Chest X-ray
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
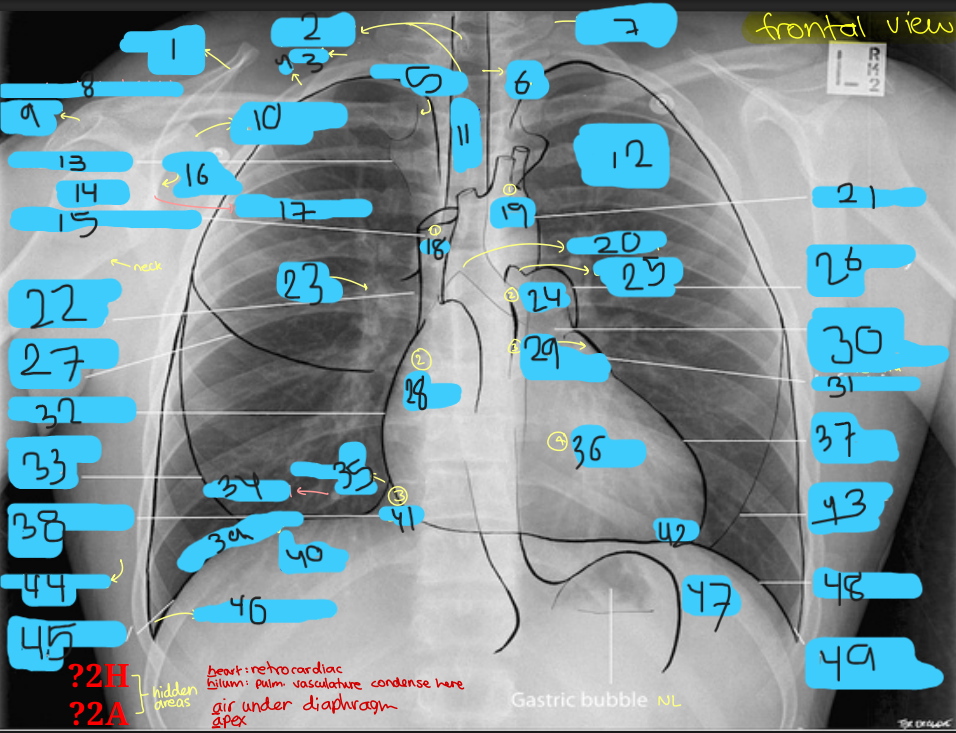
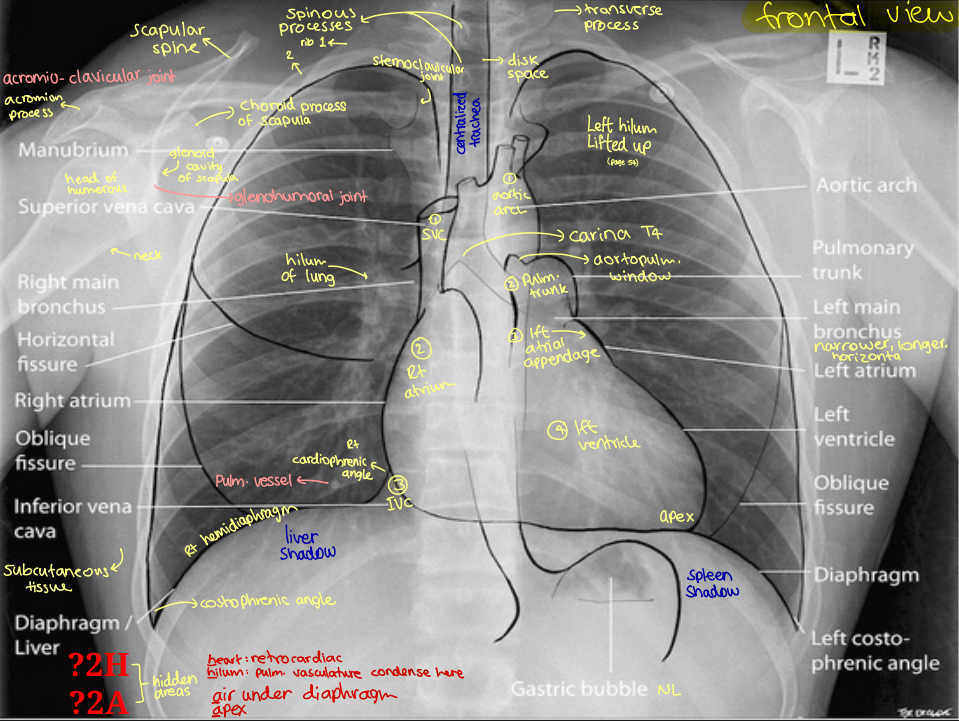
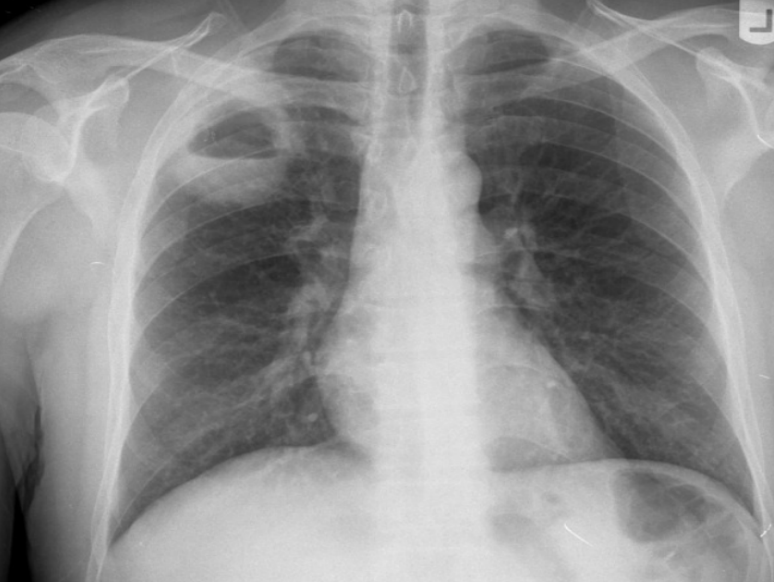
Heart right border
Right atrium
Superior vena cava entering superiorly
Inferior vena cava often seen at its lower margin
Heart left border
Left ventricle and left atrial appendage
The pulmonary artery
