PR2154 IC10 Allergic rhinitis
0.0(0)
Studied by 0 peopleCard Sorting
1/68
Earn XP
Description and Tags
Last updated 5:50 PM on 3/11/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
1
New cards
What is rhinitis?
Symptomatic inflammation of the inner lining of the nose
* rhinorrhea
* sneezing
* nasal congestion
* nasal itch
>2 consecutive days >1h each
* rhinorrhea
* sneezing
* nasal congestion
* nasal itch
>2 consecutive days >1h each
2
New cards
Which part of the nose is inflammed in rhinitis?
The inner lining
3
New cards
What are the types of rhinitis?
Allergic Rhinitis
Infectious Rhinitis
Non- Allergic rhinitis
Infectious Rhinitis
Non- Allergic rhinitis
4
New cards
What are some causes behind non-allergic rhinitis?
Drug induced
Hormonal changes (pregnancy, menstrual cycle)
Idiopathic or vasomotor (strong smell or change in temp)
Structural (septal deviation, polyps)
Traumatic
Hormonal changes (pregnancy, menstrual cycle)
Idiopathic or vasomotor (strong smell or change in temp)
Structural (septal deviation, polyps)
Traumatic
5
New cards
What are some drugs that can use drug induced non-allergic rhinitis?
NSAIDs
Antihypertensive
Oral contraceptive
prolonged use of topical congestants (rhinitis medicamentosa)
antidepressants
sedatives
Phosphodiesterase 5 inhibitor (for ED)
Antihypertensive
Oral contraceptive
prolonged use of topical congestants (rhinitis medicamentosa)
antidepressants
sedatives
Phosphodiesterase 5 inhibitor (for ED)
6
New cards
Which immunoglobulin causes allergic rhinitis?
Induced after allergen exposure by an IgE mediated inflammation of the membrane lining the nose
7
New cards
What are the types of allergic rhinitis?
Seasonal (SAR) → cyclical exacerbation
Perennial (PAR) → year round symptoms
Perennial (PAR) → year round symptoms
8
New cards
What are the types of allergens?
**Outdoor allergens → seasonal**
* pollen (trees, grasses, flowers etc)
* Mould spores
**Indoor allergen**
* Dust mites (chemical in their faeces)
* animal dander
* cockroaches
* mould spore (house plants)
* cigarette smoke
**Occupational allergen**
* wood dust
* latex
* resins
* chemical (isocyanate, glutaraldehyde)
**Ingested allergens**
* wheat
* eggs
* milk
* nuts
* pollen (trees, grasses, flowers etc)
* Mould spores
**Indoor allergen**
* Dust mites (chemical in their faeces)
* animal dander
* cockroaches
* mould spore (house plants)
* cigarette smoke
**Occupational allergen**
* wood dust
* latex
* resins
* chemical (isocyanate, glutaraldehyde)
**Ingested allergens**
* wheat
* eggs
* milk
* nuts
9
New cards
What is the pathology underlying allergic rhinitis?
Exposure to allergen → CD4+ TH2 activated B cells activated → allergens bind to allergen specific IgE (produced by B cells) → crosslinking with IgE receptor on mast cells
→ **1. Mast cell degranulation**
* Protease
* Histamine → itching, paroxysmal sneezing, vasodilation, plasma exudation
→ 2. **Mast cell activation**
* PGDs → rhinorrhea
* Kinins (bradykinins) → itchy sore throat
* neuropeptides → vasodilation
* all contribute to nasal congestion
→ **1. Mast cell degranulation**
* Protease
* Histamine → itching, paroxysmal sneezing, vasodilation, plasma exudation
→ 2. **Mast cell activation**
* PGDs → rhinorrhea
* Kinins (bradykinins) → itchy sore throat
* neuropeptides → vasodilation
* all contribute to nasal congestion
10
New cards
11
New cards
What are some classical symptoms of allergic rhinitis?
Rhinorrhea (clear and watery)
Nasal congestion
Sneezing (usually paroxysmal)
Puritis of ears, eyes and nose
* symptoms usually worse in the morning and at night
* gets better in day
Nasal congestion
Sneezing (usually paroxysmal)
Puritis of ears, eyes and nose
* symptoms usually worse in the morning and at night
* gets better in day
12
New cards
What are some other manifestation of allergic rhinitis?
Post nasal drip (can cause sore throat)
Ophthalmic symptoms (itch, irritation, allergic conjunctivitis)
Headache
Pain
Nose bleed
Ophthalmic symptoms (itch, irritation, allergic conjunctivitis)
Headache
Pain
Nose bleed
13
New cards
What are some face features of allergic rhinitis?
