Elbow, Wrist, Hand
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
Elbow Physical Exam
Palpate
Medial/lateral epicondyle
Olecranon
Cubital tunnel
Neurovascular status
Assess ROM
Flexion/extension
Pronation/supination
Intact, full, smooth motion?
Strength
Biceps/triceps
Forearm pronator/supinator
Resistance to rotation
Purely muscular/tendons
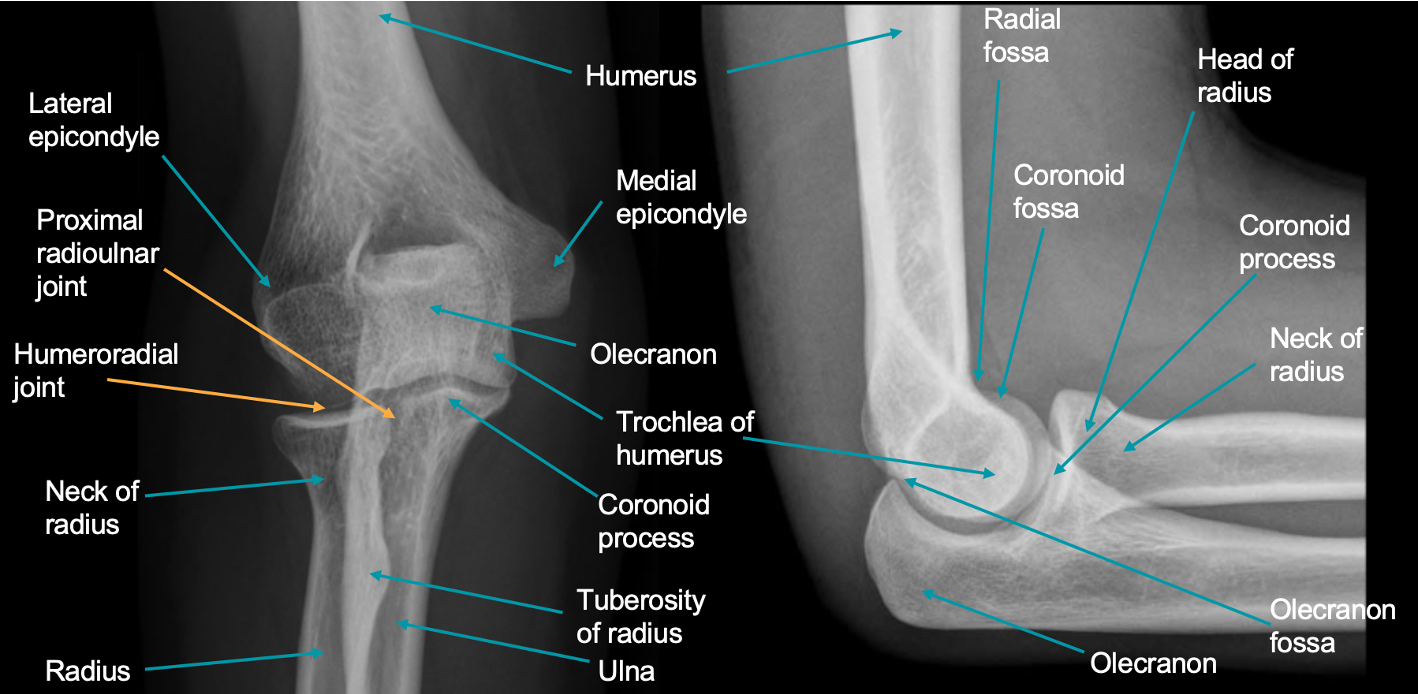
Elbow Anatomy
Olecranon important
Medial and lateral epicondyle
Fractures
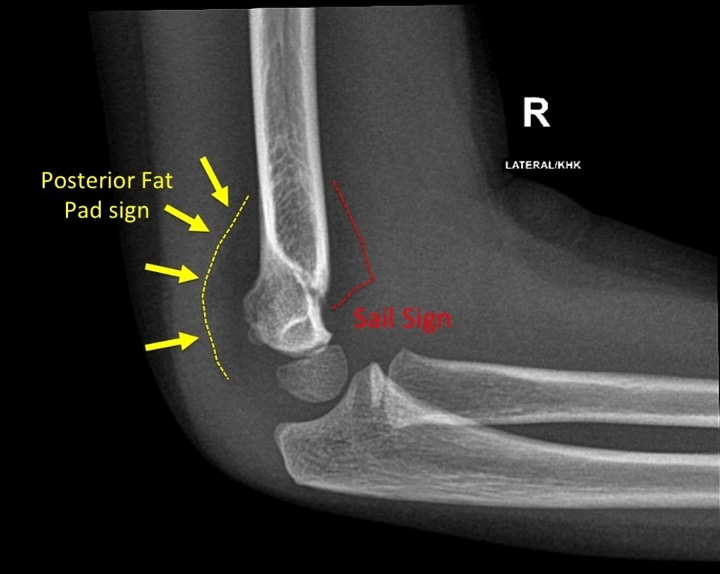
Look for sail sign
Anterior and posterior
Anterior are typical and can be seen normally
Posterior almost always pathologic
Medial Epicondylitis (Golfer’s Elbow)
Involves the tendons of the forearm flexors at the medial epicondyle
Causes
Overuse/activity (repetition)
Heavy lifting
Trauma
Weak UE
Presentation
Most common in dominant arm
Pinpoint tenderness over the medial epicondyle
+/- swelling along the medial epicondyle or proximal forearm