Aortopulmonary window
Aortic notch extend superiorly.

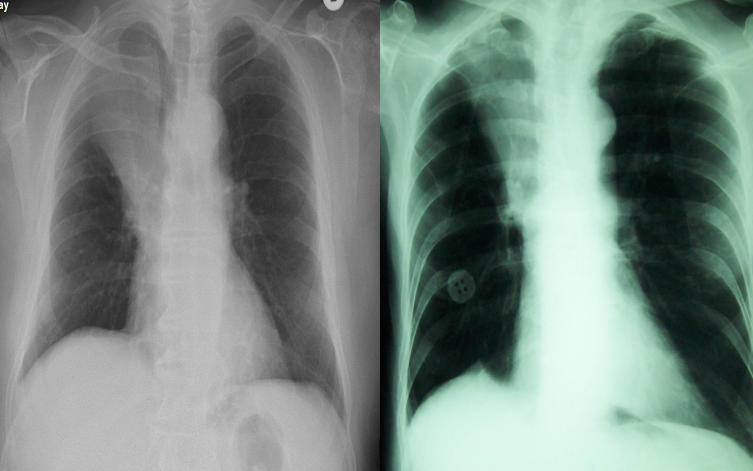
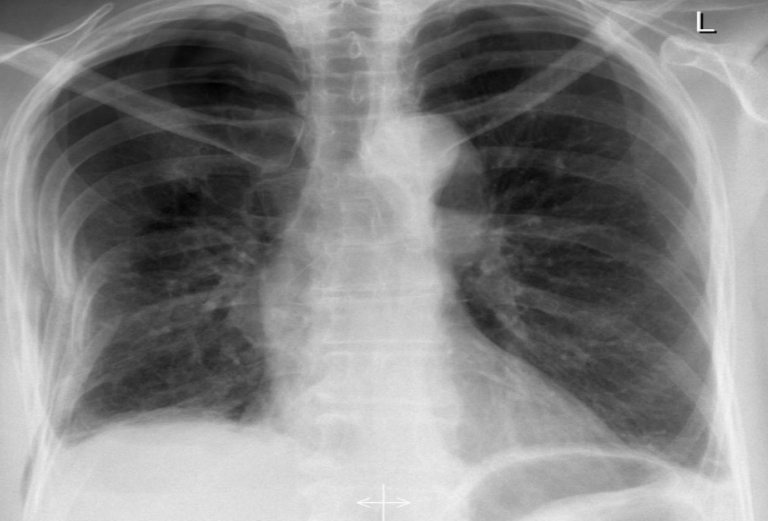
What view
PA (lower diapjragm, full lungs/large, horizontally oriented clavicales, scapula not displaced)
what view
AP (higher diapjragm, smaller lungs, obliquely oriented clavicales, scapula displaced, falsely enlarged heart and medastinum)

