Peds Exam 4 Combined
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
1st degree burns: (4)
Superficial thickness: sunburns
erythema and pain 2-3 days
intact skin
no blisters
sloughs off

2nd degree burns: (3)
superficial partical thickness; epidermis and part of dermis
blisters burst/weep!!
moist/shiny
heals w/in 3 weeks

3rd degree burn s/s: (5)
white/pale tissue
huge blisters
pale dermis visible
heals w/in 3-9 weeks
may need excisions and grafts
*deep partial thickness

4th degree Full thickness burn s/s: (3)
destroys epidermis, dermis layer
may damage nerves, bones, muscle (doesnt feel any pain)
eschar visible (thick black tissue)

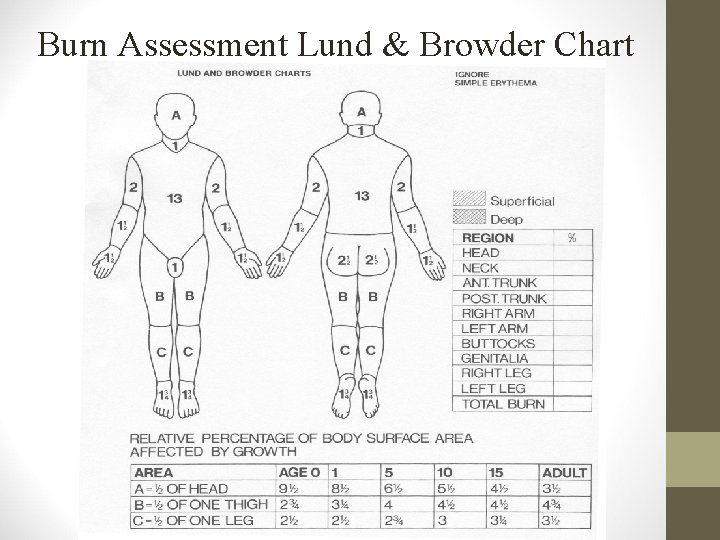
Rule of 9’s for children: (2)
Lund Brunder chart
Head is proportionally larger in children
subtract 1% from head for each yr over 1 y/o
Legs are proportionally smaller in children
add ½ % to each leg for each yr over 1 y/o
Minor burn interventions: (4)
superficial: soak in tepid water (luke warm water)
partial thickness w/ blisters: soak in tepid water
no greasy lotion, ice or butter
dont break blisters!!!
What fluids would u give major burn victim first?
Lactated Ringers!!! for first 24 hrs
has more electrolytes than NS
Priority care for major burns: (4)
Airway & ventilation!!
soot in airway
stridor
100% O2
Fluid replacement LR 1st 24 hrs
burns → hypovolemic shock
maintain urine output: 0.5-1 mL/kg/hr if child < 30kg
low output = shock and loss of fluids
Why protect airway in burns? (2)
rapid airway edema → obstruction
inhalation injury can cause pneumothorax or hypoxia
Singed nasal hairs
soot
What causes burn shock? (3)
massive edema
⬇ perfusion → organ failure!!
fluids shifts out of vessels

ideal urine output range for major burn patient?
if child weighs < 30 kg, ideal range is 0.5-1 mL/kg/hr
if child is 23 kg, pee has to be around 11-23 mL/hr
Infection prevention for Burns: (3)
aseptic dressing change 2x daily
wound cultures 2x weekly
topical antimicrobial agents
SILVER nitrate
SILVER sulfadiazine
Sylfamyoin

When are 2 nurses needed for burn care? (2)
burn injuries > 80% of body
dressing changes to face/neck of intubated child
trache care

how does impetigo begin and end?
starts as minor cuts, insect bites, broken skin around mouth/nose
sores/blisters rupture→ oozing and crusts over

