324-Exam 1 (Cardiac, Electrolytes, Acid Base, Hematology, PeriOp)
1/181
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
182 Terms
Osmolarity vs Osmolality
Osmolality and osmolarity both measure the concentration of solute particles in a solution, but differ in their unit of measurement. Osmolality measures osmoles of solute per kilogram of solvent (mOsm/kg, temperature-independent), while osmolarity measures osmoles per liter of solution (mOsm/L, temperature-dependent).
Key Differences:
Definition: Osmolality is based on weight (kg), while Osmolarity is based on volume (L).
Isotonic Solution
0.9% saline
Hypertonic Solution
3 or 5% saline or partenteral solutions
Hypotonic Solution
0.45% Saline
Insensible Water Loss
Fluid loss that cannot be measured (Respiration, sweat, tears, weeping, wounds, stool)
Sodium Range
135-145 mmol/L
Hyponatremia range and Causes
<135 mEq/L, Critical Value <120
Causes: Diuretics (esp Furosemide), NPO, low-salt, excessive ingestion of hypotonic fluids (Ex. >18L of tap water per day)
What are the cerebral assessment signs of hyponatremia?
Sudden confusion, change in behavior, change in level of consciousness (LOC)
What are the neuromuscular assessment signs of hyponatremia?
Muscle weakness; check respiratory effectiveness
What are the intestinal assessment signs of hyponatremia?
Increased motility
What are the cardiovascular assessment signs of hyponatremia?
Severe orthostatic hypotension, decreased blood pressure, rapid weak thready pulse
Hyponatremia Interventions
-Tolvaptan (Drug that causes hypernatremia, salt based)
-Reduce dose of drugs that increase sodium loss
-IV saline infusion
Hyponatremia Correction Max
Correction of hyponatremia should never exceed max rate of 8 mEq/L in any 24hr period
Hypernatremia Range and Causes
Range >145
Causes: NPO, fever, dehydration, excess intake, IV hypertonic
What are the neurological signs of hypernatremia?
Altered mental status, agitation, confusion, short attension span
What are the neuromuscular signs of hypernatremia?
Muscle twitching, irregular muscle contraction, reduced or absent deep tendon reflex
What are the cardiovascular signs of hypernatremia?
Increased pulse rate, hypotension
Hypernatremia Interventions
Prevent dehydration and hyponatremia. NS or dextrose 5% in 0.45% NaCl. Adequate water intake and avoid processed foods
Potassium Range
3.5-5.0 mEq/L
Hypokalemia Range and Causes
<3.5 mEq/L
Causes: Diuretics (furosemide), diarrhea/vomit, prolonged NG suction, water intoxication, NPO, heat induced sweating
What are the cardiovascualr assessment findings of hypokalemia?
Weak/thready pulse, ECG change, irregular pulse, hypotension
What are the neuromuscualr assessment findings of hypokalemia?
Muscle weakness, altered mental status
What are the respiratory assessement findings of hypokalemia?
Shallow respirations, increased effort, increased rate and depth, alkalosis
Hypokalemia Interventions
Priority= Adequate gas exchange, prevents fall, monitor response
PO/IV Potassium Chloride (stop immediately if potassium infiltrates the interstitial space)
What is the ECG change of hypokalemia?
Shallow T-wave, presence of a U wave
Hyperkalemia Range and Causes
>5.0
Causes: Salt substitutes, potassium (PO or IV), blood transfusion, tissue damage, K+ sparing diuretics, uncontrolled diabetes, ACE/ARBS
What is an example of a potassium sparing diuretic that can cause hyperkalemia?
Spironolactone
What are the neuromuscular assessement findings of hyperkalemia?
Skeletal muscle twitch, tingling/burning, parasthesia
What are the cardiovascular assessment findings of hyperkalemia?
Bradycardia, hypotension, ECG changes, Vfib
What are the GI assessment findings of hyperkalemia?