Overexposed (can be confused with COPD patients)

underexposed

underexposed
trachea divaiated to the right due to rotation.
distance between clavical and spinuss process not equal on both sides. rotated to the left.
Left hilum higher than right (NL)
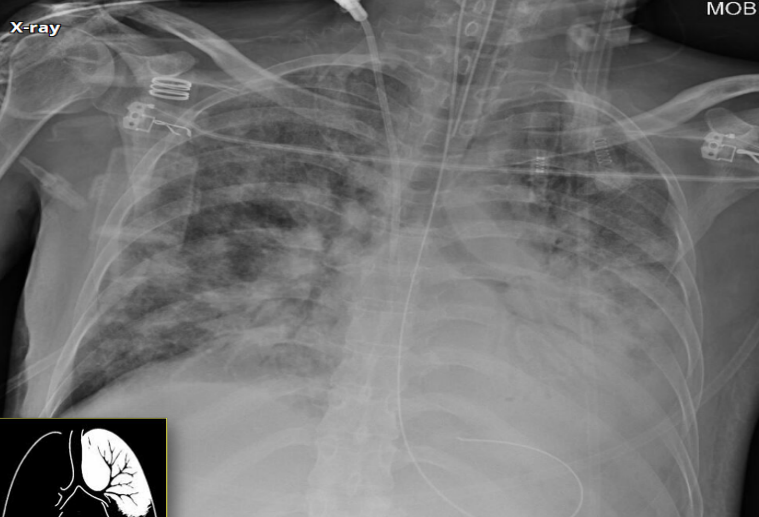
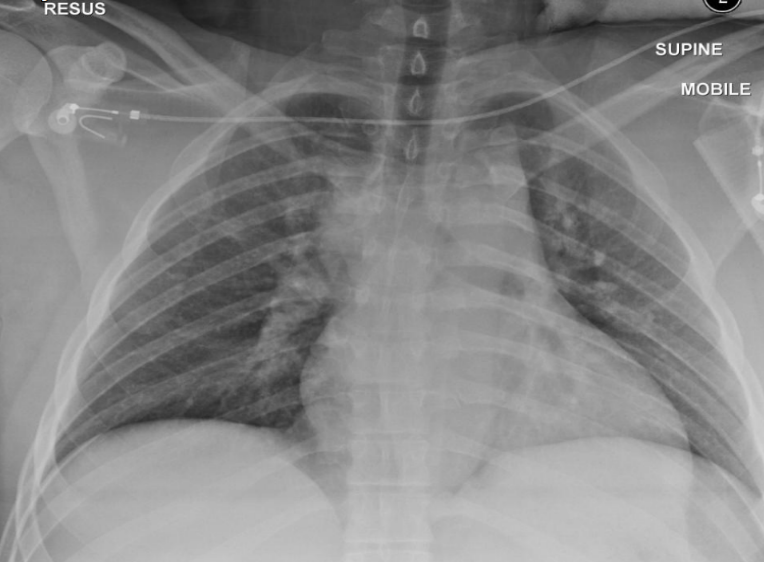
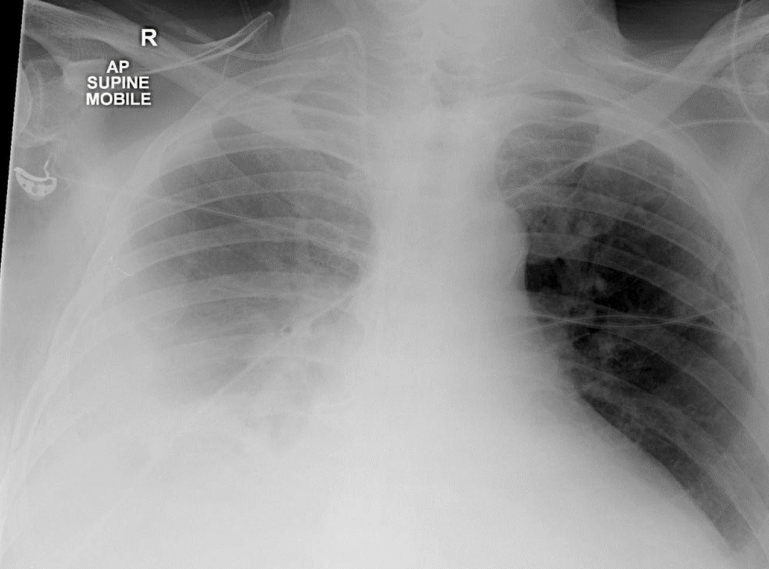
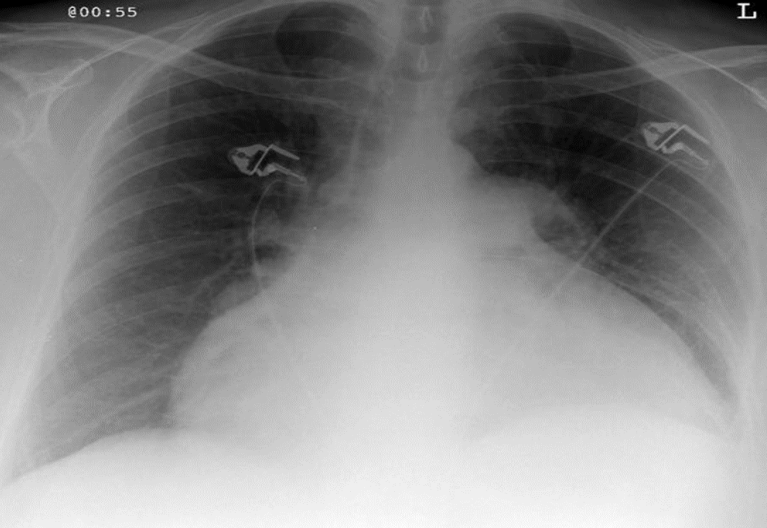