Impetigo key points:
how contagious?
causes? (3)
HIGHLY contagious
will STOP being contagious after 24 hrs abx
cause: (3)
crowded areas (Schools/daycare)
climate (tropical)
poor hygiene
what causes cellulitis: (2)
s/s (4)
tx
strep, staph, after skin breaks
redness/warmth
swelling
tender
fever
tx: antibiotics

scabies cause and tx:
scabies mites, through direct contact
5% permethrin or Ivermectin cream

scabies parent education: (4)
apply 5% permethrin cream to all of body (leave overnight, wash in morning)
no home remedies
wash everything in HOT water
if cant wash, put in bag for 14 days
Pediculosis Capitis (lice) tx: (3)
1% permethrin shampoo
benzyl alcohol
comb through hair daily for nits
can take months
boil brushes

Diaper dermatitis causes (3)
tx (barrier, antifungals, severe)
causes:
urine/feces friction
irritants: detergents
candida albicans (yeast infections)
long term use of abx
tx:
zinc oxide (barrier)
antifungals (nystatin, clotrimazole)
severe→ hydrocortisone

atopic dermatitis (eczema) tx: (3)
hydrate skin (non scented)
tepid baths
fragrance free lotion

DM labs if diabetic: (4)
8 hr fasting glucose will be >120 mg/dL
random blood glucose will be > 200mg/dL
oral tolerance is >200 mg/dL
HgA1c is >6.5%
okay range: 6.5%-8% in children
over a 3 month period
Hypo/Hyperglycemia glucose level:
< 60mg/dL hypo
>250 mg/dL hyper
hypoglycemia signs: (10)
hunger
shaky/dizziness
pallor
diaphoresis
tachycardia/palpitations
tremors
slurred speech
shallow respirations
blurred vision
⬇LOC (lethargic→ comas)

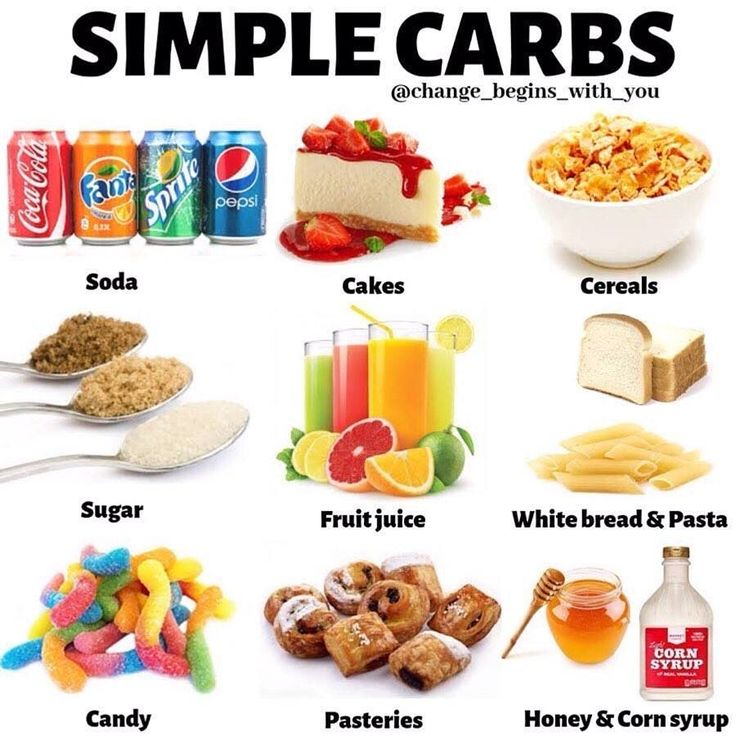
hypoglycemia management: (3)
give 10-15 g simple carbs (1 TBsp sugar)
4 oz OJ
4 oz regular soft drink
8 oz milk
2-3 glucose tablets
re-check glucose after 15 mins
follow with complex carbs
PB crackers
turkey club sandwich
cheese and crackers
if child is unconscious/cant swallow in hypoglycemic episode, what do u do?
admin IM glucagon!!!
then give simple carbs if tolerated
watch vomiting
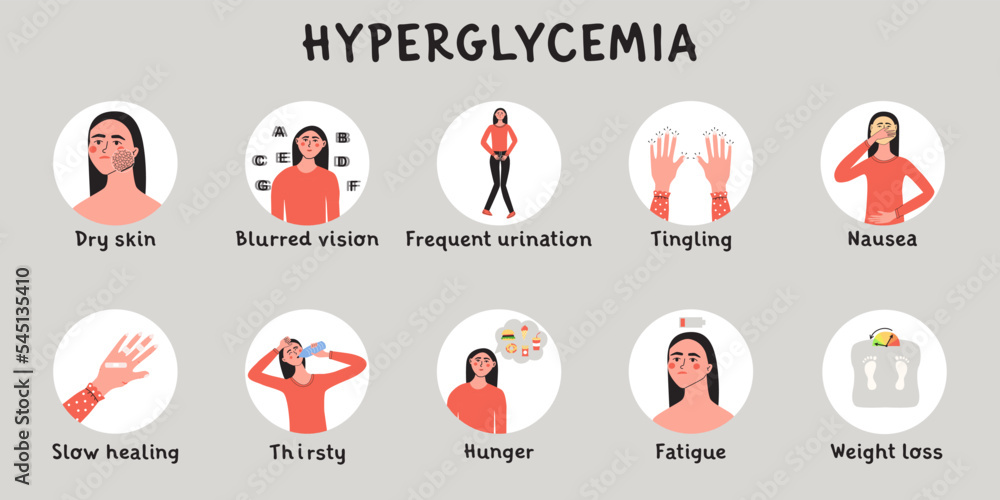
hyperglycemia s/s: (8)
poly-uria, dipsia, phagia
rapid, deep breathing & acetone/fruity odor & positive ketones (Kussmauls)
oliguria (later)
recurrent yeast infx (means early T2 DM)
warm, dry, flushed skin
dry mucous membranes
weak pulse
⬇DTR
hyperglycemia management: (3)
"DRY”
Dehydrated: oral fluids
Raise insulin: give rapid acting (Lispro)
You monitor ketones, K+

