Module 7 SCI
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
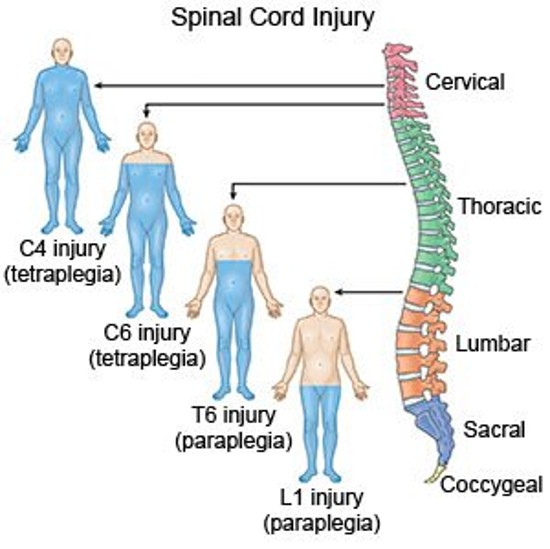
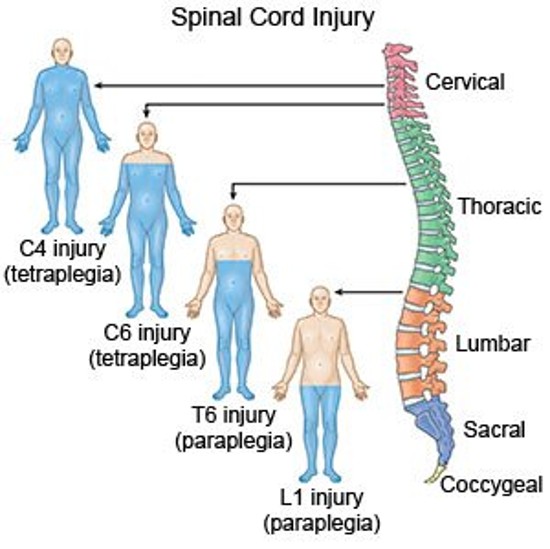
How are spinal cord injuries described by?
Level of the injury- the cord segment or dermatome level
Such as C6; L4 cord injury
Para
meaning two extremities
tetra or quadra
all four extremities
Paresis
weakness
Plegia
paralysis
Manifestations are related to?
The level and degree of injury
The higher the injury
The more severe the symptoms
C1-C7
Tetraplegia
T1-L4
Paraplegia
Primary Spinal Cord Injury- Initial mecahnism of injury
Compression
Interruption of the blood supply
Traction
Penetrating Trauma
Secondary Spinal Cord Injury
Ongoing progressiv damage
Ischemia
Hypoxia
Micrhemorrhage
Edema
What occurs in the cord post inury causing more damage?
Hemorrhage and edema
Apoptosis
Programmed cell death
can continue for weeks
What occurs over the first few days of the SCI? What happens at 72 hours?
a.) Extension of the cord injury from cord edema
b.) Prognosis
Which nerve should be watched? Why?
Phrenic nerve- because it is the nerve that controls the diaphragm, which is responsible of for breathing
What is initially experienced?
Initially SCI experience spinal shock
Depression of all cord & ANS function below injury. Lasts from few minutes to weeks
Spinal Shock
Decreased reflexes and loss of sensation below the level of injury
Motor loss- flaccid paralysis below the level of injury
Sensory loss- loss of touch, pressure, temperature, pain, and proprioception perception below the injury
Last days to weeks Maks post-injury function
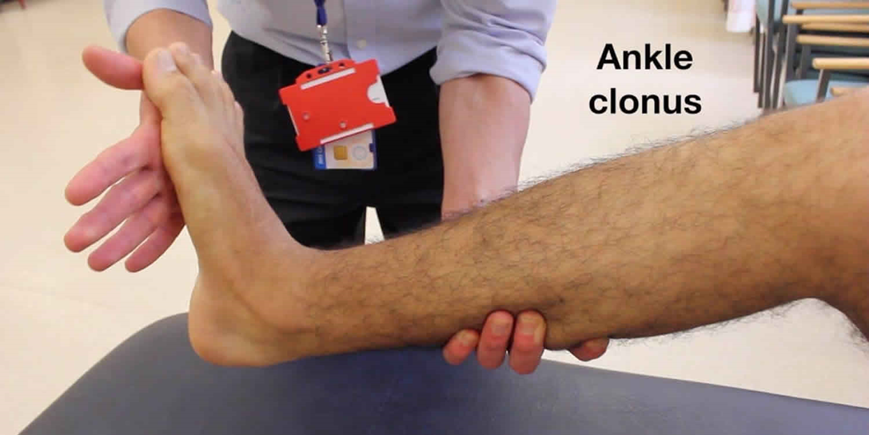
Sign of the return of function
Clonus
Neurogenic Shock
Cervical or High thoracic injury (T6 or higher)
Loss of SNS innervation results in parasympathetic dominance with vasomotor failure
Causes peripheral vasodilation, pooling, and decreased cardiac output
Hypotension and Bradycardia
Orthostatic hypotension and poor temperature control (poikilothermic)
Poor perfusion can worsen spinal cord ischemia
How is Neurogenic Shock Treated?
