TBI, Glasgow Coma Scale, Rancho Los Amigos Scale of Cognitive Functioning
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
Severe TBI
Open-head injury, penetration to skull due to falls, car crash, struck by object
Closed head injury, no penetration to skull due to firearm injuries or struck by sharp object
Non-traumatic TBI
Drug overdose: both recreational & prescribed
Chronic substance use: Alcoholism, chronic drug use
Carbon monoxide: Depletion of oxygen
Environmental exposure: Toxins
Anoxia: Depletion of oxygen
TBI: Immediate medical interventions
Surgical Interventions
Removal of objects ( i.e., bullet. debris)
Evacuation of hematoma
Tumor removal
Bone flap
TBI: Clinical signs and symptoms - Secondary issues
Orthopedic-weight-bearing status may interfere with ability to participate fully in the rehab program
Pulmonary: may affect upright tolerance and endurance
Decubitus ulcers: an ulcer initially of the skin, due to prolonged pressure
Combo injuries: SCI/TBI account for 30 to 50% of brain injury cases
OT rehab focus (general info)
Splinting and casting-upper extremity
Neuromuscular re-education
Cognitive retraining
Participation in self-care (ADLs)
Bed positioning, transfers, and mobility (W/C)
Transfers
Wheelchair positioning and mobility
Equipment needs (W/C), bath equipment
Caregiver training
Home evaluation
If there is a time and need, OTs also work on:
Meal plan preparation, home management
Money-management
Pre-driving (usually addressed post-rehab)
Pre-vocational (usually addressed post-rehab)
Community skills
TBI: Clinical signs and symptoms
Decorticate or decerebrate posturing
Retrograde, anterograde, or post-traumatic amnesia
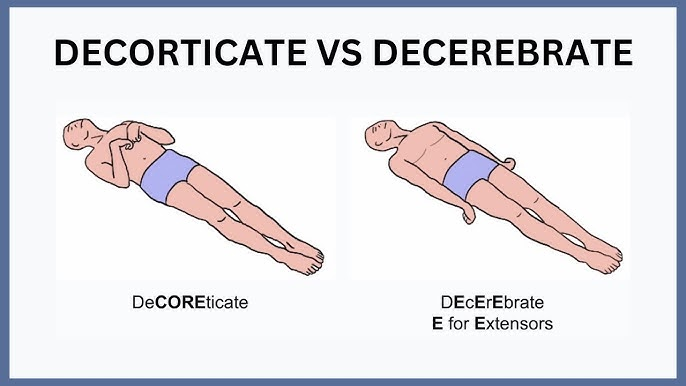
TBI: Decorticate posturing (core; abnormal flexion)
UE in a spastic, flexed position, internal rotation (IR) and adduction
LE spastic extended, IR and adduction
Location: Cerebral hemisphere, internal capsule, above the superior colliculus
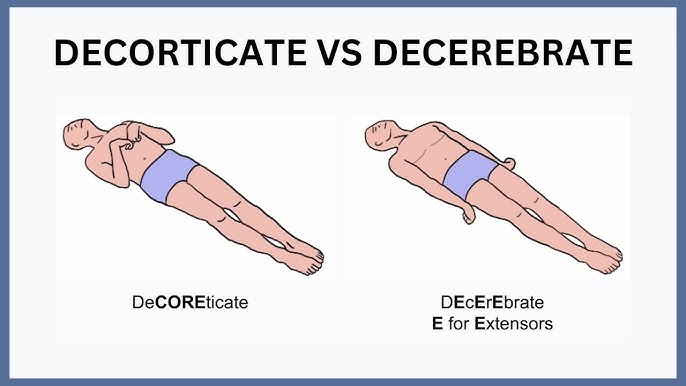
TBI: Decerebrate posturing (extensor response)
UE and LE in extension, adduction and internal rotation (IR)
wrist & fingers in flexion (lesion below the superior colliculus, brainstem region)
poorer prognosis than clients with damage above the superior colliculus
TBI: Retrograde amnesia
length of amnesia for events prior to injury
unable to remember events due to neurological damage
TBI: Anterograde amnesia
length of amnesia following impact, injury
Tnable to consolidate information for storage and retrieval
TBI: Post-traumatic amnesia
Following injury where patient is confused
seems unable to store and recall new information (can refer to anterograde or retrograde subtype)
Glasgow Coma Scale: clinical tool to assess the severity of coma and impaired consciousness; one of the most commonly used scoring systems
3 - 8: severe TBI
9 -12: moderate TBI
13 -15: mild TBI
Eye-opening, best motor response, verbal performance observed
Overall coma score: add up the total numbers (E+M+V). A total of 3 is the least responsive; the highest score is 15.
