Unamplified Singing in Classical Styles
1/30
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
31 Terms
Anatomy of the Larynx
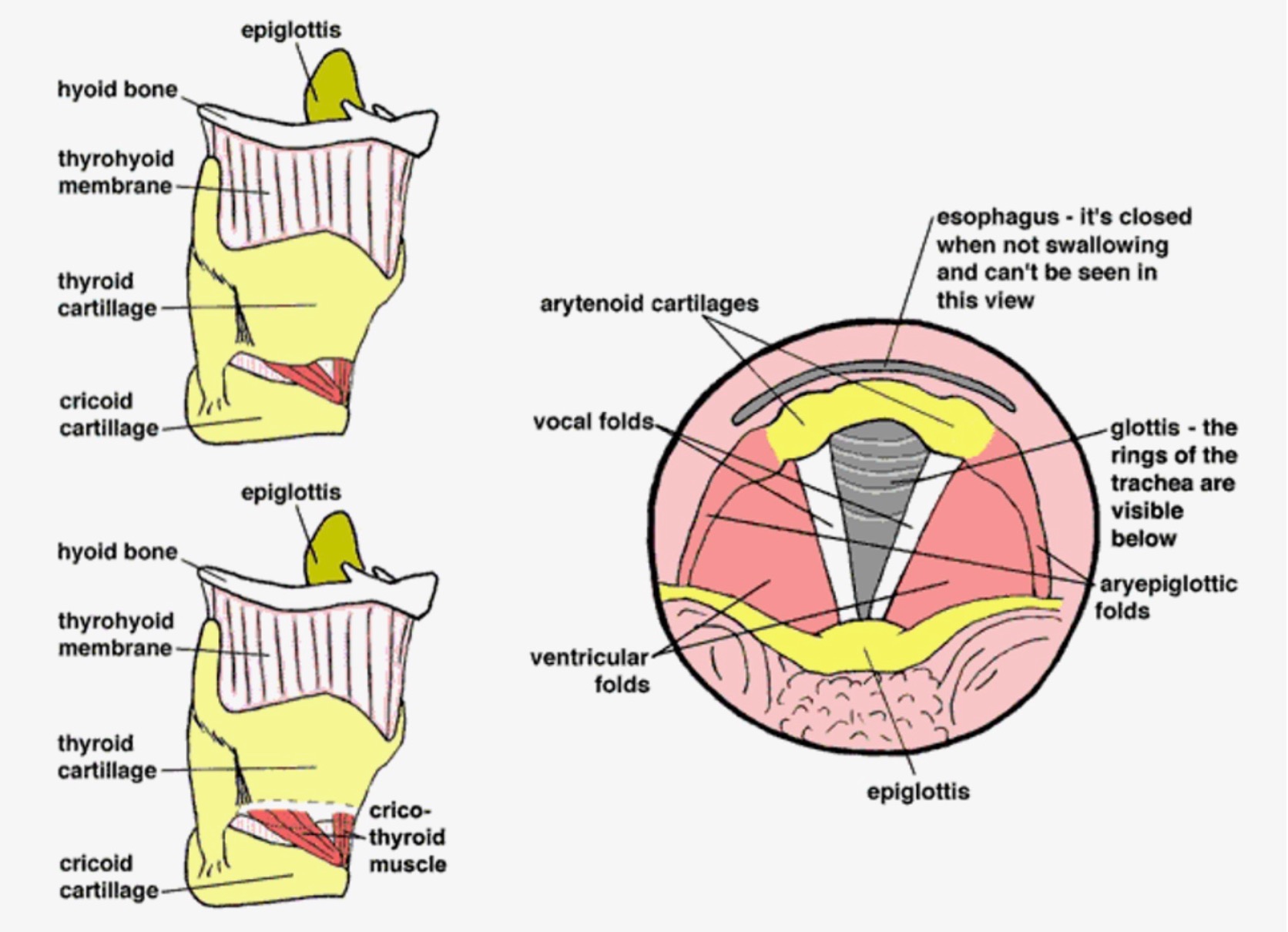
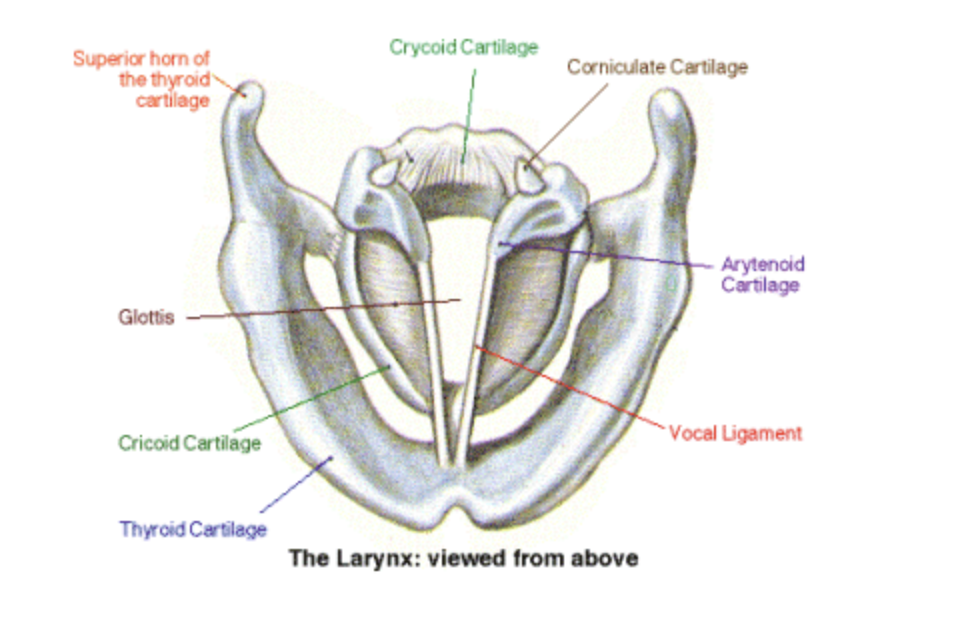
Cricoid cartilage - As the top ring of the trachea, the cricoid cartilage is shaped like a signet ring, wider in the back than the front.
Thyroid cartilage - the thyroid cartilage fits over the cricoid cartilage, and is hinged so that it can slightly rock forward and downward. The thyroid cartilage comes to a point in the front; this point is termed the thyroid notch, but is commonly called the Adam's Apple. The vocal folds attach at the inside of the thyroid notch.
Arytenoid cartilages - These sit atop the back of the cricoid cartilage and hold the back end of the vocal folds. The arytenoid cartilages can rock, glide, and pivot, thus controlling the movement of the vocal folds.
Vocal Folds - These remarkable structures provide a valve for the airway and also vibrate to produce the voice. The vocal folds are multilayered structures, consisting of a muscle covered by a mucosal covering.
Glottis - This is the space between the two vocal folds. When the vocal folds adduct, the glottis closes; when the vocal folds abduct, the glottis opens. The adjectives "glottal" and "glottic" are used to describe many aspects of vocal fold movement. The glottis opens and closes during vibration. Refer to the corresponding pictures.
Epiglottis - This soft cartilage serves as part of the protective swallowing mechanism. It folds backward over the glottis during a swallow so that food and liquids do not go into the lungs. It is not involved in normal voice production.
Hyoid Bone - This horseshoe-shaped bone is positioned slightly above the thyroid cartilage and is the only bone in the body not connected to any other bone. The hyoid bone provides the attachment for many of the muscles of the tongue, jaw, and neck.
