Palliative Medicine and End of life care
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
What medications are associated with preventable hospital admissions?
Warfarin
Insulin
NSAIDs
Digoxin
Antihypertensives
Benzodiazepines
Oral hypoglycaemics
Methotrexate
Opiated
Drugs with a narrow therapeutic window e.g. lithium, digoxin, carbamazepine →narrow but not as narrow as others
injectable or enternal medicines
Conditions associated with preventable admissions include
COPD/Asthma
Parkinson’s disease
Diabetes
Pharmacists should look out for adherence issues, a new request for compliance support or if there are social, physical or cognitive impairments
What is a clinical risk?
A clinical risk includes the disease type e.g. COPD/ heart failure/ asthma
What is a medicine related risk?
E.g. inadequate monitoring, drug adverse reactions which are associated with increased risk of admission
What is a social risk?
Social risk comes from patients who are not independent, immobile, reliant on care of others for daily activities. Many individuals require support at home and not all carers can provide support with medicines
What is the COM-B model?
This explains patient behaviour and is applied to medicine adherence, smoking cessation etc to better understand why patient does (or does not do) a particular behaviour
Capability - e.g. is the patient able to take the medication? Physical ability to open tablets? Swallow tablets? Use inhalers? Psychological ability to understand how to take medicines?
Opportunity - Quality of healthcare communication e.g. poor consults mean the patient may lack the opportunity to follow instructions. Religious or cultural beliefs that affect whether or not to take the medication.
Motivation - whether the patient wants to take their medications, driven by reflective motivation and how the patient thinks about their treatment e.g. patients will have an opinion on statins before they take it
Behaviour - this all affects behaviour
Name different aids to help medicine taking.
pill crusher
Multi-compartment aids MCAs
tablet crusher
blister popper
pill timers and alarms
devices to help administer eye drops
Why is polypharmacy a concern?
Good medicine reviews can prevent hospital admission. The more medicine a patient takes, the more potential for adverse effects which increases the risk for hospital admission. Polypharmacy increases the risk of drug interactions.
The more medicines a patient takes, the more likely they will become non-adherent
Cost burden
Increased risk of falls in elderly
Elderly patients / frail patients are at risk due to physiological variations such as weight, body mass, renal function, cancer etc - can all effect drug metabolism, drug distribution, excretion etc.
What is meant by deprescribing?
This is the planned and supervised process of dose reduction or the stopping of a medication that might be causing harm or is no longer needed/ of any benefit. Deprescribing is part of good prescribing - backing off when doses are too high or stopping medications that are no longer needed.
Active participation from the patient is required
What are the most common medications associated with adverse drug effects?
opioid analgesics
NSAIDs
Anticholinergics
Benzodiazepines
Cardiovascular agents, CNS agents and musculoskeletal agents
What are the principles of prescribing in the elderly?
Avoid prescribing prior to diagnosis
Start with a low dose and titrate slowly
Avoid starting 2 agents at the same time
Reach therapeutic dose before switching or adding agents
Consider non-pharmacological agents
What is social care?
This is the personal care that people need, which is provided in the community home, allowing people to live in their preferred place. Help with getting dressed, cleaned etc. It the person does not recieve the appropriate social care then they will end up being admitted to the hospital.
Is medicine administration in the community a health or social care task?
Everyone has a role in this, pharmacists, the providers of the services, commissioners who assess properly etc. We would administer medication e.g. oral but if it is PEG, S/C or rectal route, then healthcare concern to help with administration.
What happens when organisations only allow carers to give medicines from MDS?
Some oral medicines cannot go into MDS e.g. due to stability issues
PRN medicines in MDS may be given when they are not needed at that time. e.g. patient has UTI and prescribed antibiotics, community pharmacy delivers medication in original packaging and because they are not in trays the carer cannot give it to them.
This means in this case the carer has to support/ encourage the patient to take the medicine themselves and the carer not to document this as its technically not allowed
This will be problematic if the patient lacks the ability to take thier medication
What is needed to overcome the issue with organisation requiring MDS?
Training to administer all medicines safely
Clear understanding of benefits and risks of using an MDS system
Agencies requiring the use of MDS should establish formal contracts with community pharmacies to provide medicine support.