DM personal hygiene: (6)
NO wearing sandals
NO being barefoot outside
Wear shoes with socks
clean any cut w/ warm water, mild soap & dry dressing
examine child’s eye yearly
regular dental care

children playing sports snack times: (2)
teams sports: 30 mins before activity
prolonged sports (running): need food every 45-60 mins

Management for SICK child with diabetes: (3)
monitor blood glucose & ketones in pee q3 hrs
bad: glucose >250 mg/dL; positive ketones
sugar-free, non caffeinated drinks (keep hydrated)
eat soft carbs (rice, mashed potatoes, pasta, bread)

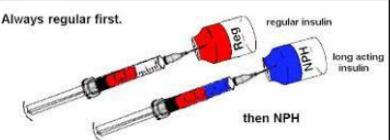
Educate families on insulin: (4)
rotate site for every 4-6 injections
90 degree angle
mixing: short acting 1st, then longer acting 2nd (clear then cloudy)
boluses can be given b4 meals
Rapid insulin
name
onset
peak
duration
Lispro
onset: 15-30 mins
peak: 30 min-3 hrs
duration: 3-5hrs
Short insulin
name
onset
peak
duration
Regular
onset: 30 mins-1hr
peak: 1-5 hrs
duration: 6-10 hrs
Intermediate insulin
name
onset
peak
duration
NPH
onset: 1-2 hrs
peak: 4-14 hrs
duration: 14-24 hrs
Long insulin
name
onset
peak
duration
Glargine
onset: 1-4 hrs
peak: NONE
duration: 24 hrs
DKA glucose level:
what happend in DKA?