Allergic shiners (black under eye)
Dennie-Morgan folds (line under eye)
Allergic crease (line on nose)
Dennie-Morgan folds (line under eye)
Allergic crease (line on nose)
14
New cards
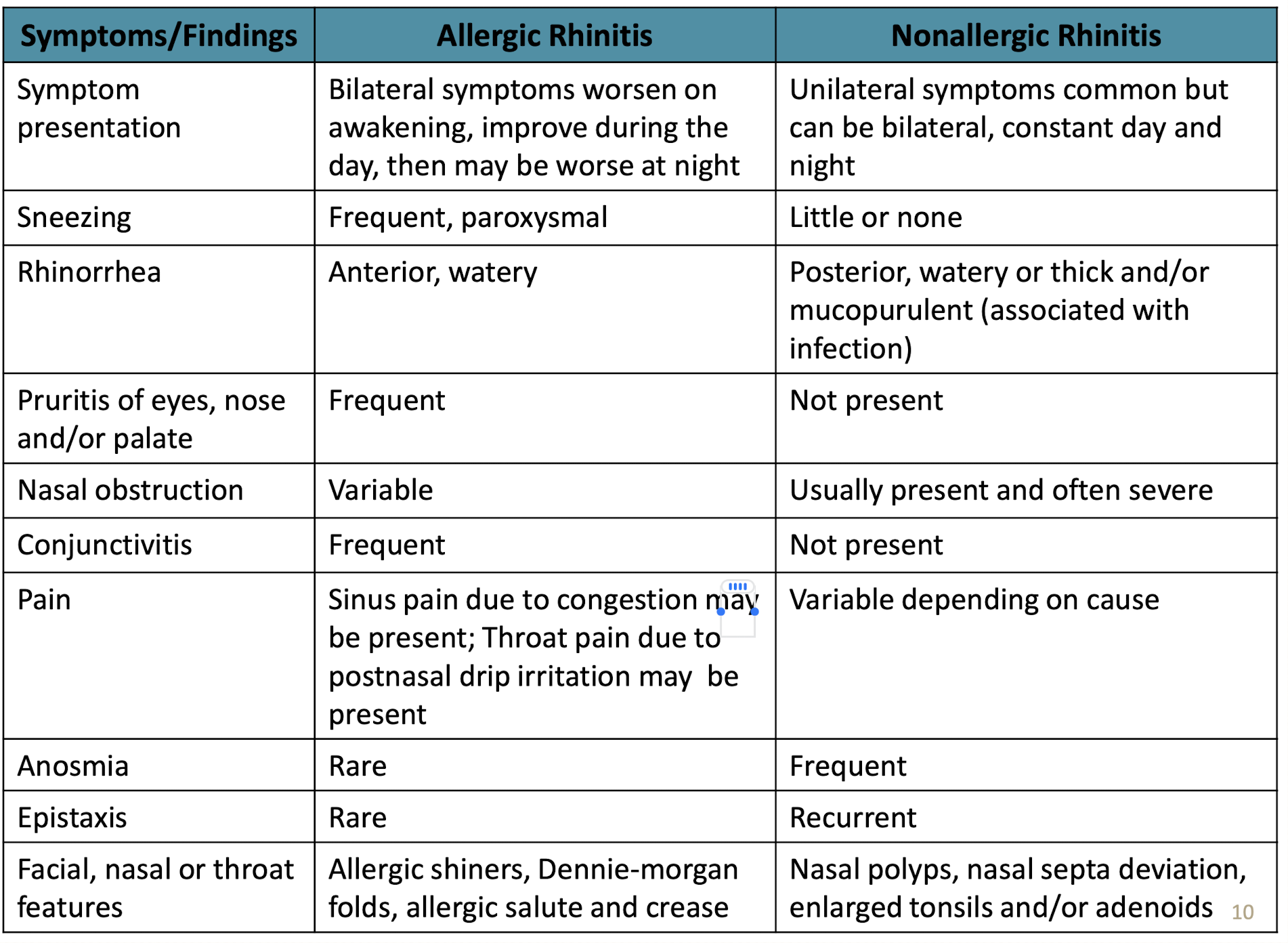
What are some indicative differences between Allergic rhinitis and non-allergic rhinitis?
\
15
New cards
What are some risk factors for allergic rhinitis?
Environmental
* pollution
* irritants
Exposure to allergens
Genetic and family history
* Family history of atopy (asthma, atopic dermatitis)
* Filaggrin gene mutation (impaired skin protective barrier due to lack of filaggrin protein)
\
* pollution
* irritants
Exposure to allergens
Genetic and family history
* Family history of atopy (asthma, atopic dermatitis)
* Filaggrin gene mutation (impaired skin protective barrier due to lack of filaggrin protein)
\
16
New cards
What are the conditions closely related to allergic dermatitis?
Asthma
Atopic dermatitis
The atopic march → allergic triad
Atopic dermatitis
The atopic march → allergic triad
17
New cards
What are the associated conditions patients suspected of allergic rhinitis should be assessed on?
Sinusitis
Eustachian tube dysfunction
Otitis media
Sleep apnea (due to nasal congestion)
Dentofacial abnormalities
Eustachian tube dysfunction
Otitis media
Sleep apnea (due to nasal congestion)
Dentofacial abnormalities
18
New cards
What are the classifications of allergic rhinitis?
Mild Intermittent, Moderate to severe Intermittent (IAR)
Mild persistent, Moderate to severe persistent (PER)
Mild persistent, Moderate to severe persistent (PER)
19
New cards
What is classified as Mild intermittent allergic rhinitis?