https://med.umn.edu/ent/patient-care/lions-voice-clinic/about-the-voice/how-it-works/anatomy
Intrinsic Muscles of the Larynx
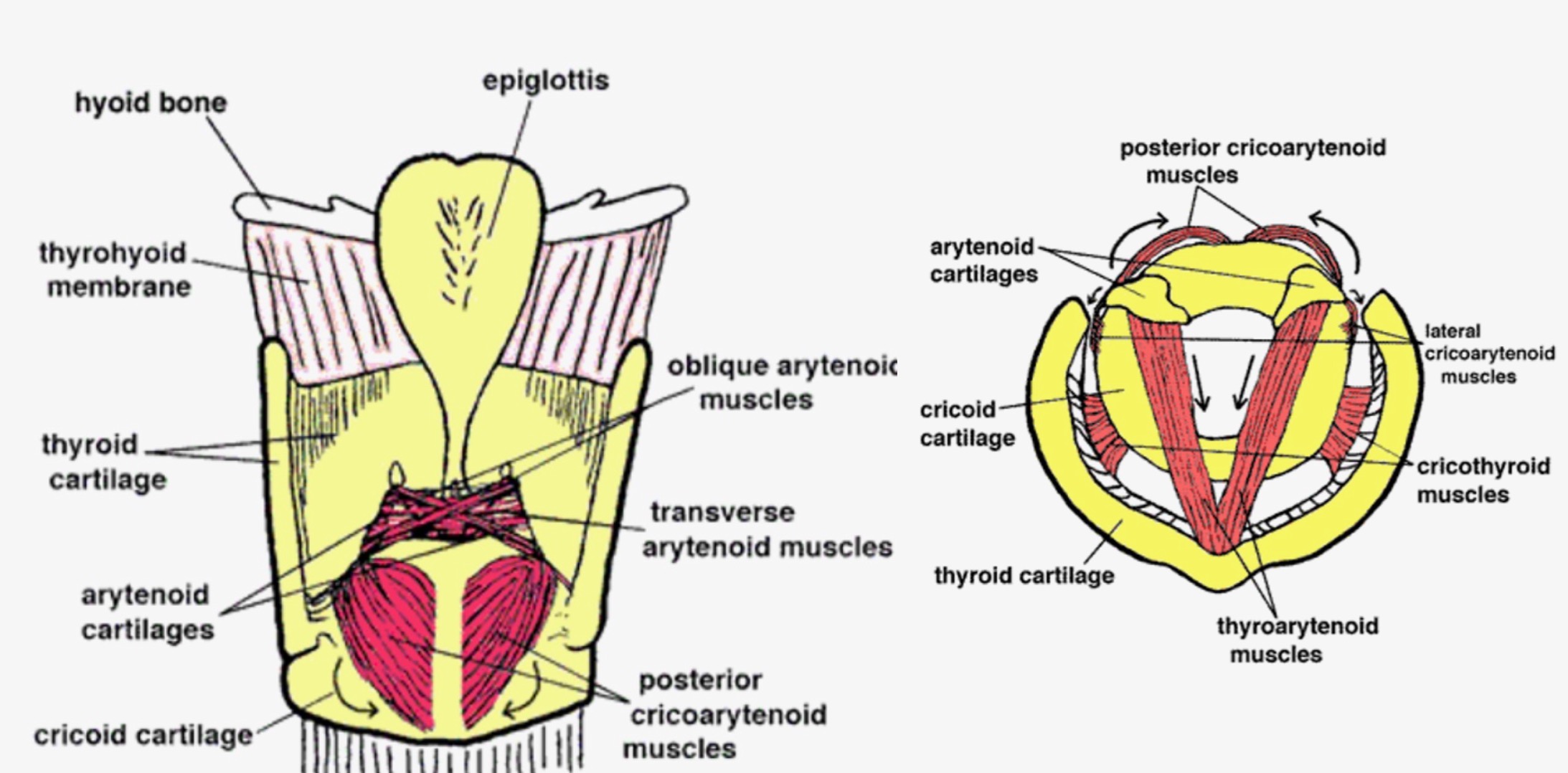
All these muscles are paired (symmetrically arranged on the left and right sides of the larynx).
Posterior cricoarytenoid - These are the only muscles involved in abduction. They open the glottis by pulling the back ends of the arytenoid cartilages together. This pulls the front ends (where the vocal folds attach) apart, therefore pulling the vocal folds apart. PCA = pull cords apart
Lateral cricoarytenoid - These are adductors. They close the glottis by pulling the back end of the arytenoid cartilages apart. This pulls the front ends together, making the vocal folds come together.
