Cardiology
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
Define Hypertension
Defined as an elevated blood pressure with systolic BP of 140mmHg or more and/or a diastolic BP of 90mmHg or more in 2 readings 4-6 hours apart, or any reading in a patient on antihypertensive medication
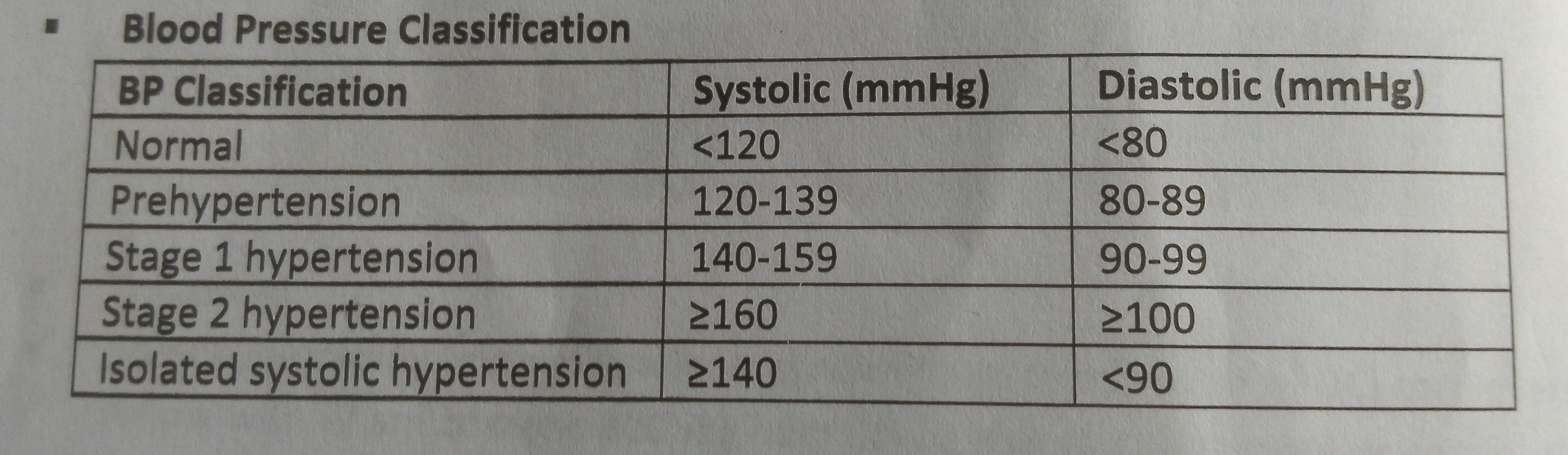
Classify Hypertension with values
Types of Hypertension
Primary Hypertension
Secondary Hypertension
Risk factors for hypertension
Age: risk rises with age
Sex: Higher in males because estrogen protects against high BP. Post menopausal women this have high risk
Race: blacks
Obesity: BMI > 30
Sedentary lifestyle
Smoking
Excessive alcohol
Environment: Urban > rural due to lifestyle
Obstructive sleep apnea
Genetics: higher concordance in monozygotic than dizygotic twins
Microalbuminuria
LBW
Causes of secondary Hypertension
Renal: Chronic glomerulonephritis, ADPKD, ARPKD, acute glomerulonephritis, obstructive uropathy, renal artery stenosis, renal vein thrombosis, renin producing tumors
Endocrine: Cushing syndrome, Conn syndrome, Hyperthyroidism, Pheochromocytoma, acromegaly, hyperparathyroidism, congenital adrenal hyperplasia
CVS: Coarctation of aorta
Drugs: NSAIDs, OCPs, Steroids, Cocaine, MAO inhibitors, TCAs, Cyclosporine
Neurogenic: Obstructive sleep apnea, Raised ICP,
Others: Pregnancy, (pre) eclampsia.