20
New cards
What is classified as Moderate to severe intermittent allergic rhinitis?
21
New cards
What differentiates between mild and moderate to severe?
As long as it affects QOL, it is moderate to severe
22
New cards
What is classified as mild persistent allergic rhinitis?
>4 days per week **AND** > 4 weeks per stretch
\
**NO impairment on quality of life:**
* normal sleep
* no impairment of daily activities, sport, leisure
* Normal work and school
* No troublesome symptoms
\
**NO impairment on quality of life:**
* normal sleep
* no impairment of daily activities, sport, leisure
* Normal work and school
* No troublesome symptoms
23
New cards
What is classified as a moderate to severe persistent rhinitis?
>4 days per week **AND** > 4 weeks per stretch
\
**Affects one or more Quality of life:**
* Abnormal sleep
* Impaired daily activities, leisure, sports
* Impacts school and work
* troublesome symptoms
\
**Affects one or more Quality of life:**
* Abnormal sleep
* Impaired daily activities, leisure, sports
* Impacts school and work
* troublesome symptoms
24
New cards
What differentiates between intermittent and persistent?
4 days per week 4 weeks per stretch rule
25
New cards
How do we diagnose allergic rhinitis?
History
* symptoms
* temporal patterns
* **allergen history and family history**
Examinations
Allergy testing
* prick test
* radioallergoabsorbent tests for specific IgE (RAST)
* Nasal allergen challenge
* symptoms
* temporal patterns
* **allergen history and family history**
Examinations
Allergy testing
* prick test
* radioallergoabsorbent tests for specific IgE (RAST)
* Nasal allergen challenge
26
New cards
According to ARIA 2008, what is suggestive of allergic rhinitis?
2 or more of the following symptoms for >1hr on most days:
watery rhinorrhea
Sneezing, esp paroxysmal
Nasal congestion
Nasal pruritis
conjunctivitis
watery rhinorrhea
Sneezing, esp paroxysmal
Nasal congestion
Nasal pruritis
conjunctivitis
27
New cards
When should you refer the patient to the specialist/physician?
**Special population**: Children<12y, pregnant women (unless approved by doctor)
**Symptoms of non-allergic rhinitis**
Symptoms of other associated conditions
Undiagnosed or uncontrolled **asthma, COPD** or other lower resp tract infection **LRTI**
Moderate or severe persistent allergic rhinitis
**Not responding** to treatment
Severe or unacceptable side effects of treatment
Medication induced rhinitis
**Symptoms of non-allergic rhinitis**
Symptoms of other associated conditions
Undiagnosed or uncontrolled **asthma, COPD** or other lower resp tract infection **LRTI**
Moderate or severe persistent allergic rhinitis
**Not responding** to treatment
Severe or unacceptable side effects of treatment
Medication induced rhinitis
28
New cards
What are some non-allergic rhinitis symptoms that render referral?
Unilateral symptoms
Mucopurlent discharge
facial pain
anosmia
Fever>38
Infection
Nasal obstruction with no other symptoms
Mucopurlent discharge
facial pain
anosmia
Fever>38
Infection
Nasal obstruction with no other symptoms
29
New cards
What do you need to do when assessing a patient suspected of allergic rhinitis?
1. Assess signs and symptoms
1. Nature
2. Severity
3. Duration
4. Onset
5. location
6. Aggravating / remitting factors
7. Presence of other associated symptoms
2. Gather age, history of allergen exposure, family history of atopy, medical history
3. Check for pregnancy and lactation
30
New cards
What are some questions to ask on the nature of the symptoms?
Sneezing? → how much
Rhinorrhea? → nature of discharge
Itchy eyes? Nose? ears?
Nasal congestion?
Bilateral or Unilateral
Rhinorrhea? → nature of discharge
Itchy eyes? Nose? ears?
Nasal congestion?
Bilateral or Unilateral
31
New cards
What are the situations that require urgent referral?
Shortness of breath (SOB)
Uncontrolled asthma
High fever
Severe headache or eye pain
Uncontrolled asthma
High fever
Severe headache or eye pain
32
New cards
What are the options for allergic rhinitis management?