Soreness of the forearm flexors
Diagnosis
Is a clinical diagnosis: do not need imaging
Treatment
Conservative
Rest
Activity modification
Brace
NSAIDs: mainstay
Topicals
Cortisone injections
PT/OT
Surgical
Medical epicondylar debridement
Tendon is reinforced with suture to decrease micro-friction
Multilayer closure
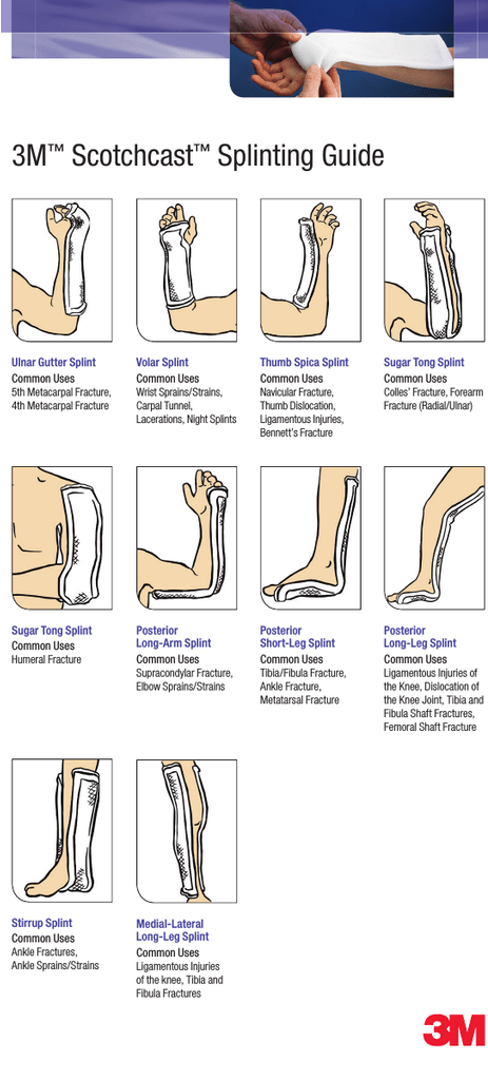
Immobilization: long arm splint for up to 2 weeks
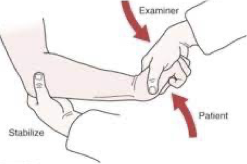
Golfer’s Elbow Test
Purpose
Assess for medial epicondylitis/epicondylagia
Position
Sitting or standing
Technique
Examiner palpate medial epicondyle of the humerus while supporting elbow with one hand
Examiner’s other hand passively supinates the patient’s forearm and fully extends the elbow, wrist, and fingers
Interpretation
(-): patient experiences no pain
(+): patient has sudden pain or discomfort along the medial aspect of the elbow or in the region of the medial epicondyle suggestive of medial epicondylitis