> 330 mg/dL
pH 7.3 (acidic)
bicarbonate < 15
yikes
→ body burns fat (turns into ketones) instead of glucose
DKA hallmark signs: (3)
fruity breath
ketones in pee
rapid deep respirations
Electrolyte to monitor in DKA:
potassium!!
initially high → give insulin
drops (hypok+)
monitor K+ bc correcting acidosis too fast→ hypoK
give sodium bicarb if severe acidosis (blood pH <7)
give O2 to children whose cyanotic and < 80%
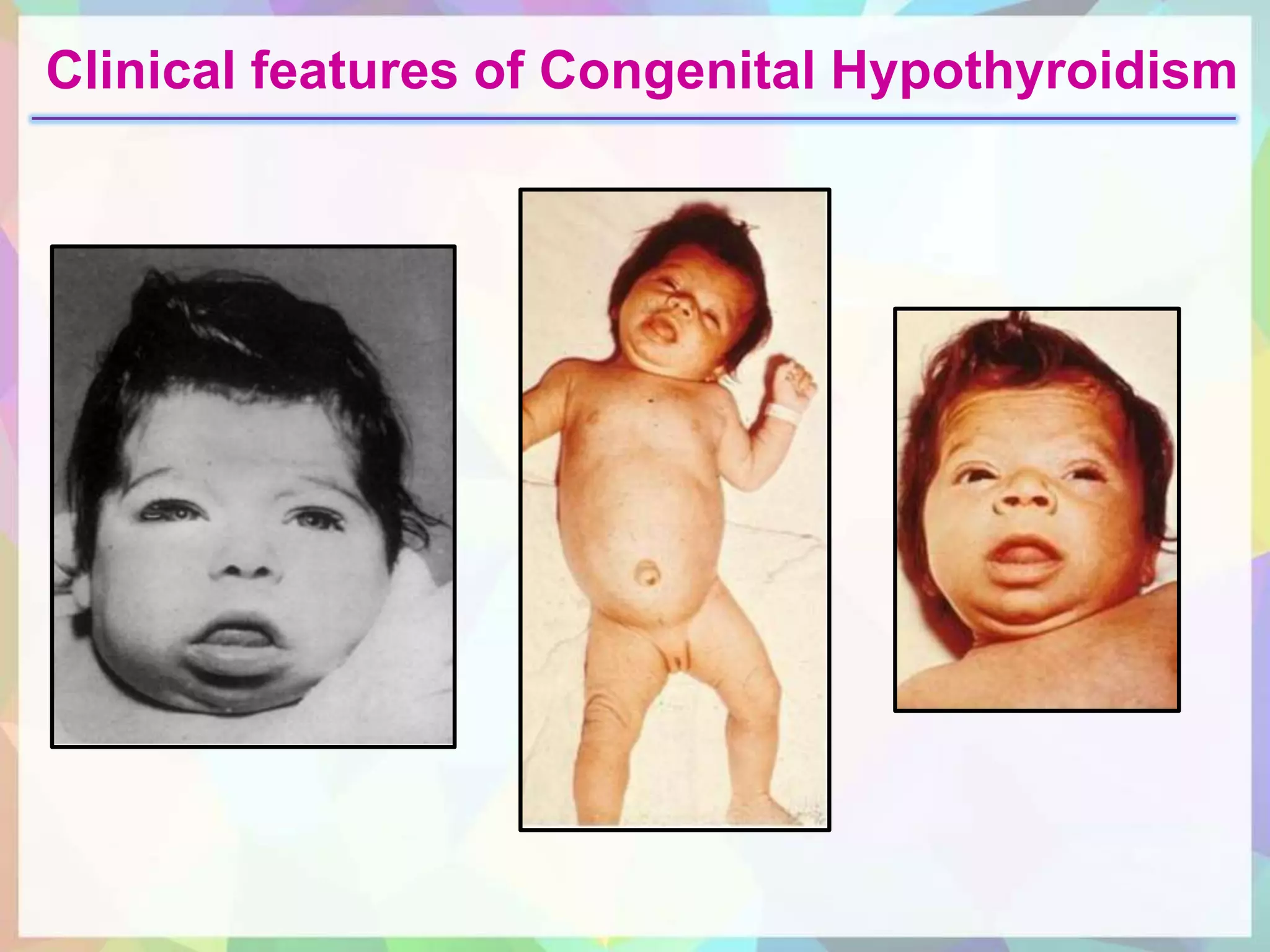
congenital hypothyroidism s/s? (7)
short, thick neck
hypotonia w/ ⬇reflexes
jaundice
enlarged tongue (macroglossia)
sleep alot
poor sucking
abd distention/constriction
baby born w/ low TH levels
nurse care for congenital hypothyroidism: (4)
give synthetic TH (levothyroxine)
give vitamin D (supports bone growth and development)
monitor TH levels (T3,T4, TSH), weight, resp status
monitor feeding
what does it mean for mom if she tests positive for PKU?
what happens if she doesnt follow?
strict diet from 3 months b4 conception throughout pregnancy
if dont follow→ baby retardation
microcephaly
cognitive impairment
heart defects
PKU signs: (5)
musty odor pee
microcephaly
blue eyes & very fair skin w/ light blonde hair
FTT
heart defects