1. Allergen avoidance & Environmental control
2. Pharmacotherapy
3. Immunotherapy
33
New cards
What are some ways patients can avoid and control **House dust mites allergen?**
Remove dust
* no dust collecting items (carpet, soft toys)
* no carpets
Protect patients
* encase bedding with impermeable covers
Control mites
* wash bedding with hot cycles >55
* vaccuum with HEPA filter
* Acaricides
* Maintain humidity 35-50%
* no dust collecting items (carpet, soft toys)
* no carpets
Protect patients
* encase bedding with impermeable covers
Control mites
* wash bedding with hot cycles >55
* vaccuum with HEPA filter
* Acaricides
* Maintain humidity 35-50%
34
New cards
What are some ways patients can avoid and control **cockroaches allergens?**
Careful food prep
Put food away, wash dishes, garbage tightly sealed
Use cockroach trap
Professional help
Put food away, wash dishes, garbage tightly sealed
Use cockroach trap
Professional help
35
New cards
What are some ways patients can avoid and control **pets danders allergens?**
Remove pet
if not:
* keep pet out of house
* keep pet out of bedroom
* keep pet in uncarpeted room with HEPA filter
* Wash pet frequently
* Wash hands after handling animal
if not:
* keep pet out of house
* keep pet out of bedroom
* keep pet in uncarpeted room with HEPA filter
* Wash pet frequently
* Wash hands after handling animal
36
New cards
What are some ways patients can avoid and control **moulds allergen?**
Remove potted plants
Remove visible molds
Dry or remove wet carpets
Fix leaks
Ensure adequate ventilation
Control humidity
Remove visible molds
Dry or remove wet carpets
Fix leaks
Ensure adequate ventilation
Control humidity
37
New cards
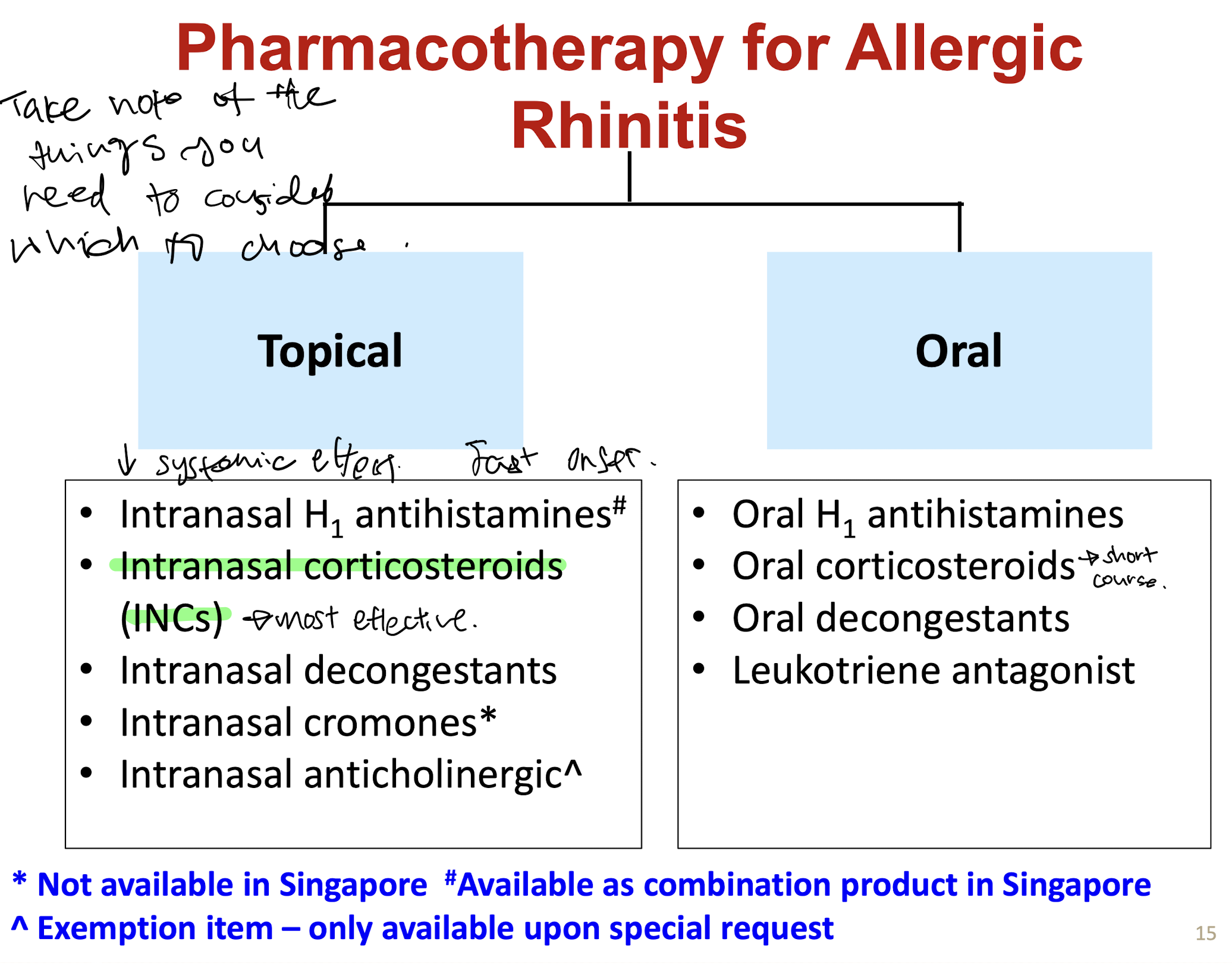
What are the pharmacotherapy available for allergic rhinitis?
38
New cards
What are the topical pharmacotherpy options available?
