COPD
0.0(0)
Studied by 5 peopleCard Sorting
1/118
Earn XP
Description and Tags
Last updated 8:02 PM on 4/1/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
119 Terms
1
New cards
Disease State of COPD
A common, preventable, treatable disease
2
New cards
COPD
Persistent respiratory symptoms and airflow limitation
3
New cards
COPD Cause
* Due to airway and/or alveolar abnormalities
* Usually caused by significant exposure to noxious particles or gases
* Usually caused by significant exposure to noxious particles or gases
4
New cards
COPD Modifiable Risk Factors
* Cigarette smoke
* Occupational dust and chemicals
* Environmental tobacco smoke (ETS)
* Indoor and outdoor air pollution
* Infections
* Occupational dust and chemicals
* Environmental tobacco smoke (ETS)
* Indoor and outdoor air pollution
* Infections
5
New cards
COPD Non-Modifiable Risk Factors
* Genes
* __**Socio-economic status**__
* Aging Populations
* __**Socio-economic status**__
* Aging Populations
6
New cards
COPD Pathology
* Chronic inflammation
* Structural changes
* Emphysema
* Structural changes
* Emphysema
7
New cards
COPD Pathogenesis
* Oxidative stress
* Protease - antiprotease imbalance
* Inflammatory cells
* Inflammatory mediators
* Peribronchiolar and interstitial fibrosis
* Protease - antiprotease imbalance
* Inflammatory cells
* Inflammatory mediators
* Peribronchiolar and interstitial fibrosis
8
New cards
COPD Pathophysiology
* Airflow limitation and gas trapping
* Gas exchange abnormalities
* Mucus hypersecretion
* Pulmonary hypertension
* Gas exchange abnormalities
* Mucus hypersecretion
* Pulmonary hypertension
9
New cards
COPD Symptoms
* Shortness of breath
* Chronic cough
* Sputum
* Saliva + mucus coughed up from respiratory tract
* Chronic cough
* Sputum
* Saliva + mucus coughed up from respiratory tract
10
New cards
COPD Diagnosis
* Spirometry results:
* ↓ FEV1 (Forced Expiratory Volume in the 1st second)
* ↓ FEV1/FVC (Forced Vital Capacity) ratio
* These results mean:
* Impaired gas exchange
* Not fully reversible
* ↓ FEV1 (Forced Expiratory Volume in the 1st second)
* ↓ FEV1/FVC (Forced Vital Capacity) ratio
* These results mean:
* Impaired gas exchange
* Not fully reversible
11
New cards
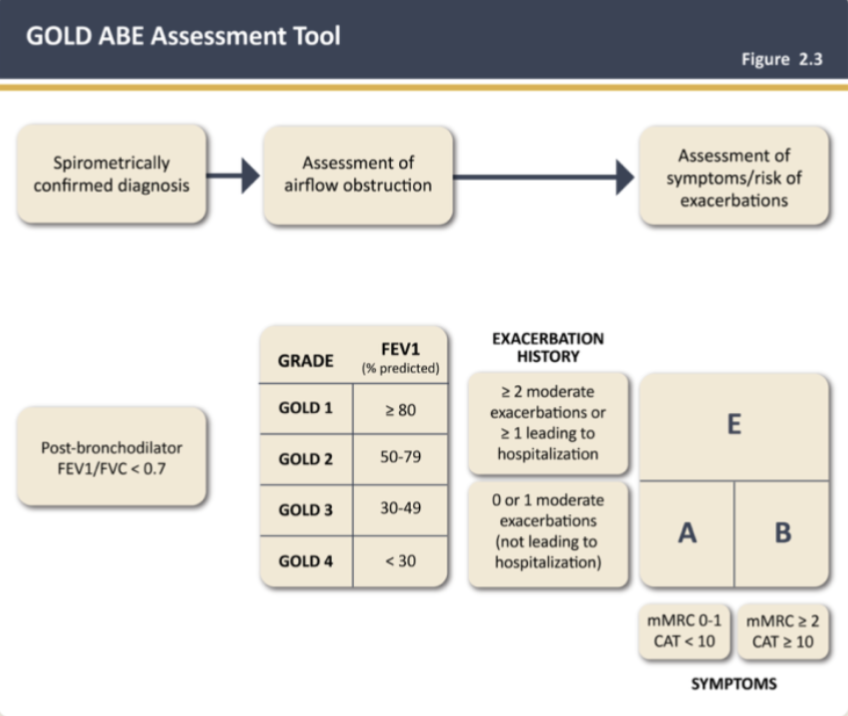
Classification of Airflow Limitation Severity in COPD (Based on Post-Bronchodilator FEV1)
In patients with FEV1/FVC < 0.70
* Gold 1
* Gold 2
* Gold 3
* Gold 4
* Gold 1
* Gold 2
* Gold 3
* Gold 4
12
New cards
Classification of Severity of Airflow Limitation: Gold 1
* Mild
* FEV1 ≥ 80% predicted
* FEV1 ≥ 80% predicted
13
New cards
