EENT
1/55
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
56 Terms
Visual acuity (using any corrected methods)
What must be documented in an eye exam in the ED?
pupillary reaction, EOMs, visual fields, fundoscopic examination (red light reflex, anterior chamber depth, optic disc, retinal circulation, macula), lid eversion, fluorescein staining, Intra-occular pressure testing (pain or redness)
Parts of the eye exam in the ED?
Indirect and direct accommodation (check for a pupil that doesn’t constrict indirectly - Marcus Gunn (afferent defect))
What are we looking for in pupillary reaction
motor nerve deficit (loss of direct in the bad eye, normal eye good)
An efferent pupillary defect is a
Sensory nerve deficit (light in bad eye, NO CONSTRICTION indirect or direct)
An afferent pupillary defect is a
Black silhouettes (could be bleeding…)
What are some red flags in a red light reflex?
10-21 mmHG
What is normal IOP?
1:2
Normal cup to disk ratio - check anybody with a HA
Viral (most common), bacterial, allergic
Etiologies of conjunctivitis
Antihistamines, lubricants, Abx (PRN - like purulent discharge in 1 eye), NO CONTACTS
Treatment plan for conjunctivitis
Antivirals, ophtho consult, NO CONTACTS
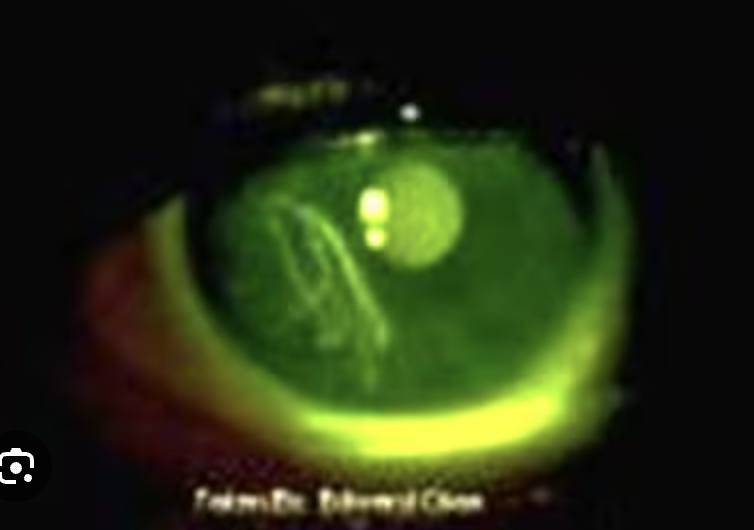
64 y/o patient presents to the ED for face pain that radiates to her eye. On physical exam you note a red rash following the trigeminal nerve zones. Fluorescein stain shows a corneal dendrite. What is your treatment plan?
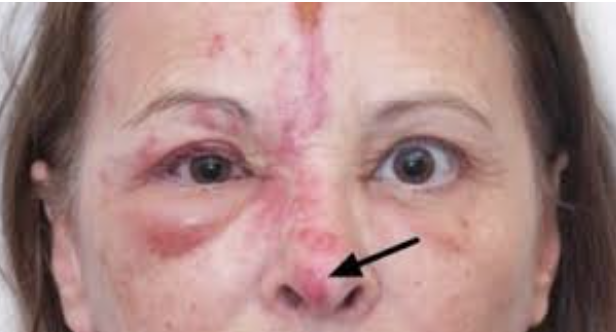
Eyeball VANC (compounded drops) every hour, NO CONTACTS
43 y/o female presents to the ED for eye pain - she says, “I think something is stuck up in there.” She wears contacts. Fluorescein stain reveals a ROUND spot that picks up the dye. What is your treatment plan?
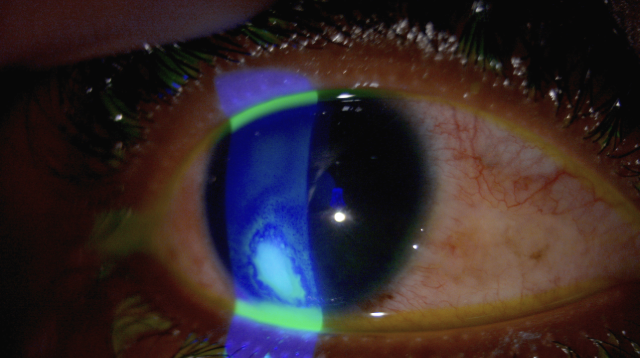
Mydriatic drops (dilating), emotional upset, sympathomimetic and anti-cholinergic drugs
Acute angle glaucoma can be precipitated by
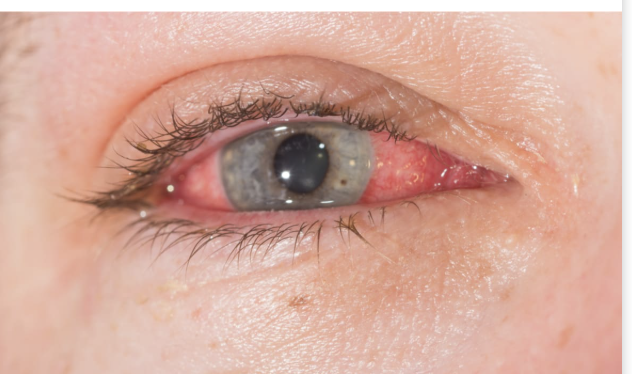
Call ophtho, timolol/pilocarpine drops, Acetazolamide/osmotic diuretics
43 y/o male presents to the ED for a HA that is exacerbated by light after “I did a whole lot of coke.” He reports that he sees “rainbow angels around the lights.” On physical exam you note decreased visual acuity of the right eye with an injected conjunctiva, a steamy cornea, and a fixed mid-dilated pupil. IOP is measured in at over 30. What do you want to do?