Intranasal H1 antihistamine (as combination)
Intranasal Corticosterioids (INC) → most effective
Intranasal decongestants
Intranasal cromones (not in SG)
Intranasal anticholinergics (exemption item)
Intranasal Corticosterioids (INC) → most effective
Intranasal decongestants
Intranasal cromones (not in SG)
Intranasal anticholinergics (exemption item)
39
New cards
What are the oral pharmacotherpy options available?
Oral H1 antihistamine ( 2nd gen preferred)
Oral corticosteroids (short course 5-7 days)
Oral decongestants
leukotriene antagonist
Oral corticosteroids (short course 5-7 days)
Oral decongestants
leukotriene antagonist
40
New cards
What are the options for topical intranasal H1 antihistamine?
Azelastine (+ fluticasone)
Olopatadine (Mometasone)
Both POM items
Olopatadine (Mometasone)
Both POM items
41
New cards
What are some side effects of Intranasal H1 antihistamines? (Azelastine, olopatadine)
Somnolence (Aze>olo)
Bitter taste
headache
Nasal discomfort
epistaxis (nose bleed)
Dizziness
Fatigue
Bitter taste
headache
Nasal discomfort
epistaxis (nose bleed)
Dizziness
Fatigue
42
New cards
What are some side effects of Intranasal corticosteroids?
Minimal systemic side effects
Local: Dryness, nasal irritation, occasional epistaxis
Local: Dryness, nasal irritation, occasional epistaxis
43
New cards
What are some precaustions for intranasal corticosteroids?
May worsen patients with cataract, glaucoma
44
New cards
What are the options of Intranasal corticosteroids available?
First gen: Systematic bioavailbility 10-50%
* Triamcinolone
Second gen: systemic bioavailability <1% or undetectable
* mometasone
* Fluticasone fuorate/proprionate
* Triamcinolone
Second gen: systemic bioavailability <1% or undetectable
* mometasone
* Fluticasone fuorate/proprionate
45
New cards
What is a special consideration for P+ item?
>18 YEAR OLD
46
New cards
What is the intranasal anticholinergic given as adjunct for rhinorrea?
Ipratropium
47
New cards
What is the adjunct option for uncontrolled rhinorrea?
Intranasal anticholinergic → Ipratropium
48
New cards
What is Leukotriene antagonist used in?
Not firstline anymore
\
Used in children and adolescents with asthma and allergic rhinitis
IT might have a place in patient with asthma
\
Used in children and adolescents with asthma and allergic rhinitis
IT might have a place in patient with asthma
49
New cards
Why is leukotriene no longer firstline?
Neuropsychiatric effects
need to inform patients and caregivers to be alert to changes in behaviour or new neuropsych symptoms
need to inform patients and caregivers to be alert to changes in behaviour or new neuropsych symptoms
50
New cards
What are the agents considered for **mild intermittent AR?**
Oral H1 antihistamine
Intranasal H1 antihistamine+ decongestant
Intranasal H1 antihistamine+ decongestant
51
New cards
What are the agents considered for **moderate to severe intermittent AR?**
Intranasal Corticosteroids INCs
Intranasal H1 antihistamine + decongestants
Oral H1 Antihistamine
Intranasal H1 antihistamine + decongestants
Oral H1 Antihistamine
52
New cards
What are the agents considered for **mild persistent AR?**
Intranasal Corticosteroids INCs
Intranasal H1 antihistamine + decongestants
Oral H1 Antihistamine
\
review patients after 2-4 weeks
Intranasal H1 antihistamine + decongestants
Oral H1 Antihistamine
\
review patients after 2-4 weeks
53
New cards
What is the monitoring for mild persistent AR?
review patients after 2-4 weeks
* failure → step up
* improved → continue for 1 month
* failure → step up
* improved → continue for 1 month
54
New cards
What are the agents considered for **moderate to severe persistent AR?**
Firstline: Intranasal corticosteroids (INCs)
\
Review patient after 2-4 weeks
* improved→ continue for 1 mo
* failed → review
* Add or increase INC dose
* Rhinorrhoea→ add ipratropium
* Nasal congestion → Decongestant or Oral CS
* Still failed → refer
\
Review patient after 2-4 weeks
* improved→ continue for 1 mo
* failed → review
* Add or increase INC dose
* Rhinorrhoea→ add ipratropium
* Nasal congestion → Decongestant or Oral CS
* Still failed → refer
55
New cards
What to do when patient also has conjunctivitis?