Lateral Epicondylitis (Tennis Elbow)
Involves the tendons of the forearm extensors at the lateral epicondyle
Causes
Overuse/activity
Heavy lifting
Trauma
Weak UE
Presentation
Most common in dominant arm
Pinpoint tenderness over the lateral epicondyle +/- swelling along the lateral epicondyle or proximal forearm
Soreness of the forearm extensors
Treatment
Conservative
Rest
Activity modification
Brace
NSAIDs
Topicals
Cortisone injections
PT/OT
Surgical
Lateral Epicondylar Debridement
Tendon is reinforced with suture to decrease micro-friction
Multilayer closure
Immobilization: long arm splint for up to 2 weeks
Cozen’s Test
Purpose
Assess for lateral epicondylitis/epicondylagia
Position
Sitting or standing
Technique
Examiner positions patient’s forearm in pronation, hand in fist, slightly radially deviated
Examiner palpates lateral epicondyle of the humerus with one hand while placing other hand over the dorsum of the patient’s fist
Patient is asked to extend wrist against the examiner’s resistance
Interpretation
(-): patient experiences no pain
(+): patient has sudden pain or discomfort along the lateral aspect of the elbow or in the region of the medial epicondyle suggestive of lateral epicondylitis
Medial/Lateral Epicondylitis Post-Op
10-14 days
Wound check and suture removal
Gentle ROM with PT
No lifting
6 weeks
ROM check
Tenderness over operative site?
Strengthening program
3 months
ROM
Strength check
If no pain or deficit, may release to normal activity
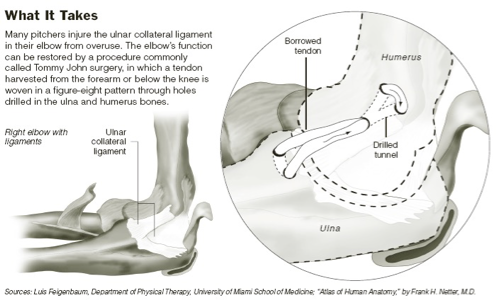
Ulnar Collateral Ligament Injury: Tommy John Surgery
Pitching Injury
UCL gets torn
Tommy John Surgery
Cannot use the torn ligament
Harvest one from the forearm or the leg
Can do figure 8 formation: tunnel through ulna and humerus and create a new one
Post-Op Plan
Splinted
Initiation of PT/OT: ROM and strength
Very tailored to the patient and the long term goal
Cubital Tunnel Syndrome
Have stenosis or compression of the ulnar nerve in the cubital tunnel
Symptoms
Elbow pain
Numbness/tingling/pain at the 5th digit and ulnar border of 4th digit
Muscle atrophy (late finding)
Diagnosis
Is clinical
May see edema or stenosis on MRI
Treatment
Conservative
Avoid provoking activities (compression)
Elbow pad to reduce elbow flexion
NSAIDs
PT/OT
Surgical
Ulnar nerve transposition
Decompression and release of the ulnar nerve from the medial aspect of the elbow
Long arm splint with elbow flexed to 90 degrees and the forearm in neutral
Tinel Sign
Purpose
Assess for cubital tunnel syndrome/ulnar nerve compression
Position
Sitting or standing
Technique
Examiner locates the ulnar nerve between the olecranon process and the medial epicondyle
Examiner repeatedly taps or percusses the trapped nerve with index finger or middle finger
Interpretation
(-): patient experiences no pain, numbness, or tingling
(+): patient experiences pain, numbness, or tingling in the ulnar nerve distribution along the forearm and/or hand associated with the tapping/percussing suggestive of cubital tunnel syndrome