Symptoms of Hypertension
Asymptomatic
Vague symptoms: Headache, insomnia, palpitations
Symptoms of underlying pathology
Symptoms of target organ damage
Hypertension target organs and damage on each
Brain
Hypertensive encephalopathy
Stroke (ischemic & hemorrhagic)
Amyloid angiopathy
Dementia
Lacunar infarcts
Heart
LVH
CHF
IHD
Arrhythmias
Aortic dissection
Sudden death
Kidneys
Focal segmental glomerulosclerosis
AKI
CKD
Eyes
Hypertensive retinopathy
Peripheral arteries
Atherosclerotic disease
Ears
Tinitus
Grade hypertensive retinopathy
Grade 1-4
Grade 1: tortuosity of retinal arteries with thick shiny walls (silver/copper wiring)
Grade 2: 1 + arteriovenous nipping ( narrowing where arteries and veins cross)
Grade 3: 2 + flame-shaped hemorrhages and cotton wool spots
Grade 4: Papilledema (swelling of the optic disc)
Examination findings in hypertension
Hypertension Investigations
CXR
ECG
Echo
E/U/Cr & Ca & Albumin
Urinalysis
Renal USS
FBS
FLP
Thyroid function test
Urinary metanepheines or catecholamines
Treatment of Hypertension
Lifestyle modifications: SAWAD
stop Smoking
reduce Alcohol
Weight reduction
increased physical Activity
Diet:
Salt reduction Nacl < 6g/day, Na < 3g/day
DASH Diet:
High in K, Low in Ca, Low saturated fats, high unsaturated fats.
Diet rich in fruits, vegetables, and low fat diary peoducts
Pharmacological Therapy: A³BCD-R
ACE Inhibitors e.g lisonpril, ramipril
ARBs e.g losartan, valsartan, candesartan
Beta blockers e.g atenolol, metoprolol, carvedilol
Calcium channel blockers e.g amlodipine, nifedipine
Diuretics
Thiazides e.g HCT
Aldosterone antagonist e.g sporinolactone
Renin inhibitors e.g Aliskiren
Alpha antagonist e g prazosin, Doxazosin
Define the following:
Hypertensive urgency
Hypertensive emergency
Malignant Hypertension
Accelerated hypertension
Hypertensive urgency: severely elevated BP (>180/110 mmHg) with no evidence of target organ damage
Hypertensive emergency: severely elevated BP (>180/110 mmHg) with evidence of target organ damage
Accelerated and Malignant Hypertension are also hypertensive emergencies with similar outcomes and therapies
Accelerated hypertension: sudden elevation of BP associated with fundoscopic vascular changes but without papilledema
Malignant Hypertension: sudden elevation of BP which can present with grade 3/4 retinopathy or hematuria and/or proteinuria
Treatment of Hypertensive urgency and hypertensive emergency
Hypertensive urgency:
there is room for oral antihypertensives
Aim to reduce MAP by 25% in 24 hours
Hypertensive emergency:
IV antihypertensives is used
Aim to reduce MAP by 25% in 1 hour
Define Heart Failure
Heart Failure is a clinical syndrome consisting of symptoms (fatigue leg swelling difficulty in breathing) and/or signs (rales, pedal edema) resulting from structural or functional abnormalities of the heart leading to inability of the heart to pump blood to meet the metabolic needs of the body or when the heart is able to do this at elevated intracardiac pressure.
Types of heart failure
Right
Left
Congestive
Systolic
Diastolic
HFpEF
HFmrEF
HFrEF
Acute
Chronic
High output
Low output
Classifications of Heart failure:
NYHA
AHA & ACC
Araoye
NYHA: CLASS I- IV
Class I: Symptoms with more than ordinary activity
Class II: Symptoms with ordinary activities
Class III: Symptoms with less than ordinary activity
Class IV: Symptoms at rest
Symptoms: Dyspnoea, fatigue, palpitations
ACC & AHA: STAGE A-D
Stage A: normal cardiac structure & functions in presence of risk factors
Stage B: Subclinical changes in Left ventricular structure and/or function
Stage C: Clinical heart failure
Stage D: Advanced heart failure
Araoye: Grade 1-3
Grade 1: Heart failure + high BP
Grade 2: Heart failure+ long term peripheral stigmata of Hypertension + Low BP which rises on treatment
Grade 3: Grade 2 + BP remains low/normal on treatment
Clinical diagnosis of Heart failure
FRAMINGHAM’S CRITERIA
MAJOR CRITERIA: PICS RANCH
PND or orthopnea
Increased venous pressure > 6 cmH2O
Cardiomegaly
Rales
Acute pulmonary edema
Neck vein distention
Circulatory time > 25 sec
Hepatojugular reflex
MINOR CRITERIA:
Night cough, ankle swelling, DOE, hepatomegaly
