LESIONS IN THE PITS & FISSURES
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
23 Terms
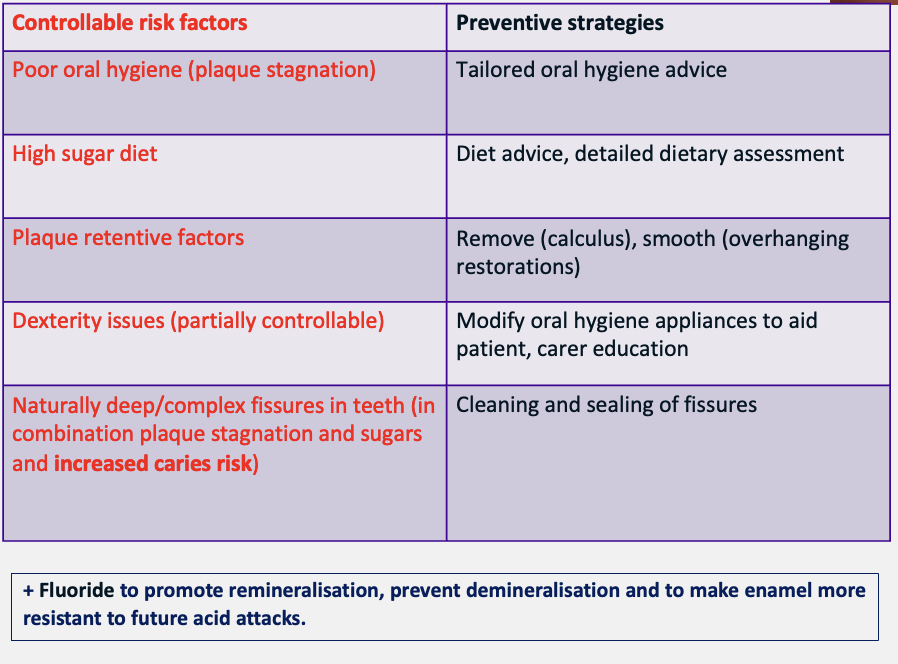
what areas of the teeth are plaque stagnation areas
occlusal
buccal
cingulum pits
fissures
why are pits and fissures areas of plaque stagnation
pits and fissures are often complex and inaccessible to oral hygiene measures - most common site to develop carious lesions
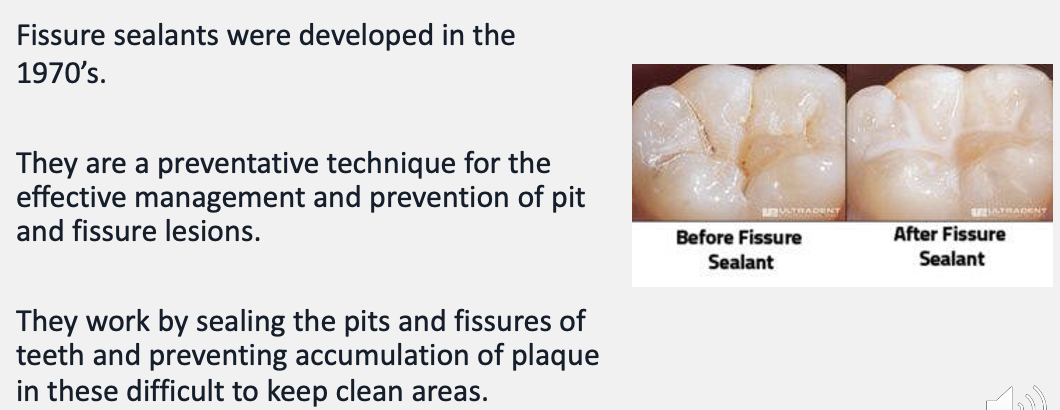
history of fissure sealants
in what two situations are fissure sealants used
a non-cavitated carious lesion
to protect sound pits and fissures in patients of high caries risk
how does fissure sealant protect against plaque development
FS provides a smoother, easier to clean surface compared to the anatomy of regular pits and fissures
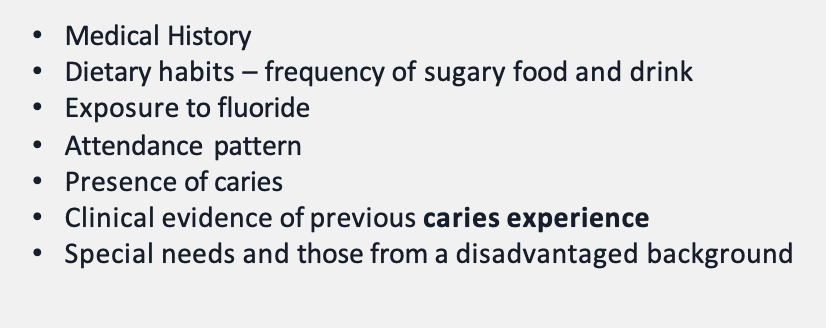
what things should be considered in a caries risk assessment
what are indications for fissure sealant
early pit and fissure carious lesions found during assessment
prevention of caries in high-risk caries groups
prevention of caries in a particularly complex fissure pattern that is proving difficult to clean
DBOH recommends the sealing of all permanent molars in children and young adults of high caries risk
what are contraindications of fissure sealant
cavitated carious lesions
inadequates moisture control
FS are (mostly) resin-based and therefore hydrophobic
no caries experience/ low caries risk
what are benefits of fissure sealants
can be used to treat early carious lesions/ prevent caries in high-risk groups
can suppress bacteria remaining in the fissure pattern by blocking their nutrient supply
makes complex fissure patterns more cleansable
proven to reduce caries incidence in high-risk groups
outline fissure sealant materials
there are two principal groups of materials:
resin-based fissure sealants - most used
glass-ionomer fissure sealants - more common in paediatric clinics
give an example of a situation where a glass-ionomer fissure sealant would be opted for
where moisture is more likely to be present e.g. fissure sealing a partially erupted tooth
instruments and materials needed to place a fissure sealant