Classification of Severity of Airflow Limitation: Gold 2
* Moderate
* 50% ≤ FEV1 < 80% predicted
* 50% ≤ FEV1 < 80% predicted
14
New cards
Classification of Severity of Airflow Limitation: Gold 3
* Severe
* 30% ≤ FEV1 < 50% predicted
* 30% ≤ FEV1 < 50% predicted
15
New cards
Classification of Severity of Airflow Limitation: Gold 4
* Very severe
* FEV1 < 30% predicted
* FEV1 < 30% predicted
16
New cards
COPD: Assessment of Symptoms
* __**COPD Assessment Test (CAT)**__
* An 8-item measure of health status impairment in COPD
* __**Modified Medical Research Council (mMRC) Questionnaire**__
* Relates well to other measures of health status and predicts future mortality risk
* An 8-item measure of health status impairment in COPD
* __**Modified Medical Research Council (mMRC) Questionnaire**__
* Relates well to other measures of health status and predicts future mortality risk
17
New cards
GOLD ABE Assessment Tool
* __**Group A and B**__: 0 or 1 moderate exacerbations (not leading to hospitalization)
* __**Groups E**__: ≥ 2 moderate exacerbations or ≥ 1 leading to hospitalization
* __**Groups E**__: ≥ 2 moderate exacerbations or ≥ 1 leading to hospitalization
18
New cards
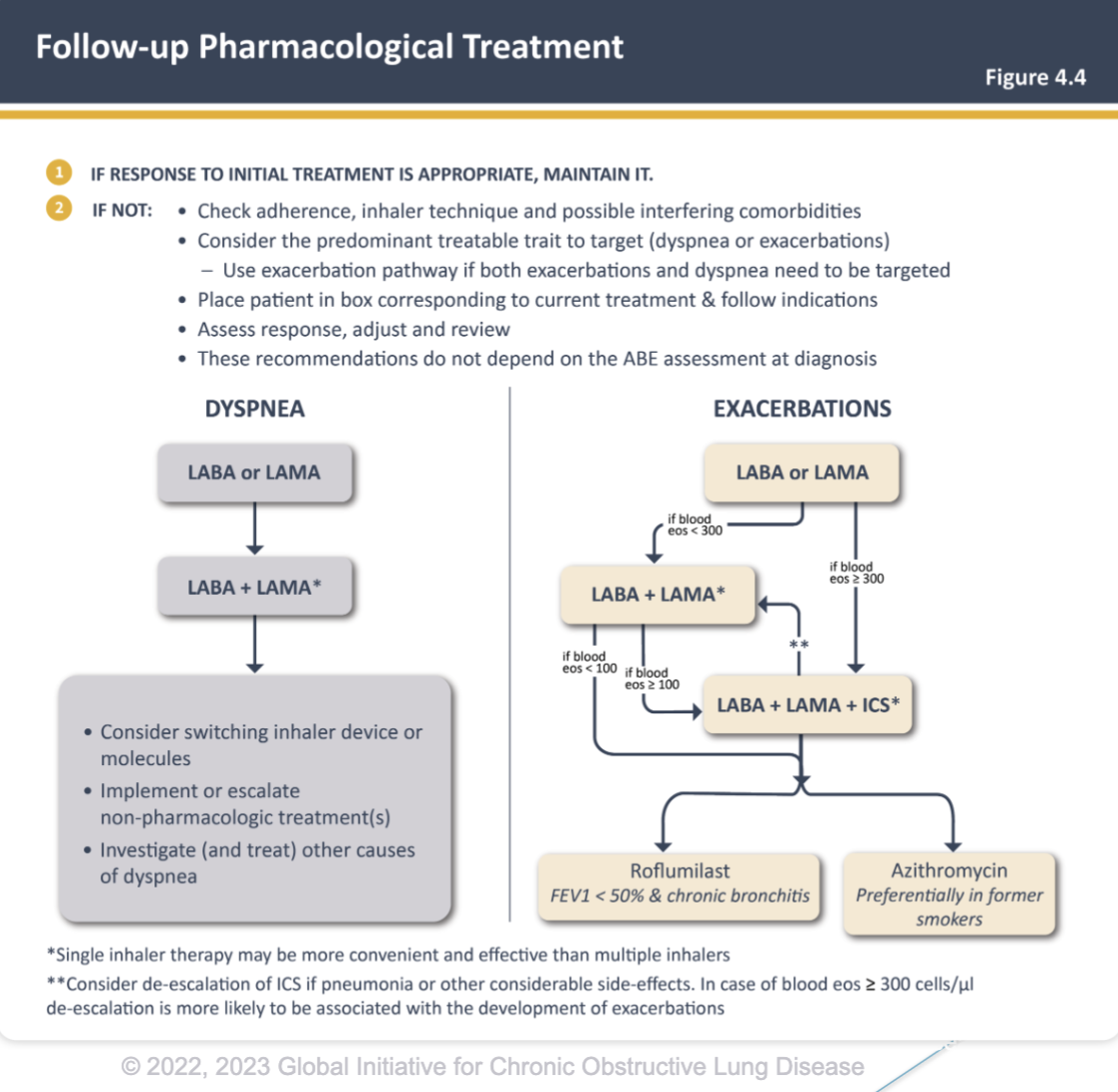
Treatment of Stable COPD: Group E Treatment
* LABA + LAMA
* Single inhaler therapy may be more convenient and effective than multiple inhaler
* Consider LABA + LAMA + ICS __**if blood eosinophil ≥ 300**__
* In patients that also have asthma, they should be treated appropriately, thus ICS is recommended
* Single inhaler therapy may be more convenient and effective than multiple inhaler
* Consider LABA + LAMA + ICS __**if blood eosinophil ≥ 300**__
* In patients that also have asthma, they should be treated appropriately, thus ICS is recommended
19
New cards
Treatment of Stable COPD: Group A Treatment
* Bronchodilator
* Short or long-acting
* Short or long-acting
20
New cards
Treatment of Stable COPD: Group B Treatment
* LABA + LAMA, if no barriers
* Single inhaler therapy may be more convenient and effective than multiple inhaler
* Neither class (LABA or LAMA) is preferred over the other for monotherapy if combination therapy isn’t appropriate
* Long-acting inhaledbronchodilators are superior to short-acting bronchodilators taken as needed
* i.e., pro re nata (prn) and are therefore recommended
* Single inhaler therapy may be more convenient and effective than multiple inhaler
* Neither class (LABA or LAMA) is preferred over the other for monotherapy if combination therapy isn’t appropriate
* Long-acting inhaledbronchodilators are superior to short-acting bronchodilators taken as needed