Pleural effusion, tachycardia (>120)
Vital capacity decreased 50% from maximal capacity
Weight loss > 4.5kg in 5 days in response to treatment
2 MAJOR
1 MAJOR + 2 MINOR
Causes of heart failure
Hypertensive heart disease
Dilated cardiomyopathy
Valvular heart disease
IHDs
Congenital heart diseases
CADs
Pericarditis
Myocarditis
Infective Endocarditis
Arrhythmias
Other Cardiomyopathies
Cor pulmonale
End myocardial fibrosis
Alcohol
Drugs
Hyperdynamic circulation
Anemia
Thyrotoxicosis
Pager disease
Risk factors for heart failure
Major
Age
Males
Hypertension
DM
Obesity
LVH on ECG
MI
Minor
Alcohol
Smoking
Dyslipidemia
Renal insufficiency
Sedentary lifestyle
Low SE status
Salt
Coffee
Impaired pulmonary function
Sleep disordered breathing
Tachycardia
Mental stress/depression
Heart Failure precipitants
HEART FAILED
Hypertension - accelerated/malignant
Endocarditis, unaccustomed Exercise
Anemia, Alcohol
Renal impairment, RHD
Thyrotoxicosis
Failure to take meds
Arrhythmias
Infections, infarction, ischemia
Lung problems ( Pulmonary embolism, pneumonia, COPD), Lifestyle
Endocrine- Pheochromocytoma, hyperaldosteronism
Dietary indiscretions
Others: pregnancy
Most common:
Chest infections
Arrhythmias
Thyrotoxicosis
NSAIDs
Steroids
Anemia
Pregnancy
Unaccustomed Exercise
Indiscriminate drug use
Pathophysiology of heart failure
Myocardial injury (e.g., ischemia, pressure overload, volume overload)
Reduced cardiac contractility (systolic dysfunction)
Impaired ventricular relaxation (diastolic dysfunction)
DECREASED cardiac output
Activation of sympathetic nervous system
INCREASED heart rate and peripheral vasoconstriction
Activation of renin–angiotensin–aldosterone system (RAAS)
INCREASED sodium and water retention
INCREASED preload
INCREASED afterload
Ventricular remodeling (hypertrophy and dilation)
INCREASED wall stress → release of ANP, BNP and C-type peptide
Neurohormonal activation (e.g., ADH release)
Fluid accumulation → pulmonary congestion and peripheral edema
DECREASED tissue perfusion
Progressive worsening of cardiac function
Symptoms of heart failure
Signs of heart failure
LHF SYMPTOMS
DOE
Orthopnea
PND
Cough productive of pink frothy sputum
Tachycardia
SIGNS
Basilar rales
Pulmonary edema
S3 Gallop
Pleural effusion
Cheyne-stokes respiration
RHF SYMPTOMS
Abdominal pain
Anorexia - due to gastric edema
Nausea
Bloating
Leg/body swelling
SIGNS
Peripheral edema
Jugular venous distention
Tender hepatomegaly
Other signs and symptoms depending on etiology
Investigations done in heart failure
Chest X-ray: ABCDE
Echocardiography
ECG
Cardiac biomarkers assay
FBC
E/U/Cr
LFT
TFT
C-reactive protein
Non pharmacological management of heart failure
Bed rest
Cardiac position
Low salt diet (Na <2.4g/day)
Weight reduction
Stop alcohol
Stop smoking
Stress reduction
Avoid constipation
Principles of Management of heart failure
Resuscitate
Reduce preload- furosemide
Reduce afterload- ACE Inhibitors, ARBs
Increase contractility of heart- digoxin
Reduce morbidity or mortality
Identify & treat etiology
Identify & treat precipitants
Treat complications
Goals of Management of heart failure
Complications of heart failure
Cardiogenic shock
Arrhythmias
Stroke
DVT
Pulmonary embolism
Intracardiac clots
Cardiac cirrhosis
Electrolyte derangements
AKI
CKD
Congestive hepatopathy
Weight loss - cardiac cachexia
Death
Causes of weight loss in heart failure
Early satiety
Anorexia
Vomiting
Cardiac cachexia
Hypoxia- cellular death
Poor Prognostic factors for heart failure
Clinical
Age
Men
Blacks
NYHA 4
Regular hospitalization
Cardiac cachexia
Syncope
S3
Arrhythmias
Biochemical
Hypokalemia
Hyponatremia
Hypernatremia
BNP >400 nanograms
proBNP > 1200 nanograms
Elevated creatinine
Elevated urea
Low GFR
Imaging
Reduced LVEF
Positive X ray features
RV dysfunction on echo
Pulmonary Hypertension
Functional
Frailty
6 minute walk distance - worse if patient CAN tolerate this
Low peak VO2 (<14ml/kg/min)
Contraindications to cardiac transplantation
Active infection
Active malignancy
Poor adherence to medical therapy
Active substance abuse (alcohol, drugs)
Severe irreversible pulmonary hypertension
Advanced irreversible renal failure