What are environmental causes of falls?
rugs
doormats
slippery stairs
wet floors
slipper baths
lives alone
alcohol
What are muscular causes of falls?
muscle weakness
arthritis
spinal disease
pain
use of walking aids
What are the neurological causes of falls?
medication
stroke
epilepsy
parkinsons disease
dementia
neuropathy
depression, anxiety
Name medications which increase risk of falls
BZDs
Zopiclone
Sedating antihistamine
Dopamine agonists
Alpha blockers
Anti-anginals
All work on the circulation to increase risk of falls - can lead to sedation, hypotension, postural hypotension, bradycardia, tachycardia, ortostatic hypotension
What are the current roles of pharmacists in care homes?
supply
medication handling
wastage reduction
storage
training
information and advice
medicine reviews
prescribing
parent/ family discussions
Pharmacists have key role in communication when transferring between care providers, community pharmacy can provide information to secondary care and vice versa
What is the discharge medicine review service?
This allows community pharmacists to review discharge medicines to help patients understand discharge processes.
In palliative care, what medications would we consider deprescribing?
Aspirin - for primary prevention - no longer needed now as we are preventing something that is a long-term issue. Only placing the burden of medicine
lipid-lowering medication - deprescribe
Blood pressure - no longer worried about this in palliative care
Anti-ulcer medication
Oral hypoglycaemics / anti-diabetic medications - risk of fall decreases
Osteoporosis - risk of falls is low when palliative
Vitamins/ minerals - can do without, not really required
Medicines can always be restarted if required
What do we mean by palliative care?
This is an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessments and treatment of pain and other problems, physical, psychological or spiritual
What are conditions that would be considered life-threatening?
cancer
motor neuron disease
dementia
parkinsons
multiple sclerosis
stroke
frailty
heart failure
COPD
Pulmonary fibrosis
renal failure
liver failure
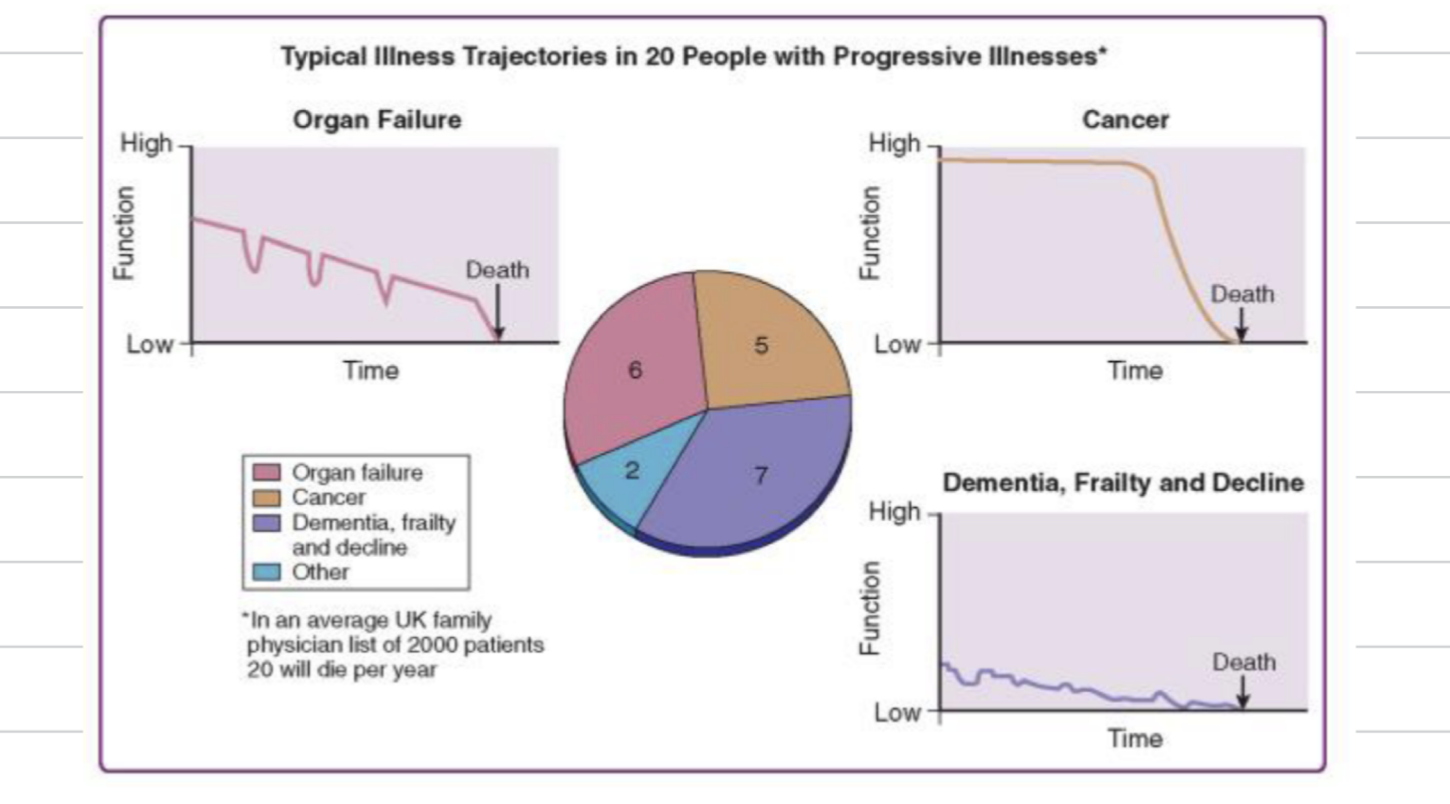
For each of the following, explain the decline in patients before death occurs
Organ failure
Cancer
Dementia & Frailty
Organ failure - steady decline over time, patients become more frail and have an acute crisis period where they are hospitalised
Cancer - patients remain function for sometime and then rapid decline before death