AP chest X-ray (critically ill patient and intubated)
tracheal intubation (above the carnia. if lower it will inter right main stem bronchous→leads ti left lung collaps)
NG tube
Central line (into SVC)
left main stem bronchous showing radio-opacity and patent bronchioles→Air broncho-grams (if localised→indicates infectious process)
Bilateral diffuse lung opacities on both lung fields (slightly more on left side)
Ddx: ARDs, decomensated heart failure, aspiration
Air bronchograms
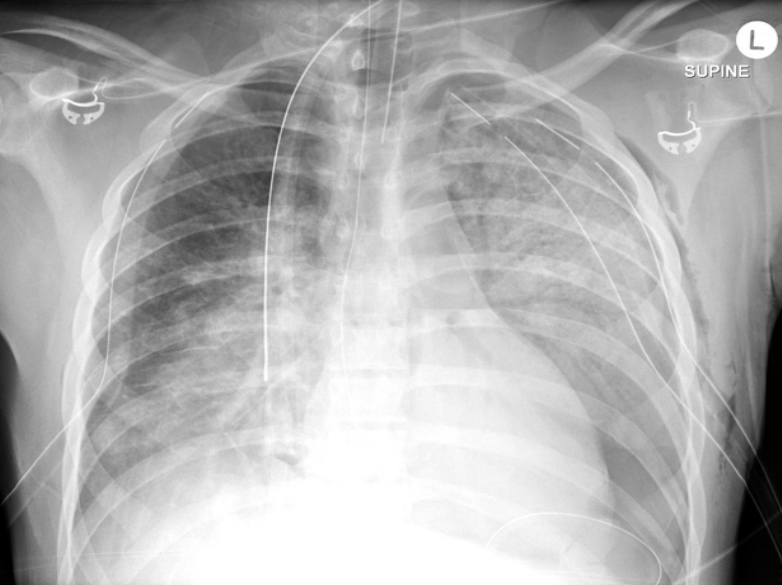
AP chest X-ray
chest tube
tracheal tube
NG tube
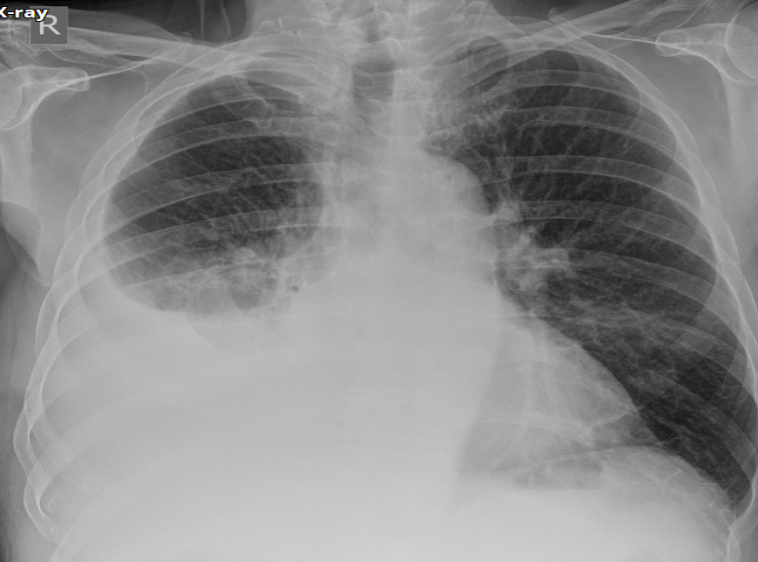
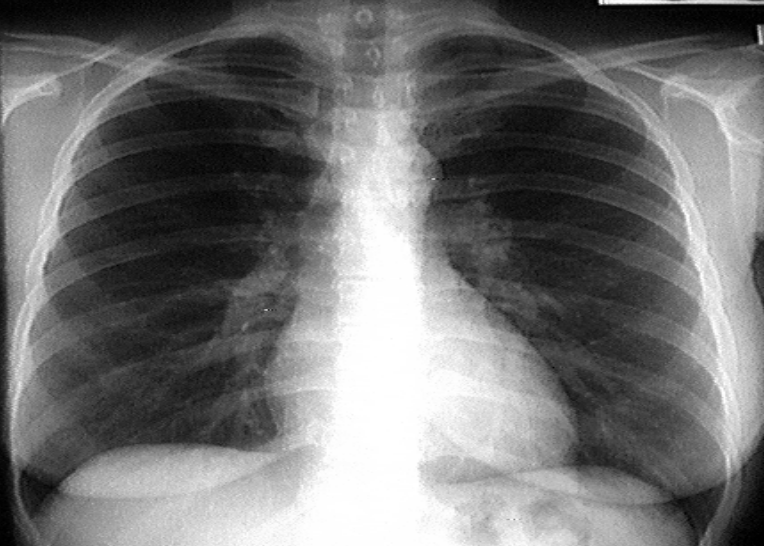
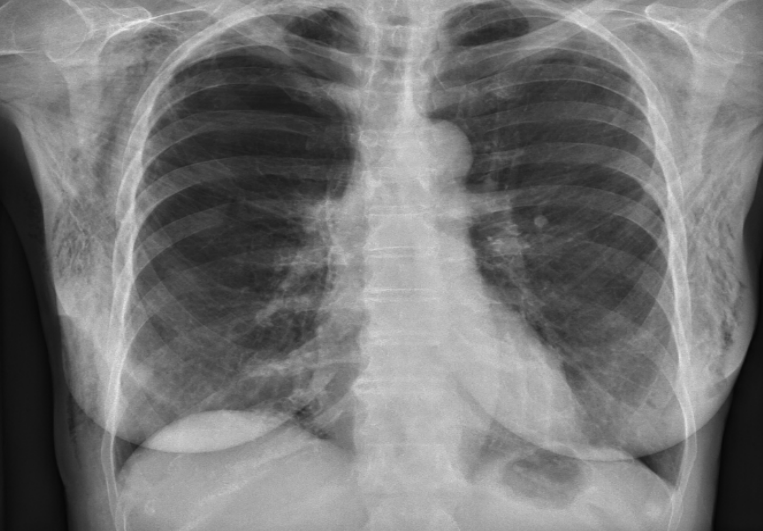
PA chest X-ray
Opacity on right side
Miniscus sign (indicates pleural effusion in PA view)
