what is malnutrition?
a state of nutrient imbalance where energy (calories) intake either exceeds (overnutrition/obesity) or does not meet energy needs (undernutrition)
is malnutrition most often associated with overnutrition or undernutrition?
undernutrition
undernutrition can occur due to:
inadequate intake, poor absorption, and increased utilization of energy
how is starvation-related malnutrition defined
a prolonged duration of inadequate intake or feeding intolerance
what is typically a chronic process with unintentional weight loss
starvation-related malnutrition
what may influence starvation-related malnutrition?
behavioral, socioeconomic, and environmental factors
Instances of starvation-related malnutrition
inadequate food supply, anorexia nervosa or disordered eating patterns, major depression, and feeding aversions
how is disease-related malnutrition defined
disease associated with an inflammatory state which results in increased energy (calories) or protein needs
what is chronic disease-related malnutrition?
lasting for 3 or more months with mild-moderate degree of inflammation
Instances of chronic disease-related malnutrition
inflammatory bowel disease, cancer, organ failure, cystic fibrosis, and malabsorption
what is acute disease-related malnutrition?
lasting for < 3 months with severe degree of inflammation
Instances of acute disease-related malnutrition:
burns, trauma, traumatic brain injury, major surgery, serious infection
How to diagnose malnutrition
Has there been a recent weight loss of at least 5-10%?
Has there been inadequate intake for at least 1-2 weeks
if either criteria is matched→ patient should be referred for full nutritional assessment
Patient history malnutrition risk factors:
acute/chronic inflammatory diseases associated with malnutrition
socioeconomic factors that may result in food insecurities or reduced intake
altered absorption of nutrient
medications
poor nutritional habits
alcohol/substance abuse
what is the other name for actual body weight (ABW)
total body weight (TBW)
how to convert from pounds to kg
1 kg = 2.2 lbs
IBW equation for males formula
50 kg + (2.3 kg * total inches > 60)
IBW equation for females formula
45.5 kg + (2.3 * total inches > 60)
how to calculate Adjusted body weight (AdjBW)
IBW + (0.4 * (TBW-IBW))
how to calculate BMI from kgs
weight (Kg) / height (m2 )
how to calculate BMI from lbs
[weight (pounds) / height (inches2 )] * 703
how to calculate % difference ABW vs. IBW
(ABW/IBW) * 100%
what is the BMI for underweight category
< 18.5
what is the % difference for the underweight category
ABW is < 90% IBW
what is the BMI for normal/healthy category
18.5 - 24.9
what is the % difference for the normal/healthy category
ABW is 90-120% IBW
what is the BMI for the overweight category
25-29.9
what is the % difference for the overweight category
ABW is > 120 to < 150%
what is the BMI for the obese (Class I + Class II) category
30-39.9
what is the % difference for the obese (Class I + Class II) category
ABW is ≥ 150 to < 200%
what is the BMI for the severe obesity (Class III) category
≥ 40
what is the % difference for the severe obesity (Class III) category
ABW is ≥ 200% IBW
What are the subcategories of underweight?
Mild malnutrition, moderate malnutrition, and severe malnutrition
what is the BMI for the mild malnutrition subcategory
17-18.5
what is the % difference for the mild malnutrition subcategory
ABW is 80-89% IBW
what is the BMI for the moderate malnutrition subcategory
16-16.9
what is the % difference for the moderate malnutrition subcategory
ABW is 70-79% IBW
what is the BMI for the severe malnutrition subcategory
< 16
what is the % difference for the severe malnutrition subcategory
ABW is < 69% IBW
what is the criteria for malnutrition diagnosis
1. Reported insufficient intake of calories (energy) (at < 75% of daily needs for at least 1-2 weeks)
2. Recent unintentional weight loss (loss of at least 10% of body weight in 6 months or 5% in 1 month)*
3. Decreased muscle mass
4. Decreased subcutaneous fat
5. Fluid accumulation
6. Decreased functional status (such as grip strength)
Note: the first two are a Simplified approach to screening; if yes to either then refer for full nutritional assessment
what is the principle “start low, go slow” utilized in?