Increased motility (diarrhea), hyperactive bowel tones
Hypokalemia Drug Interventions
Patriomer (poop out K+), Insulin (given with 50% dextrose), potassium wasting diuretics (Furosemide)
What is the ECG change of hyperkalemia?
Peaked T waves, wide QRS, and loss of P wave. (In order from least severe to most severe)
Calcium Range
9.0-10.5 mg/Dl
Requries active form of Vit D to be absorbed. Think muscle/heart!
Hypocalemia Range and Causes
<9.0 mg/dL
Causes: Inadequate oral intake of calcium, Vit D or Diarrhea
Result: Bone resorption (osteoclasts)
Hypocalcemia Signs/Cues
Muscle spasms, thyroid surgery, parasthesia of hands and feet, tingling, loss of bone density, height changes, chrons or celiacd disease, prolonged QT/ST
Positive Chvostek's sign
A sign of hypocalcemia. Tapping on facial nerve stimulates facial twitching.
Positive Trousseau's sign
A sign of hypocalcemia. BP cuff inflated to create hypoxic condition on arm, hand and finger will go into spasm
Hypocalcemia Interventions
Calcium/Vit D supplementation
Reduce environment stimuli
Prevent injuries (weak bones)
Hypercalcemia Range and Causes
>10.5 mg/dL
Causes: Excessive oral intake (ex. TUMS), use of thiazide diuretics, immobility, dehydration, glucocorticoids
What are the CV assessment findings of hypercalcemia?
Increased HR, Increased BP (acute), slow HR (chronic), poor perfusion, ECG changes
What are the NM assessment findings of hypercalemia?
Severe muscle weakness, decreaed deep tendon reflexes, confusion, lethargy
What are the GI assessment findings of hypercalcemia?
Constipation, nausea, vomiting, ab distension, hypoactive bowel tones
Hypercalcemia Interventions
Prevent calcium resoprtion with phosphorus, calcitonin, and bishosphonates
NS, discontinue supplementation
Magnesium Range
1.6-2.2 mg/dL
Hypomagnesmia Range and Causes
<1.6, Critical <1.2
Causes: Malnutrition, starvation, diarrhea, alcohol use disoder, loop or thiazide diuretics
Hypomagemesmia Cardiovascular Assessment Findings
Arrhythmia, QT and PR prolongation, hypertension
Hypomagnemesia NM Assessment Findings
Tetany (involuntary spasms/cramps)
Hypomagnemesia GI Assessment Findings
Anorexia, nausea, paralytic ileus
Hypomagnemesia Interventions
Restore normal calcium levels, IV magnesium, discontinue: loop diuretics, aminoglycoside, antibiotics
Hypermagnesmia
>2.2, Critical >4.0
think lethargy
Hypermagnesmia CV Assessment Findings
Bradycardia, peripheral vasodilaton, hypotension, ECG changes
Hypermagnesmia NM Assessment Findings
Weakness, respiratory depression, decreased mental function, dowsy, fatigue. Not usually apparent symptoms until critical
Hypermagnesmia Interventions
Reduce serum level, Mg2+ free IV fluids, loop diuretics, Calcium (if cardiac problems)
What are cardiovascular cues of fluid overload?
Hypertension, bounding pulse, tachycardia, JVD, S3 heart sound
What are respiratory cues of fluid overload?
Crackles, shortness of breath (SOB), orthopnea, pulmonary edema (PE), decreased O2
What are peripheral cues of fluid overload?
Edema, rapid weight gain, tight shiny skin
What are neurologic cues of fluid overload?
Headache, confusion, restlessness
What laboratory findings are associated with fluid overload?
Decreased hemoglobin, decreased hematocrit, hyponatremia
Dehydration Assessment Findings
Increased HR, decreased BP, concentrated urine (specific gravity >1.030), elevated hemoglobin, hematocrit, serum osmolarity, etc.