Glasgow Coma Scale: Eye opening (E)
Spontaneous-4
To speech-3
To pain-2
Nil-1
Glasgow Coma Scale: Best motor response (M)
Obeys-6
Localizes- 5
Withdraws-4
Abnormal flexion- 3 (decorticate posturing)
Extensor response-2 (decerebrate posturing)
Nil-1
Glasgow Coma Scale: Verbal performance (V)
Oriented-5
Confused conversation-4
Inappropriate words- 3
Incomprehensible sounds-2
Nil-1
Galveston Orientation & Amnesia Test (GOAT)
Measures cognitive level of patients post-injury so that a more realistic recovery plan can be communicated. Including length of stay, rehab therapy plan, and prediction of recovery information for patient’s family
LOW GOAT score: longer duration of the post-traumatic amnesic period.
An increased duration of the post-traumatic (PTA) was found in patients with diffuse or bilateral brain injuries.
The longer the confused state, the more difficult for the patient to return to pre-injury cognitive levels.
Rancho Los Amigos (RLA) Scale of Cognitive Functioning (8)
Rehab evaluation tool. Focuses on client’s abilities and behaviors. Clients move through the stages during recovery process; they can start or stop at any level, or skip a stage.
No Response
Generalized Response
Localized Response
Confused, Agitated
Confused, Inappropriate, Non-agitated
Confused, Appropriate
Automatic, Appropriate
Purposeful, Appropriate
Recovery Process, RLA 1-3: Requires…
Total Assistance
RLA 1 (Coma)
Not arousable, not responsive
Absence of awareness of self and the environment despite maximum stimuli
No periods of wakefulness in the coma state
When sedating and hypnotic medications are removed, coma rarely lasts more than weeks
Coma rarely lasts > 3 to 4 weeks unless medication induce
RLA 2: Persistent vegetative state (PVS) = Awake but unaware
No awareness of self or environment: Cannot attend, follow commands
No intelligible verbal response/communication, automatic motor response or localizing
Incontinence bowel and bladder
Positive signs
Sleep/wake cycles
Brainstem, autonomic functions: gag, swallow, cough, temperature regulation
Random vocalizations, movements
RLA 3: Minimally conscious state
Some awareness with wakefulness
Definite reproducible behavioral evidence of some awareness of self or environment
Follows commands
Gestures or verbal response to questions
Intelligible sounds
Crying, laughing, smiling to relevant stimuli
Reach/hold objects
Visual tracking
Locked-In Syndrome
Loss of voluntary motor control in a setting of preserved consciousness
Tetraplegia and bulbar weakness; vertical eye movement and blinking usually intact
Damage to corticospinal and corticobulbar pathways; lesion in basis pontis classic
May be difficult to demonstrate conscious behavior because of motor limitations
Persistent Vegetative State (PVS) = Diagnosis (Dx)
Describes past and current state
After one month in a vegetative state
Permanent (Irreversible) Vegetative State
12 months after TBI
3 months after non traumatic brain insult.
Determine level of medical support, nutrition. Advanced Directives helpful, but rarely present!
Musculoskeletal Problems from Vegetative State
Goal: allow sitting, standing, positioning
Fractures: clarify weight-bearing parameters before admission
Heterotopic ossification: abnormal bone growth in soft tissue
Symptoms 2-8 weeks post injury, usually detected by therapists, nurses, families
X-rays, triple phase bone scan
NSAIDs for pain, inflammation
IV etidronate-oral for 6 to 9 months to prevent further bone deposits
ROM: continuous passive motion
RLA 1-3: Wheelchair positioning
Prevent deformity
Tone normalization
Pressure management
Promote function
Increase sitting tolerance
Enhance respiratory function
Provide proper body mechanics
Dynamic head positioning device provides alignment & freedom of movement, promotes function
RLA 1-3: Spasticity Management = goal to normalize tone w/ minimal daytime sedation
Position in bed, chair
Sitting/standing opportunities: two people treatment
Neuromuscular blocks plus casting
phenol: motor points for large muscles, musculocutaneous nerve (biceps), obturator nerve (thigh adductors)
Bupivacaine: any nerve, allows immediate casting in relaxed position
Botulinum toxin: every three months, small to medium sized muscles
Systemic medications
Dantrolene, baclofen
Intrathecal baclofen pump after 4 to 6 months
Positioning and casting consume the most time and resources: early treatment makes a difference by reducing the need!