Dementia, frailty - function is low before decline and death
How do we know if a patient needs palliative care? What conversations do we need to have?
Would we be surprised if this patient dies in the next 6 months?
Assess the patient, family, and dependents including children for supportive and palliative care needs
review treatment and medication priorities
consider patient for general practice palliative care register
consider advance care plan discussion with patient and family - e.g. organising where the patient will be when they die.
What are clinical indicators that someone is dying?
Performance status is poor - limited self care - in bed / chair 50% of the day or deteriorating
Progressive weight loss over the past 6 months
two or more unplanned admissions in the past 6 months
a new diagnosis of progressive, life limiting illness
two or more advanced or complex conditions
Patient is in a nursing care home or NHS continuing care unit or needs more care at home
How would you describe someone’s breathing, blood pressure, pulse rate, and renal function
Breathing - breathlessness or chest pain at rest
Blood pressure - systolic reading less than 100mmHg
Pulse rate - over 100
Renal impairement - less than 30 ml/min
Heart failure also - severe valve or corary artery disease
What symptoms do patients get when they die and what medicines do we use?
Pain - opioids - morphine/ oxycodone
Breathlessness - opioids or midazolam
Agitation / restlessness - Midazolam / levomepromazine
Nausea and vomiting - cyclizine, metoclopramide, haloperidol
Respiratory secretions - Hyoscine hydrobromide, glycopyrronium
Dry/sore mouth - biotene toothpast
pressure areas - pressure relieving mattresses
What formulation do medications need to be for palliative care?
Medications need to be injectables suitable for subcutaneous route
How are palliative care medications administered?
Given via syringe driver
What is anticipatory prescribing?
typically seen in community pharmacy
typically on friday afternoon so patient have medications at home if they die over the weekend
Medication will be ampoules e.g.
morphine sulphate 10mg/ml - 5mg to be used subcutaneously as directed - supply 10 ampoules
Midazolam injection 10mg/2ml - 5mg to be used subcutaneously as directed - supply 10 ampoules
Hyoscine hydrobromide injection 400mcg - as directed - supply 3 ampules
Levomepromazine injection 25mg/ml - as directed - supply 5 ampoules
haloperidol injection 5mg/ml - as directed - supply 5 ampoules
water for injection as directed - supply 5 ampoules