Wrist/Hand MSK Conditions & Deformities
1/13
Earn XP
Description and Tags
FF Week 3
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
14 Terms
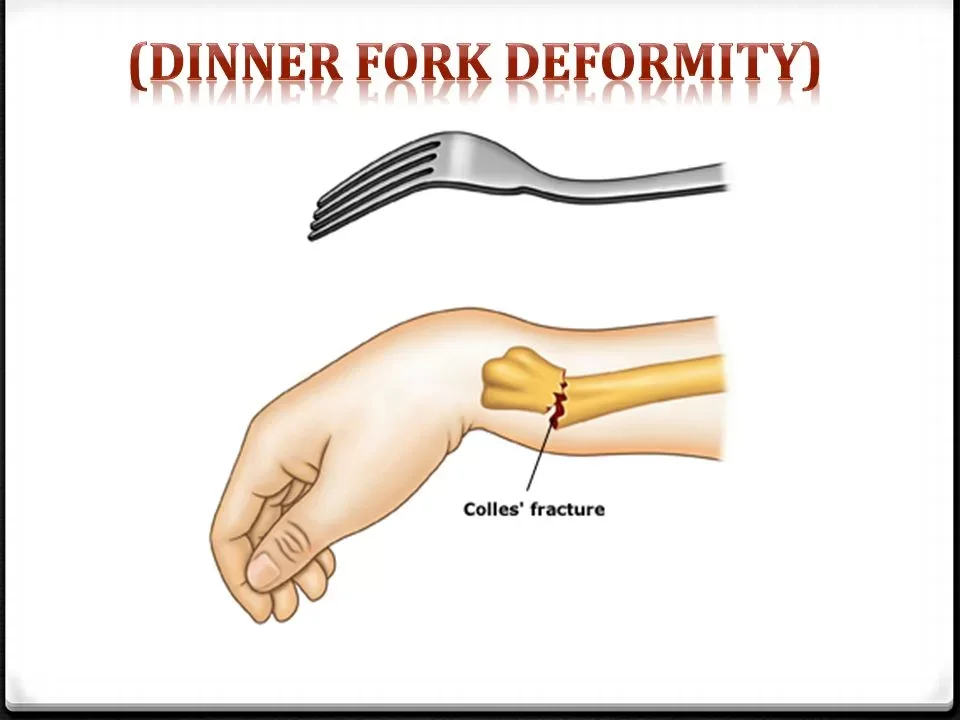
Colles Fracture
Characteristics:
Fracture of distal radius d/t FOOSH or blow to palmar side of wrist
Fragment displaced in dorsal and posterior direction
“Dinner fork” deformity
“Call me back for dinner”
Call = colles
Back = dorsal/posterior
Dinner = dinner fork
Presentations:
Wrist pain, swelling, and deformity
Limited ROM
Tenderness over distal radius
Complications:
Complex regional pain syndrome
Decreased grip strength
Loss of ROM
Extensor pollicis longus tendon tear
Smith’s Fracture
Characteristics:
Fracture of distal radius d/t fall on the back of flexed hand or blow to dorsal side of wrist
Fragment displaced in the palmar and anterior direction
“Garden spade” deformity
“Mrs. Smith loves to garden in her front yard”
Mrs. Smith = Smith’s fracture
Garden = “garden spade” deformity
Front = volar/palmar/anterior
Presentations:
Wrist pain, swelling, and deformity
Limited ROM
Tenderness over distal radius
Complications:
Complex regional pain syndrome
Malunion

Rheumatoid Arthritis (RA)
Characteristics:
Systemic autoimmune disease causing chronic inflammation of synovial lining and connective tissue
Common in small joints of hands, feet, wrists, and ankles
Presentations:
Age: 30-60 years of age
Females > males
Symmetrical involvement
Pain and tenderness
Morning stiffness
Warm joints
Swan neck and boutonniere deformities
Trigger finger
Rheumatoid factor blood test and X-ray used for diagnosis
Treatments:
Reduce inflammation and pain
Promote joint function
DMARDs (disease-modifying antirheumatic drugs)
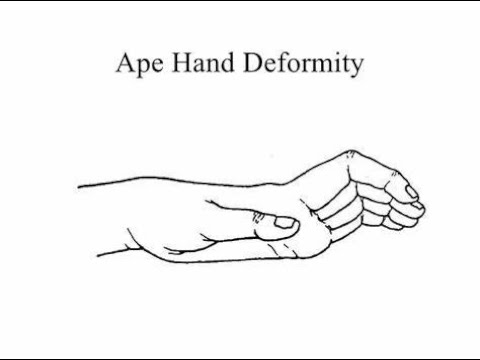
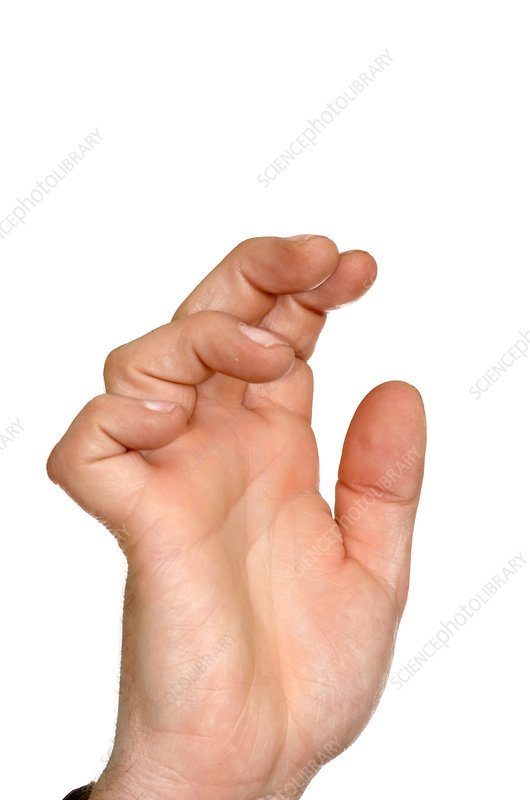
Ape Hand deformity
-Wasting of thenar eminence d/t median nerve palsy
-Thumb falls back in line with fingers d/t pull of extensor muscles
-Pt unable to flex or oppose thumb
Bishop’s Hand/Benediction/Claw Hand
-Wasting of hypothenar eminence, interossei muscles, and 2 medial lumbricals muscles d/t ulnar nerve palsy
-Hyperextension of MCP joint and flexion of PIP/DIP joints for 4th and 5th digits

Claw fingers