AP chest X-ray
Opacity on right side
Grading sign (indicates pleural effusion in AP view)

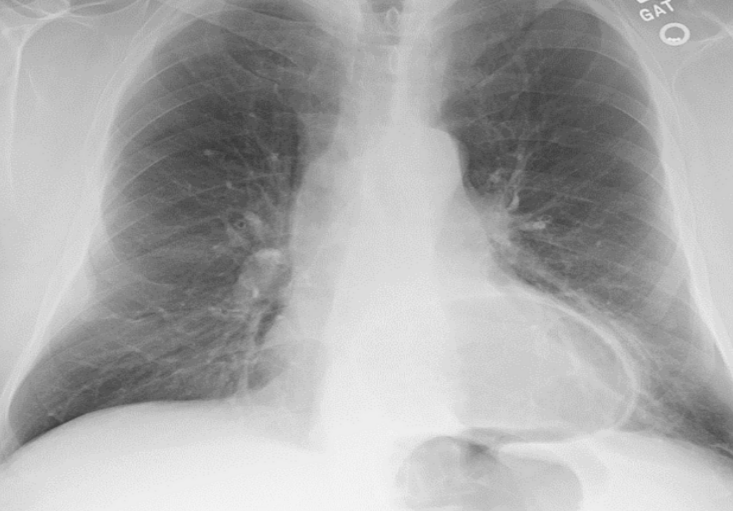
PA chest X ray
left lung lucency
veceral pleural line visible on left side
no tracheal divation and centralised mediastinum →so left sided simple pneumothorax
CP angle obliterated on left and no miniscus sign→air fluid leveling→pleural effusion on left side.