Hemoconcentration
An increase in the concentration of red blood cells, hemoglobin, and hematocrit, generally caused by a reduction in plasma volume
Human Arterial Blood pH Range
7.35-7.45
Fatal pH Ranges
>6.9 or >7.8
What are pH buffers?
Compounds that help keep the pH from changing drastically by soaking up or releasing H+ ions.
What are some examples of pH buffers?
Phosphate, proteins, albumin, globulins, hemoglobin.
What is the first line of defense for pH regulation?
pH buffers.
What is the second line of defense for pH regulation?
The respiratory system. (Quick)
What is the third line of defense for pH regulation?
The kidneys. (Slow but effective, 24-48hrs)
Greatest risk for acidosis
Patients with breaht problems (COPD, asthma) and chronic health conditions
Causes of metabolic acidosis
Diabetes/DKA, shock, diarrhea, renal failure, liver disease, sepsis, use of aspirin (salicyates), CO poisoning
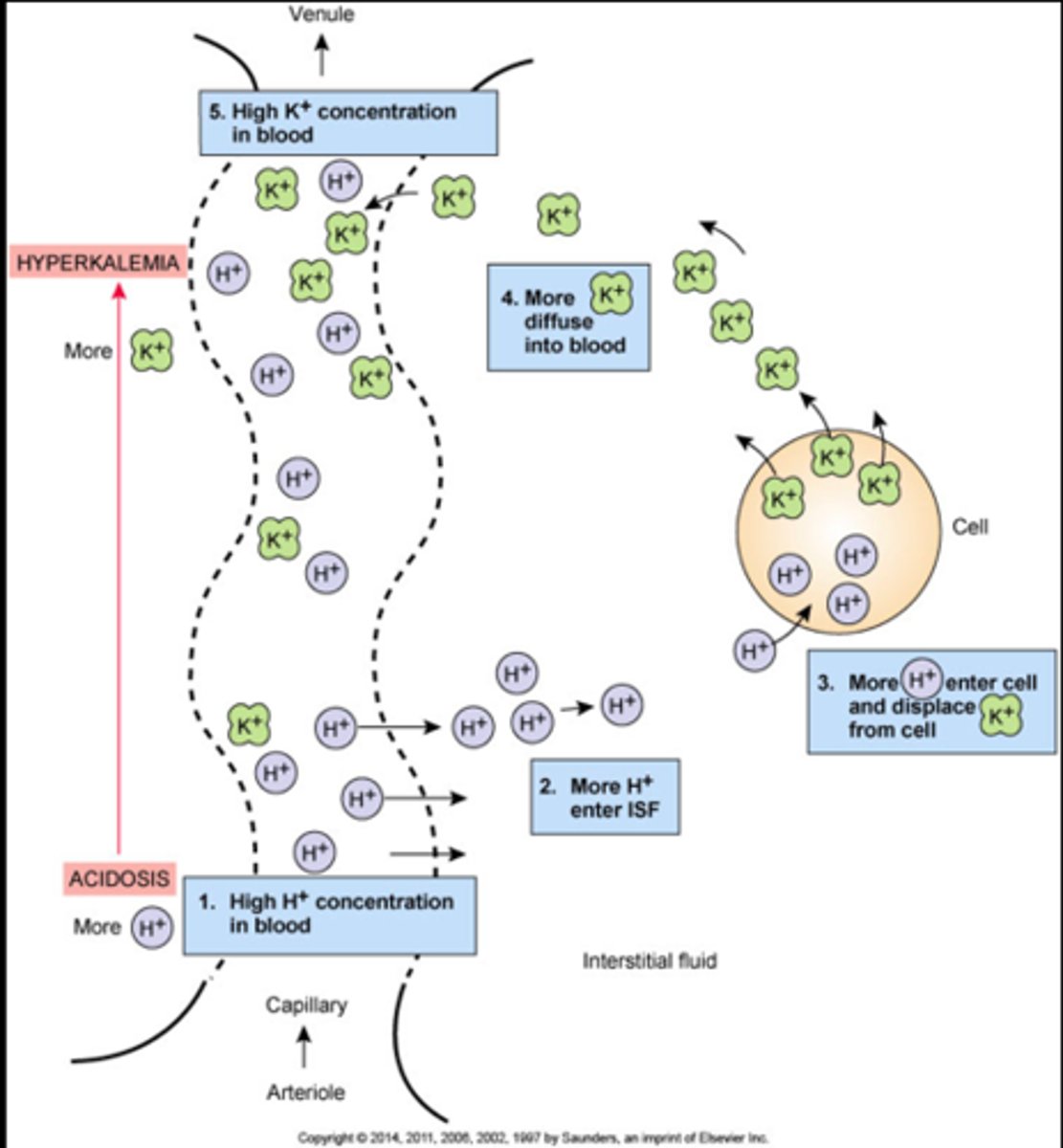
Biggest concern of acidosis
Cardiovascular problems due to risk for hyperkalemia
(Too much H+ kicks K+ out of cells)
Common cause of Metabolic Alkalosis
Vomiting or NG suctioning (losing stomach acid). Also, excessive intake of antacids, durietic use, hypovolemia
Relative Alkalosis
No increase in base, acid decreases
Alkalosis Outcomes
Hypokalemia (K+ leaves cell to resotre balance of no H+), increased CNS activity, irritability, seizures, positive chvostek sign/trosseus sign
What two electrolyte imbalances are often seen with alkalosis?
Low potassium and low calcium often go together
What precautions should an alkalotic patient be put on?
Seizure precautions
polydipsia
Excessive thirt, and ingestions of fluid (>3L/day). Could be related to SIAHD, DI or psychiatric
BNP
Hormone produced by heart in response to stretching, an indicator of heart failure
Oliguria
Low urine output, less than 400 ml/day or <20-30mL/hr
Anuria
absence of urine production
Polyuria
excessive production of urine (>2.5-3L/day)
Dysuria