-Loss of intrinsic muscle action and the over-activation of the extrinsic extensor muscles on the proximal phalanx of the fingers
-MCP joints are hyperextended and PIP/DIP joints are flexed
-Caused by combination of median and ulnar nerve palsy
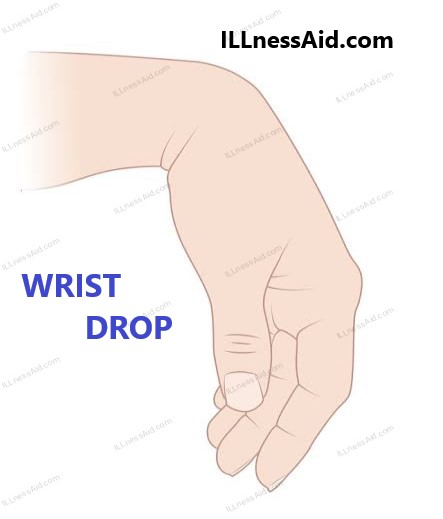
Drop-Wrist deformity
-Radial nerve palsy
-Wrist extensors can’t oppose wrist flexion
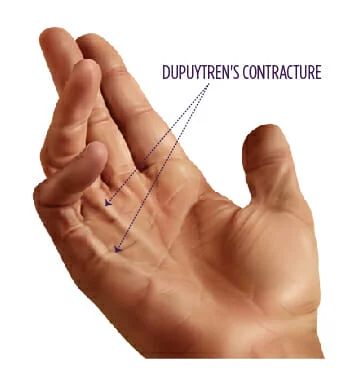
Dupuytren’s Contracture
-Contraction of palmar fascia, fixed flexion of MCP and PIP joints of 4th &/or 5th digits
-Males > females
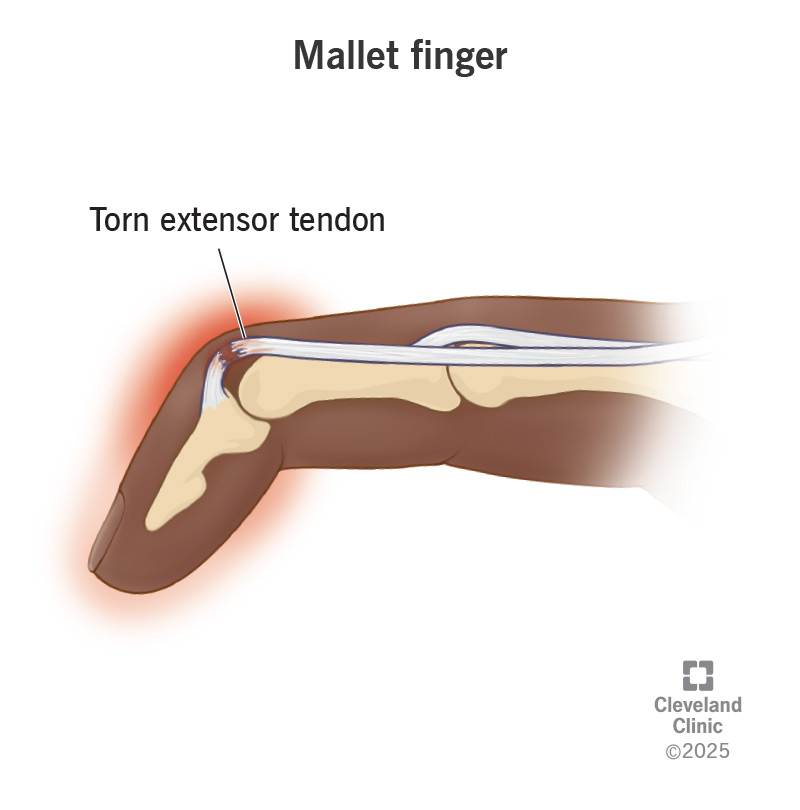
Mallet Finger
-Due to rupture or avulsion of the extensor tendon at distal phalanx of finger
-Distal phalanx rests in flexion
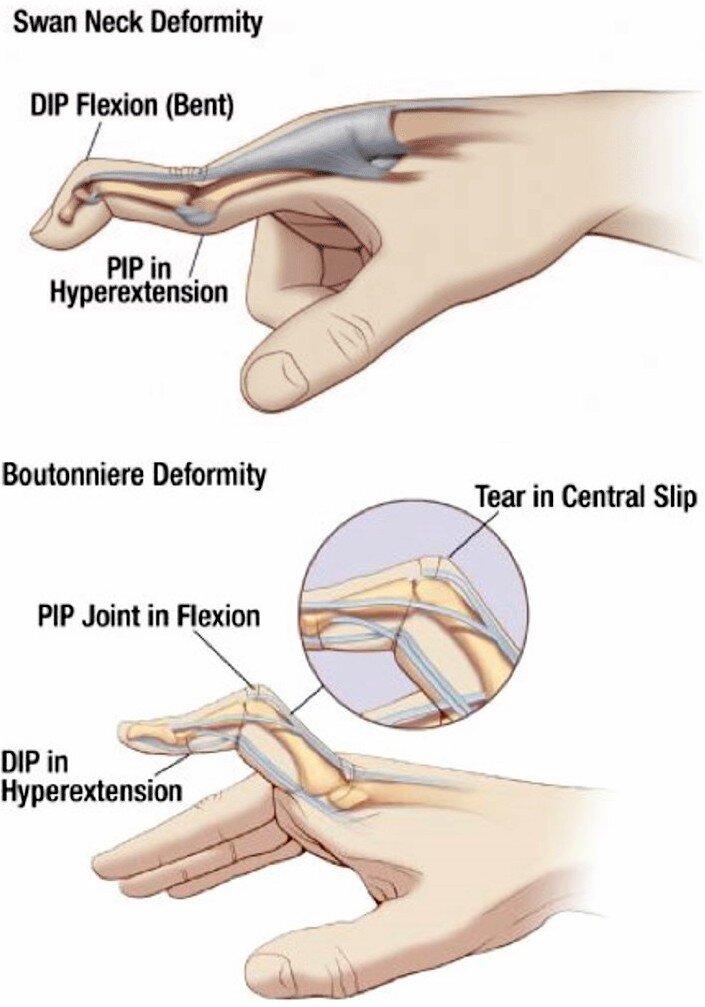
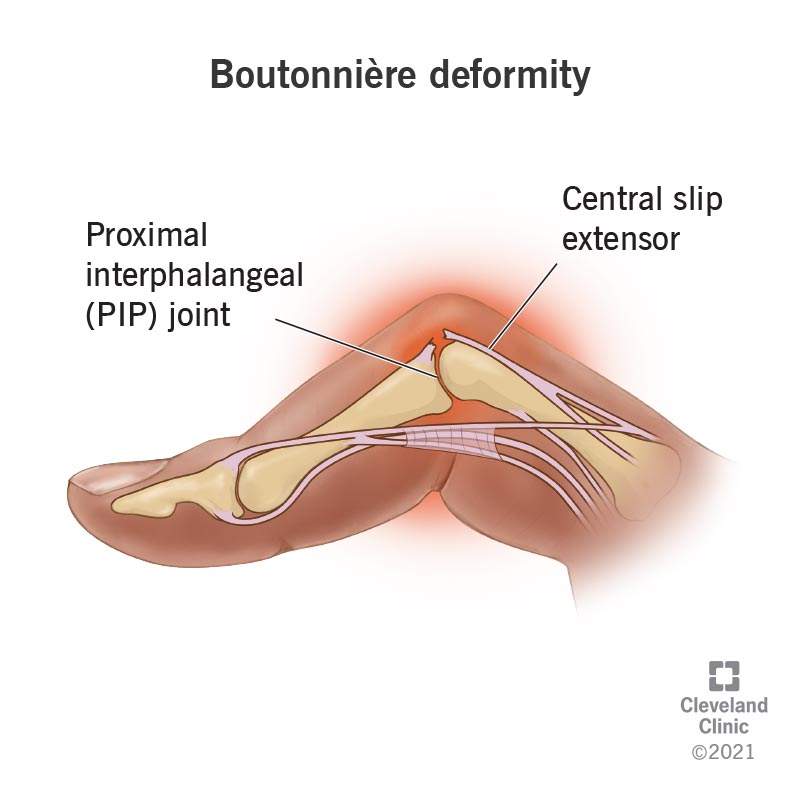
Boutonniere deformity
-Extension of MCP and DIP joints and flexion of PIP joint
-Result of rupture of the central tendinous slip of the extensor hood
-Most commonly d/t trauma or RA
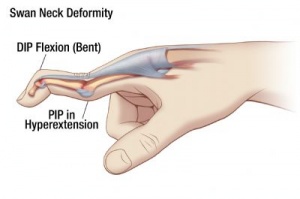
Swan Neck deformity
-Extension of PIP joint and flexion of MCP and DIP joints
-Result of contracture of intrinsic muscle or tearing of volar plate
