Human Physiology Exam 2
1/98
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
99 Terms
Neural Pathways
Divergence: e.g. “group text”
one neuron affects many post-synaptic cells
Convergence
many pre-synaptic neurons affect a smaller number of post-synaptic neurons
post-synaptic neuron will integrate these signals and sum into one signal
Summation of Signals: Spatial Summation
Graded potentials from many locations in the neuron are added together
total of all potentials determines whether an A.P. is generated
Distance → farther away = less input
Original amplitude → whichever signal is most intense has most input
EPSP or IPSP → if inhibitory signal is closer/stronger, it can cancel excitatory signals
Time of arrival → if the signals are disjointed, there won’t be an action potential
Summation of Signals: Temporal Summation
must arrive at same time to sum
two graded potentials will be added if they arrive at the trigger zone in a short timeframe
1st potential hasn’t yet returned to resting potential
Inhibition at Synapses
Receptor
antagonist blocks neurotransmitter → no graded potential generated
Selective Pre-Synaptic
axon terminal is inhibited → no voltage-gated Ca2+ channels open
sometimes this blocks a response because it needs a coordinated response
Global Pre-Synaptic
dendrite is inhibited, no Action Potential is generated in axon
Ohm’s Law and Electric Signaling
electric signals are created when charges flow across the membrane
V=IR
V = charge gradient → membrane insulates and separates charges
I = flow of charge → charges flow through channels
R = resistance to flow → membrane insulates, prevents flow of charges
Electrical Disequilibrium
Active transport causes chemical gradients: outside the cell, [Na+] increases. inside the cell [K+] increases
many substances are charged
Movement across the membrane of a charged substance = e-gradient
cell is essentially neutral: there are regions of charge difference
opposite charges attract
membrane is an insulator
charges are moved across the membrane in a selective manner (mediates transport or channels)
Resting membrane potential: the electrical disequilibrium which exists while the cell is at rest → only a small number of ions need to move to change the potential
Active transport and a mechanism to separate charges are required to establish electrical disequilibrium.
Resting Membrane Potential
Cell = (-) → -40 to -90 mV for neurons and muscle cells
selective permeability of membrane → most permeable for K+
forms e-gradient
Equilibrium Potential
potential where the electric and chemical gradients are balanced
Determined by Nernst Equation, which accounts for: temperature, charge, [inside], and [outside]
Graded Potential
signal is received and transduces through the membrane via an open channel down a gradient → graded potential
G.P. arc is summed at axon hillock, if it meets threshold, an AP is generated
AP causes Na+ channels to open, Na+ floods into cell, depolarizing membrane. The K+ channels are stimulated to open
At peak, Na+ channels close, K+ channels open, and K+ leaves, re-polarizing then hyper-polarizing the membrane.
Na+/K+/ATPase pumps help return to resting membrane potential
Causing an Action Potential
Distance Traveled = farther allows more leak
Original Amplitude = larger means more impact, + vs ++++
EPSP (depolarizing +) increases the chance of an AP, while IPSP (hyper-polarizing -) decreases the chance of an AP
Timing = must arrive at the axon hillock at nearly the same time to be summed
Peripheral Nervous System
Afferent: Sensory
sensory receptors sense external and internal stimuli
transduce stimuli into electric signals
Efferent: Somatic
skeletal muscle
mostly voluntary
Efferent: Autonomic
smooth and cardiac muscle
adipose tissue
glands
Structural Proteins
Integral → transmembrane
Channels, transporters, receptors, structural proteins, enzymes
Peripheral → outside or inside of p.m., connected to another protein
receptors, structural support, enzymes
Lipid-anchored