Cubital Tunnel Syndrome Post-Op Plan
3-5 days
Early mobilization?
Removable splint
10-14 days
Suture removal
ROM
Symptom check
6 weeks
ROM
Wound healing
Sensitivities
Olecranon Bursitis
Bursa sac is such a finite space
Etiology does matter
Sometimes do not know what happened
Causes
Overuse/repetitive activity (more common)
Trauma
Gout
Autoimmune
Infectious
Treatment
Conservative
NSAIDs
Medrol pack: should not be taking NSAIDs (bleeding risk) and should be on GI protection (PPI)
Warm compresses
ACE wrap/compression
Aspiration/injection
Use aseptic technique
Should be going parallel: collection is protruding so far out that you have so much space and have decreased risk of injecting the bone
If fluid is suspicious, then aspirate should be sent for culture, crystals, cell count, gram stain, etc… → do not inject cortisone
If fluid straw colored, then cortisone can be injected to help decrease inflammation
Always clean site, Band-Aid, and ACE wrap to help compress dead space
Can re-accumulate: may need serial aspirations
Surgical
Olecranon bursectomy
May sedimentize with crystals if they have had serial injections with cortisone (> 3 times in a lifetime) → over injection has reverse effect and causes more issues

Olecranon Bursitis Post-Op Plan
10-14 days
Wound check
Suture removal
Splint check
6 weeks
Wound healing
ROM
Return to normal activity
Posterior Elbow Dislocation
Very rare
Force from front pushes through forearm
See protrusion of olecranon posteriorly
Traction down and pull forward to reduce: should not be done outside of an emergent setting
Worried about nerves and blood vessels: brachial artery/entrapment
Need to check for perfusion first before reduction because fracture itself can cause bleeding/entrapment

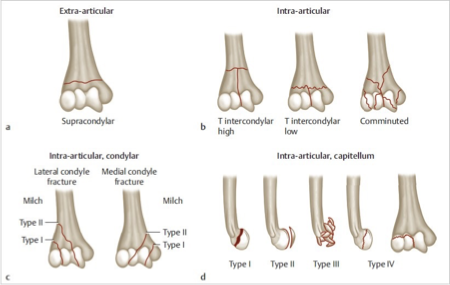
Elbow Fractures
When elbow fractures occur, it should be an elbow specialist
Not held responsible for the image
Every single type of fracture can result in functional deficit
Fat Pad/Sail Sign
Suggests the presence of an occult fracture of the elbow
Anterior fat pad → often normal
Posterior fat pad → always abnormal → consider CT/MRI
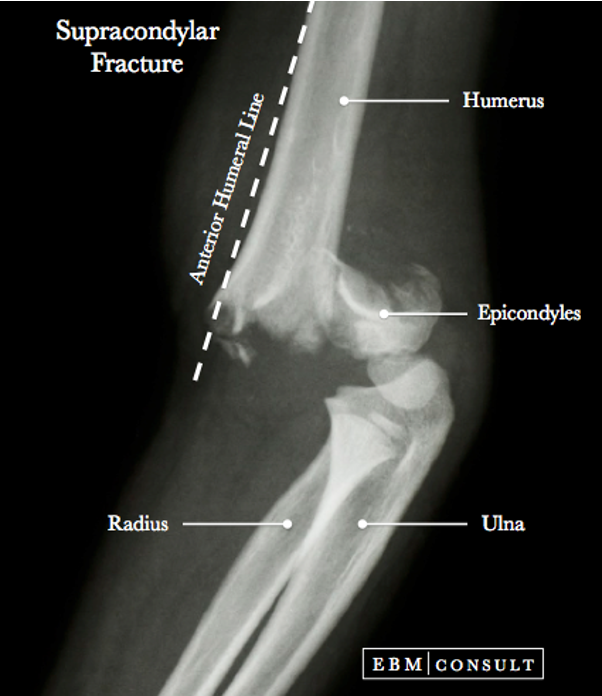
Supracondylar Elbow Fractures
Can be very devastating
Have vital structures in ante-cubital fossa → often occurs with a dislocation
Have shift of anatomy and shards of bone that can puncture structures
Supracondylar ORIF
Complications
Volkmann’s Contracture
Occurs in the absence of blood flow to the forearm
Causes muscles to shorten and contracture of forearm
Usually associated with elbow fractures, bleeding disorders, and animal bites
Sometimes cannot be reversed