Thyroarytenoid - These are the muscles that form the body of the vocal folds themselves. They shorten the vocal folds by pulling the arytenoid (back) end of the vocal folds toward the thyroid (front) end. This shortens the vocal folds and bunches them up, which causes them to vibrate more slowly, thus lowering pitch. The thyroarytenoid muscles also have a force to strengthen glottic closure. That is, they help bring the vocal folds together and keep them together to resist the airstream from the lungs.
Cricothyroid - These are the vocal fold lengtheners. They pull the thyroid cartilage down and forward on its hinge, which increases the distance between the arytenoids and the thyroid notch (the Adam's Apple), thereby lengthening and tightening the vocal folds; this causes them to vibrate faster, thus raising pitch.
Interarytenoids - There are 2 sets of these: the transverse arytenoids and the oblique arytenoids. They bring the two arytenoid cartilages together to provide medial compression for the vocal folds. In other words, the vocal folds squeeze together tighter to resist the air pressure from the lungs (shown on figure 7).
https://med.umn.edu/ent/patient-care/lions-voice-clinic/about-the-voice/how-it-works/anatomy
Extrinsic Muscles of the Larynx
These are the muscles of the front of the neck and jaw that surround the larynx. The muscles of the front of the neck are also collectively referred to as the "strap" muscles.
There are many to give the head and jaw their wide variety of movements. These muscles can provide stability for the larynx during phonation.
Though each of the strap muscles is responsible for a single specific movement, when there's tension in the neck, the muscles tend to contract as a unit (all at once). This tension can make it harder for the intrinsic laryngeal muscles to do their job. Extrinsic laryngeal muscle tension is a factor in many voice disorders
https://med.umn.edu/ent/patient-care/lions-voice-clinic/about-the-voice/how-it-works/anatomy
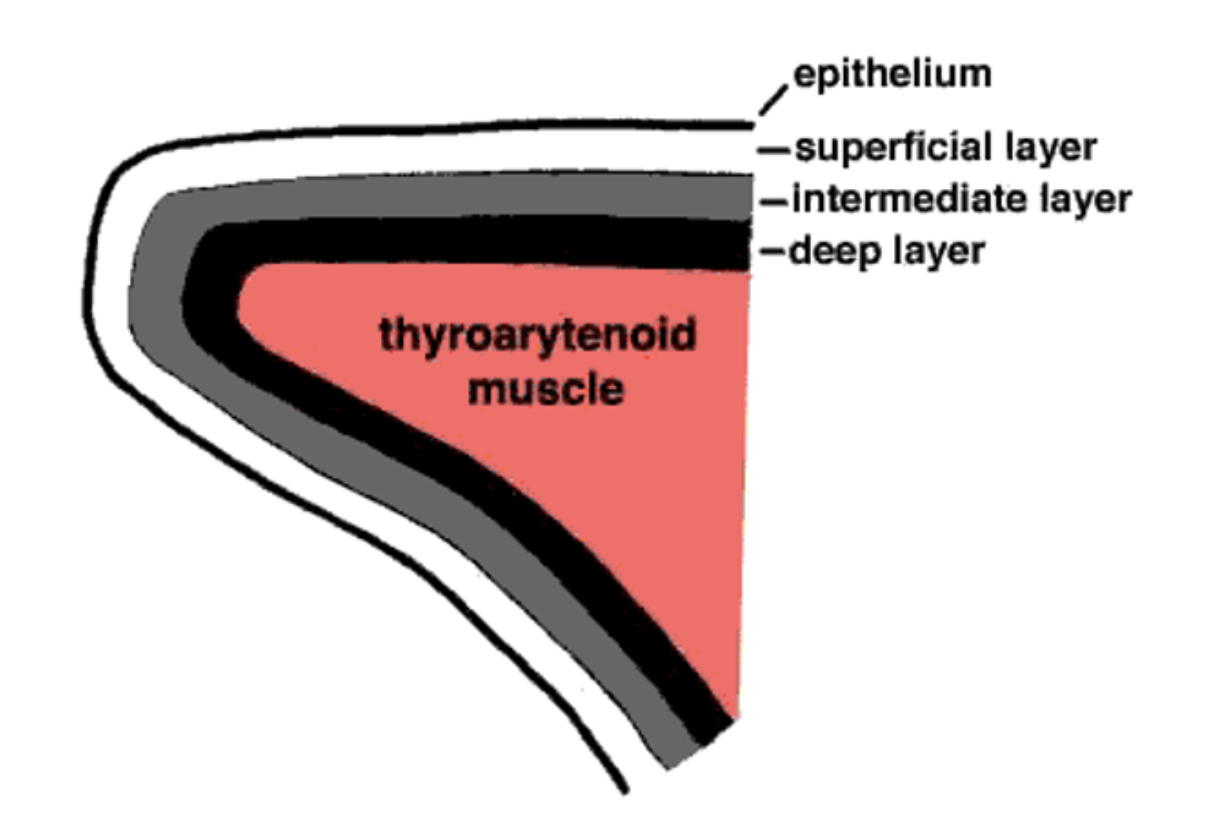
Vocal Fold Structure
Vocal folds used to be called vocal cords (and are still often referred to that way) because it was thought that they vibrated much like strings on a violin. Also, from above, as seen from the laryngeal mirror, they do look like little pieces of cord. Now, we know more about them.