With vasopressors to maintain MAP and help perfuse spinal cord and IV fluids to maintain BP
Classifications of SCI
Mechanism of Injury
Skeletal and Neurologic Level
Completeness (degree) of Injury
Skeletal Level of Injury
The vertebral level where the most damage to the bones
Neurological Level of Injury
The lowest segment of the spinal cord with normal sensory and motor function on both sides of the body
Spinal Cord Level of Injury
When referring to spinal cord injury, it is the reflex arc level (neurologic), not the vertebral or bone level
The thoracic, lumbar, & sacral reflex arcs are higher than where the spinal nerves actually leave through the opening of the vertebral bone
Complete Injury
Total loss of sensory & motor function below the level of injury
Incomplete Degree of Injury
Mixed loss of voluntary motor activity and sensation; leaves some tracts intact
Incomplete Spinal Cord syndromes
Central cord syndrome
Anterior Cord syndrome
Brown Sequard Syndrome
Posterior Cord Syndrom
Causa Equine and Conus Medullaris
Complete Deficitis After Spinal Shock
Motor deficits: spasitc paralysis below the level of injury
Sensory- Loss of all sensory perception
Autonomic deficits- vasomotor failure and spastic bladder
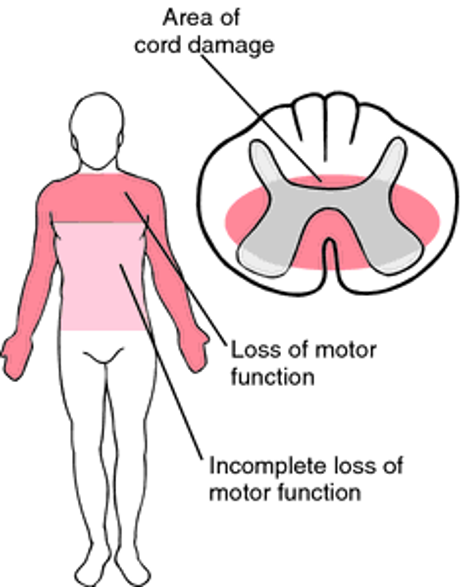
Central Cord Syndrome
Injury to the center of the cord by edema and hemorrhage
Motor weakness and sensory loss in all extremities
Upper extremities affected more
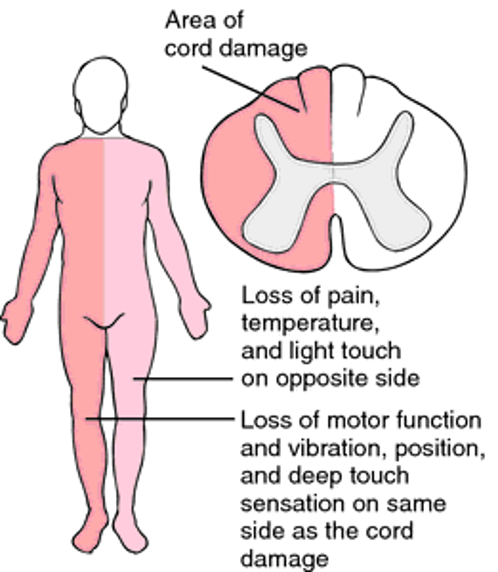
Brown Sequard Syndrome
Incomplete
Hemi section of cord
Ipsilateral paralysis
Ipsilateral superficial sensation, vibration, and proprioception loss
Contralateral loss of pain and temperature perception
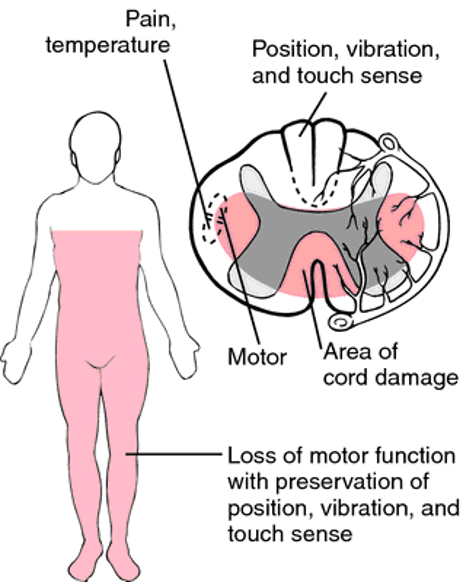
Anterior Cord Syndrome
Incomplete
Injury to the anterior cord
Loss of voluntary motor, pain, and temperature perception below the injury
Retains posterior column function (sensations of touch, position, vibration, motion)
Conus Medullaris
Incomplete
Injury to the sacral cord (conus) and lumbar nerve roots
Result- areflexic (flaccid) bladder and bowel, flaccid lower limbs
Cauda Equina
Incomplete
Injury to the lumbosacral nerve roots
Result- areflexic (flaccid) bladder and bowel, flaccid lower limbs
Acute Care Diagnostics
Immobilization
Hx & PE
ABGs, O2, intubation, Serial bedside PFT
Cardiac Output- MAP, BP, HR
Electrolytes, glucose, H&H, coagulation studies