RLA 1-3: only cast when…
Splinting has failed to control severe tone or contractures from developing
Positional cast is necessary for continued use (bivalve, cut in 2 and easily removable cast)
Range of motion is decreased and prolonged stretches necessary
RLA 1-3: Consequences of Lack of Intervention
Contractures
Limited head and trunk control
Increased caregiver assistance
Limited participation in daily occupations, limited mobility
Transportation difficulties
Recovery Process: RLA 4-6
Confused
RLA 4/IV: Confused/Agitated (Max A)
Alert and often a heightened level of activity
Purposeful attempts to remove tubes, restraints, or crawl out of bed
Absent short-term memory
May cry or scream out of proportion to stimulus
May exhibit aggressive and/or flight behavior
Wide mood swings with no apparent relationship to environmental events
Require max A
RLA IV/4: Behavior management program
provide an environment that motivates patients to participate in a comprehensive rehab program at their optimal capacity
To integrate family members into the rehab team and treatment plan development process
To maintain a safe environment through a multifaceted safety program
minimize the use of all restrictive modalities
Provide education to patients, family, and staff
To identify patients with substance use disorders and initiate specialized treatment
RLA IV/4: Behavior management interventions - Environment 👂
Decreased auditory and visual stimulation
Reduce noise levels ( TV, staff communication)
Provide consistency and structure
Know the patient’s care plan and unique behaviors
RLA IV/4: Behavior management interventions - Communication/interaction 💬
Model behaviors for the patient
Speak calmly, slowly, and in simple sentences
For agitated/restless patients that want to walk, do not restrain them. Walk with them, this will help calm patient
Give praise and attention for the desired behavior when it occurs
Do not reinforce undesirable behavior
Redirect patients when they’re agitated or perseverating
Provide choices whenever possible
RLA 5/V: Confused, inappropriate, non-agitated
Alert but not agitated
Not oriented to person, place, or time
Frequent periods of non-purposeful sustained attention
Unable to learn new material
Able to respond to simple commands fairly consistently with external cues
Able to converse on a social automatic level for brief periods of time
Verbalizations about present events often inappropriate and confused
Requires max A
RLA 6/VI: Confused, appropriate
Inconsistently oriented to person, place and time
Remote memory more accessible than recent memory
Able to use assistive memory devices with max A
Supervision needed for execution of previously learned tasks (self-care)
Shows carry over for relearned familiar tasks (self-care)
Unaware of impairments, disabilities, safety risks
Requires mod A
RLA 7-8: Automatic, purposeful
Recovery process ✅
RLA 7/VII: automatic, appropriate (min A)
Consistently oriented to person, place and time
Increased attention and able to work for 30 minutes on highly familiar tasks
Minimal supervision for new learning
Initiates and carries out familiar self-care and household tasks but may have limited memory of events
Unrealistic planning for the future
Overestimates abilities
Unable to think about consequences
Unaware of others’ needs and feelings
Requires min A for ADLs
RLA 8/VIII: Purposeful, appropriate (standby A)
Consistently oriented to person, place and time
Attention increased to 60 minutes for familiar tasks
Able to recall past events and integrate with recent events
Initiates and carries out steps for familiar personal, household, community, work, and leisure routines and can slightly modify a plan when needed with minimal assistance
Requires no assistance once a new task/activity is learned
Needs assistance to make corrective measures when a plan needs substantial alterations
Thinks about consequences of actions
Irritable and depressed
Acknowledges others’ needs and feelings
Requires stand-by A (SBA)/supervision
Involuntary Movement Disorders
Occur most often from damage to the basal ganglia structure
Movements occur at rest and may also be seen during volitional tasks
Involuntary Movement Disorders: Chorea
quick, jerky, involuntary movements; seen with damage to the caudate nucleus
Involuntary Movement Disorders: Hemiballism
flailing, ballistic movements (rare); seen with damage to the subthalamic nucleus
Involuntary Movement Disorders: Athetosis
slow, sinuous movements; general damage to basal ganglia
Involuntary Movement Disorders: Dystonia
slow, twisting, contorted movements; general damage to basal ganglia
Involuntary Movement Disorders: Resting tremor (person @ rest)
Damage to substantia nigra
Involuntary Movement Disorders: Clonus
Involuntary, rhythmic muscular contractions & relaxations caused by neurological conditions (ALS, brain injury, CVA, CP, etc) due to upper motor neuron lesions involving descending motor pathways
To test: Hold the ball of the client's foot
Quickly dorsiflex the foot and then release pressure but DON’T let go of the foot
Observer/feel for alternating movement of dorsiflexion and plantarflexion of the foot after this stimulus
Voluntary Movement Disorders
occur at rest; related to damage of the cerebellum where the grading of movement is compromised
poor control of agonist/antagonist during the movement
Voluntary Movement Disorders: dysmetria
inability to correctly estimate ROM needed (overshooting/undershooting a target)
Voluntary Movement Disorders: Dysdiadokokinesia
Impairment of the ability to make rapid alternating movements
Voluntary Movement Disorders: Ataxia
delayed initiation, poor coordination, lack of smooth movement, wide-based gait
Voluntary Movement Disorders: Intention tremor
tremor triggered by movement toward an object
Voluntary Movement Disorders: Hypotonia
low tone that impacts movement
Voluntary Movement Evaluation: Cerebellar coordination tests
Finger to nose
Heel to shin
Thumb to fingertip
Diadochokinesia: alternating pronation/supination
Gait assessed by PT. OT concerned about energy expenditure with abnormal gait and safety; but the PT provides intervention to correct gait deviations