Nervous System and Innervation of the Larynx
Innervation: how the brain communicates with the body's muscles and tissues using nerves. Nerves carry signals from the brain to activate muscles and carry sensory information back to the brain. There are 12 cranial nerves that innervate the neck and head.
Vagus nerve: the 10th Cranial Nerve and primary nerve responsible for the innervation of the larynx. Branches into the RLN and SLN
Recurrent Laryngeal Nerve (RLN):
Innervates all the intrinsic muscles of the larynx except the cricothyroid muscle.
Called "recurrent" because it travels down to wrap around the aorta before coming back up to attach to the larynx (on the left side)
Injury can lead to Vocal Fold Paralysis, leading to hoarseness and aspiration
Superior Laryngeal Nerve (SLN):
Innervates the cricothyroid muscle
Swallowing Mechanics
Swallowing is a coordinated process involving the closure of the glottis by the adduction of the vocal folds and the folding of the epiglottis over the glottis, along with the elevation of the larynx, to ensure that food and liquids pass into the esophagus and not the trachea (windpipe).
Mechanics of Swallowing
The larynx separates the respiratory and digestive tracts. The larynx’s biological purpose is to protect your lungs from food and water. Voice production is secondary.
The epiglottis (piece of soft cartilage located on the top of the larynx) folds backward over the glottis
The glottis (space between VF) closes tightly during swallowing. This adduction of the VF forms a valve that tightly seals to protect the airway
Simultaneously, the larynx rises up, and the esophagus opens to allow food and water to enter
If food or water goes "down the wrong pipe" and hits the vocal folds, a cough reflex is triggered to expel the substance and keep it out of the lungs. This mechanism is very fast (second only to an eye blink)
Basic Swallowing Anatomy Chart
https://www.ohsu.edu/ent/voice-swallowing-anatomy
Physiology of Voice Production
During phonation, the vocal folds are brought together (adducted) by the contraction of the lateral cricoarytenoid muscles (LCA), interarytenoid muscles (IA), and thyroarytenoid muscles (TA).
Air comes out of the lungs, through the trachea, and into the larynx. The air makes the vocal folds vibrate. The vibration is due to the vocal folds alternately trapping and releasing air.