receptors, structural support, enzymes
Long-term Potentiation
Used to strengthen synapses, which are used frequently and with intensity
increased sensitivity of post-synaptic cell
increased release of neurotransmitter by presynaptic cell
Muscle: Major Functions
generate motion and force
generate heat
maintain homeostasis of body temperature: regulate heat gain and loss
Muscle Types
Skeletal
attached to skeleton
allows body movement
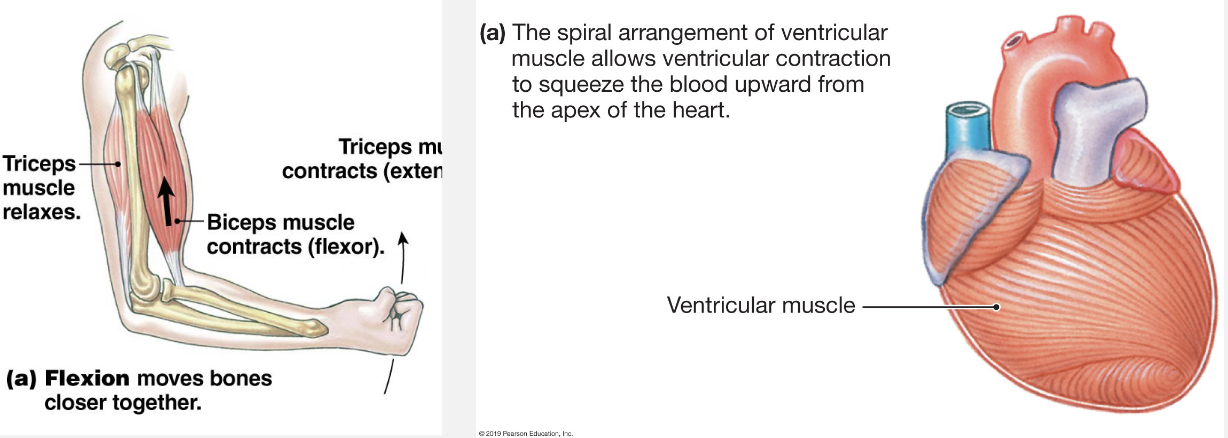
Cardiac → shares characteristics of both skeletal and smooth muscle
only found in heart
pumps blood throughout body
Smooth
moves substances in, out, and through body (GI tract, blood vessels, lining of organs)
Skeletal Muscle
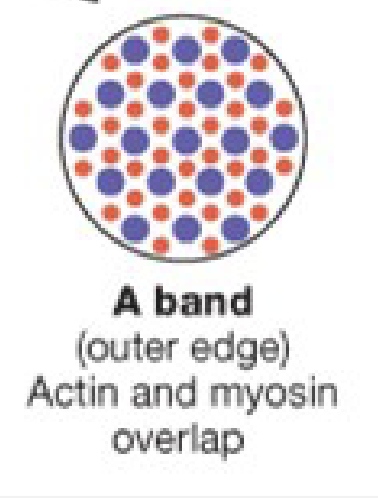
Striated = due to regular arrangement of actin and myosin
Multi-nucleated = skeletal muscle cells started as many cells → elongated/fused into 1 long cell during development, causing formation of a multi-nucleated cell
Voluntary control = can choose to override a reflex = voluntary
requires neuronal input: somatic division → somatic motor neurons
No Gap Junctions → all other muscle types have gap junctions
Ca2+ and troponin
Fastest contraction of all muscle types
Cardiac Muscle
Semi-striated
single neurons
involuntary control
stimulated by pacemaker cells → doesn’t need nervous system, regulated by autonomic NS
Gap Junctions → Need them to contract bc electric signals pass btw cells, causing contraction at the same time = pump
Medium contraction rate
Smooth muscle
no striation
mono-nucleated
involuntary control → e.g. uterine contractions aren’t controlled
stimulated by: hormones, pacemaker cells and have irregular rhythm, chemical changes, autonomic NS, stretch
Gap Junctions
Ca2+ and calmodulin
Slowest contraction of all muscle groups
Skeletal Muscle Characteristics
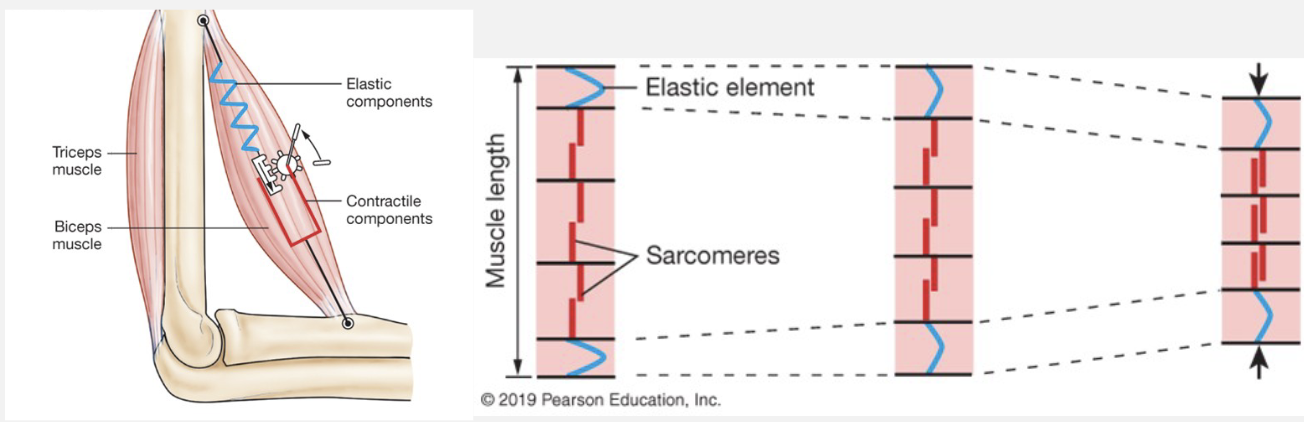
Attached to bone by tendons in antagonistic pairs
flexion: toward body, decreases angle at joint
extension: away from body; increases angle at joint
origin: stationary bone → typically proximal/medial
insertion: mobile bone → typically distal/lateral
myofibril: bundle of contractile proteins
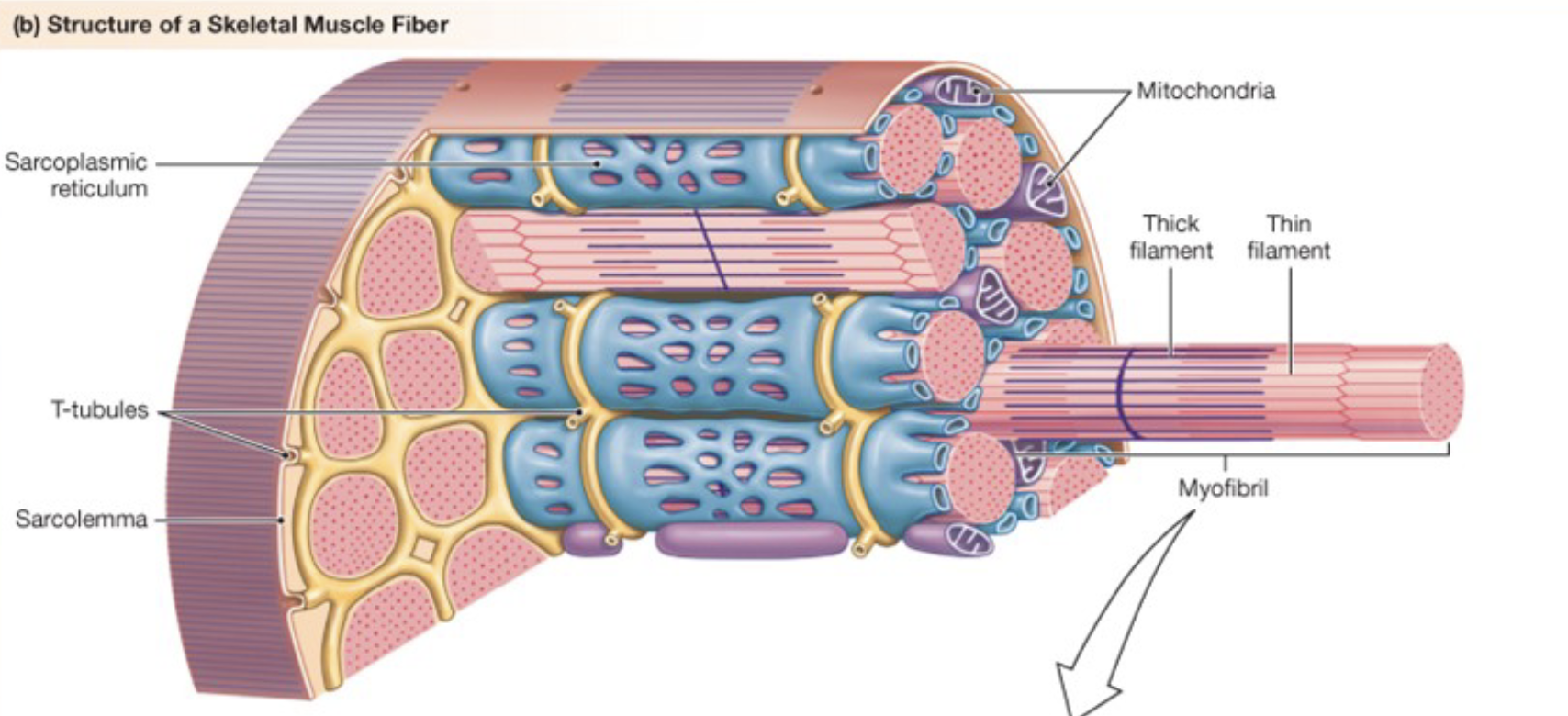
Anatomy of a skeletal muscle fiber
blue mesh = sarcoplasmic reticulum → stores Ca2+
T-tubules = action potentials travel through here
Mitochondria = ATP production
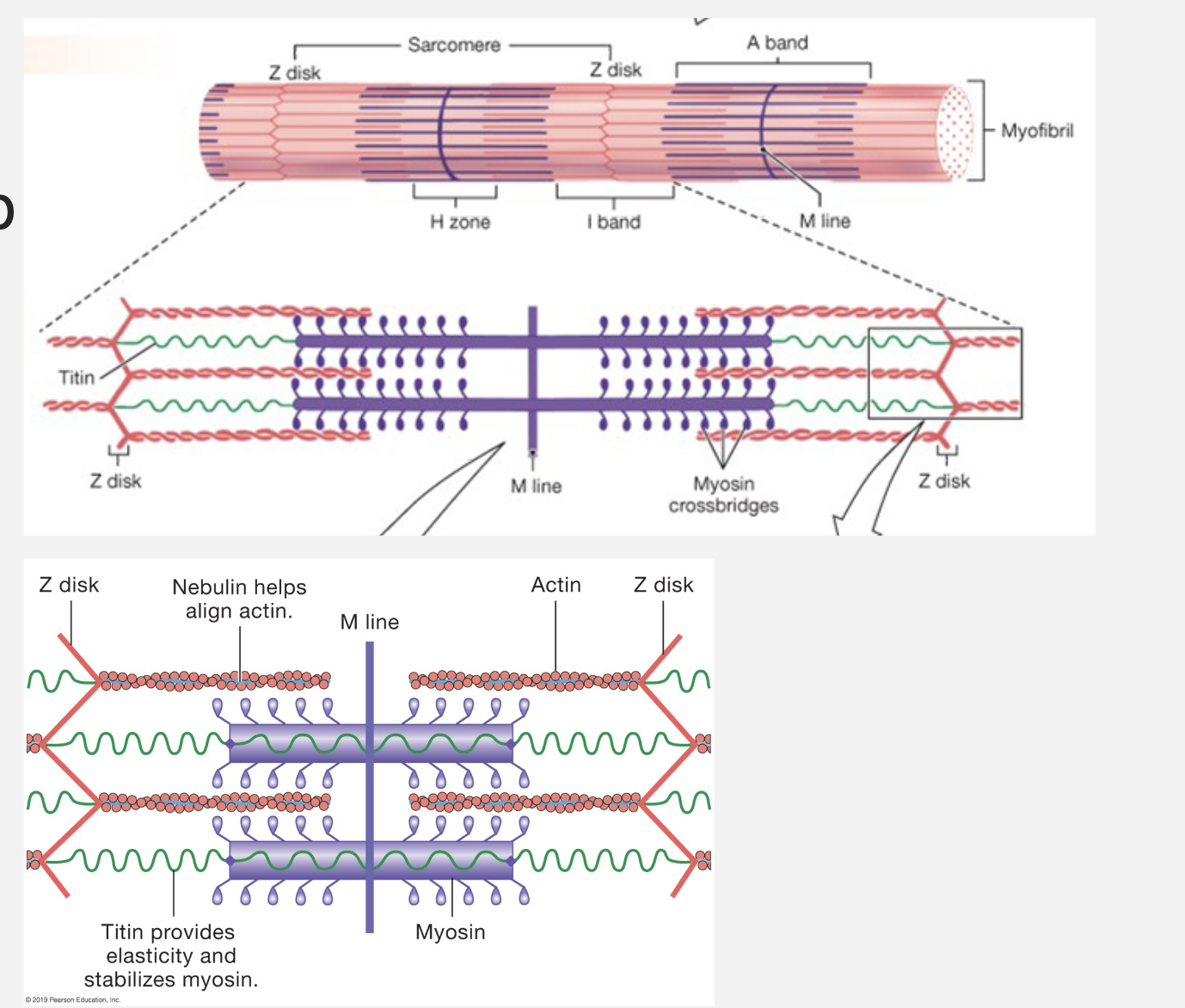
sarcomere = contractile unit of skeletal and cardiac muscle
actin = thin filament
myosin = thick filament
myosin heads = form cross-bridges
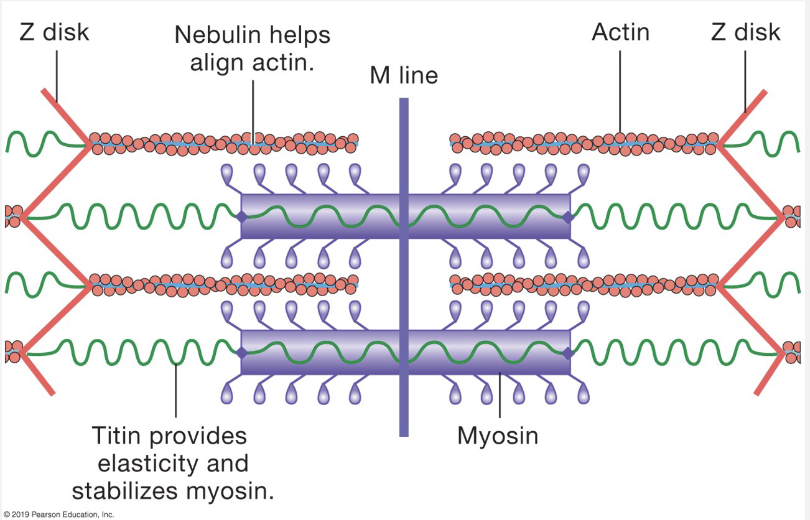
nebulin - keeps actin in alignment
Titin = provides elasticity and stabilizes myosin → returns sarcomere to original length
Sliding Filament Theory
Actin and myosin slide past each other → shortens sarcomere length (z-disk to z-disk)
Myosin heads attach to actin → cross-bridges form
Can only occur when Ca2+ is present → allosteric modulation
Requires ATP
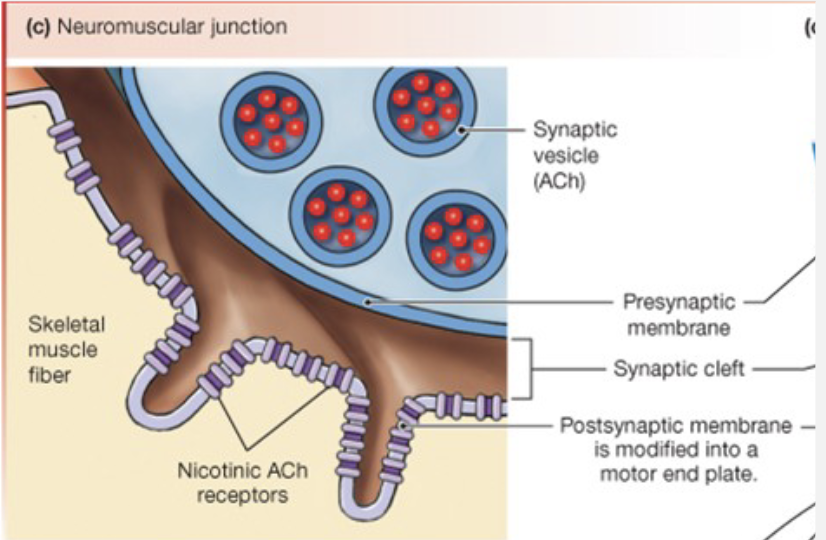
Neuromuscular Junction (NMJ)
synapse between neurons and skeletal muscle
Acetylcholine (ACh) is the neurotransmitter
Causes depolarization (Na+ goes in immediately, K+ goes out later) of muscle fibers (myofibers)
AP is generated by myofiber →
Release of Calcium
ACh is released at NMJ
muscle is depolarized bc ACh opens channels; AP is generated
AP travels through T-tubules
V-gated channels (DHP) linked to Ca2+ release channels
ryanodin receptors on SR increase [Ca2+]
![<ul><li><p>ACh is released at NMJ</p></li><li><p>muscle is depolarized bc ACh opens channels; AP is generated</p></li><li><p>AP travels through T-tubules</p></li><li><p>V-gated channels (DHP) linked to Ca<sup>2+</sup> release channels</p></li><li><p>ryanodin receptors on SR increase [Ca<sup>2+</sup>]</p></li></ul><p></p>](https://assets.knowt.com/user-attachments/8ae92411-bd57-40f2-8691-ffcec5f99cca.png)
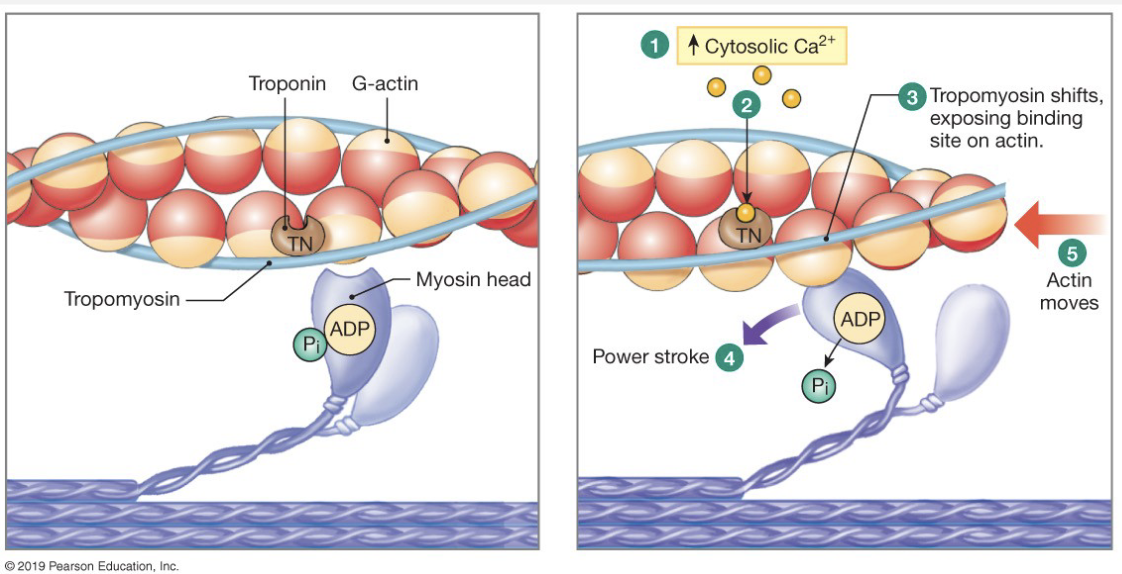
Regulation of Contraction
binding site = troponin and is blocked by tropomyosin