-Common in RA
Trigger Finger (Tenovaginitis Stenosans)
-Result of a thickening of the flexor tendon sheath (Notta’s nodule) which causes sticking of the tendon when the patient attempts to flex the finger
-Low grade inflammation of the proximal fold of flexor tendon leads to swelling and constriction in digital flexor tendon. When patient attempts to flex finger, the tendon sticks, and the finger “lets go”, often with an audible “snap”
-As condition worsens, eventually finger will flex and not “let go”
-Usually occurs in 3rd or 4th finger
-Usually associated with RA and tends to be worse in morning
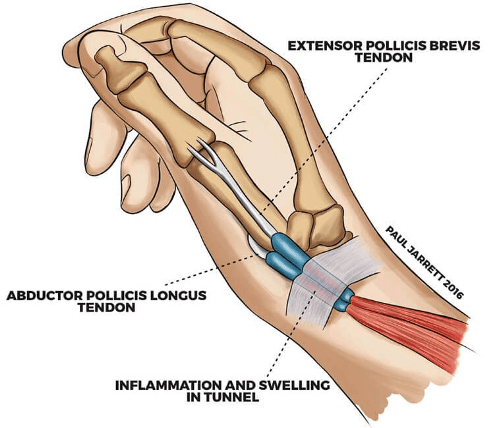
De Quervain’s Tenosynovitis
-Inflammation of extensor pollicis brevis (EPB) and abductor pollicis longus (APL) tendons at 1st dorsal compartment
-Pain at anatomical snuffbox, swelling, decreased grip/pinch strength
-Positive Finkelstein’s test
-Common in pregnancy
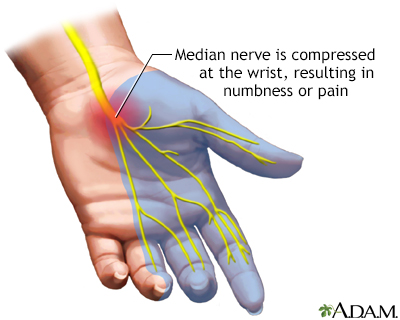
Carpal Tunnel Syndrome
-Compression of median nerve
-Burning, tingling, pins & needles, numbness at night
-Positive Tinel’s sign
-Common in pregnancy, DM, and RA