PKU screening requirements: (3)
normal level: phenylalanine 0.5-1 mg/dL
repeat screen @ 1-2 weeks
newborn metabolic screen w/in 2 days of birth
PKU dietary restrictions: (5)
NO high PKU foods: eggs, meat, milk/yogurt, soy products, beans (no high protein)
EAT fruits/veggies, low protein grains (bread, pasta, rice)
initiate regimen ASAP or w/in 7-10 days of birth
formula low in PKU
can breastfeed in moderation
contains protein
whats the intake of PKU/ kg of body weight/day:
whats the ideal PKU level for PKU pts?
limit intake to 20-30 mg PKU/kg of body weight/day
PKU level for PKU pts: < 8mg/dL ideal
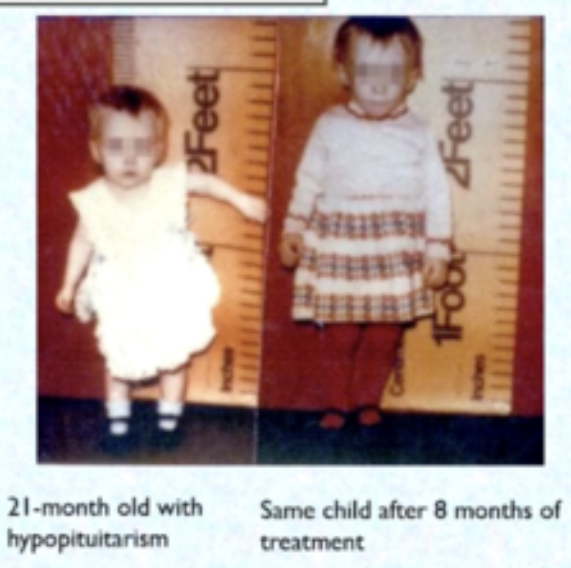
Whats growth hormone deficiency?
Hypopituitarism
low secretion of pituitary hormone
signs of Hypopituitarism: (4)
short stature but proportional
child is shorter than expected for their age, but their body proportions are normal
delayed epiphyseal closure
growth plates at the ends of long bones stay “open” longer than usual
⬆insulin sensitivity
body responds more strongly to insulin, meaning blood sugar is used efficiently
delayed dentition, jaw, sexual development
Teeth come in later than normal
Jaw growth may be slower
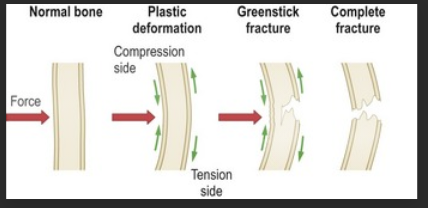
What are common peds fractures? (3)
greenstick: incomplete fracture
plastic deformation: bone bent no more than 45 degrees and doesnt break
buckle (torus): one side bulges (like dent)
Risk factors for peds fractures? (4)
obese
bad nutrition
low calcium/vitamin D (milk and sun)
developmental stage
learns to walk
normal play
falls
sports