AP depolarizes cell → travels down T-tubules
Ca2+ enters cell (via diffusion through channel, fast); binds to troponin → rolls and exposes binding site
Troponin pulls tropomyosin off of binding site
cross-bridges are formed and start the power-stroke cycle
Ca2+ is pumped back into the SR → pump is slow
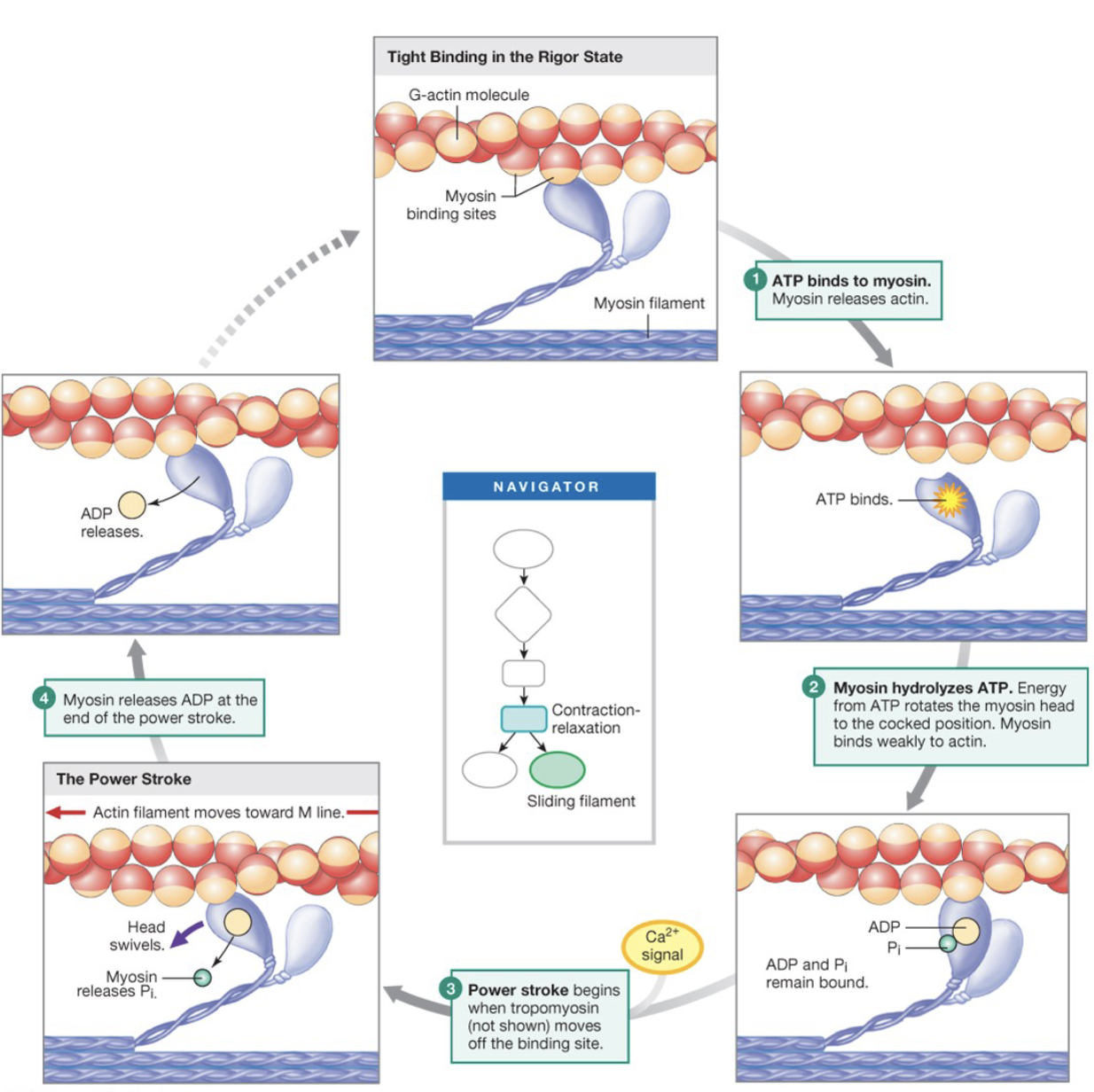
Power-Stroke Cycle
ATP binds to myosin, causing it to release actin
Myosin hydrolyzes ATP. Energy from ATP rotates the myosin head to the cocked position. Myosin binds weakly to actin
Power-stroke begins when tropomyosin moves off of the binding site
Myosin releases ADP at the end of the power-stroke
Muscle relaxation
destroying cross-bridges until they’re all gone
Ca2+ ATPase pump removes Ca2+ from cytosol, continually pumping it back into the SR
once free, Ca2+ is removed, Ca2+ releases from troponin
Troponin allows tropomyosin to slip back over actin binding site
cross-bridges can no longer be formed
muscle is relaxed
Time and Contraction Events
contraction caused by single AP = twitch
latent period: start of stimulus (muscle AP) to response to stimulus (contraction/twitch)
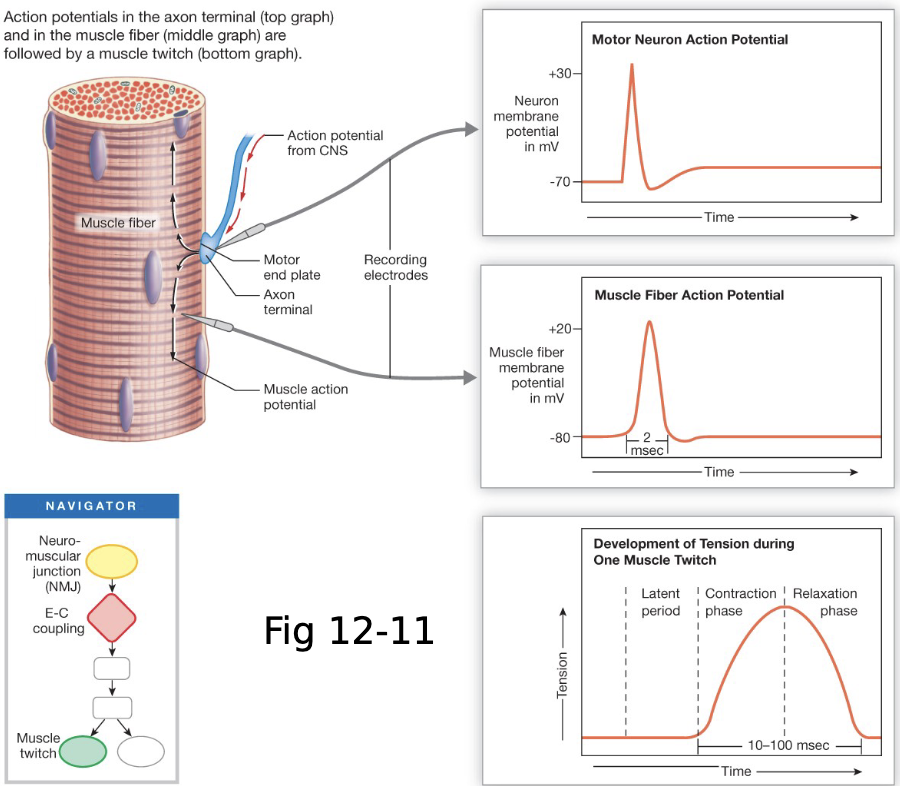
Time and Contraction Events: The Latent Period
Latent Period: time btw stimulus (AP) and the start of contraction
AP travels down the T-tubules
Voltage sensor triggers opening of Ca2+ gate
Ca2+ release from SR
Ca2+ diffuses and binds to troponin
Troponin pulls tropomyosin away
Cross-bridges can be formed and tension generated
Energy for Contraction
Must have ATP: power-stroke cycle, active transport of [Ca2+] into SR, Na+/K+/ATPase pump to replace Na+/K+ from AP
Phosphocreatine
Anaerobic glycolysis: glycolysis (Cori/Lactate Cycle)
Aerobic metabolism: glycolysis, citric acid cycle, ETS
both phosphocreatine and anaerobic glycolysis produce ATP in low [O2] env.
Aerobic metabolism
Glycolysis → pyruvate + ATP → Citric Acid Cycle → NADH + FADH2 + ATP → ETS → lots of ATP
Muscle Fatigue
physiological → muscle can no longer contract
long, lower intensity exertion → depletion of glycogen
fast, maximum exertion → build up of Pi, increasing extracellular [K+]
prevents P from leaving cell or decreases chance of AP
![<ul><li><p>physiological → muscle can no longer contract</p></li><li><p><strong>long, lower intensity exertion</strong> → depletion of glycogen</p></li><li><p><strong>fast, maximum exertion</strong> → build up of P<sub>i</sub>, increasing extracellular [K+]</p></li><li><p>prevents P from leaving cell or decreases chance of AP</p></li></ul><p></p>](https://assets.knowt.com/user-attachments/d72caba1-5ff7-49f0-813a-72346a5a94b6.png)
Muscle Fatigue: Neuronal Factors
depletion of ACh.
Plays a role in disease, abnormal
Types of Fatigue
central: CNS → psychological effects, protective factors
peripheral: PNS → decreased neurotransmitter release, decreased receptor activation, change in muscle membrane potential
Tension and Fiber Type
Fast-Twitch Glycolytic → fatigues easily
white (glycogen)
glycogen and anaerobic metabolism
most force generated
Fast-twitch Oxidative (intermediate)
red (myoglobin)
glycogen and mix of aerobic/anaerobic
Slow-Twitch Oxidative → fatigue resistant, slow contraction, least amount of force but lasts longer
red (myoglobin)
oxidative, aerobic metabolism (increased number of mitochondria)
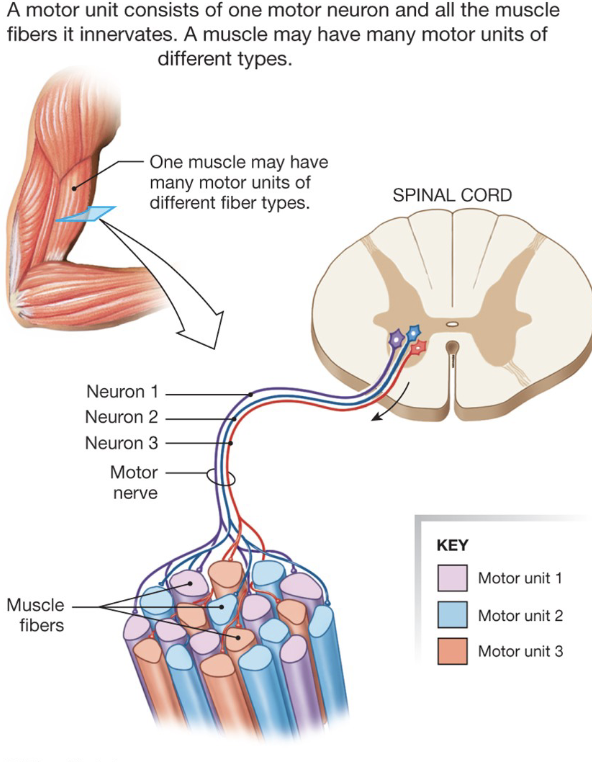
Types are mixed within a muscle, a neuron will only go to one fiber type
Motor unit
somatic motor neuron + all the fibers it innervates
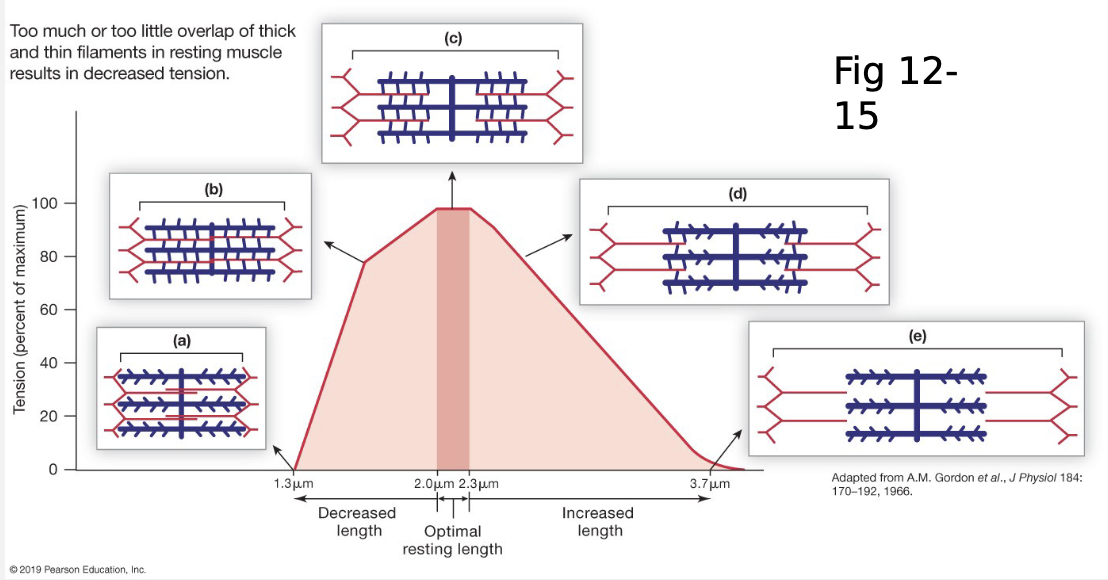
Length-Tension Relationships
Tension is directly proportional to the number of cross-bridges formed
length is related to cross-bridges formed
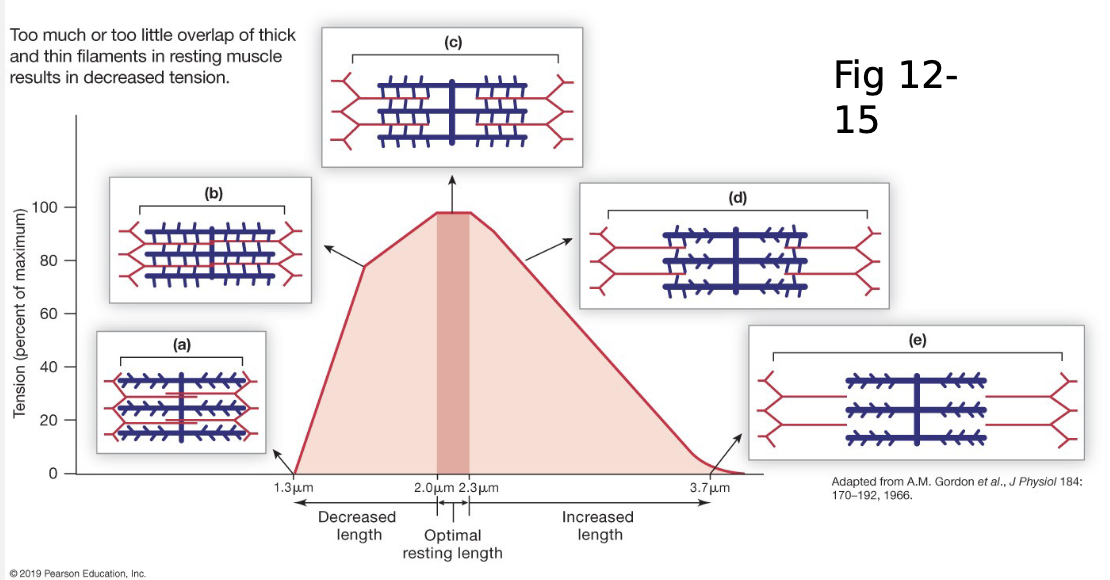
Mechanism for Increasing Tension
length-tension curve
mechanical summation
motor unit recruitment
muscle fiber type
low length = high number of cross-bridges, but they’re fighting against titin
normal people will have muscle length at/around the ideal length bc it’s attached to bone, which prevents over-extending or over-contracting