* i.e., pro re nata (prn) and are therefore recommended
21
New cards
22
New cards
Management of Stable COPD: Goals of Therapy
* Reduce symptoms
* Reduce risk
* Reduce risk
23
New cards
COPD Goals of Therapy: Reduce Symptoms
* Relieve symptoms
* Improve exercise tolerance
* Improve health status
* Improve exercise tolerance
* Improve health status
24
New cards
COPD Goals of Therapy: Reduce Risk
* Prevent disease progression
* Prevent and treat exacerbations
* Reduce mortality
* Prevent and treat exacerbations
* Reduce mortality
25
New cards
Management for Stable COPD
* Smoking Cessation
* Vaccinations
* Vaccinations
26
New cards
Management for Stable COPD: Smoking Cessation
* __**Greatest capacity to influence natural history of COPD**__
* Slows/halts COPD progression
* Strategies to help:
* 5 A’s
* Ask
* Advice
* Assess
* Assist
* Arrange
* Slows/halts COPD progression
* Strategies to help:
* 5 A’s
* Ask
* Advice
* Assess
* Assist
* Arrange
27
New cards
Management for Stable COPD: Vaccinations
* Influenza vaccination can reduce serious illness and death in COPD patients
* COVID-19 vaccination recommended for all people with COPD
* Pneumococcal vaccinations, PCV13 andPPSV23, are recommended for all patients >65 years of age
* CDC recommends Tdap vaccination in those who weren’t vaccinated in adolescence and Zoster vaccine to protect against shingles for adults with COPD > 50
* COVID-19 vaccination recommended for all people with COPD
* Pneumococcal vaccinations, PCV13 andPPSV23, are recommended for all patients >65 years of age
* CDC recommends Tdap vaccination in those who weren’t vaccinated in adolescence and Zoster vaccine to protect against shingles for adults with COPD > 50
28
New cards
COPD Pharmacological Therapies
* Bronchodilators
* Anticholinergics
* Beta-2 agonists
* Theophylline
* Corticosteroids
* Inhaled vs systemic
* Additional therapy
* Antibiotics
* Roflumilast
* Anticholinergics
* Beta-2 agonists
* Theophylline
* Corticosteroids
* Inhaled vs systemic
* Additional therapy
* Antibiotics
* Roflumilast
29
New cards
Anticholinergic Agents
* Ipratropium (Atrovent HFA)
* Tiotropium (Spiriva)
* Tiotropium (Spiriva)
30
New cards
Anticholinergic Agents Indication
Safe & well tolerated considered first line therapy in COPD
31
New cards
Anticholinergic Agents MOA
Airway smooth muscle relaxation
32
New cards
Ipratropium (Atrovent HFA)
* Decreased systemic absorption
* MDI or nebulizer
* MDI or nebulizer
33
New cards
Ipratropium (Atrovent HFA): Onset and Duration
* Onset 1-2 hours
* Duration 4-6 hours
* Duration 4-6 hours
34
New cards