Intraocular H1 antihistamine (eyedrops)
oral H1 antihistamine
oral H1 antihistamine
56
New cards
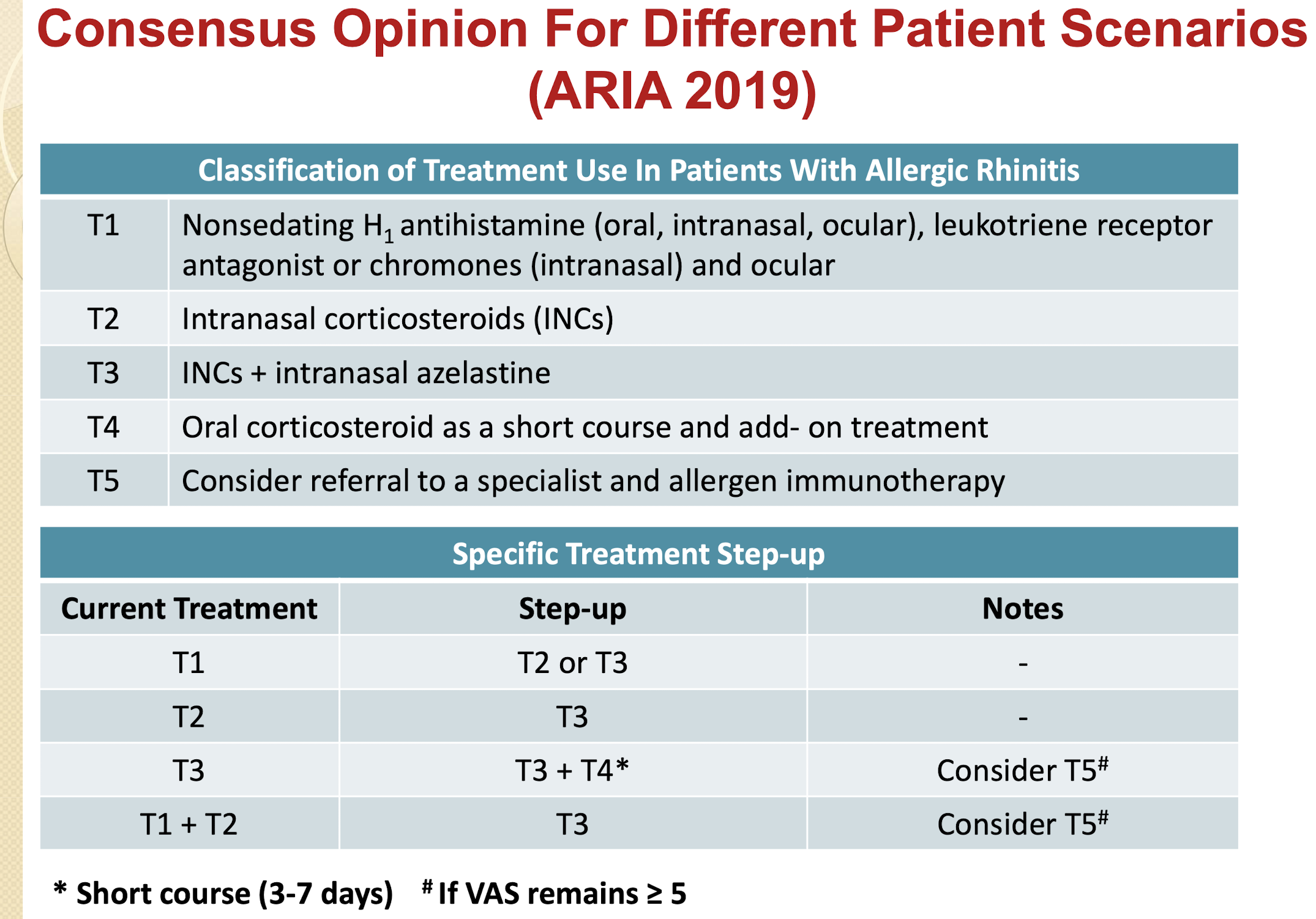