Advanced irreversible liver disease
Severe chronic lung disease
Uncontrolled diabetes mellitus with end-organ damage
Significant peripheral vascular disease
Severe psychiatric illness
Systemic disease with poor prognosis
HIV with uncontrolled disease
Morbid obesity
Advanced age (relative)
Causes of mitral stenosis
Rheumatic fever
Degenerative valvular disease
Chemotherapy
Radiotherapy e.g breast Ca
SLE
Rheumatoid arthritis
Malignant carcinoid disease
Cor triatriatun
Left atrial myxoma
Congenital
Degenerative valvular disease
Chemotherapy
Radiotherapy
Connective tissue disease
Congenital heart diseases
Normal area of mitral valve orifice
4-6 cm²
Pathophysiology of mitral stenosis
Mitral valve narrowing →obstructed LV filling (LVH) → ELEVATED LA pressure & enlargement →pulmonary venous congestion →pulmonary Hypertension →right ventricular enlargement →right heart failure →tricuspid & pulmonary regurgitation
Symptoms of mitral stenosis
Dyspnoea
Cough- PH
Hemoptysis - PH
Easy fatiguability
Chest pain
Palpitations ( left atrial enlargement → arrhythmias AF)
Systemic emboli
Hoarseness ( enlarged LA compression on recurrent laryngeal nerve)
Dysphagia ( enlarged LA compression on esophagus)
Signs of mitral stenosis
Inspection & palpation:
Malar flush
Small volume pulse
Raised JVP
Tapping apex beat
Auscultation
Loud S1
Loud P2
Opening Snap
Mid diastolic murmur
Graham Steell murmur ( an end diastolic murmur due to pulmonary regurgitation)
Mitral stenosis investigations
Echo: Diagnostic shows fusion of mitral valve commisures. Also shows diastolic and systolic dysfunction
ECG: P-mitrale/bifid p wave (LA enlargement), right axis deviation (RVH), Atrial fibrillation
CXR: Mitralization, double heart shadow, ABCDE of HF
Angiography
MRI
FBC
E/U/Cr
Mitral stenosis treatment
Recurrent rheumatic fever prophylaxis: Oral penicillin
Treat atrial fibrillation: beta blockers, verapamil etc
Low salt diet
Heart failure: Low dose diuretics
Surgery:
Open surgery mitral Valvulotomy
PMBV
Commisurotomy
Mitral Valve replacement
Metallic- for life, need anticoagulants use for life
Bioprosthetic- 10 years
Mitral regurgitation causes and types
Acute MR:
IHD, Infective endocarditis, rupture of chordae tendinae
Chronic MR:
RHD, MV prolapse, calcification of MV annulus
Degenerative valvular disease
Chemotherapy
Radiotherapy
Connective tissue disease
Congenital heart diseases
Mitral regurgitation pathophysiology
Acute MR: No time for LA dilation, so large regurgitant volume is delivered into a LA with normal compliance leading to markedly increased pulmonary pressure and pulmonary edema
Chronic MR: There's sufficient time for LA dilation and accommodates regurgitant volume, so LA pressure is normal/slightly elevated however chronic atrial dilation leads to Atrial fibrillation.
Mitral regurgitation symptoms
Dyspnoea
Fatigue
Symptoms of HF
Symptoms of atrial fibrillation
Mitral regurgitation signs
Soft S1
Wide splitting of S2
Prominent S3
Loud P2
Laterally displaced apex beat with systolic thrill
Grade 3/4 pansystolic murmur radiating to axilla
Mitral regurgitation investigations
Echo
ECG
CXR
Angiography
MRI
FBC
E/U/Cr
Barlow syndrome
Barlow’s syndrome:
Associated conditions
Symptoms
Signs
Complications
Treatment
Aortic stenosis etiology
Aortic stenosis pathophysiology
Aortic stenosis symptoms
Aortic stenosis signs
Aortic stenosis investigations
Aortic stenosis treatment
Aortic regurgitation types and etiology
Aortic regurgitation symptoms
Aortic regurgitation signs
Aortic regurgitation investigations
Aortic regurgitation treatment
Define infective Endocarditis
Risk factors for infective Endocarditis
Etiology (organisms) of infective Endocarditis
Most common organism causing infective Endocarditis in:
Native valve Endocarditis
Prosthetic valve Endocarditis
IV drug associated endocarditis
Signs and symptoms of infective Endocarditis - systematically
Describe the pathology of infective Endocarditis
Diagnostic criteria for infective endocarditis
Investigations done in infective endocarditis
Treatment of infective endocarditis
Indications for surgery in infective endocarditis
Complications of infective endocarditis