Ipratropium (Atrovent HFA): Dosing
* MDI: 2 pugs inhaled 4 times daily
* Neb: 0.5mg (2.5mL) inhaled every 6-8 hours
* Neb: 0.5mg (2.5mL) inhaled every 6-8 hours
35
New cards
Tiotropium (Spiriva)
* Dry powder & soft mist inhaler
* Newer options:
* Aclidinium bromide (Tudorza Pressair)
* Glycopyrrolate (Seebri Neohaler)
* Umeclidinium (Incruse Ellipta)
* Newer options:
* Aclidinium bromide (Tudorza Pressair)
* Glycopyrrolate (Seebri Neohaler)
* Umeclidinium (Incruse Ellipta)
36
New cards
Tiotropium (Spiriva) Duration
Duration = 24 hours
37
New cards
Tiotropium (Spiriva) Dosing
Once daily dosing
* DPI: 2 puffs (1 cap) daily
* Soft Mist: 2 pugs (5mcg) daily
* DPI: 2 puffs (1 cap) daily
* Soft Mist: 2 pugs (5mcg) daily
38
New cards
Beta 2 Agonists MOA
* Stimulation of beta-2 adrenergic receptors
* Resulting in airway smooth muscle relaxation
* Alternative to anticholinergic agents
* Resulting in airway smooth muscle relaxation
* Alternative to anticholinergic agents
39
New cards
Beta 2 Agonists ADE
* Safe and well tolerated
* May use without inhaled corticosteroids (ICS) in COPD
* May use without inhaled corticosteroids (ICS) in COPD
40
New cards
Types of Beta 2 Agonists
* Short-acting
* Long-acting
* Long-acting
41
New cards
Short-Acting Beta 2 Agonists Product
* Most common is albuterol
* Levalbuterol also available
* Levalbuterol also available
42
New cards
Short-Acting Beta 2 Agonists Indication
* “Rescue” inhale for acute symptoms
* Alternative to LABA for maintenance
* Treatment of acute exacerbation
* Alternative to LABA for maintenance
* Treatment of acute exacerbation
43
New cards
Short-Acting Beta 2 Agonists: Maintenance Dose
2 puffs every 4-5 hours
44
New cards
Long-Acting Beta 2 Agonists Products
* Salmeterol (Serevent Diskus)
* Arformoterol (Brovana)
* Formoterol (Perforomist)
* Indacaterol (Arcapta Neohaler)
* Olodaterol (Striverdi Respimat)
* Arformoterol (Brovana)
* Formoterol (Perforomist)
* Indacaterol (Arcapta Neohaler)
* Olodaterol (Striverdi Respimat)
45
New cards
Long-Acting Beta 2 Agonists Dosing
* Salmeterol (Serevent Diskus)
* 1 puff inhaled every 12 hours
* 1 puff inhaled every 12 hours
46
New cards
Combination Bronchodilators Indication
Better response compared to monotherapy
47
New cards
Types of Combination Bronchodilators
* Short-acting
* Long-acting
* Long-acting
48
New cards
Short-Acting Combination Bronchodilator Products
* Ipratropium + albuterol
* Duoneb® (nebulizer)
* Combivent® (inhaler)
* Duoneb® (nebulizer)
* Combivent® (inhaler)
49
New cards
Long-Acting Bronchodilators Products
* Umeclidinium + vilanterol (Anoro Elipta®)