Urinlaysis
CT, MRI, EMG
X rays
NGT/ Foley
Nutrition
Health History
Description of how and when the injury occurred, e.g., falls, gunshot or stabbings, sports injuries- description
Other Illnesses or disease processes
Physical Exam
Ability to move, breathe, and associated injury such as a head injury,fractures
LOC and pupils- may have indirect SCI from head injury
Respiratory status- phrenic nerve (diaphragm) and intercostals; lung sounds
Vitals
Motor Sensory
B/B function
Motor Assessment
Upper Extremity
Movement, strength, and symmetry, hand grips, flex and extend the arm at the elbow with and without resistance
Lower extremity
Flex and extend leg at the knee with and without resistance, plantar and dorsi flexion of foot, and assess for clonus
Sensory assessment
With the sharp and dull ends of a paperclip have the individual, with their eyes closed identify, use the dermatome as reference to identify level
C6 thumb
T4 nipple
T10 naval
How much respiratory loss is associated with cervical injury above C3?
total loss
What controls the diaphragm bilaterally?
The phrenic nerve (C3-5) in a cervical injury C3-5
If the nerve is nonfunctioning then the individual is ventilator dependent
How is the respiratory system affected with a cervical injury below C6?
Patient cannot cough effectively
Decreased chest expansion
Cough reflex & vital capacity
What can cause hypoventilation, atelectasis, & pneumonia in Cervical & Thoracic injuries?
Paralysis or weakening of the abdominal and intercostal muscles
Respiratory System Interventions
Assess RR, rhythm, depth, breath sounds, respiratory effet, ABGs, O2 sat
Assess signs of impending extension of SCI up cord to phrenic nerve level (C305)
Need for ventilatory assistance, tracheotomy, ventilator
O2, suctioning
Tilt bed (spine immobilized)
Quad cough (assistive cough, chest PT, BiPAP
Cardiovascular System Manifestations of SCI
Bradycardia
Peripheral vasodilation
Decreased CO
Relative hypovolemia
What causes Bradycardia? Interventions?
Decreased SNS
Cardiac monitoring necessary
Atropine may be needed
What does Peripheral vasodilation cause? Interventions?
causes hypotension decreased CO
IV fluids or vasopressors (norepinephrine) may be needed
Maintain MAP at 85-90
What is the main cause of relative hypovolemia?
venous dilation
What are some ways to prevent/ treat orthostatic hypotension?