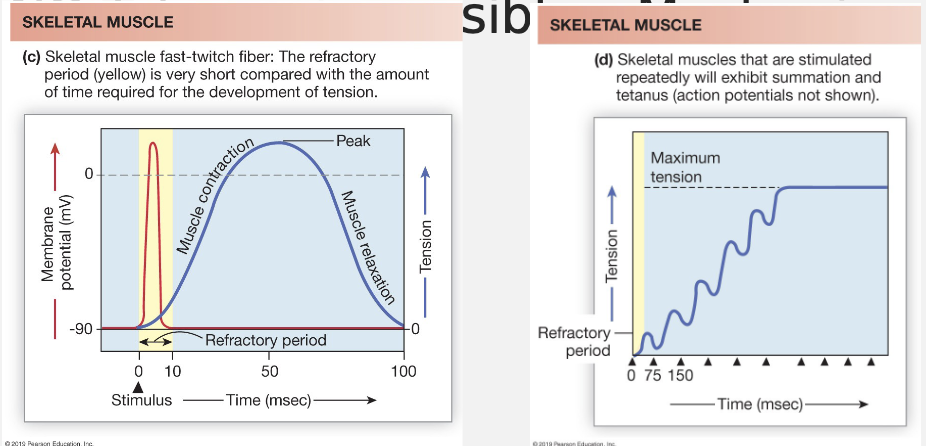
Tension and Twitch Summation
aka mechanical summation/wave summation
AP can’t be summed
mechanical event (twitch) can be summed. How? v-gated Ca2+ channels
Single twitch
muscle relaxes completely between stimuli
all Ca2+ is put back into cytosol
Summation
stimuli closer together don’t allow muscle to relax fully
new Ca2+ is released before old Ca2+ is put back fully, this allows higher [Ca2+] in cytosol and increases binding to troponin, and therefore causes an increase in the formation of cross-bridges
Tetanus: state of constant contraction
increase frequency of AP = increased [Ca2+] in cytosol
summed twitches generate more tension because they cause increased formation of cross-bridges
Tension and Recruitment
motor units are recruited when tension is generated
slow twitch first; fast twitch glycolytic last
recruit slow 1st bc they don’t fatigue as fast
fast twitch 2nd bc provide most force, but fatigue very quickly
this provides more controlled movement
Asynchronous: don’t want to recruit all muscle units at the same time bc you want to be able to recruit new units as the old ones fatigue
works for all except maximal contractions
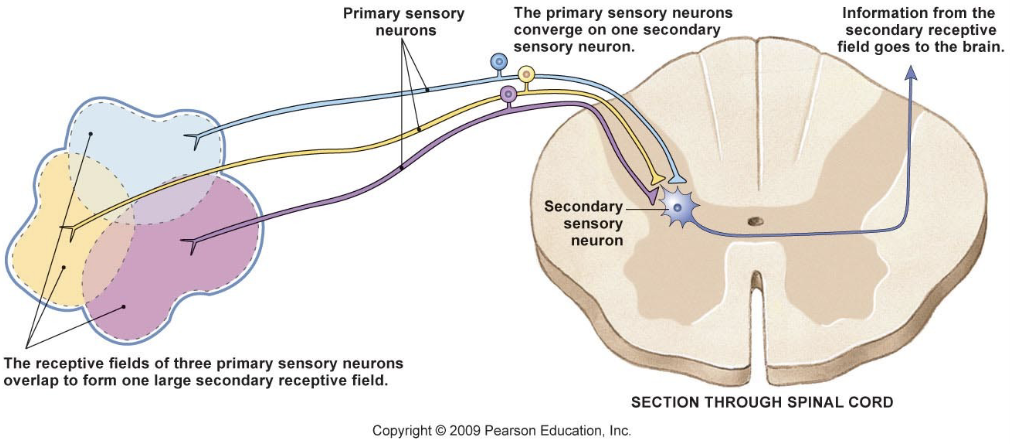
Properties of Sensory Systems
Receptive Fields
region where sensory info is gathered by a single sensory neuron
two-point discrimination test
Sensory unit: sensory neuron and all of its receptors → parallels motor units
larger receptive fields = less sensitive area
Sensory Vs Motor Units
Sensory
smaller unit = higher sensitivity
larger unit = lower sensitivity
fewer sensory units/area
Motor
smaller units = less strength, more precision
larger units = more strength, less precision
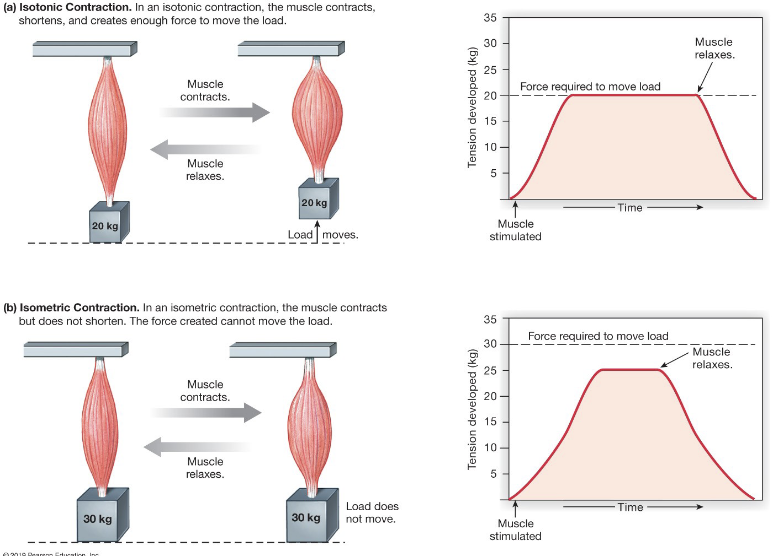
Contraction Type
Isotonic
same tension, length changes, causes movement
Isometric
same length, tension changes, no movement
All muscle contractions start out as Isometric, then move to Isotonic
Role of elastic elements in isotonic vs isometric contractions
work = force x distance
when there’s enough tension in elastic elements, the muscle will contract (sarcomeres shorten) and lift the load
can isometric contraction perform work?
No, because no movement happens
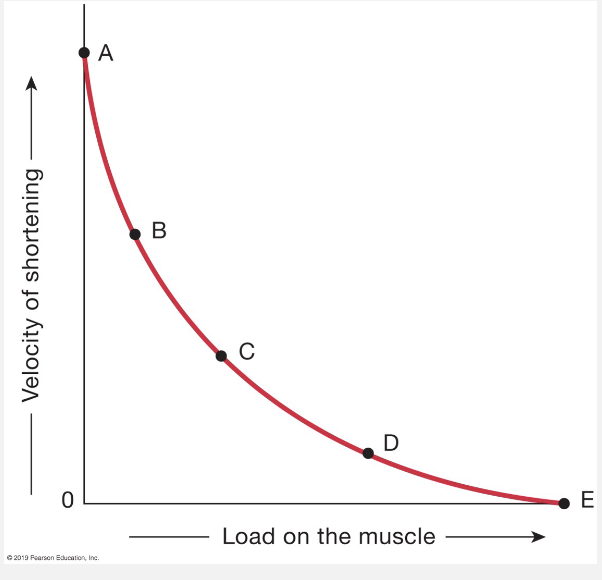
Load-Shortening Velocity
No load, highest shortening velocity
heavy load, slow velocity
Power = load x velocity
Skeletal Muscle Disorders
Atrophy
loss of muscle mass from lack of use
require stimulation from neurons to stay healthy
Neuromuscular Junction
botulism decreases ACh release (Botox)
Myasthenia Gravis (autoimmune disease) blocks ACh receptors
Both
lead to death bc skeletal muscle loss prevents breathing
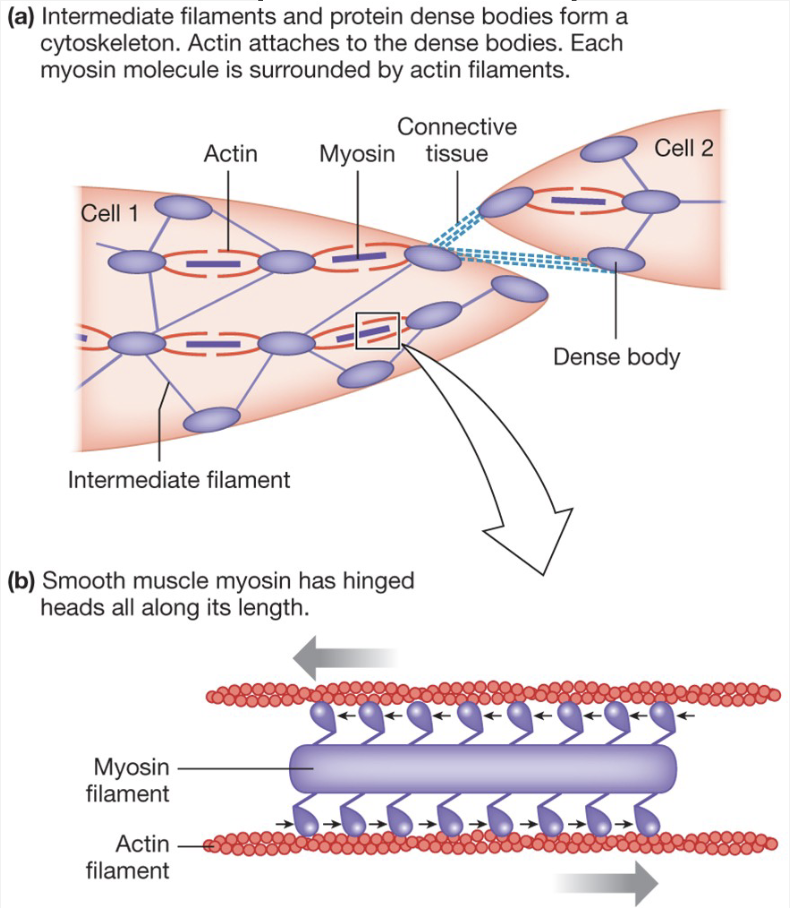
Smooth Muscle: Actin and Myosin Arrangement
Actin and myosin arrangement is irregular → no striations
Contraction still caused by actin and myosin sliding past each other
myosin heads still bind to actin and slide past it
actin is bound to dense bodies
myosin is in middle, actin binds to outside and pulls myosin in opposite directions
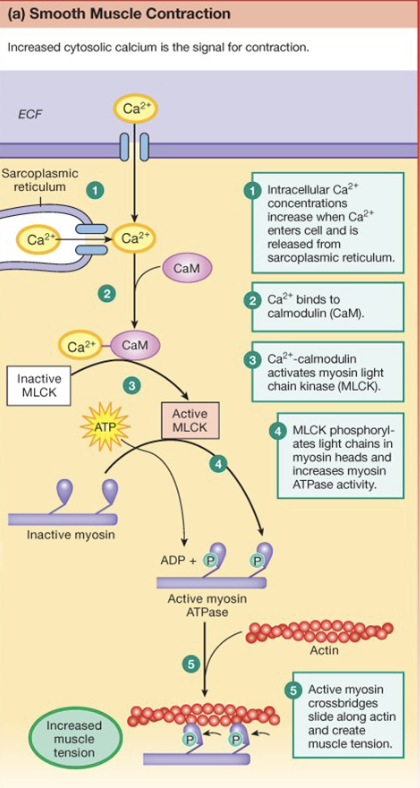
Smooth Muscle - Regulation of Contraction
Cell is depolarized due to Ca2+
Ca2+ triggers Ca2+ release from Sarcoplasmic Reticulum → Ca2+ is from the AP coming into the cell
Ca2+ binds to Calmodulin; complex activates MLCK → kinase adds P to myosin and causes increased affinity to actin
cross-bridges are formed
Myosin Light Chain Phosphatase removes P from myosin → decreases affinity to actin and decreases cross-bridges
smooth muscle: any hollow organ or tube: blood vessels, GI tract, uterus, bladder, etc
Skeletal Muscle Reflexes
Proprioreceptors
tells body where it is in space
muscle spindles (intrafusal fibers)
Golgi Tendon Organ
Joint Mechanoreceptors: found in joints and sense mvts
Efferent Pathways
Alpha motor neurons → extrafusal fibers
Gamma motor neurons → intrafusal fibers
Mechanoreceptors
mechanical stimuli
baroreceptors: pressure
osmoreceptors: cell stretch
hair cells: sound waves