* Tiotropium + oladaterol (Stiolto Respimat®)
* Glycopyrrolate + indacaterol (Utibron Neohaler®)
* Glycopyrrolate + formoterol (Bevespi Aerosphere®)
* Tiotropium + oladaterol (Stiolto Respimat®)
* Glycopyrrolate + indacaterol (Utibron Neohaler®)
* Glycopyrrolate + formoterol (Bevespi Aerosphere®)
50
New cards
Theophylline Indication
* Place in therapy – controversial
* Less effective than inhaled therapy
* Risks outweigh benefits
* 2nd or 3rd line
* Less effective than inhaled therapy
* Risks outweigh benefits
* 2nd or 3rd line
51
New cards
Theophylline Dosing
* Use long-acting formulations
* 300-900 mg daily
* 300-900 mg daily
52
New cards
Theophylline ADE
* Toxicity
* Palpitations (atrial or ventricular)
* Grand mal convulsions (irrespective of prior epileptic history)
* Palpitations (atrial or ventricular)
* Grand mal convulsions (irrespective of prior epileptic history)
53
New cards
Inhaled Corticosteroids
* Decrease symptoms, exacerbations
* Does not alter progression
* Does not alter progression
54
New cards
Inhaled Corticosteroids Indications
Combined with a LABA for patients with exacerbations despite appropriate bronchodilator therapy
55
New cards
Inhaled Corticosteroids ADE
* Pneumonia, increased fracture risk, others
* Increased exacerbation with withdrawal
* Increased exacerbation with withdrawal
56
New cards
Inhaled Corticosteroids: Single Agent Product
__**Not approved for COPD**__
* Beclomethasone
* Fluticasone
* Beclomethasone
* Fluticasone
57
New cards
Inhaled Corticosteroids: Combination Products
* Budesonide + formoterol (Symbicort®)
* Fluticasone + salmeterol (Advair®)
* Fluticasone + vilanterol (Breo Elipta®)
* Fluticasone + salmeterol (Advair®)
* Fluticasone + vilanterol (Breo Elipta®)
58
New cards
Inhaled Corticosteroids: Newer Therapies
* Trelegy Elpita® (fluticasone + umeclidinium + vilanterol)
* Breztri Aerosphere® (budesonide + glycopyrrolate + formoterol)
* Breztri Aerosphere® (budesonide + glycopyrrolate + formoterol)
59
New cards
Systemic Corticosteroids Indication
* Maintenance therapy
* Avoid if possible
* No evidence of long-term benefits
* Avoid if possible
* No evidence of long-term benefits
60
New cards
Systemic Corticosteroids ADE
* Steroid myopathy
* Glucose effects
* Bone effects
* Glucose effects
* Bone effects
61
New cards
Systemic Corticosteroids: Dosing and Administration
* Lowest effective dose
* Dose in the morning, once daily administration
* Dose in the morning, once daily administration
62
New cards
Roflumilast (Daliresp®) MOA
* PDE4 inhibitor
* Reducing inflammation by inhibiting the breakdown of intracellular cyclic AMP
