lect 3 - artificial set up, modelling, investing with/without shaft, completion of partial denture, immediate partial dentures, kennedy dentures and dentures with pelots
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
prognosis
medical prediction regarding likely course, duuration and outcome of a disease/injury
also includes chance of recovery or recurrence
deciding whether a tooth is worth including in prosthetic treatment
understanding that with appropriate maintenance the tooth provides a reasonable 5 year prognosis for survival
do they require restoration with surveyed crowns?
how much do they provide to the prosthesis, support/retention?
any splinting needed?
is it symmetrical as this will affect distribution
is there a strong patient desire to maintain teeth?
comparative functional expectations between a mucosal-borne denture and RPD that uses teeth for some support, stability and retention
restoration with surveyed crowns
specialised full-coverage restorations designed to support RPDs by creating optimal contours, guide planes and rest seats
wax rim and types
prismatic bodies made of pink wax cross section 1cm2
compensate the atrophy of alveolar ridges
prefabricated
laboratory made
elliptical (for maxilla)
parabolic (for mandible)
guides
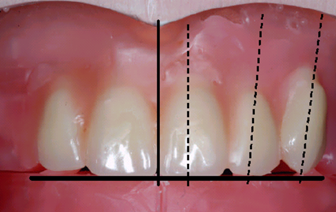
guidelines :
midline
high lip line
canine line
proper placement of occlusal plane
proper lip support
correct jaw relationship (vertical dimension of occlusion and centric relation)
alveolar ridge resorption
in anterior maxilla its
anterior mandible is down and lingual
anterior maxillary teeth setting
central incisor :
incisal edge contacts the horizontal plane
long axis parallel to sagittal plane
frontal inclination 5-8o
overlap with lover incisors should be 1
lateral incisor :
0.7mm-1mm above the horizontal plane
sagittal inclination 10-20o
frontal inclination 8o
canine :
cusp in contact with plane
sagittal inclination 7-10o
axial rotation of the crown so that when viewed from the front only the mesial part is visible
neutral zone
potential space between the lips/cheeks and tongue where the forces between the tongue and cheeks are equal
area of equilibrium is the neutral zone
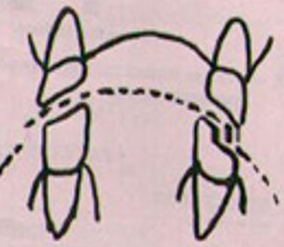
position of posterior teeth in relation to alveolar bone
on the ridge crest
important for lower denture stability
balanced occlusion
bilateral simultaneous, anterior and posterior occlusal contact of teeth in centric and eccentric position
eccentric position includes lateral and protrusive positions in both working and balancing sides
central occlusion and eccentric
central is the maximum intercuspation (tighteest fit) of upper and lower teeth - bite
eccentric is any tooth contact during mandibular movement away from that central position
CO stationary
EO movement
compensating curve
curving in anteroposterior median plane and mediolateral frontal plane
alignment of occluding surfaces and incisal edges used to develop balanced occlusion
its the arc introduced to construct complete RPD to compensate for the opening influenced produced by the condylar and incisal guidance during lateral and protrusive mandibular excursive movements
anteroposterior curve (curve of Spee)
anatomic curve made of occlusal alignment of teeth with the cusp tip of mandibular canine following the buccal cusps of the premolar and molars till it reaches the anterior border of the mandibular ramus ending at the mandibular condyle
curve of monson
ideal curve of occlusion where each incisal edge conforms to a segment of a sphere 8 inches in diameter at the crista galli
curve of Wilson
mediolateral curve
occlusion should be spherical, lower bridge is concave adn upper bridge is convex, the curvature in the lower arch is affected by equal lingual inclination of right and left molars so the tip points can be placed on the circumference of a circle
curve of Villain
in abrasion