Each release sends a little puff of air into the pharynx and is the beginning of a sound wave. The sound wave is enhanced as it travels through the vocal tract
The frequency of these vibrations determines the pitch of the sound, while the strength of the air explosion and vocal tract enhancement influence the loudness
https://med.umn.edu/ent/patient-care/lions-voice-clinic/about-the-voice/how-it-works/physiology
Vocal Fold Vibration and Pitch
Hertz (Hz) is the term for vibrations, or cycles, per second
The speed of vibration changes the frequency (faster = higher)
Men's vocal folds vibrate around 90 - 500 Hz
Women's vocal folds vibrate around 150 - 1000 Hz
Every time you go up an octave, you double the frequency of vibration
The cricothyroid (CT) contributes to higher pitch by pulling the thyroid cartilage forward and downward, stretching the vocal ligaments
The thyroarytenoid (TA) contracts, brings the arytenoid cartilage closer to the thyroid cartilage, resulting in a slackening or loosening of the vocal ligaments, which produces lower pitch sounds.
The vocalis muscle (part of the TA) makes small adjustments that change pitch and voice quality
https://med.umn.edu/ent/patient-care/lions-voice-clinic/about-the-voice/how-it-works/physiology
Vocal Fold Vibration & Loudness
Loudness is determined by subglottal pressure and vocal tract shaping
There is an "explosion" of air after a closed phase in the vocal fold vibration cycle. A longer closed phase leads to a greater buildup of subglottal pressure and a stronger explosion
The sound wave generated at the vocal folds is shaped and enhanced by the vocal tract which acts as a resonator, influencing the final perceived loudness
Amplitude
The amplitude of vibrations relates to the strength of the sound wave and influences the loudness we perceive. A greater amplitude generally leads to a louder sound.
The relationship between amplitude and perceived loudness is not a direct one-to-one correlation. Acoustic scientists differentiate between the amplitude of vibration, the intensity (sound pressure level), and the perceived loudness, as these are measured differently
https://med.umn.edu/ent/patient-care/lions-voice-clinic/about-the-voice/how-it-works/physiology
Alignment
Alignment refers to how the head, shoulders, spine, hips, knees, and ankles relate and line up with each other in order to transfer weight via an aligned skeletal structure. Proper alignment of the body puts less stress on the spine and helps reduce the need for muscular bracing.
● The vertical balance of the weight of the body on the skeletal structure via aligning weight transfer points: Atlanto-occipital joint (between the ears) over the shoulders, hip joints, knees, and the arch of the foot
● Vertically balanced pelvis, neither tipped forward nor rolled under
● Unlocked knees
● Shoulders released to the sides, neither curled forward, nor overly
pulled back
● Chest comfortably expanded (i.e., not collapsed, slumped)
● maintained by free, subtle micro-movements (not fixed or rigid)
Messa di voce
Literally, placing of the voice. To crescendo (increase volume) and decrescendo (diminish volume) a sustained pitch (tone) from soft-to-loud-to-soft dynamic levels.
Acoustic efficiency
Shaping the vocal resonator in such a way as to provide an acoustic “boost” to the sound; getting the most “gain” with the least expenditure of energy.
The way the sound wave is enhanced by the vocal tract is "the MOST Important factor affecting loudness!"
Search for Efficient Voice Production Article:
the ease in which glottal airflow is converted to acoustic pressure at the mouth
use of the vocal tract to create an "inertial suction effect" that delays the reduction of glottal flow, thereby increasing vocal output for the same vocal fold vibration and conserving average airflow
Voice Acoustics
https://med.umn.edu/ent/patient-care/lions-voice-clinic/about-the-voice/how-it-works/acoustics
Acoustic flow
Acoustic flow refers to pressure sound wave propagation, which travels at the speed of sound. Acoustic flow is what carries the sound signal to listeners.
Airflow
Steady flow refers to the airflow which passes through the glottis and vocal tract, dispersing and declining rapidly upon leaving the mouth. It is not the carrier of acoustic energy.
Belting
A chest-voice dominant vocal quality used in many styles of musical theatre and contemporary commercial singing
Belt Is Legit Article, Robert Edwin Journal of Singing
https://www.nats.org/_Library/Kennedy_JOS_Files_2013/JOS-064-2-2007-213.pdf
Passaggio
A commonly used classical voice pedagogy term for the acoustic and/or physiologic transitions between registers. Sometimes referred to as a voice register break.
Laryngeal registration: the muscular adjustment of the vocal folds.