* Reducing inflammation by inhibiting the breakdown of intracellular cyclic AMP
63
New cards
Roflumilast (Daliresp®) Dosing
Once daily oral medication
64
New cards
Roflumilast (Daliresp®) Clinical Effects
Small decrease in the rate of exacerbation
65
New cards
Roflumilast (Daliresp®) ADE
* N/V
* Weight loss
* Abdominal pain
* Sleep disturbance
* Headache
* CNS
* Psychiatric
* Weight loss
* Abdominal pain
* Sleep disturbance
* Headache
* CNS
* Psychiatric
66
New cards
Other Therapies
* Antibiotics
* Mucolytics–N-acetylcysteine
* Statins
* Leukotriene modifiers
* Vasodilators
* Mucolytics–N-acetylcysteine
* Statins
* Leukotriene modifiers
* Vasodilators
67
New cards
COPD: What to Avoid
* Cough suppressants
* Beta-blockers OK if indicated for cardiovascular disease
* Beta-blockers OK if indicated for cardiovascular disease
68
New cards
Antibiotics Indications
Chronic azithromycin reduces exacerbations
69
New cards
Antibiotics ADE
Increases resistance and hearing loss
70
New cards
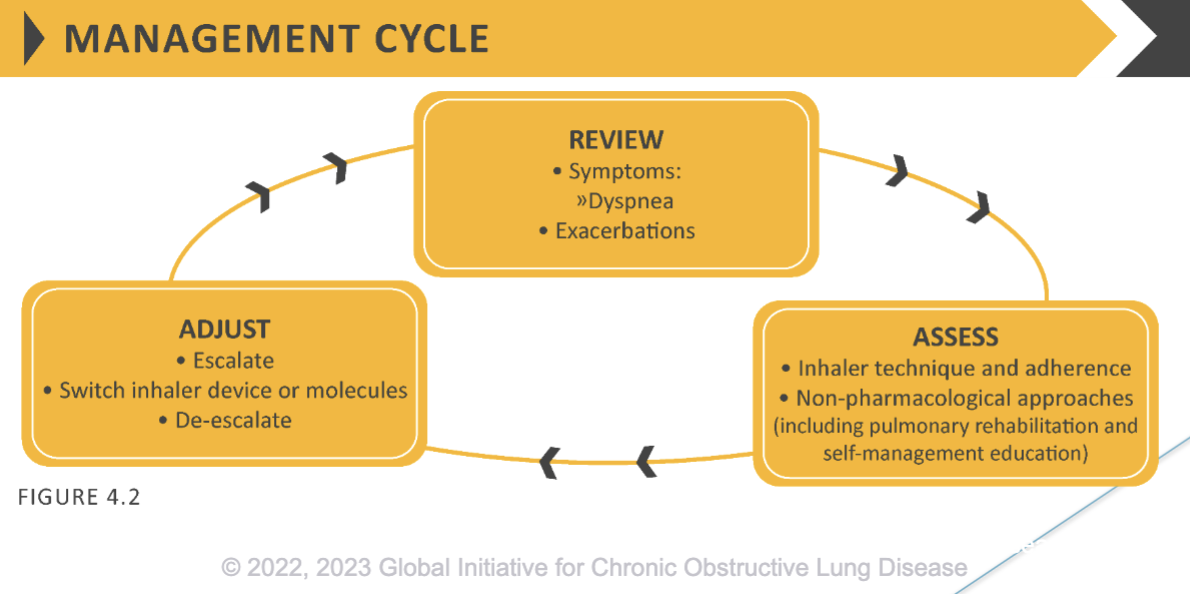
Treatment of Stable COPD: Reassessment
* Patients should be reassessed for attainment of treatment goals and identification of any barriers for successful treatment
* Following review of the patient response to treatment initiation, adjustments in pharmacological treatment may be needed
* Following review of the patient response to treatment initiation, adjustments in pharmacological treatment may be needed
71
New cards
What to Check if Patient Isn’t Responsive to Initial Treatment
* Adherence
* Inhaler technique
* Possible interfering comorbidities
* Consider the predominant treatable trait to target
* Dyspnea or exacerbations
* Inhaler technique
* Possible interfering comorbidities
* Consider the predominant treatable trait to target
* Dyspnea or exacerbations
72
New cards
COPD Follow-Up Treatment Flow-Chart
73
New cards
Non-Pharmacological Management
* Education and self-management
* Physical activity
* Pulmonary rehabilitation programs
* Exercise training
* Self-management education
* End of life and palliative care
* Nutritional support
* Vaccination
* Oxygen therapy
* Physical activity
* Pulmonary rehabilitation programs
* Exercise training
* Self-management education
* End of life and palliative care
* Nutritional support
* Vaccination
* Oxygen therapy
74
New cards
What to Monitor
* Measurements
* Symptoms
* Exacerbations
* Imaging
* Smoking status
* Symptoms
* Exacerbations
* Imaging
* Smoking status
75
New cards
Monitoring and Follow-up: Measurements
Decline in FEV1 can be tracked by spirometry performed at least once a year
76
New cards
