compare outcomes. waitlist control, placebo, alternative treatment
meta-analysis research methods
pools results from separate but similar studies to get a more accurate estimate of the effect
late positive potential
positive is down
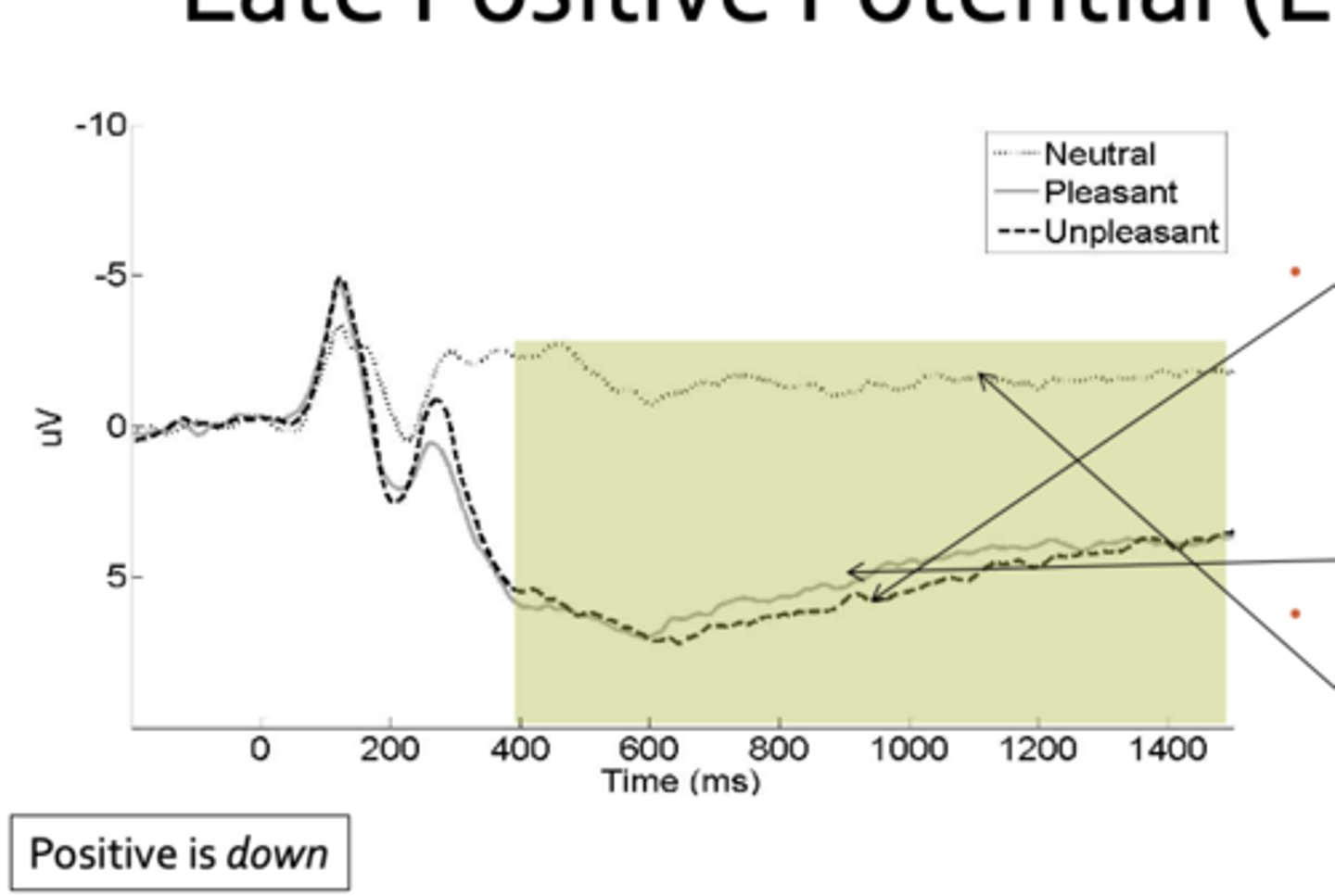
suicidal ideation study
152 outpatients all with anxiety, mdd, bipolar with no history of suicide attempts. 83 outpatients with a history of suicide attempts. control for current suicidal ideation. passive picture viewing task (threatening, gory images, eroti, affiliative images, neutral images)
NSSI in real time - when it is likely to occur
if participants had intense but brief thoughts about self-harming, they were more likely to do it. thoughts about NSSI were more likely to occur when participants were feeling overwhelmed or scared/anxious (feeling rejected, holding anger towards oneself or others, self hatred, feeling numb.nothing predicted NSSI).
function of NSSI
most common reason was to decrease/distract from negative thoughts/feelings. ppl upset right before and happier after