nociceptors: pain, tissue damage
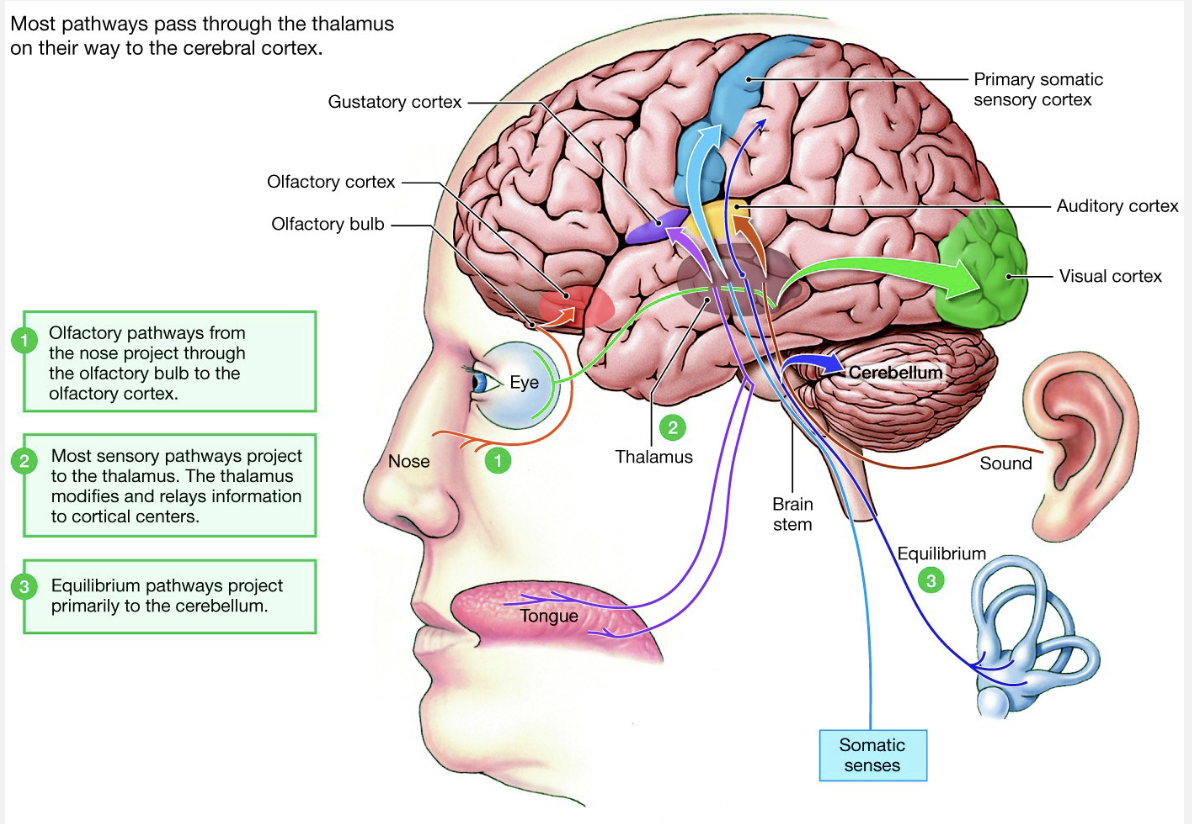
once the stimulus enters the CNS, it’s directed to a specific
Properties of Sensory Systems
sensory receptors are most sensitive to one type of stimuli, BUT can respond to others
sensory information carried to brain based on typical stimulus types
Problems
stimulus type will be perceived incorrectly
rewiring can course incorrect perception of location of stimulus
Modality
type of stimulus
wiring (labeled line coding)
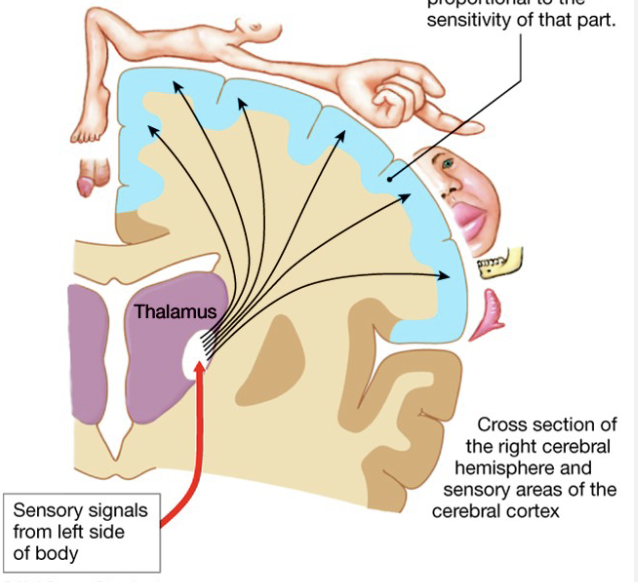
Location
localization in brain wiring
timing: hearing and smell
lateral inhibition
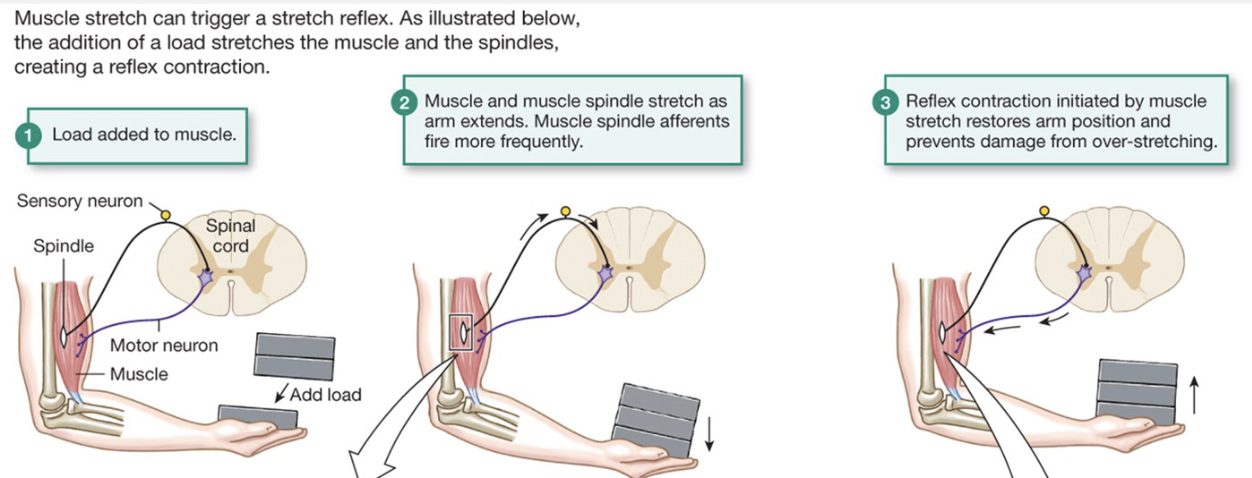
Stretch Reflex
Muscle spindles sense stretch
travel to CNS
Alpha motor neuron: extrafusal fibers contractions
Gamma motor neuron: intrafusal fibers contraction
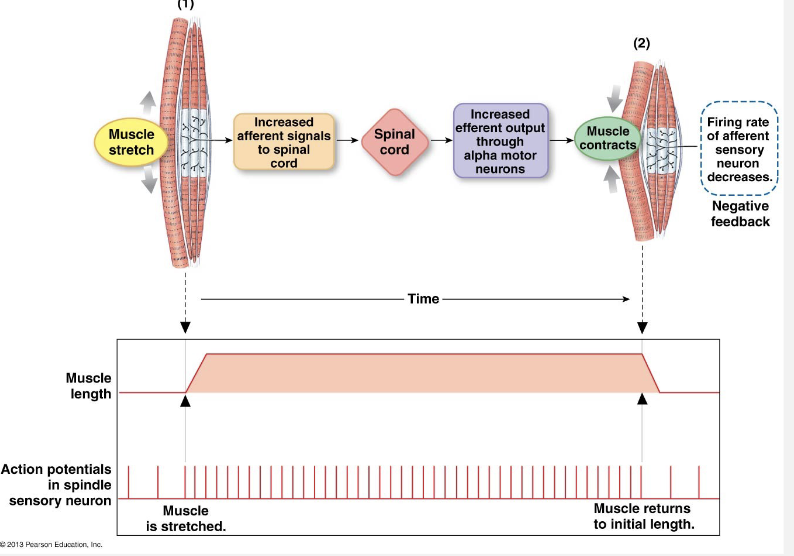
Stretch Muscle/Muscle Spindle Reflex
load added to muscle
Muscle and muscle spindle stretch as arm extends. muscle spindle afferents fire more frequently
Reflex control initiated by muscle stretch restores arm position and prevents damage from over-stretching
Generates more tension so you don’t drop the load
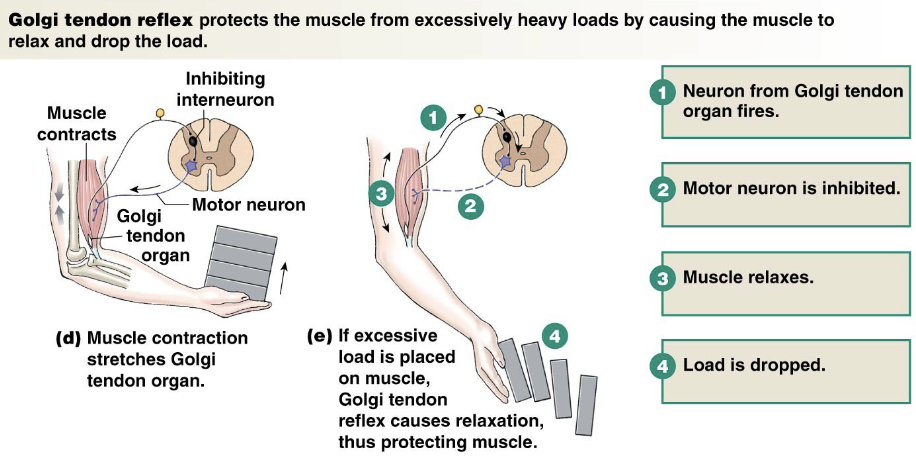
Golgi Tendon Organ Reflex
Golgi Tendon organ senses tension → contraction
inhibits alpha motor neuron activity
protects muscle from injury
Inhibition At Synapses
Receptor
antagonist blocks NT
Selective Presynaptic
axon terminal is inhibited
Global Presynaptic
dendrite is inhibited, no AP is generated in axon
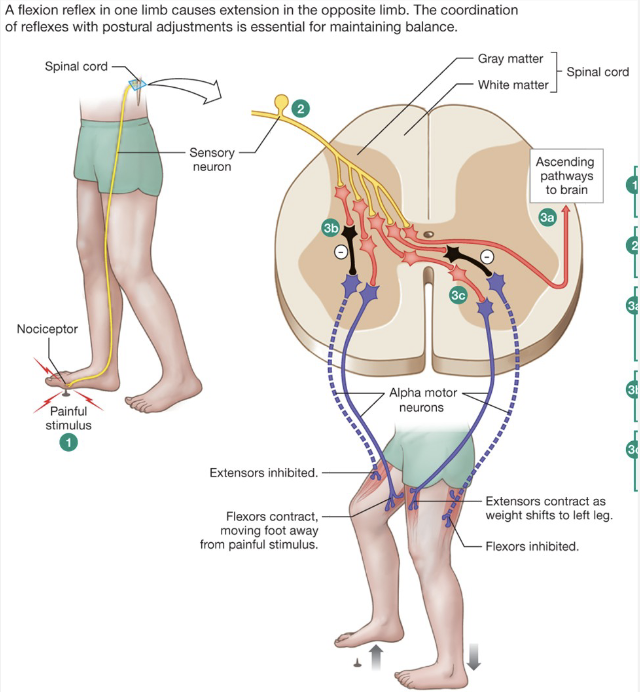
Flexion Reflex and Crossed Extensor Reflex
Nociceptor senses pain
Ipsilateral
extensors inhibited
flexors contract
Contralateral
extensors contract
flexors inhibited
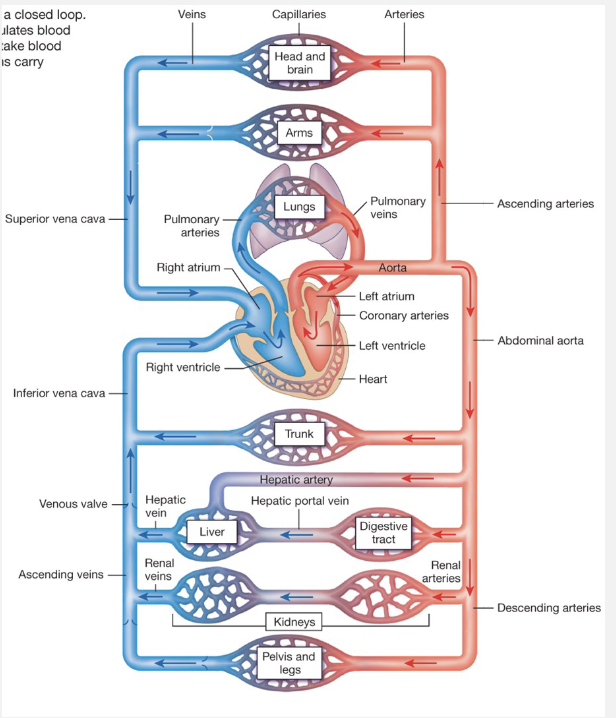
Cardiovascular System
Major Function: Transportation
Gases: O2 and CO2
Nutrients
Waste Products
Immune cels
Hormones
Heat
Anatomical Parts
Heart (Pump)
2 atria
2 ventricles
Blood Vessels
Arteries: Carry blood away from heart
Capillaries: Site of exchange
Veins: Carry blood back to heart
Capillaries: site of exchange
Veins: carry blood back to heart
Blood
Ohm’s Law
V = IR
V = driving force
I = flow
R = resistance
ΔP = FR
P = pressure differences
F = flow of blood
R = resistance to flow
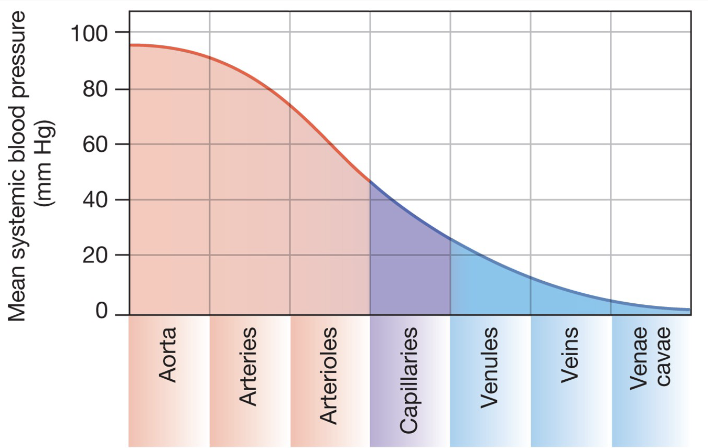
Pressure Gradient
Hydrostatic Pressure
increased by heart pumping
maintained by constriction of arteries
decreases with friction
decreases over distance
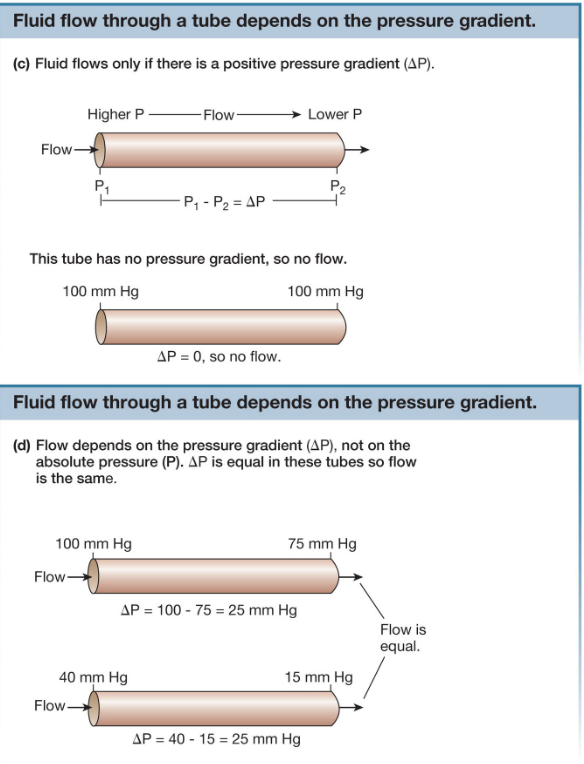
Pressure and Flow
Fluid moves from high to low pressure
Flow is dependent on DIFFERENCES in pressure
pressure and flow are directly proportional
Resistance
R = 8Ln/πr4
L = length of tube
n = viscosity of fluid
r = radius of tube → inversely proportional to resistance. most important factor, can change at a moment’s notice. main regulatory factor. can control it to its 4th factor
The smaller the radius, the greater the resistance
vasodilation and vasoconstriction of arteries
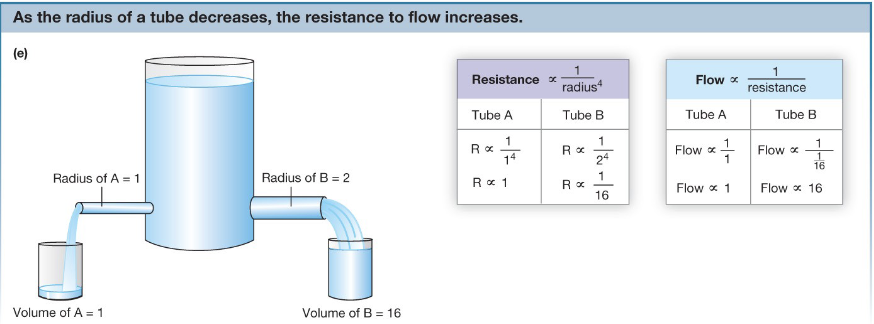
Resistance and Flow
Resistance and flow are inversely proportional
Radius and flow are proportional
the tube with the highest radius and shortest length will have the greatest flow
Flow
Flow rate = volume of blood/time
Flow velocity = speed of blood
same volume of blood in same period of time
the smaller the diameter of the tube, the faster the blood will travel
individual capillaries = slow bc gas exchange
Heart: Generates Pressure Differences
4 Chambers
2 Atria: receives blood
2 Ventricles: sends blood
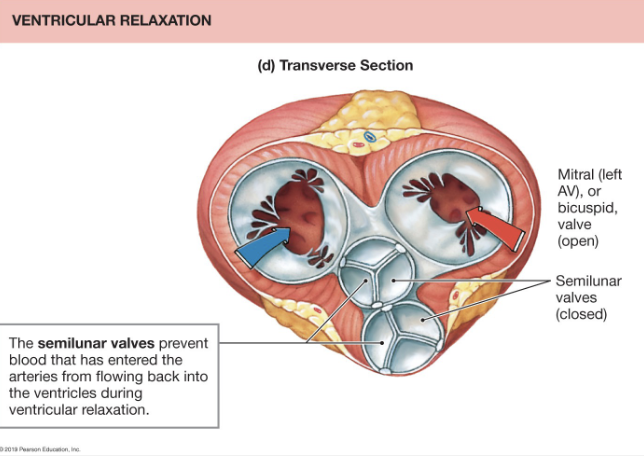
Valves: one way flow
left ventricle has more muscle bc it pumps blood to body, which requires more force
right ventricle has less muscle bc it’s going to lungs = short distance requires less force
Flow of Blood Through Body
Right Atrium, Right AV Valve (tricuspid), Right Ventricle, Pulmonary semilunar valve
Lungs
Left Atrium, Left AV Valve (bicuspid or mitral), Left Ventricle, aortic semilunar valve
Body
How Does the Heart Pump?