max post teeth contact
posterior buccal surfaces make contact with a straight line drawn from the labial surface of the canine and the premolar and vestibular surfac eof the molars 155o
poster
upper premolars and molars
1st premolar - contacts horizontal plane buccal cusp ONLY
2nd premolar - contacts horizontal plane BOTH cusps
1st molar - horizontal plane mesiolingual cusp, mesiovestibular cusp 0.5mm, distolingual cusp 1mm, distovestibular cusp 1.5mm over plane
2nd molar - mesiobuccal cusp 1mm above planne, distobuccal cusp 1.5mm above plane, palatal cusp closer to or lightly contacting plane
lower premolars and molars
1st premolar - vestibular cusp in contact with central groove of antagonist
2nd premolar - vestibular cusp in contact with central groove of antagonist
1st molar - key of occlusion, MV of upper 1st contacts groove between MV and DV cusps on vestibular surface of lower 1st molar
2nd molar - vestibular cusps in contact with central groove of antagonist
snowshoe principle
best support with least load per unit area
secondary retention
adhesion is the attraction of saliva to the denture and tissues
cohesion attraction of molecules to saliva to eachother
atmospheric pressure dependent on a border seal and results in a partial vacuum beneath the denture base when a dislodging force is applied
physiologic molding of tissues around the polished surface of the denture
effects of gravity on mandibular denture only
maxillary distal extension
bases are extended buccally within physiologic tolerance of borders structures
it covers both the maxillary tuberosities and extend into the pterygomaxillary notches and provide adaptation along the posterior border
makes sure it doesn’t extend into the soft palatal flexure
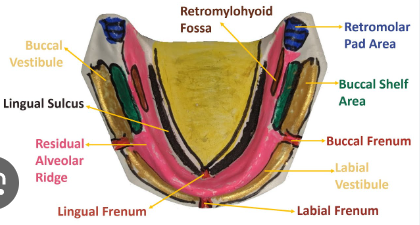
mandibular bilateral distal extension
bases are extended buccally within physiologic tolerance of borders structures
cover retromolar pads and extend into retromylohyoid fossae
basic principles of denture base
width of denture base is inversely proportional to number of abutment teeth (less abutment larger base)
denture base material (acrylic resin or dental alloy)
artificial teeth must respect the form and position of natural teeth
flasking key times
after putting both moulds together with the model being isolated put in boiling water for 3 minutes
any longer will melt the shellac making it harder to remove
open and rinse wax and remove shellac
isolate when flask is still hot
put acrylic in press and leave in for 20 minutes
run under cold water for 5-8
long - put flask in at room temp heat for 30 mins while temp rises to 60c leave at 60 for 1hr heat for another 30min till 100c and slow cool for 2.5 hrs
instruments
steel burs
tungstene carbide burs
diamond
cutters which are metal or carbide
abrasive stones (corundum or carborundum)
abrassive separators (corundum, steel, diamond)
sandpaper
abrasive rubber
brushes
polishing pastes
Kemeney denture indications to use
RPD with plastic dento-alveolar clasps
abutment teeth mobility I-II degree
caries resistant teeth
retentive alveolar ridge
esthetics - priority

Kemeney denture indications not to use
teeth with no vestibular infrabuldge
caries unresistant teeth
nonretentive alveolar ridge

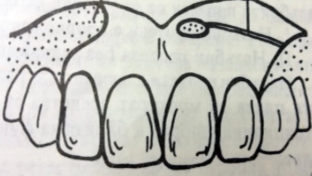
indication for RPD with pelots
mobile teeth
retentive alveolar ridge
in upper frontal area
immediate RPD ad/dis
any removable dental prosthesis fabricated for placement immediately after removal of natural teeth
indications : pathological teeth mobility III in the visible zone
ad :
high psych-prophylactic effect
preserving the height of occlusion
short period for adaptation
conductive influence of denture towards the healing process of extraction wound
dis :
need of relining after 2-3 months
*The mobile teeth should be ligatured before taking the impression from the mouth, if there is a high risk of
preliminary extraction