s/s of fractures: (5)
edema
crepitus
deformed
ecchymosis
wont use limb
nurse care for fractures: (6)
immobilize (splints)
elevate to decrease swells
ice first 24 hrs
look for shock
take stuff off (bracelets etc)
monitor fat embolism s/s (SOB, petechiae)
compartment syndrome causes: (5)
tight cast/dressing
skin traction
trauma
burns
IV infiltration
→ due to ⬆pressure in muscle and cuts off blood flow (ischemia)
signs of compartment syndrome: (6)
6 P’s
pulselessness
pain
pallor
paresthesia
paralysis
poikilothermia
body can’t regulate temp → matches environment
nurse interventions for compartment syndrome (3)
check limb q4hrs for 1st 24 hrs
make sure 1 finger fits under cast
loosen tight dressings
osteomyelitis signs: (5)
edema
pain ⬆w/ mvmt
wont use limb
tender/warm to touch
fever/irritablility/tachycardic
infx of bone d/t fractures etc
pt education abt osteomyelitis: (5)
watch for ototoxicity!! (side effect of abx)
limit mvmt duh..
proper nutrition (high protein+cals→ tissue healing and immunity)
no weight bearing stuff
finish long term abx treatment
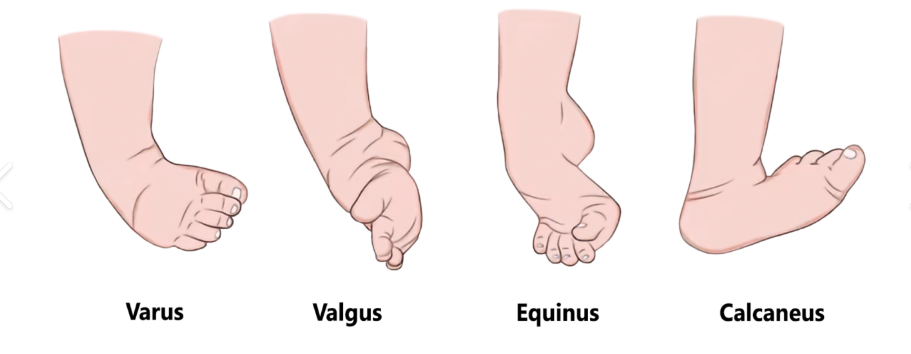
Clubfoot (talipes equinovarus) findings: (4)
affected foot shorter + smaller w/ empty heel pad
visible plantar crease
calf atrophy
unilateral deformity

types of clubfoot: (4)
talipes varus: inversion
talipes valgus: eversion
talipes calcaneus: dorsiflexion
talipes equinus: plantar flexion
nurse care clubfoot: (3)
parents hold/cuddle baby
do neurovascular checks and skin integrity checks (redness/blisters)
6 p’s
cast care
keep dry
dont shove anything in it
no scratching
regular cast changes
proper cast care: (8)
keep it dry (water weakens it→ skin irritation/bateria)
cover in plastic when showering
no lotions/powders
no inserting objects in cast
check circulation in fingers and toes
elevate limb and ice it
turn q2 hrs
soak limb in warm water after removal
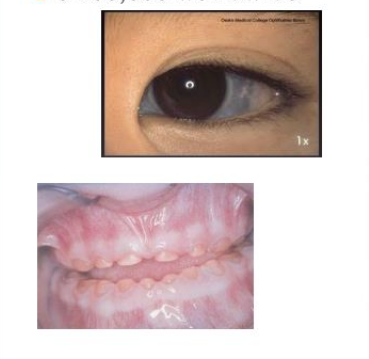
whats osteogenesis imperfecta?
s/s: (4)
“brittle bone disease”
multiple bone fracture
blue sclera
early hearing loss
small, discolored teeth
Osteomyelitis imperfecta education: (6)
oral care (soft toothbrush)
fix positions frequently
dont pull them
prevents contractures
help w/ braces and splints
NO LIVE vax
monitor heart and dysrhythmias!!
meds: bisphosphonates→ strengthens bones
adverse effects of biphosphorous: (8)
hypoK+
hypoMag+
hypoCa+
hypoP+
thrombocytopenia
neutropenia (so no live vax)
dysrhythmias (bc of electrolytes)
kidney failure
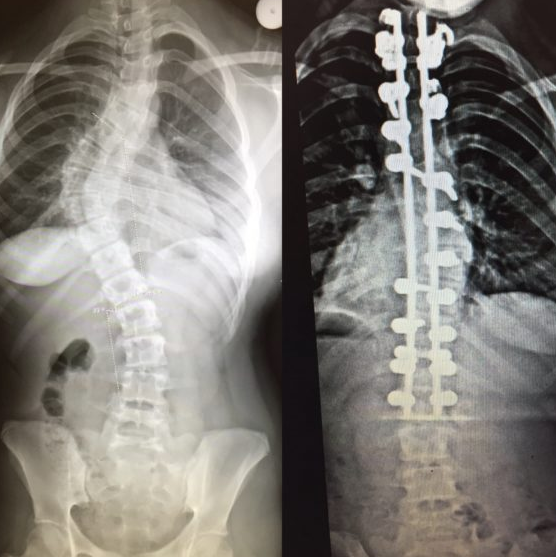
scoliosis findings: (3)
asymmetry in scapula, ribs, flanks, shoulder, hips
bad fitting clothes (one leg shorter than other)
more common in females (8-15 y/o)