Electrical Stimulus
pacemaker cells
modified by autonomic NS
spreads via gap junctions
Mechanical Contraction
linked to electrical stimulus
Contraction Period
same as skeletal
power-stroke cycle
Relaxation Period
Ca2+ returns to SR and ECF by active transport
Ca2+ released from troponin and tropomyosin slides back
Overview of Heart Pumping
pacemaker cells create AP
AP travels through T-tubules
Ca2+ from AP→Ca2+ released from SR
Ca2+ binds troponin, pulling tropomyosin
myosin heads bind to actin, forming cross-bridges
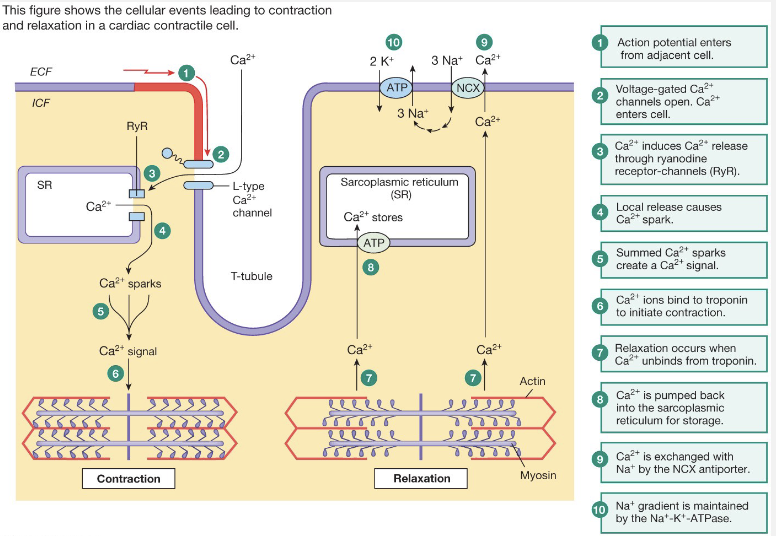
Regulation of Cardiac Muscle Contraction
AP enters via gap junctions
Ca2+ enters, triggers release of more Ca2+ from SR
Ca2+ binds to troponin, moves tropomyosin out of the way
Myosin heads can form cross-bridges with actin
Ca2+ is re-sequestered into SR and pumped out of cell
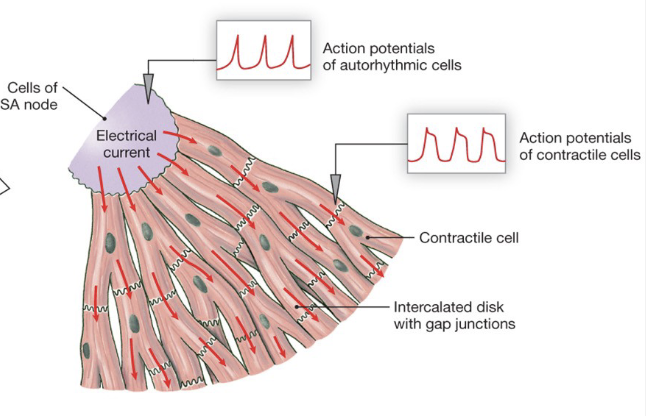
Electrical Stimulation
Due to autorhymic cells
Permeability of membrane changes, causing depolarization
Modified by autonomic division
AP spreads through heart via gap junctions
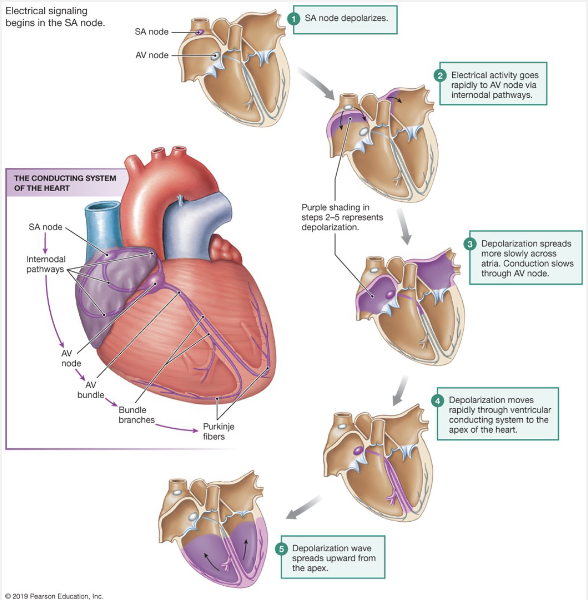
SA (sinoatrial node) → set of pacemaker cells
internodal pathways → used to send depolarized signal to atria
AV node (atrioventricular) delay → set of pacemaker cells, slower rate SA
gives time for atria to top off the ventricle, pushing out the rest of the blood
AV bundle → splits into left and right bundle branches. some pacemaker cells have slower rate
split into conduction myofibers
AV node follows SA node
AV node has its own rhythm, acting as a backup. If atria doesn’t contract, it’s inconvenient, if ventricle doesn’t contract, you die.
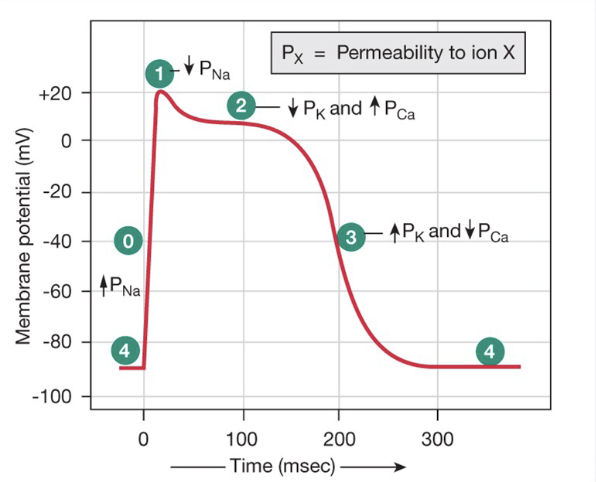
Measuring Electrical Activity
Action potential for contractile
Depolarization = Na+
Plateau = Ca2+
Re-polarization = K+
Note time frame: hundreds of ms. Skeletal muscle = 10s of ms
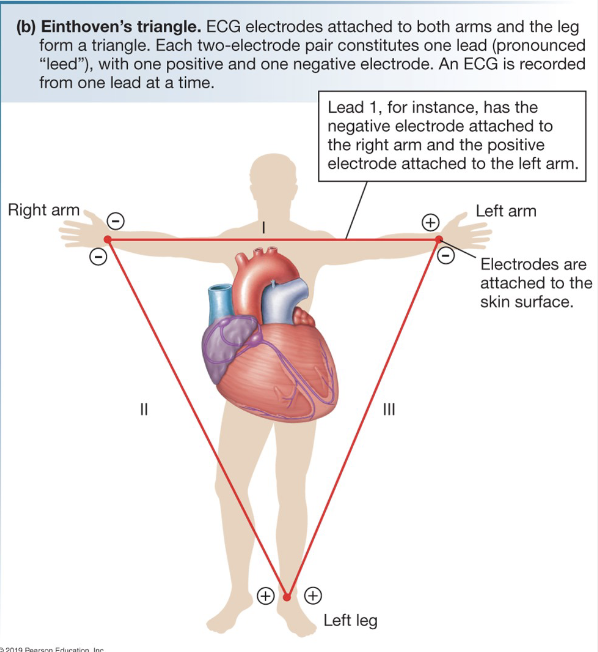
Electrocardiogram (EKG/ECG)
Measures overall electrical activity of heart outside of body
Pattern based on position of leads
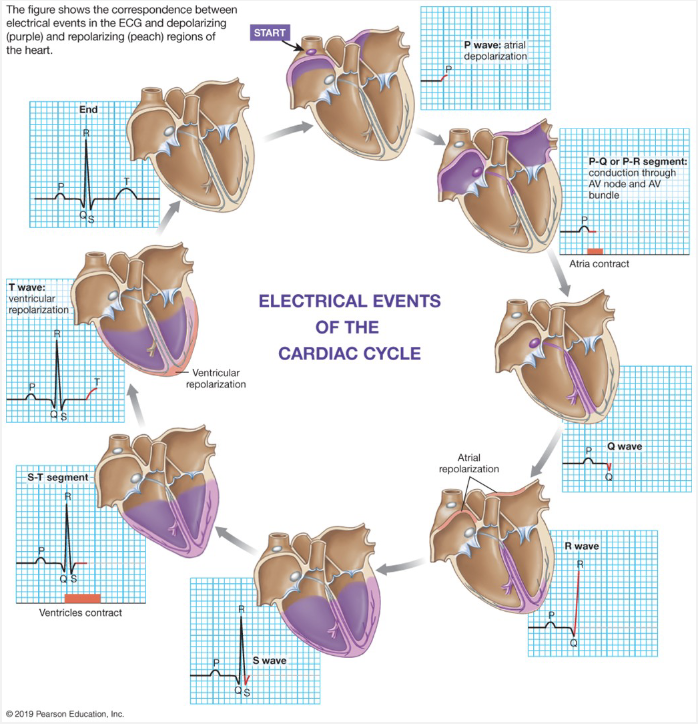
Measuring Electrical Activity:
P-wave
QRS complex
T-wave
P-wave:
(E) atrial depolarization
(M) atrial contraction (red block)
QRS complex:
(E) ventricular depolarization → atrial re-polarization happens during this event
(M) ventricular contraction
T-wave:
(E) ventricular re-polarization → causes T-wave
(M) ventricular relaxation → associated with re-polarization
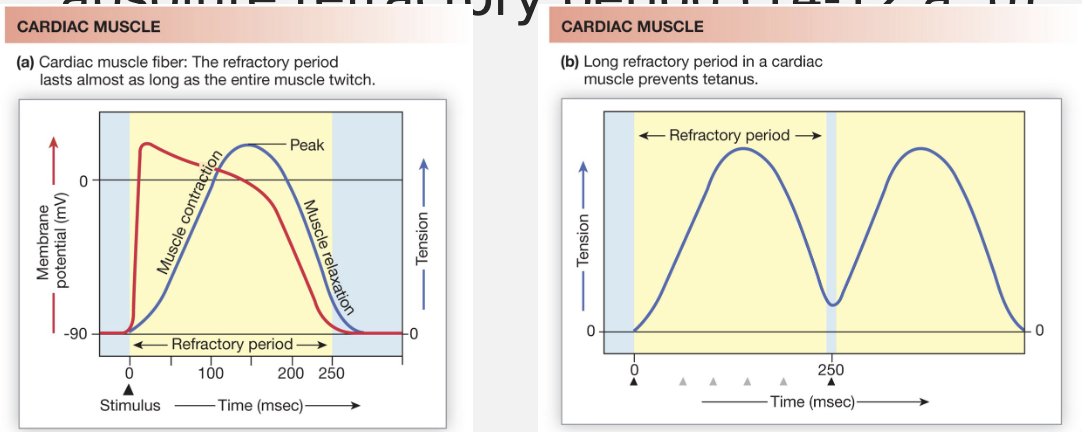
Mechanical Activity
AP trigger contraction
Cardiac muscle contractions cannot be summed, unlike skeletal muscle
No tetanus is possible → mechanism: AP is almost as long as the contraction/relaxation cycle
cardiac AP lasts 100s of ms
Cardiac muscle contraction lasts 100s of ms
Contractions ends about the same time as absolute refractory period
relaxation period of cardiac muscle = filling period of the heath
Cardiac muscle vs Skeletal Muscle
Cardiac
isovolumic contraction
isotonic contraction
Skeletal
isometric contraction
isotonic contraction
Measuring Mechanical Activity
Use indirect measures of cardiac muscle tension and work
Blood pressure (load on heart)
stroke volume (movement of blood out of heart) → volume/beat
Heart sounds (due to pressure changes) → closing of valves creates noise