Supracondylar ORIF Post-Op Plan
Splinted intra-operatively by surgeon
Splints are perfectly tailored to the patient
7-10 days
Wound check
Suture removal
Splint check
+/- X-rays
2-4 weeks
X-rays
Wound healing
PT/OT: a lot
Forearm Fractures
Happen anywhere along the ulna and radius
Usually have to be fixed with plates and screws

Monteggia Fracture
Ulnar fracture and radial head dislocated

Galeazzi Fracture
Radial fracture and ulna dislocated
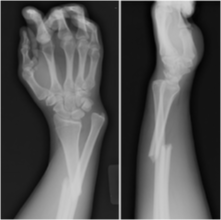
Distal Radius Wrist Fractures
Use intra-operative fluoroscopy and open reduction internal fixation
K wires are used to hold the reduction internally until the hardware can be placed in a stepwise formation

Colle’s Fracture
Falls outward
Hand goes forward and the bone goes anteriorly


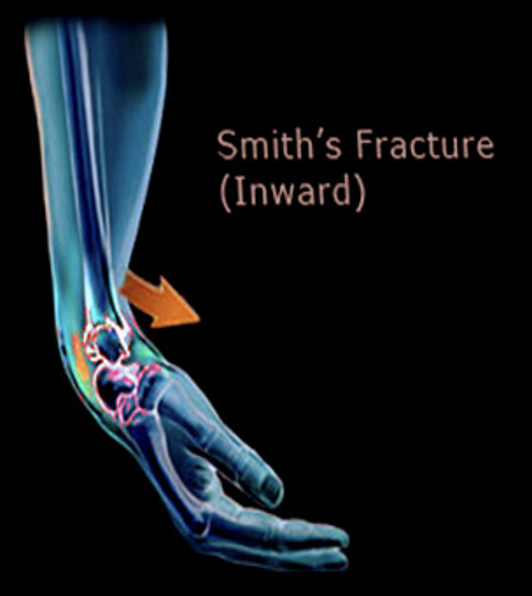
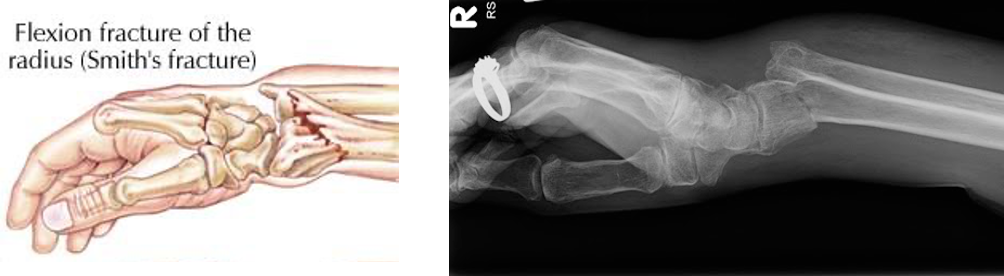
Smith Fracture
Falls inward
Force generated dorsally/posteriorly: bone shifted that way
Wrist/Hand Exam
Palpate
Distal radius: styloid
Distal ulna: styloid
Carpals: scaphoid (snuffbox) and scaphoid tubercle (volar)
Assess ROM
Flexion/extension
Radial/ulnar deviation
Strength
Wrist flexors/extensors
Resistance to rotation
Wrist/Hand Anatomy
Scaphoid injury most important