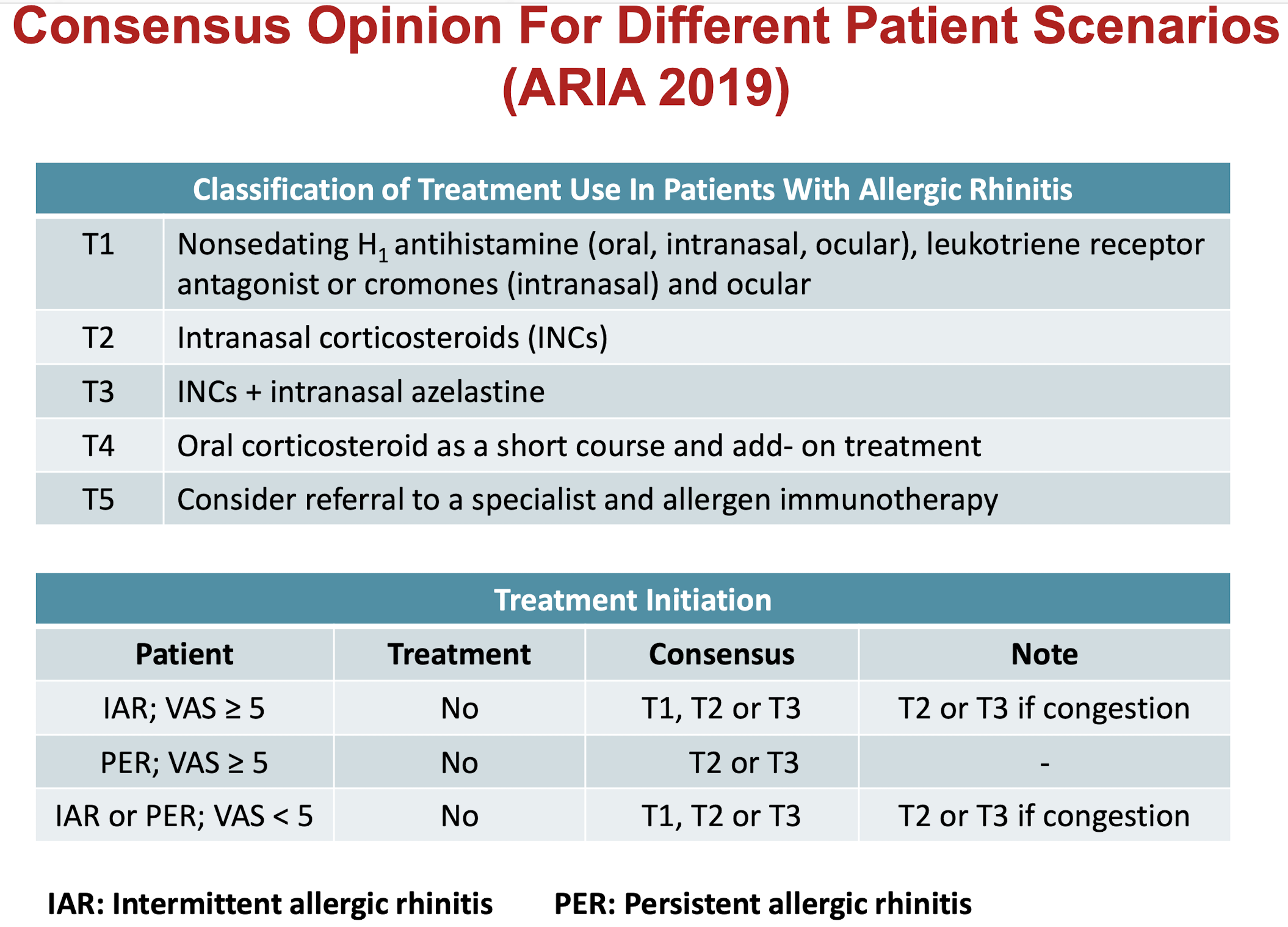
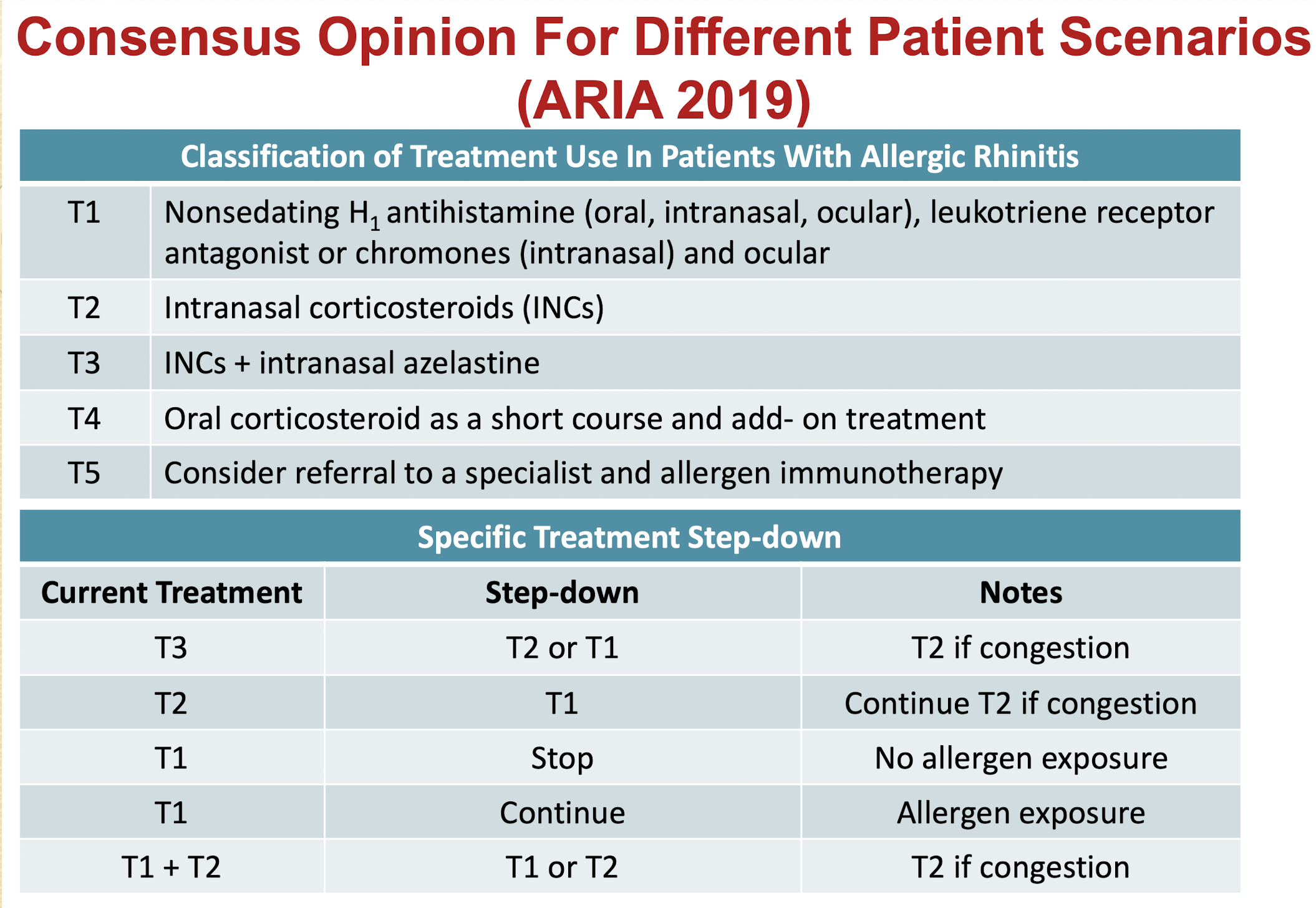
What do the T1 T2 T3 T4 T5 stand for?