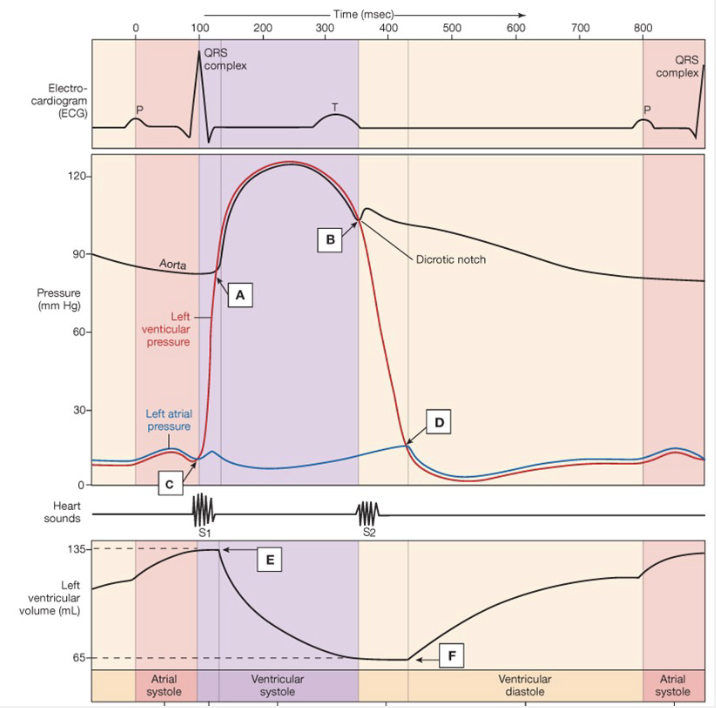
Wigger’s Diagram
P-Wave: atrial depolarization → atrial contraction
atrial pressure increases
ventricular volume increases
QRS: ventricular depolarization → ventricular contraction
left ventricular pressure increases
pushes blood out
heart sound
open aortic semilunar valve
Left Ventricular Volume decreases
pressure starts to decrease
T-Wave: relaxation phase
rapid drop in ventricular pressure
AV valve opens
2nd heart sound
ventricular volume increases
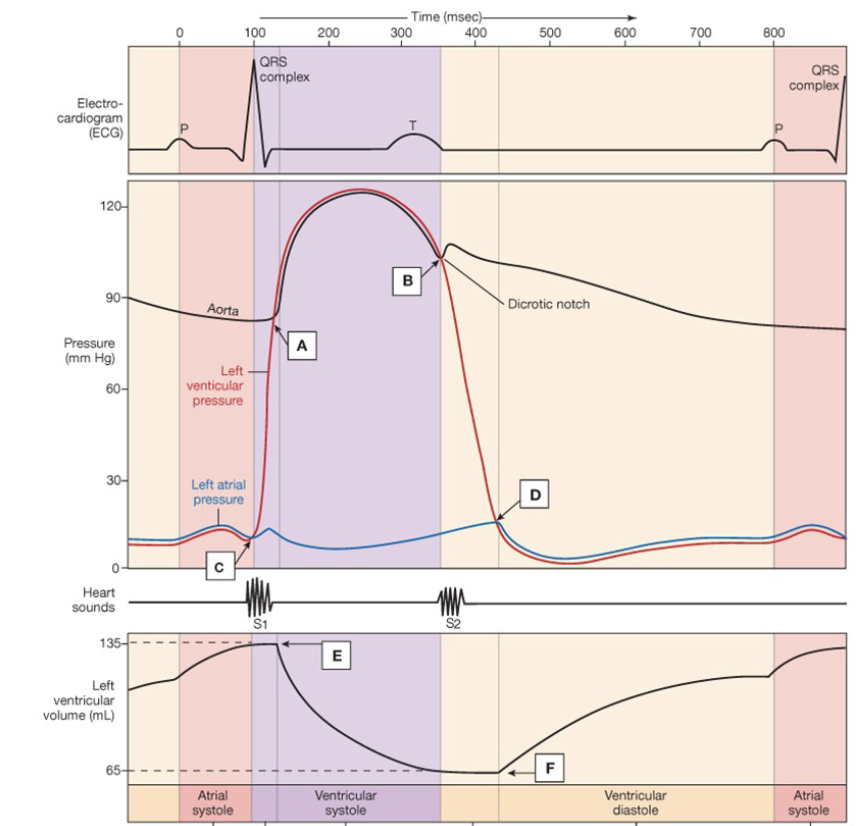
Wigger’s Diagram Summary
Diastolic → point A → # closest to point
Systolic → heart contracts → highest point
end diastolic → heart relaxes → increasing volume
end systolic → heart empties → decreases volume
electric activity → P-wave, QRS, T-wave
heart sounds → valves closing
Calculating Pressures
Blood Pressure
Systolic/Diastolic
Pulse Pressure
Systolic - Diastolic
Mean Arterial Pressure (MAP)
Diastolic + 1/3 Pulse Pressure
e.g. 90 + 1/3(30) = 100 mmHg
Calculating Volumes
Stroke Volume
End Diastolic - End Systolic
e.g. 135mL - 65mL = 70mL
Cardiac Output
Heart rate x Stroke volume
e.g. 70bpm x 70mL = 4900 mL/m
Ejection Fraction
(SV/EDV) x 100%
e.g. (70mL/135mL) x 100 = 51.8%
Calculating Peripheral Resistance
RP = resistance in arteries
ΔP = F x R
MAP = CO x RP
RP = MAP/CO
e.g. 100 mmHg/4.9 L/min → 100 mmHg/5 L/min = 20 mmHg/L/min
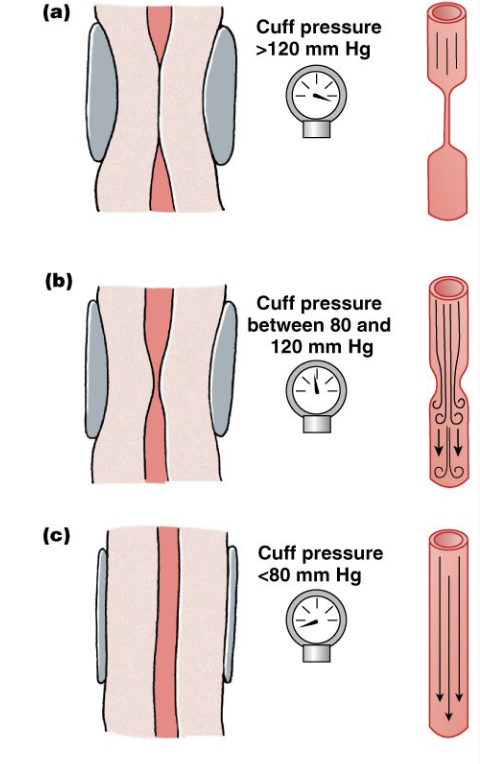
Regulating Mechanical Aspects
Measuring blood pressure
High pressure blocks flow
slowly release pressure
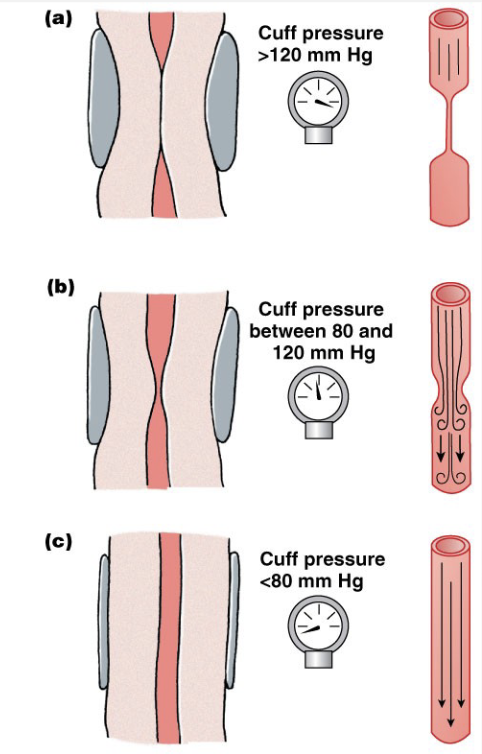
What determines systolic and diastolic pressure?
the point at which you hear “quiet flow” is diastolic pressure
Regulating Blood Pressure
Blood Vessels
Arteries have most control over dilation/constriction → most smooth muscle
Capillary beds can open and close
veins are pliable; serve as blood reservoirs → low smooth muscle, high flexibility
Volume of Blood
high volume = high pressure
drinking large volumes
high [salt] = high osmolarity = high blood volume
high heart rate → doesn’t change total volume, but increases the blood in arterial side
![<p><strong>Blood Vessels</strong></p><ul><li><p>Arteries have most control over dilation/constriction → most smooth muscle</p></li><li><p>Capillary beds can open and close</p></li><li><p>veins are pliable; serve as blood reservoirs → low smooth muscle, high flexibility</p></li></ul><p><strong>Volume of Blood</strong></p><ul><li><p>high volume = high pressure</p></li><li><p>drinking large volumes</p></li><li><p>high [salt] = high osmolarity = high blood volume</p></li><li><p>high heart rate → doesn’t change total volume, but increases the blood in arterial side</p></li></ul><p></p>](https://assets.knowt.com/user-attachments/2e4c4086-0d13-4104-838a-90395d915758.png)
Regulating Volumes and Flow: Stroke Volume
EDV - ESV
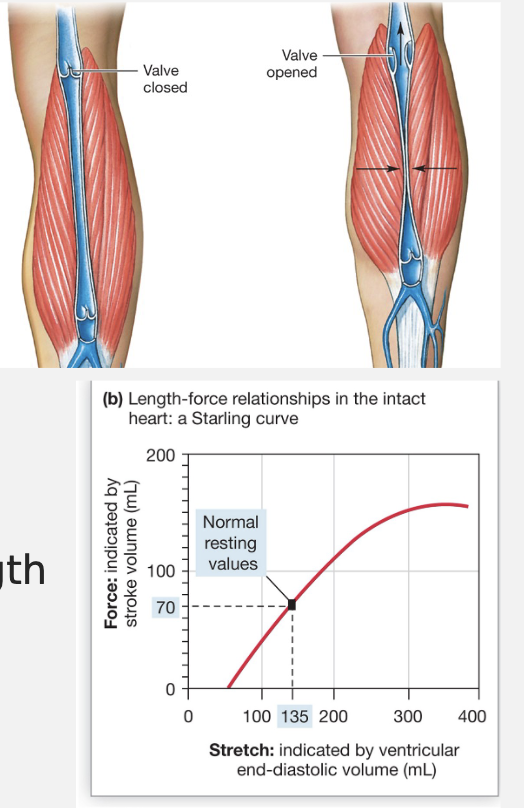
Veinous Return
amount of blood that returns to the heart
Pocket Valves: prevent blood from flowing backwards
Skeletal Muscle Pump: contract muscle and squeezes blood up. When relaxed, the blood could move down, but the pocket valves prevent that.
Respiratory Pump: creates areas of low pressure. When you inhale, there is a decrease in pressure in the thoracic cavity and heart → helps draw blood from the rest of the body back to the heart.