routine examination kit: mirror, probe, tweezers
high-speed handpiece: adjusting and finishing the sealant
slow-speed handpiece: used with bristle brush and pumice
isolation kit
etchant and microbrush
resin-based sealant, composite gun and light-cure unit
articulating paper and finishing burs
what is the most common cause of FS failure
saliva contamination
how many teeth should be isolated during FS
single tooth isolation is sufficient for placing a FS
often also need LA due to clamp pressure
outline tooth preparation for FS
tooth must be plaque free and free from debris
use a rubber cup/ bristle brush with pumice or any non-fluoride, non-oil based paste to clean the surface
thoroughly wash and dry tooth to prepare for acid etching
outline enamel etching for FS
cover the fissure pattern with etch - aim to etch a greater area than the area that will be covered by FS
wait 30s and aspirate and wash the etch
dry the tooth - the enamel must appear frosted/ chalky
what substance is used for acid etching
phosphoric acid [37%]
how does acid etch work
etch slightly demineralises the enamel surface, creating porosities that the FS can flow into
if the tooth becomes wet via saliva contamination after the etching procedure, what should be done
re-etch but for a shorter period of 10-15s (you can tell if acid etching has not worked if the enamel is not chalky)
outline FS application
place sealant into pits and fissures
can soak up with cotton pledgets if too much FS is dispensed
lightly run a probe through the sealant to eliminate air bubbles
light cure for 20s to set
check margins with a probe
check occlusion with articulating paper
high spots can be adjusted with finishing burs in a high-speed handpiece
outline FS maintenance
fissure sealants should be assessed at recurrent dental visits
check for any loss of material (plaque retentive factor) and discolouration around the edges or under the sealant
what are common ways FS fail
debonding
fracture
adhesive failure - poor moisture control upon placement
adhesive failures tend to be immediate
porosities - may develop due to water contaminants during placement
heavy occlusal contacts
caries