painful or difficult urination, often associated with a UTI
Nocturia
frequent urination at night
Cardiac Output
Amount of blood pumped by the heart every minute
Stroke Volume
Volume of blood pumped out of left ventricle during each contraction
HR x SV = Cardiac Output
Stroke Volume= Preload-Afterload
Preload (Stretch)
Amount of blood in left ventricle after filling (pre-ejection)
Afterload (Squeeze)
Pressure your heart has to pump against to eject the blood from the left ventricle (Goal=low)
What does the term cardiomyopathy refer to?
It describes all diseases of the heart muscle.
What effect does too much preload have on the heart?
It can overstretch the heart.
What is the impact of too much hypertension on the heart?
It increases afterload pressure, making the heart work harder.
Mean Arterial Pressure
Force (pressure) being exerted against vessel walls at any given point OR the average arterial pressure during a single cardiac cycle
Cardiac Cycle
The complete, rhythmic sequence of electrical and mechanical events in the heart, lasting about 0.8 seconds (at 75 bpm) from the start of one heartbeat to the next. It consists of systole (contraction/ejection) and diastole (relaxation/filling)
3 P's of Perfusion
Pump (heart), Pipes (blood vessels), Plasma (blood)
Conductivity of cardiac cells
The ability of all cardiac muscle cells to transmit electrical impulses, effected by levels of K+, Ca+, Mg, Na
Automaticity of Cardiac cells
The cells ability to spontaneously depolarize (generate electrical impulse) without external nerve stimulation
Excitiability of Cardiac Cells
The ability of cells to generate electrical signs to trigger coordinated contractions
Contractility of Cardiac Cells
ability to respond mechanically to an impulse. Intrinsically generate force and pump blood
Intrinsic Cardiac Pace Maker
SA Node (60-100 BPM), shown by P wave
AV Node Rate
Produce impulses from 40-60bpm
Bundle of His and Purkinje fibers Rate
20-40 bpm
P wave indicates what?
atrial depolarization (contraction)