Monitoring and Follow-up: Symptoms
* At each visit, information on symptoms since last visit should be collected including:
* Cough and sputum
* Breathlessness
* Fatigue
* Activity limitation
* Sleep disturbances
* Cough and sputum
* Breathlessness
* Fatigue
* Activity limitation
* Sleep disturbances
77
New cards
Monitoring and Follow-up: Exacerbations
The frequency, severity, type and likely causes of all exacerbations should be monitored
78
New cards
Monitoring and Follow-up: Imaging
If there is a clear worsening of symptoms, imaging may be indicated
79
New cards
Monitoring and Follow-up: Smoking Status
At each visit, the current smoking status and smoke exposure should be determined followed by appropriate action
80
New cards
COPD Exacerbations
Defined as an acute worsening of respiratory symptoms that result in additional therapy
81
New cards
COPD Exacerbations Classifications
* Mild
* Moderate
* Severe
* Moderate
* Severe
82
New cards
Mild COPD Exacerbations
Treated with short-acting bronchodilators (SABD) only
83
New cards
Moderate COPD Exacerbations
Treated with SABD plus antibiotics and/or oral corticosteroids
84
New cards
Severe COPD Exacerbations
* Patient requires hospitalization or visits the emergency room
* May be associated with acute respiratory failure
* May be associated with acute respiratory failure
85
New cards
COPD Exacerbation Causes
* Viral or bacterial infections
* Air pollution
* No identifiable cause
* Rule out other co-morbid conditions
* Pneumonia
* Heart failure exacerbation
* Acute coronary syndrome
* Air pollution
* No identifiable cause
* Rule out other co-morbid conditions
* Pneumonia
* Heart failure exacerbation
* Acute coronary syndrome
86
New cards
Management of Exacerbations
* 3 classes commonly used for COPD exacerbations
* Bronchodilator
* Corticosteroids
* Antibiotics
* Bronchodilator
* Corticosteroids
* Antibiotics
87
New cards
COPD Exacerbations: Brochodilators
* No high-quality evidence from RCTs
* Recommended that SABAs, with or without short-acting anticholinergics, are the initial bronchodilators for acute treatment of a COPD exacerbation
* Recommended that SABAs, with or without short-acting anticholinergics, are the initial bronchodilators for acute treatment of a COPD exacerbation
88
New cards
COPD Exacerbations: Corticosteroids
* Data suggests systemic glucocorticoids in COPD exacerbations shorten recovery time and improve lung function (FEV1)
* They also improve oxygenation, the risk of early relapse, treatment failure, and length of hospitalization
* They also improve oxygenation, the risk of early relapse, treatment failure, and length of hospitalization