Assess BP, especially when rising
Abdominal binder, calf compressors, TED hose
Assist PT with tilt table as individual gradually gets used to being in an upright position
Midrodine, salt
VTE prophylaxis
ROM, fluids, SCD’s Assess for VTE
Heparin
Assess skin breakdown thrombophlebitis; remove TED hose at least every shift
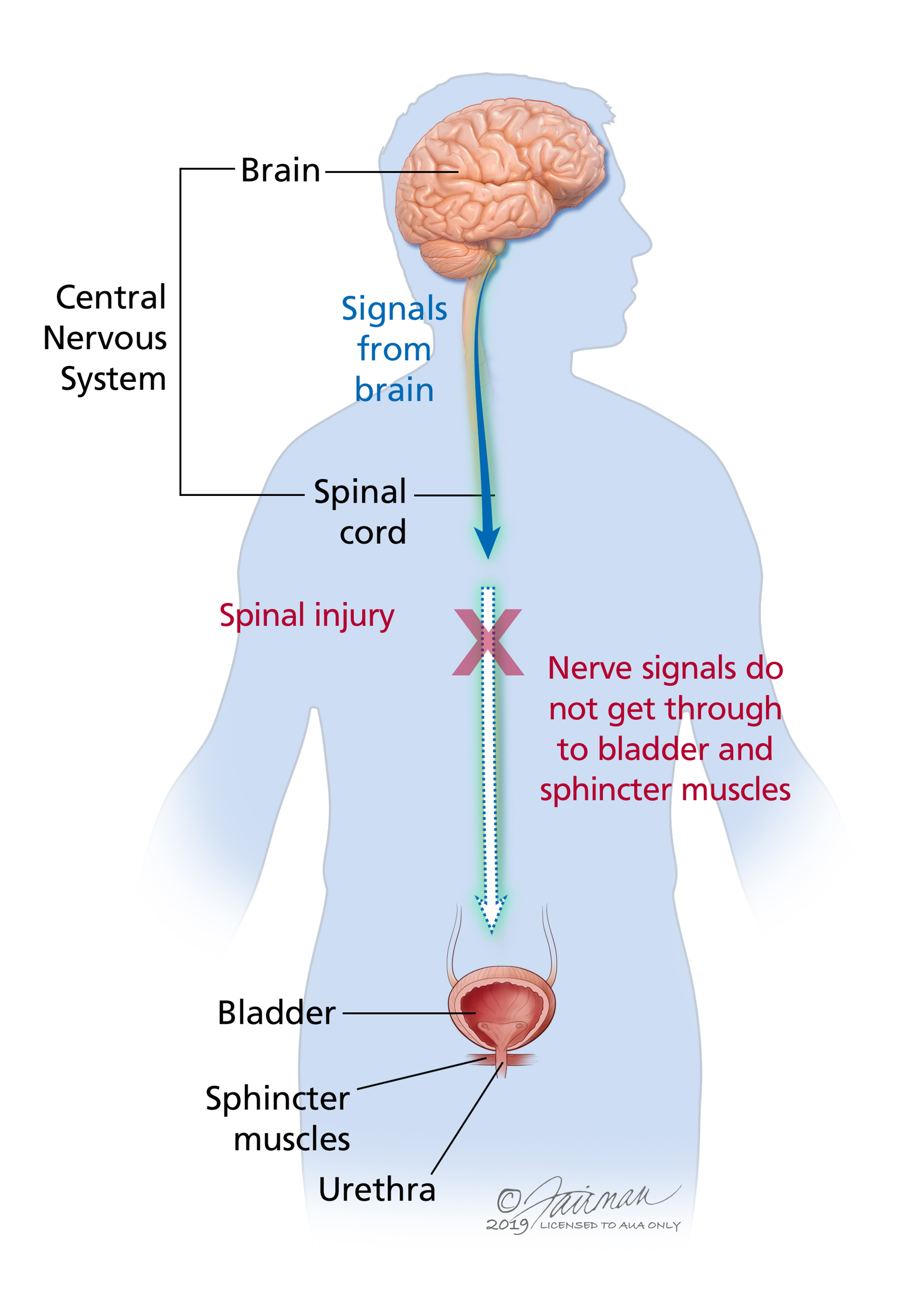
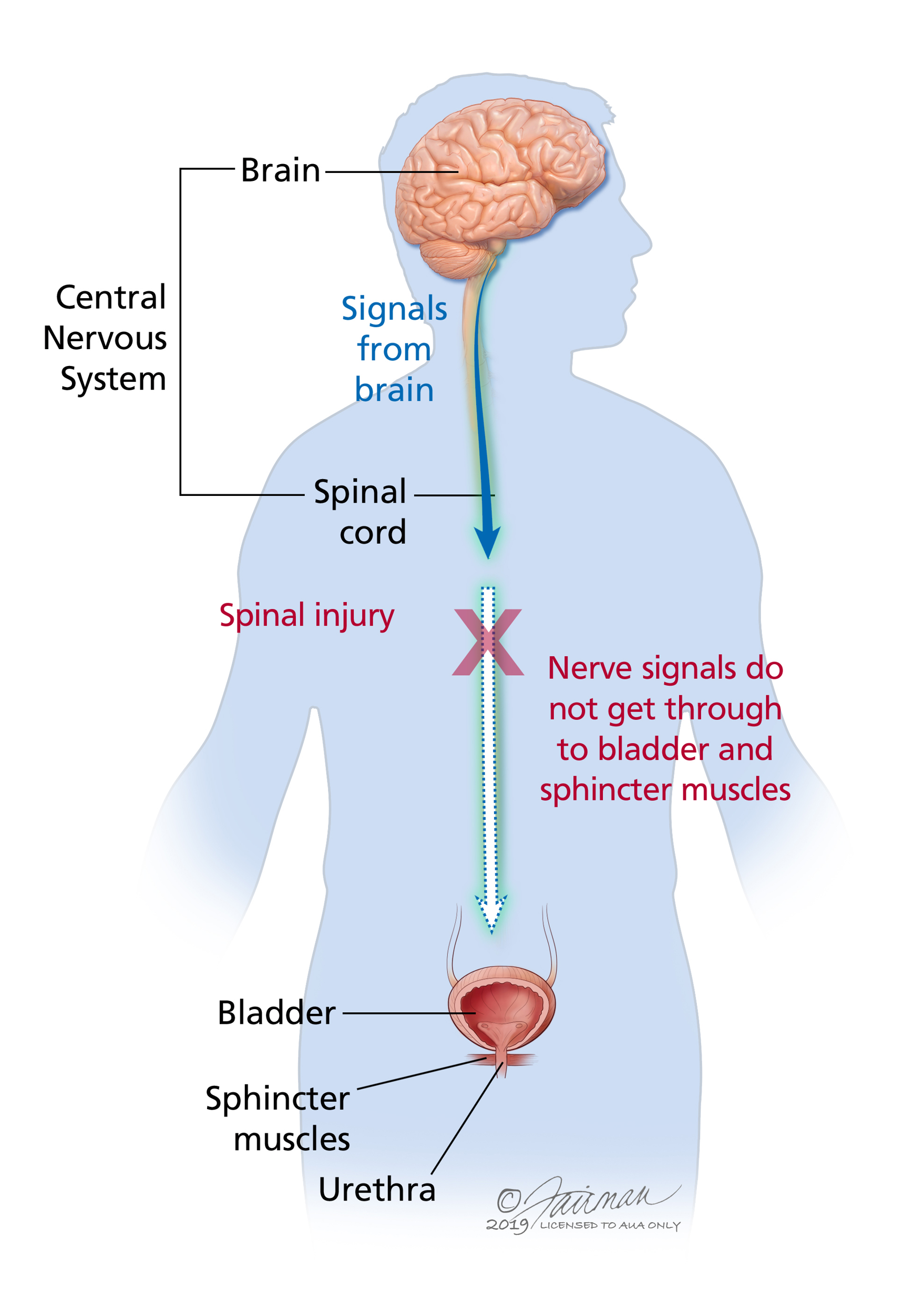
Urinary System Manifestations
Urinary retention
Flaccid Bladder
Spastic Bladder
Urinary retention
Common with spinal shock and acute phase of SCI
Post acute phase- hyperirritable bladder causing reflex emptying
What is the bladder function dependent on? What are urinary carre goals? Risks?
dependent on the level of injury
goal is to prevent infections, minimize/ contain incontinence
Risk for renal calculi, UTI, and reflux.