T1→ Oral/intranasal/ocular h1 antihistamine
T2→ Intranasal CS
T3 → Intranasal CS + Intranasal H1 antihistamine
T4→ short course CS (5-7 days)
T5→ Referral for Immunotherapy
T2→ Intranasal CS
T3 → Intranasal CS + Intranasal H1 antihistamine
T4→ short course CS (5-7 days)
T5→ Referral for Immunotherapy
57
New cards
How do you do step up treatment?
58
New cards
What should you give acc to ARIA?
59
New cards
How do you do step down?
60
New cards
What is the safest option for pregnant woman?
Saline nasal rinse
INCs→ Budesonide
Oral antihistamine → Loratadine, cetirizine preferred after 1st trimester after discussion with obstetrician (avoid 1st gen)
\
INCs→ Budesonide
Oral antihistamine → Loratadine, cetirizine preferred after 1st trimester after discussion with obstetrician (avoid 1st gen)
\
61
New cards
What is contraindicated for pregnant woman?
Oral and nasal decongestant
62
New cards
What is the safest option for lactating woman?
saline nasal rinse
\
All intranasal CS are probably safe
\
All intranasal CS are probably safe
63
New cards
What is contraindicated in lactating women?
Avoid oral and nasal decongestant → limit breast milk secretion
64
New cards
What are the patient education points?
1. Environmental control measures
2. Appropriate use of device
3. Common side effects
4. When to seek medical assistance
1. new symptoms
2. doesnt get better
65
New cards
What is the monitoring for allergic rhinitis?
Review response to therapy after 2-4 weeks of treatment
66
New cards
Who is suitable for immunotherapy for AR?
Patient with moderate to severe rhinitis
* not adequately controlled
* experienced unacceptable adverse events
* want to reduce long term use of med
* able to comply with protocol
* Allergic asthma
* not adequately controlled
* experienced unacceptable adverse events
* want to reduce long term use of med
* able to comply with protocol
* Allergic asthma
67
New cards
Who is not suitable for immunotherapy for AR?
Uncontrolled asthma
Patient taking beta blockers
Patient taking beta blockers
68
New cards
What are the score and grade of AR control? Visual Analogue scale
>50mm uncontrolled AR
20-50mm partially controlled
<20mm well controlled
20-50mm partially controlled
<20mm well controlled
69
New cards
How do you administer nasal spray?
Administration of intranasal Steroid Sprays
1. Wash your hands well with soap and water.
2. Remove the packaging from the nasal spray pump.
3. Some nasal sprays need to be **primed before use**. As well, some nasal sprays **need to be shaken**. If your spray needs to be primed before using, squeeze it a few times into the air as directed until a fine mist appears.
4. Gently blow your nose to clear your nostrils
5. **Tilt you head forward**, depress one nostril, insert the tip into other nostril. Aim the **nozzle away from the nasal septum** and gently squeeze the nozzle. Inhale gently and breathe out through the mouth after each spray
6. If more than 1 spray is required per nostril, alternate the spray between nostrils one by one to prevent medication wastage.
7. If **taste** of medicament is present, **rinse mouth after use.**
8. Put the cap back onto the nasal spray container.
9. Try not to blow your nose for several minutes after using the spray.
1. Wash your hands well with soap and water.
2. Remove the packaging from the nasal spray pump.
3. Some nasal sprays need to be **primed before use**. As well, some nasal sprays **need to be shaken**. If your spray needs to be primed before using, squeeze it a few times into the air as directed until a fine mist appears.
4. Gently blow your nose to clear your nostrils
5. **Tilt you head forward**, depress one nostril, insert the tip into other nostril. Aim the **nozzle away from the nasal septum** and gently squeeze the nozzle. Inhale gently and breathe out through the mouth after each spray
6. If more than 1 spray is required per nostril, alternate the spray between nostrils one by one to prevent medication wastage.
7. If **taste** of medicament is present, **rinse mouth after use.**
8. Put the cap back onto the nasal spray container.
9. Try not to blow your nose for several minutes after using the spray.