treatment of severe malnutrition
why is start low, go slow utilized in malnutrition?
to ensure medical stabilization and prevent refeeding syndrome
what is refeeding syndrome?
occurrence of electrolyte abnormalities in severely malnourished patients during initiation of nutritional supper (calories) in an individual who has been exposed to undernourishment for a substantial amount of time
why is refeeding syndrome dangerous
initiation of nutritional therapy, containing glucose shifts to anabolic state→ insulin release will drive electrolytes intracellularly
potassium, phosphate, and magnesium; hypo!
Total energy expenditure (TEE) calculation
patient’s BEE, plus their additional metabolic needs(BEE* activity*stress)
Activity Factors
Confined to bed = 1.2
Out of bed, ambulatory = 1.3
Stress Factors:
Minor surgery = 1.2
Infection = 1.4
Major trauma, sepsis, burns 0-30% BSA = 1.5
Burns > 30% BSA = 1.5 to 2
what are the activity factor values for patients confined to bed
1.2
what are the activity factor values for patients out of bed, ambulatory?
1.3
what are the stress factor values for patients getting minor surgery
1.2
what are the stress factor values for patients with infections
1.4
what are the stress factor values for patients with major trauma, sepsis, and burns 0-30% BSA
1.5
what are the stress factor values for patients with burns > 30% BSA
1.5-2.0
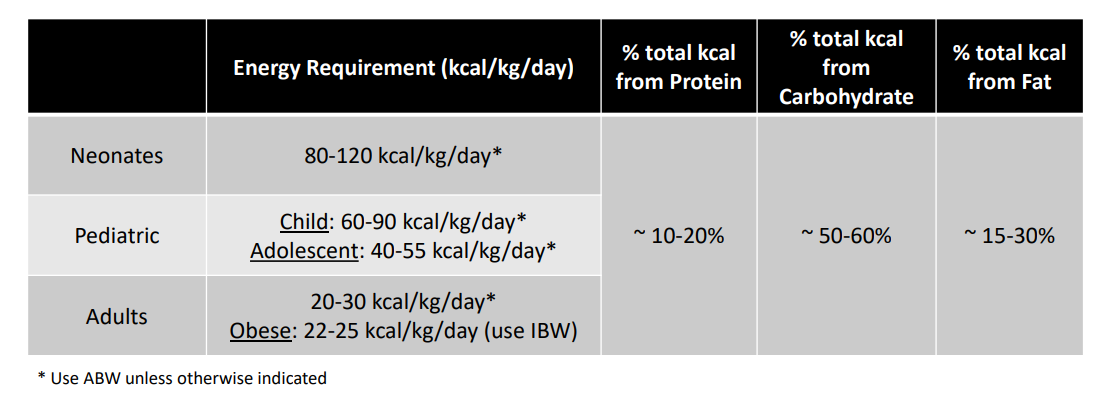
How to calculate a patients energy goals?