Flaccid bladder
lower motor neuron lesion
No reflex from S2,3, 4
Automatic emptying of bladder
Urine fills the bladder and dribbles out
Need Foley or frequent intermittent self-catheterization
Spastic bladder
upper motor neuron lesion
Reflex arc but no connection to or from brain
relfex firres at will
Bladder training- trigger points to stimulate emptying; self-catheterization
What stages will require an indwelling? What happens once stable?
a. early stages require an indwelling cath
b. clean intermittent catheterization (CIC) q 4-6h/ 24 hours
Urinary antiseptic
Lidocaine
Use bladder scan to see amount of urine in bladder
Goal- residual <100mL/ 20% bladder capacity
hydration
Other urinary interventions?
Condom catheter, bladder tapping, supra pubic cath, stoma
assess effectiveness of meds:
Urecholin- stimulates bladder contraction
Oxybutynin- to relax bladder
GI Manifestation of SCI
Decreased GI motility- Injury at T6 and ^, decreased GI motility, NG tube for intermittent suction
Stress ulcer prophylaxis- 6-14 day ^ risk, test stool and NGT drainage for blood, Monitor labs for decreased HCT, H2 blockers/ PPIs
Neurogenic bowel- reflex emptying occurs, bowel program

GI Interventions
Bowels rely more on bulk than on nerves
Fiber, fluids, bulk laxatives, stool softeners
Stiimulate bowels at the same time each day
Best after a meal when normal peristalsis occurs
Below T-12 may have Valsalva ability
Individual may progress from Dulcolax suppository to glycerin then to gloved finger for digital stimulation
Assess bowel sounds before giving food for the first time- paralytic ileus
What is a significant risk for the integumentary system?
Pressure ulcer and long term complication is pressure injury
Prevention is the goal
What are the contributing factors of pressure ulcers?
lack of movement
loss of sensation
compromised circulation
weight loss/ weight gain
incontinence
Integumentary systemt interventions
change position frequently- Q2h
Keep skin clean and dry
protection from extremes in temperature
inspect skin at least 2x/day especially over boney prominences
care for traction, collars, splints, braces
Avoid shearing and friction to soft tissue with transfers
removal of TED hose Q8h
Assess nutritional status/hydration
pressure mattress
Management of Temperature Control
thermoregulation
Poikilothermism- adjustment of body temp to room temp
Interruption of the sympathetic nervous system prevents temperature sensation from reaching the hypothalamus
Decreased ability to sweat of shiver below level of lesion
Hypothermia is common
Monitor temperature Q4h during acute phase
Adequate clothing in cool environment
Management of Nutrition
48-72 hours- GI tract may stop- paralytic ileus
NGT to suction
Weight loss (> than 10%)
Nutritional support wi/i 72 hours
parenteral nutrition
bowel sounds/ flatus/ swallow test before eating
refer to a dietitian
Musculoskeletal manifestations
joint contractures
bone demineralization
osteoporosis
muscle spasms
muscle atrophy
pathologic fractures
para/tetraplegia
Musculoskeletal Interventions
Log roll as a single unit; assist as needed to keep alignment; teach patient
care for traction, collars, splints, braces, assistive devices for ADLs
Flaccid paralysis interventions
use high top tennis shoes or splints to prevent contractures.
remove at least Q2h for ROM- active is best
Spastic Paralysis interventions and prevention
prevent spasms by avoiding; sudden movements or jarring of the bed'; internal stimulus (full bladder/skin breakdown; use of footboard; staying in one position too long; fatigues)
Treat spasms by decreasing causes; hot of cold pack; passive stretching; antispasmodic meds
Male sexuality Manifestations
UMN lesion
reflexogenic (S2,3,4) erections
LMN lesion
psychogenic erections
ejaculation/fertility may be effected
Female Sexuality Manifestations
Hormones more than nerves regarding fertility
C-section b/c of chance for autonomic dysreflexia during labor
Lack of sensation/ movement affects sexual performance