Acoustic registration: the timbral transitions that occur from harmonic;resonance interactions. All acoustic register events involve harmonic interactions with the second resonance (vowel mod) - what happens above the larynx of the vocal tract. Second passagio is acoustic
Lower voices: only acoustic needed unless conscious laryngeal change
first shift around F3-C4
second shift Eb4-G4
Higher voices:
first shift is laryngeal based and from M1 to M2 Eb4-G4
second shift is resonance based Eb5-F#5
Range/tessitura
Voice Range and Tessitura Chart
Tessitura: the most comfortable and frequently used part of a voice range, as opposed to the full range of pitches it can produce
Range or Tessitura (?) according to link:
Soprano: C4-A5 / Tenor: B2-G4
Mezzo soprano: A3-F5 / Baritone: G2-E4
Alto: F3-D5 / Bass: E2-C4
Subglottal Pressure
A measure of the lung pressure below the glottis during a phonation.
Timbre
Aspects of sound other than pitch and loudness; primarily composed of the relative intensities of the frequencies in the sound spectrum.
Vowel Modification
As pitch ascends, its harmonic set rises, causing its changing frequencies to migrate through their inherent spectral tone color gradients; furthermore, as source harmonics move into and through vocal tract resonance peaks, their intensity rises and falls, changing their individual contribution to the overall, composite vowel percept. This is especially evident when harmonics rise into and through the first resonance (F1)
—
Singers modify vowels by adjusting the vocal tract to align vowel formants with the sung pitch or its harmonics, resulting in an "acoustical boost". The goals of this modification include "enhanced dynamic range and control", to allow for a wider range of loudness with potentially less effort
Definition:
Adjusting the shape of the vocal tract while singing to strategically align vowel formant frequencies with the sung pitch or its harmonics. This provides an acoustical boost to the sound
Involves shading vowels with respect to the location of vowel formants, rather than completely changing the vowel
Goals:
Achieve a unified vocal quality throughout the entire vocal range
Create smoother transitions between vocal registers
Enhance dynamic range and control
Improve intelligibility of the sung text
Achieve acoustic efficiency by shaping the vocal resonator for the most "gain" with the least energy
Key Concepts:
Formants are frequency bands in the vocal tract
The amount of modification needed is individual and varies
Males often modify vowels to match formants with harmonics above the fundamental [conversation history].
Females, especially in the upper register, often reinforce the fundamental frequency by matching it to lower formants (F1) [conversation history].
General "rules" for modifying formants by adjusting the vocal tract
Lowering the larynx or protruding the lips lowers all formant frequencies uniformly.
Lip rounding lowers formants, lip spreading raises them.
Fronting/arching the tongue lowers F1, raises F2.
Backing/lowering the tongue raises F1, lowers F2.
Opening the jaw raises F1, lowers F2.
Can involve shading vowels towards more open or closed versions
Some singers use spectrum analysis programs for feedback
Elite singers make subtle changes in vowels
What are some essential differences between amplified and unamplified singing?
What are some strategies a singer could employ to enhance their volume while singing? What muscles are involved in those strategies?
What are semi-occluded vocal tract exercises, and how do they assist singers with establishing greater efficiency of vocal production?
Why might an unamplified singer choose to employ active vowel modification?
How might certain types of consonants (e.g., plosives/stops, fricatives/affricates) be used to assist singers with establishing desirable vocal qualities and eliminating or minimizing undesirable one?
Describe the anatomy of the larynx, including the cartilages and the intrinsic muscles, and explain their primary functions in voice.
How do the vocal folds produce sound, and what is the role of airflow in this process?
What is the concept of "cover" in singing, and how does it relate to formant frequencies, particularly F1?
Explain the role of subglottal pressure in controlling loudness and pitch in singing. What challenges do singers face in coordinating subglottal pressure with musical demands?
What is the "tracheal pull," and how does the position of the diaphragm (related to lung volume) potentially influence the contraction of the cricothyroid muscles, which are major agents for pitch control?
How does the shape of a singer's vocal tract change the sound wave that comes out when they sing?