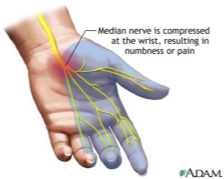
Carpal Tunnel Syndrome
Compression of the median nerve as it passes through the carpal tunnel
Transverse carpal ligament
Pulls inward and compresses the median nerve underneath
Causes
Diabetes
Hypothyroidism
Obesity
Pregnancy (retention of fluid)
Overuse/compression (typing)
Masses
Presentation
Numbness, tingling, pain
Thumb, index, middle and radial border of ring finger
Night pain
Weakness of abductor pollicis brevis
Thenar atrophy
Impaired thenar innervation due to chronic median nerve compression, if left untreated, can lead to thenar atrophy
Will have permanent deficit
Act on sensory issues before motor issues become a problem
Diagnosis → clinical
Treatment
Conservative
Braces/splints
PT/OT
+/- NSAIDs
+/- PO corticosteroids (Medrol packs: can cause high BGL in diabetics and cause SVT)
Cortisone injections with
Surgical
Carpal tunnel release
Can be open vs endoscopic
Place blade to slice the ligament and unroofs it to give the median nerve more room
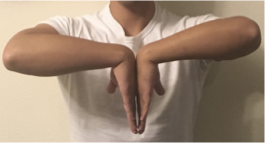
Phalen’s Test
Purpose
Assess for carpal tunnel syndrome
Position
Sitting with elbows flexed on the table, wrists filly flexed
Technique
Ask patient to push the dorsal surface of the hands together and hold position for 30-60 seconds
Interpretation
(-): patient has no CTS symptoms during the test, even for prolonged time
(+): patient experiences reproducible CTS symptoms including numbness, tingling, and/or burning along the distribution of the median nerve suggestive of CTS
Tinel’s Sign
Purpose
Assess for carpal tunnel syndrome
Position
Sitting with forearms supinated
Technique
Examiner supports patients supinated wrist and hand in one hand while using the index or middle fingertip to percuss over the transverse ligament
Interpretation
(-): patient has no CTS symptoms while percussing
(+): patient experiences reproducible CTS symptoms including numbness, tingling, and/or burning along the distribution of the median nerve suggestive of CTS

Carpal Tunnel Release Post-Op Plan
Post-op follow up within 1 week of surgery
Wound healing/dressing/splint fit
Check motor and sensory function
PT/OT plan
Overall plan per surgeon’s protocol
Dupuytren’s Contracture
Palmar fascia
Protective barrier between the skin and tendons: helps bend fingers
Thickens and drawn inward: causes finger to become bent by the force of the contracture
Most common affects 4th and 5th digits
Can be linked to alcoholism/overuse
Presentation
Scar like band at base of fingers
Inability to lay hand flat on table
Unable to straighten finger mechanically: fascia has contracted and cannot push past it
Treatment
PT/OT
Steroid injections
Radiation therapy
Enzyme therapy
Needling
Surgery → skin grafting