Use the aspen tables:
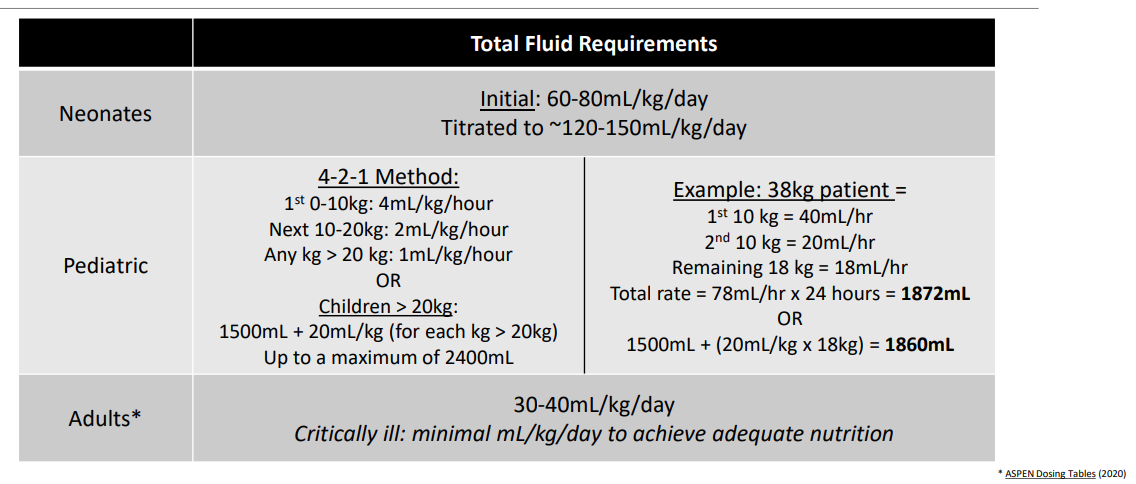
How to calculate fluid goals/requirements?
Use aspen tables:
which patient specific factor needs increased energy (kcal) goals?
critically ill (infection, burns, trauma)
which patient specific factor needs decreased fluid than goal?
Kidney dysfunction and heart failure
T/F: utilization of supplemental nutrition is based on patient-specific assessment rather than a diagnosis of presence of a particular disease state
true
what needs to be evaluated to determine route of administration of nutritional supplementation?
feasibility of utilizing the gut
what is parenteral nutrition reserved for?
if intestinal tract is not functional/unable to access and instances where energy needs/goals are greater than what the patient can tolerate
what is the order of nutritional supplementation
oral intake —→ enteral nutrition (via tube) ——> parenteral nutrition (intravenous)
Guidelines for Starting Enteral Nutrition (EN) in Hospitalized Patients:
If patient is:
High-Risk, in the ICU or Malnourished Patients: Start EN within 24–48 hours of hospital admission, including in the ICU.
If patients are well-nourished, have low risk, and likely to start eating within 5–7 days: EN can be delayed.
Caution in Specific Cases: For patients at risk of refeeding syndrome or with digestive symptoms, introduce EN slowly and carefully.
Malnourished: less than 75% of daily requirements
What needs to be noted about EN therapy?
Caution in patient with metabolic instability – delay until patient condition improving
when to start Parenteral Nutrition (PN) in adults:
Well-Nourished, Stable Adults: If they cannot take enough enteral nutrition (EN), start PN after 7 days.
Nutritionally-at-Risk Patients: If they’re unlikely to meet their nutrition goals with EN, start PN within 3–5 days.
Moderate-to-Severe Malnutrition: If EN isn’t possible, start PN as soon as possible.
What qualifies someone as being nutritionally at risk?
Unintentional weight loss of 10% in 6 months or 5% in 1 month
BMI less than 18.5 kg/m²
High metabolic needs
Modified or restricted diets
Indications for PN in Pediatrics
• Infants: Initiate within 1-3 days* if unlikely to tolerate EN for extended time
• Children/Adolescents: Initiate within 4-5 days* if unlikely to tolerate EN for extended time
Why do pediatric patients have shorter times to initiation for PN?
Decreased metabolic stores/reserves available
Higher energy requirements
Indications for PN in Neonates
neonates are between 0-28 days old
Very-low birth weight neonates (< 1.5kg): Initiate promptly after birth
Indication for preterm and critically ill term neonates→ Initiate when EN unable to meet energy requirements for growth
What is there to know about PN treatment in neonates
Essential fatty acid deficiency can develop if fat is withheld from diet for 3 days
What conditions do you use Parenteral nutrition?
Impaired absorption→ short bowel syndrome, gastroschisis, intestinal fistula
Mechanical/motility issues→ bowel obstruction, ileus, inflammatory disease
Bowel reset→ pancreatsis, ischemic bowel, pre/post operative
inability to use gut→ low weigh neonate, low BP, severe bleeding