89
New cards
Bronchodilator Therapy
Initiate or continue maintenance inhalers when stable
* Albuterol
* 2.5-10 mg every 20 min x 3 then every 1-4 hours as needed by nebulizer
* Ipratropium
* 0.5 mg every 6 hours by nebulizer
* Albuterol
* 2.5-10 mg every 20 min x 3 then every 1-4 hours as needed by nebulizer
* Ipratropium
* 0.5 mg every 6 hours by nebulizer
90
New cards
Steroid Therapy in Exacerbation: Benefits
* Moderate benefit
* Improves patient outcomes:
* Recovery time
* Lung function
* Relapse
* Improves patient outcomes:
* Recovery time
* Lung function
* Relapse
91
New cards
Steroid Therapy in Exacerbation: Monitoring
* Monitor for adverse effects
* Hyperglycemia
* Worsening heart failure
* Hyperglycemia
* Worsening heart failure
92
New cards
Steroid Therapy in Exacerbation: Dosing and Administration
**40 mg of prednisone once daily for 5 days**
93
New cards
Antibiotic Therapy Indications
* Still evolving, limited evidence
* 3 cardinal symptoms OR have 2 of the 3 with one being increase of purulence of sputum
* Dyspnea
* Sputum volume
* Sputum purulence
* 3 cardinal symptoms OR have 2 of the 3 with one being increase of purulence of sputum
* Dyspnea
* Sputum volume
* Sputum purulence
94
New cards
Antibiotic Therapy: Appropriate Agents for Uncomplicated Patient
* Macrolide – azithromycin, clarithromycin
* 2nd or 3rd generation cephalosporin
* Doyxcycline
* May need to consider resistant organisms
* 2nd or 3rd generation cephalosporin
* Doyxcycline
* May need to consider resistant organisms
95
New cards
Antibiotic Therapy Duration
5-7 days
96
New cards
Other Interventions
* Assess risk for DVT – consider prophylaxis
* Maximize therapy for comorbid conditions
* Knowing patients end of life wishes
* Maximize therapy for comorbid conditions
* Knowing patients end of life wishes
97
New cards
Other Interventions: Assess Risk for DVT – Consider Prophylaxis
* Heparin 5000 units SQ every 8 hours
* Enoxaparin 40mg SQ daily
* Fondaparinux 2.5 mg SQ daily
* Enoxaparin 40mg SQ daily
* Fondaparinux 2.5 mg SQ daily
98
New cards
Other Interventions: Maximize Therapy for Comorbid Conditions
* IV fluids
* Diuretics
* Nutrition support
* Diuretics
* Nutrition support
99
New cards
Consequences Of COPD Exacerbations
* Negative impact on quality of life
* Impact on symptoms and lung function
* Increased economic costs
* Increased mortality
* Accelerated lung function decline
* Impact on symptoms and lung function
* Increased economic costs
* Increased mortality
* Accelerated lung function decline
100
New cards
COPD: Age of Onset
Usually > 40 yrs