Left sided hydropneumothorax
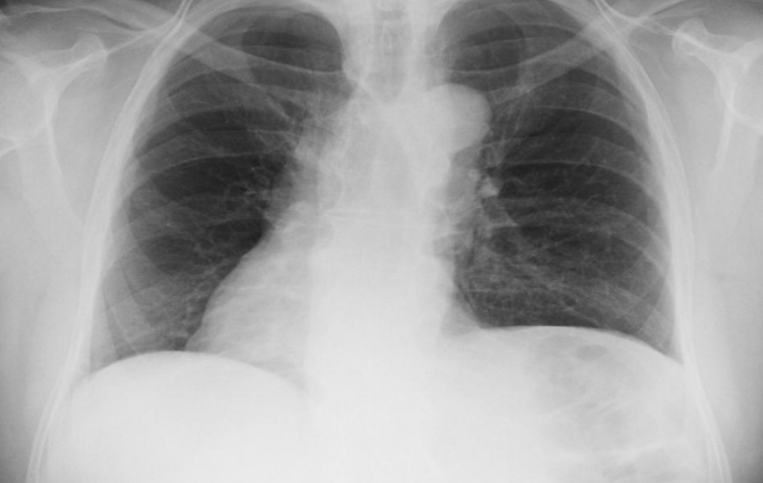
radio-opacity on right upper lung zone
right hilum lifted upward
trachea divated to ipsilateral side (to the right)
Ddx: atelectasis/lung collapse, lung fibrosis, iatrogenic (lobectomy)
sharp line of demarcation of right upper lobe opacity (everything below is normal)→right upper LOBE collapse
causes of collapse→anything obstructing rught upper lobe bronchous; tumor, mucus blood.
tinted right hemidiaphragm (can also be seen in upper lobe collapse)
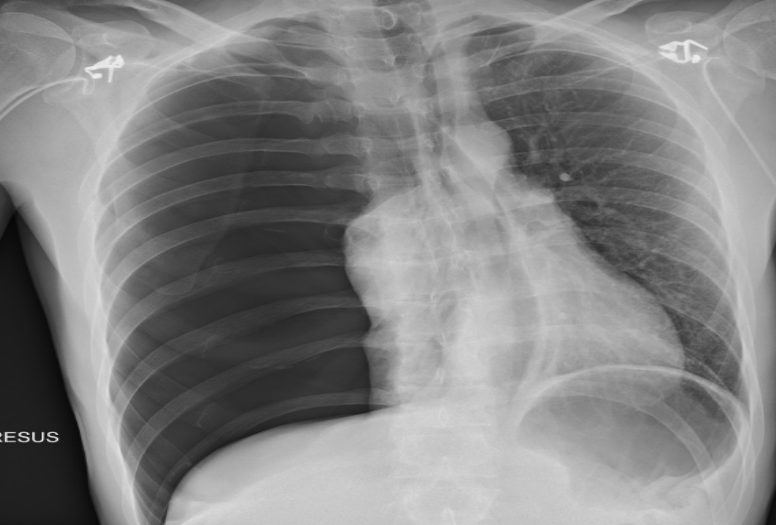
right side peunothorax
tracheal deviation to left
compresed/shifted heart
absent vasculature on right
Rught lung abcess (apperse well defined radio-opaque with air fluid level)

Right middle lobe pneumonia
pulmonary infeltrat
radio-opacity (air bronchograms)
Silhouette sign→loss of sharp border of the heart (on the right for this picture)

Right lower lobe pneumonia
Silhouette sign with right diaphragm (loss of sgarm border of right diaphragm)