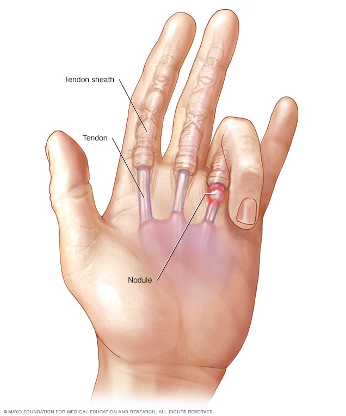
Trigger Finger
Tendon
Helps finger bend toward the palm
Surrounded by sheath
Lined with synovium: produces fluid to help tendon glide as finger bends and straightens
In trigger finger, tendon inflames and sheath thickens
Typically involves one finger: tendon or sheath becomes very inflamed and enlarged and cannot fit through smoothly and becomes stuck in a bent position (usually at lower portion of finger)
Finger remains bent when asked to straighten finger: may feel a pop as it straightens
Can be mechanically extended: is the pulley of the flexor tendon that is the problem
Treatment
Conservative
NSAIDs
Cortisone injection: need U/S guidance to make sure you do not rupture the structures
PT/OT
Splinting
Surgical
Tendon sheath incision/A1 pulley release
Open the tendon sheath and unroof it
Trigger Finger Post-Op
10-14 days
Suture removal
Wound check
PT/OT protocol
4 weeks
Final ROM
Wound check
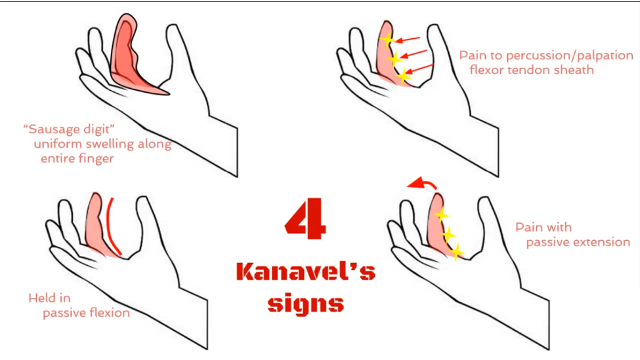
Infectious Flexor Tenosynovitis
SURGICAL URGENCY
People can lose fingers or hand
Four Kanavel Signs
Finger held in flexed position for comfort
Intense pain with passive extension
Uniform (fusiform) swelling of digit (not just localized)
Tenderness along the entire flexor tendon sheath
Patient needs incision and drainage and IV antibiotics
May need to go in, unroof, and debride to allow for antibiotics to penetrate (may not penetrate)
De Quervain’s Tenosynovitis
Inflammation of the tendon/tendon sheath along the thumb (radial side)
Cause → repetitive motion
Presentation
Pain/tenderness along the wrist/base of thumb
Treatment
Conservative
Thumb spica splint (immobilization)
PT/OT (anti-inflammatory modalities)
Cortisone injection
Surgical
Incision of the extensor tendon sheath
An incision is made through the extensor retinaculum to release the tendons from underneath and remove the friction that was causing the tendon sheaths to become inflamed with repetitive activity
Finkelstein Test
Purpose
Assess for tenosynovitis involving the extensor pollicis brevis and abductor pollicis longus
Position
Sitting or standing
Technique
Examiner asks the patient to position hand so the thumb is facing toward the ceiling
Patient is asked to adduct the thumb and wrap the fingers around it (makes a fist around the thumb) then perform an ulnar deviation
Interpretation
(-): patient has no pain or discomfort during the test
(+): patient experiences pain over the first extensor compartment over the wrist and potentially proximally along the forearm, originating at the thumb

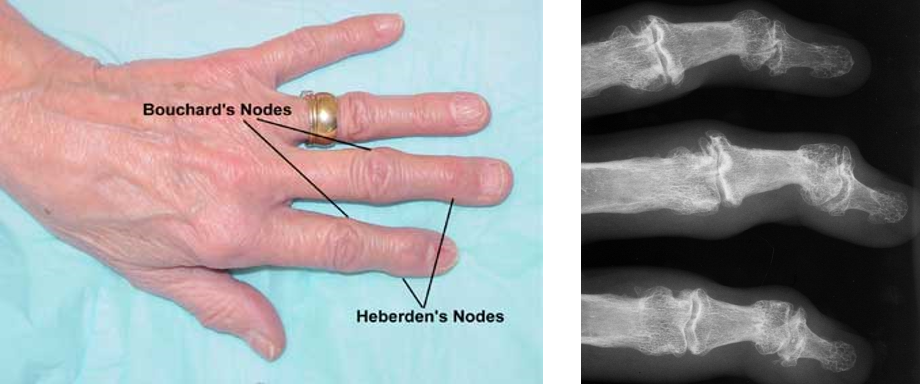
Osteoarthritis of the Hand
Symptoms
Increase as day progresses
Pain during and after use
Bouchard’s (PIP) and Heberden’s (DIP) nodes
Majority of symptoms can be from soft tissue swelling
Treatment
Conservative
NSAIDs/PO pain relievers
Aspiration/cortisone injection
Activity modifications
+/- intermittent PT/OT
+/- intermittent splinting
Surgical
Can do a joint replacement → only definitive treatment but is a last ditch effort (have to exhaust all other options)
Osteoarthritis Post-Op Plan
7-14 days
Wound check
Suture removal
+/- X-ray
PT/OT
Post-op visits per MD protocol
Wound check
ROM
Strength
X-rays
PT/OT progress
Metacarpal Fractures
Causes
Trauma
Striking with a closed fist
Boxer’s only used for 5th metacarpal
Presentation
Pain and reduced motion
Mechanism
Closed or open fracture
What did the hand make contact with? (human saliva, rusty metal, etc…)
Metacarpal Fracture ORIF Post-Op Plan
5-7 days
Wound check
10-14 days
Wound check
Suture removal
X-ray
Immobilization in splint or cast
PT ROM protocol
4 weeks
Wound and motion check
Strengthening
6-8 weeks
Motion check
X-ray
Phalanx Fractures
Causes
Trauma/sports → jammed finger
Presentation
Pain and reduced motion
Mechanism
Closed or open fracture
What did the hand make contact with
Other questions to ask
Which part of the phalanx is implicated
Intra-articular or extra-articular
Simple or comminuted
Displaced or non-displaced
Can usually leave alone but if it is intra-articular, angulated, comminuted → patients will lose function and it needs to get fixed