scoliosis tx: (2)
bracing: slows curvature
surgery: spinal fusion w/ rod placement if severe (>45 degrees)
what could be complications of scoliosis? (3)
and post op complications? (6)
breathing difficulties
can compress lungs
low self esteem
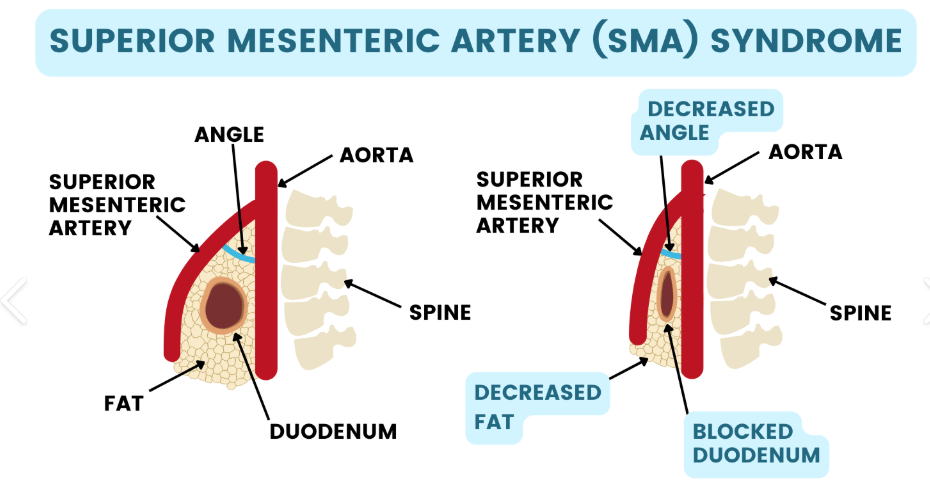
superior mesenteric artery syndrome
compression of the duodenum by the aorta and superior mesenteric artery, leading to obstruction.
“squeezes intestines”
postop complications: (6)
Spinal cord or neuro injury
Pneumothorax (decreased mobility)
Atelectasis (decreased mobility)
Ileus (decreased mobility)
Hypotension (blood loss)
Infection (wound)
scoliosis pt pre and post op teachings:
pre (3)
post (5)
pre op:
teach respiratory techniques: IS, turning, coughing, deep breathing to prevent complications.
teach PCA pump use
inform pt abt autologous (self-donated) blood donations if blood loss happens during surgery
post op:
go to PT (ROM)
log rolling
roll pt like log so spine stays aligned
keep favorite things w/in reach (helps them be independent)
ambulate on 2nd-3rd day post op
check for pressure ulcers