dextrocardia
important to look at past patient imaging and rest of organs to check for dextro totalis

Lung mets (RCC mc cause)
variable in size, well defined, radio-opacities, diffuse, bilateral
Canonball appearance
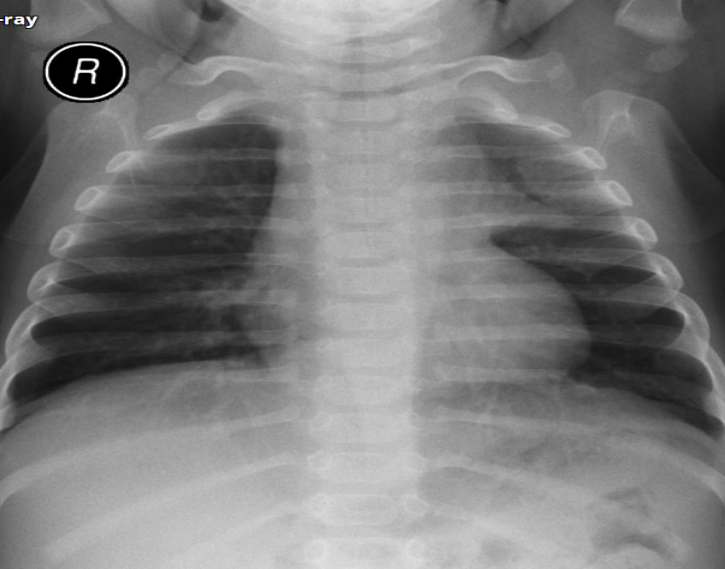
Peds patient
Sail sign (indicates thymus gland)
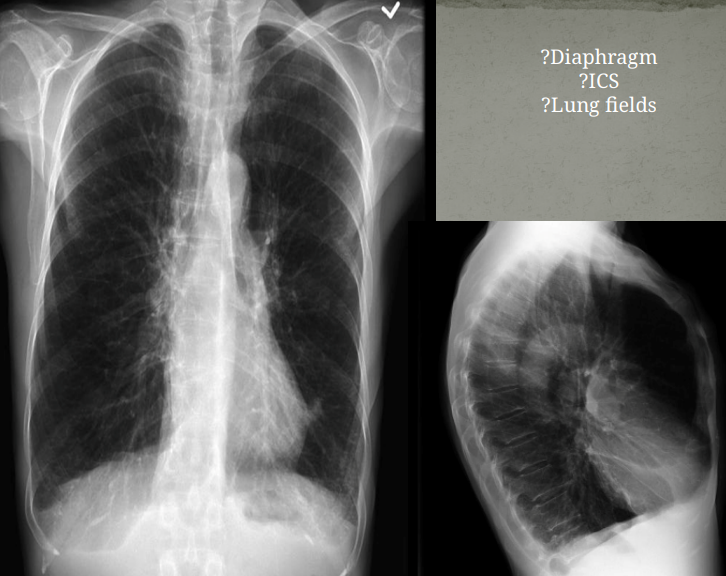
COPD patient
diaphragm flat
barrel chest on lateral view (AP diameter increase)
widened intercostal spaces
lungs hypper enflated→globular heart
Hidden area showing hiatal hernia
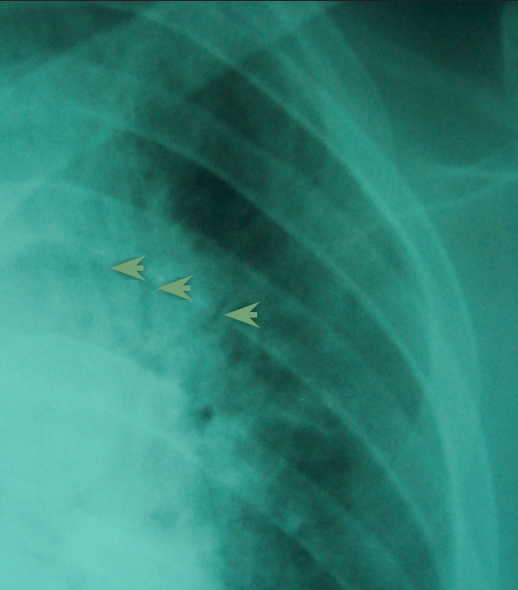
RTA patient with multiple rib fractures
discontinuity in ribs
multiple right sided rib fracture
subtle simple apical pneumothorax on right side
hemothrax in CP angle on right side
(rib fracture can be complicated by pneumothorax or hemothorax so always check)
cardiomegaly
AP chest X ray and yet heart is still grossly enlarged
subcutaneous emphysema
radio-lucency in subcutanous planes showing/enhancing the pectoralis major fibers