Contractility of the Heart
Increased Ca2+: can’t do mechanical summation because of the longer AP. Cardiac muscle gets Ca2+ from extracellular fluid, if more channels open, more Ca2+ in → more Ca2+: out of SR → generates more force
Sympathetic Division
Increasing Muscle Fiber Length → Frank Sterling Law
increase by changing EDV, increased EDV = increased stretch = increased formation of cross-bridges
creates more force
Regulating Volumes and Flow: Cardiac Output
heart rate: autonomic division
stroke volume
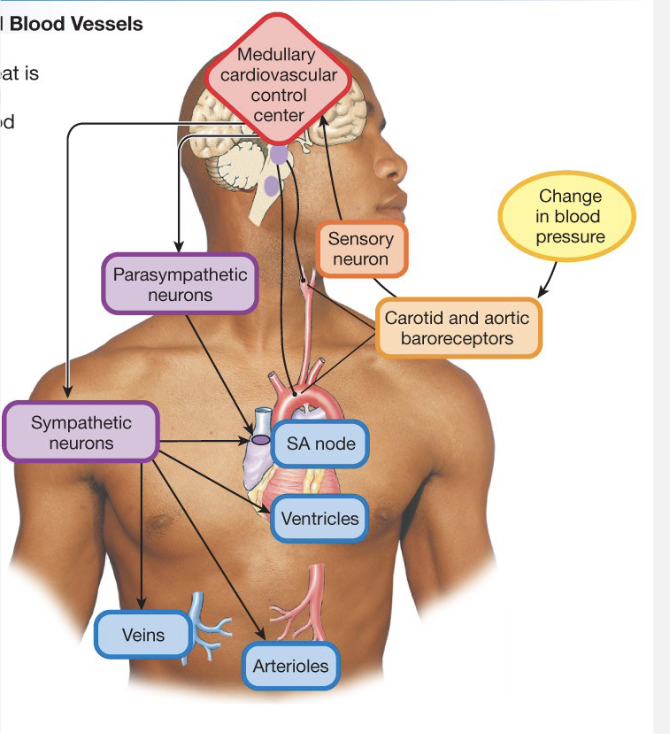
Regulating Mechanical Aspects
Feedback Loops
Sensors
baroreceptors: pressure
increased pressure increases Action Potentials
Carotid bodies: in carotid arteries → go to brain
Aortic bodies: goes out to body
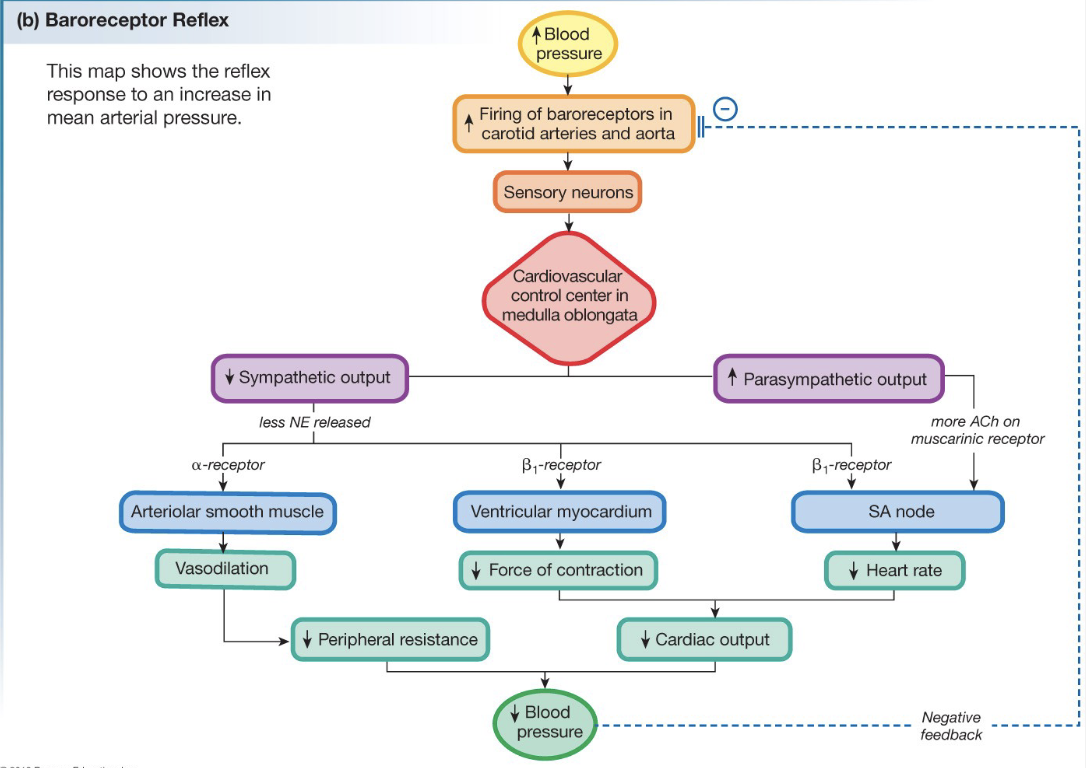
Baroreceptor Reflex Flow-Chart
Controlling Blood Flow
Flow to Tissues is determined by:
Dilation/Constriction of arteries
O2/CO2 levels
H+ levels
K+ levels
NO
Autonomic System
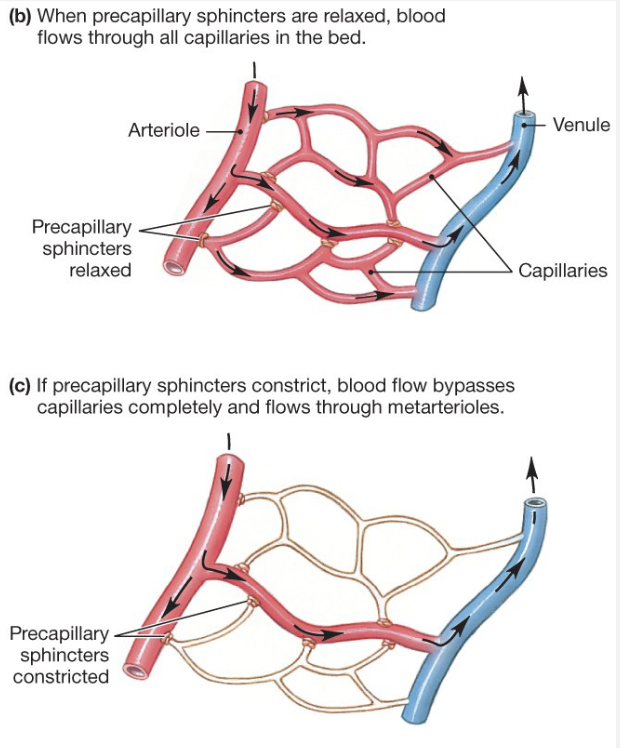
Pre-Capillary Sphincters (PS)
When PSs are relaxed, blood flows through all capillaries in the bed
if PSs constrict, blood flow bypasses capillaries completely and flows through meta-arterioles
PS regulate which capillary beds are open, most often depending on the metabolic needs of the capillary
Exchange at Capillaries
Characteristics
thin walls, small diameters
high density of blood vessels
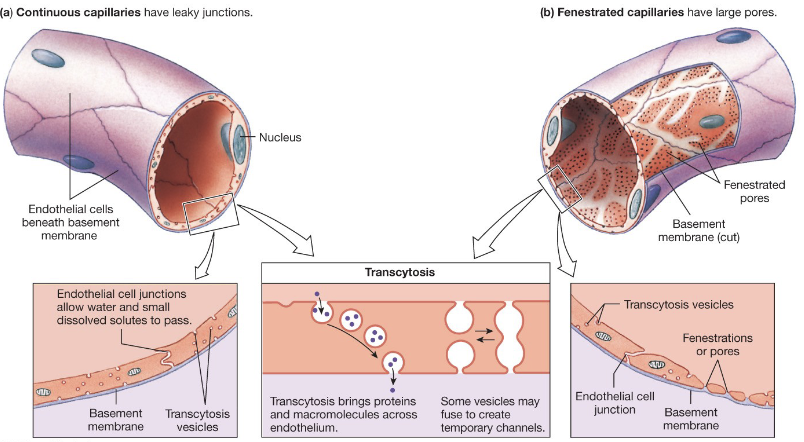
Types
continuous: leaky, most common and basically everywhere → fluids, small particles, no cells/proteins
fenestrated: more leaky → no cells/proteins → found in GI tract, kidneys
sinusoidal/discontinuous: most leaky, least common → leak everything including rbcs, cells, and large proteins → found in bone marrow, spleen, and liver
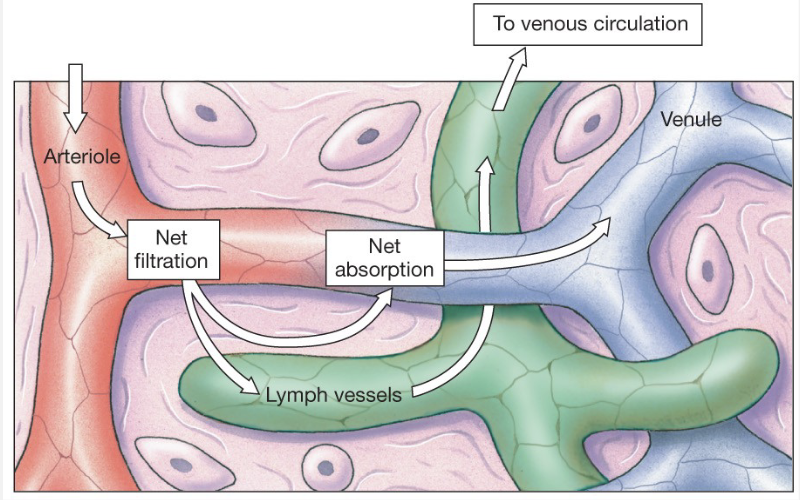
Filtration and Absorption
occur as a result of pressures → constant exchange btw circulatory system and the interstitial fluid
filtration at arterial end
absorption at venule end
excess reabsorbed by lymph system
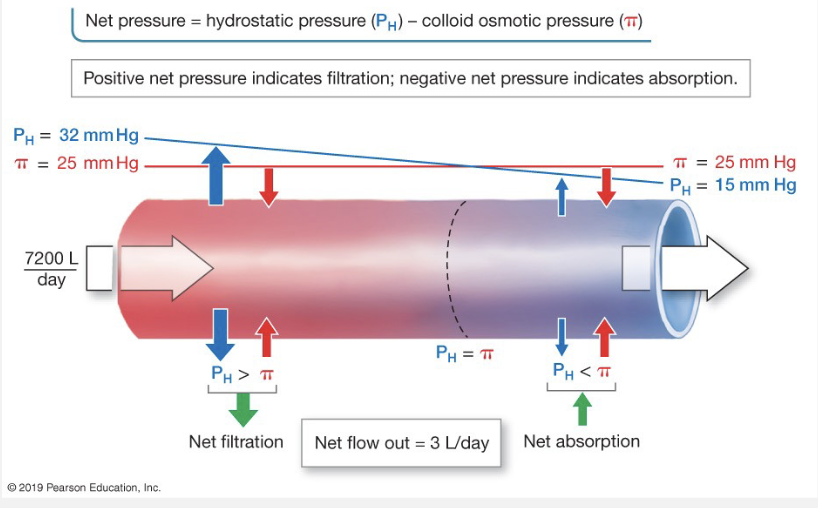
Pressures Affecting Filtration
Hydrostatic pressure
inside and outside of capillary
HP pushes away, goes high to low
beginning of capillary = high HP
end of capillary = low HP
Oncotic (Colloid Osmotic) Pressure
pressure in and out of capillary
increases osmotic pressure in an area
oncotic pulls stuff toward areas of high concentration to dilute them
beginning of capillary = low oncotic pressure
end of capillary = high oncotic pressure → fluid comes back into capillary
Imbalances in the Filtration and Absorption
Edema results from imbalance in the system
Causes of Imbalances
Hydrostatic pressures: higher in cap, lower outside cap
high bp, low interstitial pressure
Colloid Osmotic Pressures: low in cap, high outside cap
Blood Components
Blood cells (red and white) from bone marrow → carry O2 and function in immune system
Plasma: water, salts/ions, proteins/organic molecules, gases → transport cells in fluid
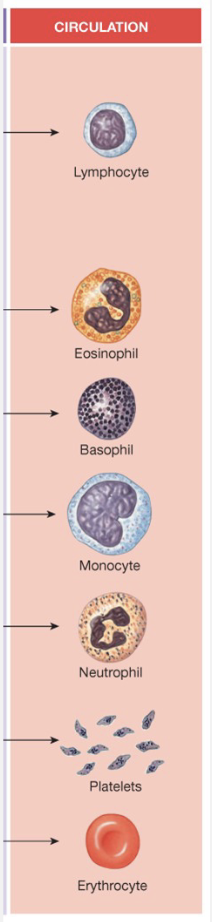
Blood Cells
Erythrocytes → Red Blood Cells
Bind O2 and some CO2
Hematocrit; Erythropoietin increases
Leukocytes → Immune System
eosinophils, basophils, monocytes, neutrophils
Platelets
allows clotting
Plasma
Proteins
Albumin - bind hormones
Globulin - antibodies
fibrinogen - clotting
Organic Molecules
vitamins
glucose
nitrogenous wastes
lipids
The Immune System
Major Functions
protect against invaders
remove dead/damaged cells
identify and remove abnormal cells
Major pathogens
bacteria
viruses
Bacteria
Structure
cell w/ cell wall
occasional capsule
Living Conditions
anywhere
Reproduction
by itself
Antibiotics
susceptible when not resistant
Viruses
Structure
DNA or RNA encased by proteins
Living Conditions
must have a host
Reproduction
must have a host → uses host machinery
Antibiotics
not susceptible, it’s a virus