Phalanx Fracture ORIF Post-Op Plan
5-7 days
Wound check
10-14 days
Wound check
Suture removal
3-4 weeks
PCP can be removed if present
Wound healing
Aggressive PT
Bennet Fracture
Fracture/dislocation of the metacarpal bone at the base of the thumb

Scaphoid Fracture
Mechanism
Fall on outstretched hand
Patient report
Pain in anatomic snuffbox
Pain with ROM
Pain with weight bearing
Treatment
Conservative
Non-displaced fracture < 3 weeks old
Thumb-spica (used for anything that affects radial side of the wrist) splint for immobilization (88-95% healing rate)
Follow up every 3-4 weeks for splint change and X-ray
Continue conservative splinting or discuss surgery if non-union
Surgical
ORIF
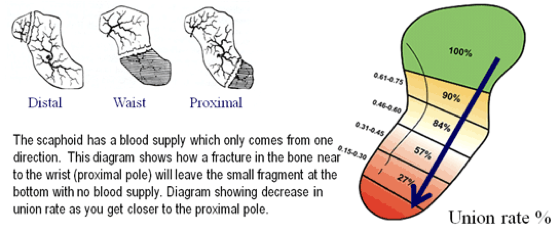
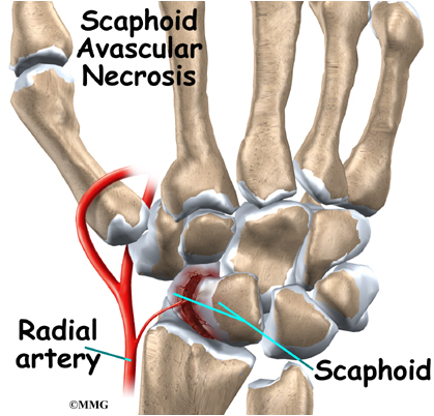
Avascular Necrosis
Disruption of blood flow to the bone → bone cell death, destruction/collapse of the bone, disability, pain
Does start immediately
Can be reversible if it is dealt with in the first couple of weeks → after that it is irreversible
Radial artery comes up and flows backwards
The distal portion of the scaphoid had the best flow while the proximal portion has close to none
Have break midway or proximally: chances of union are very low especially if it is displaced
Osteoarthritis usually develops 10-15 years later
Scaphoid ORIF Post-Op Plan
10-14 days
Wound check
Suture removal
PT protocol
6 weeks
Wound healing
Motion
X-ray healing
3 months
Motion
Tenderness
X-ray healing
If no evidence of healing → bone stimulator
If no healing > 6 months → non-union
Subungual Hematoma
Huge blood collection under nail plate and causes pressure → can kill the plate if left untreated
Trephination
Hot coil and burn hole into plate and erupts
Immediate pain relief and evacuates the hematoma

Paronychia
Will pack the negative space

Felon
Collection of infectious fluid in the fingertip (have compartments that become filled)
Treatment
Incision and drainage
Incision made on one or both sides of the fingertip
Break up the compartments
Gauze will be placed into the wound to aid the initial drainage
Flush out with a sterile solution
Antibiotics

Ganglion Cyst
Benign
Can be recurrent
Encapsulated
Can be loculated
Usually filled with joint fluid
Usually from overuse/activity/inflammation
Can feel hard or firm
Can restrict movement
Usually leave alone if causing no symptoms