Consensual photophobia
What are you going to see on physical exam for iritis and uveitis?
Lubricating drops and Ophtho consult, ocular NSAIDs after the consult
What is your game plan for episcleritis?
Oral NSAIDs and ophtho follow up
23 y/o male presents to the ED for eye pain. On physical exam, you note NORMAL visual acuity, pain with EOM, and a SUPER RED EYE!! What is your treatment plan?
Rebreathe CO2, gentle eyeball massage, IOP lowering drugs (timolol, acetazolamide), Optho consult
46 y/o female presents to the ED for sudden left eye vision loss that started 30 minutes ago. She reports no pain. On physical exam you note a cherry red spot. What do you want to do?
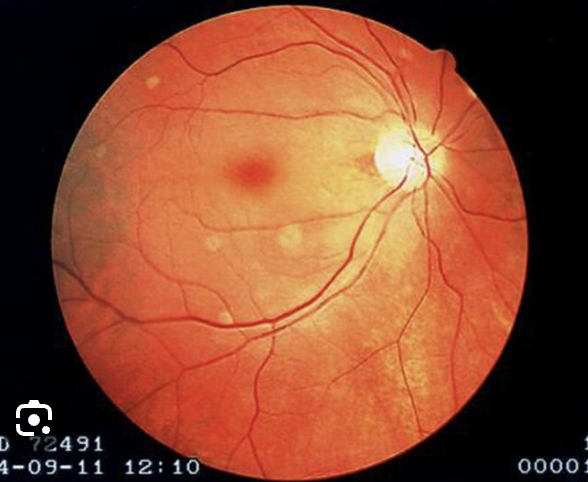
Call the eyeball guys
37 y/o female presents to the ED for left eye vision loss that has occured over a couple minutes. On physical exam you note diffuse blood and thunder on the retina, What is your gameplan

Call the eyeball guys
56 y/o male presents to the ED for right vision loss, that came on “like someone was pulling the wool over my eye literally.” On physical exam you note some black things floating around on the red light reflex and the retina blowing in the wind on fundoscopic exam. What do you want to do
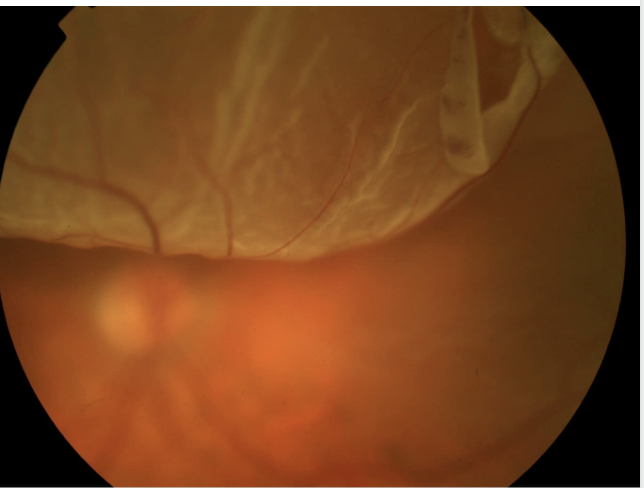
CT orbits/sinuses, LOOK AT THE EYBALL, PO abx, close follow up
32 y/o woman presents to the ED for face pain. Vitals are stable with the exception of 123 bpm and 101.2 temp. On physical exam you note PRONOUNCED periorbital edema, but no vision changes or pains on EOM. What is your gameplan?
CT orbits/sinuses, CBC, culture (blood and eye goo), lumbar puncture (maybe), LOOK AT THE EYEBALL, IV abx, ophtho consult
32 y/o woman presents to the ED for face pain. Vitals are stable with the exception of 123 bpm and 101.2 temp. On physical exam you note a swollen right eyelid with proptosis, PAINFUL EOM, and double vision. What is your gameplan?
Abx drops, NO CONTACTS
17 y/o female presents to the ED for eye pain possibly due to a foreign body. She said it happened RIGHT after she took her makeup off. On physical you note linear uptake with fluorescein. What’s your gameplan?
CT orbits, Cover both eyes, Start Abx, get’em to the eye guys
45 y/o male presents to the ED for getting a wire stuck in his eye. On physical exam you note a small wire that penetrates the right globe, decreased visual acuity and Seidel sign with fluorescein stain. What is your gameplan?
Ophtho consult, abx (augmentin 🙄)
58 y/o male presents to ED post-bicycle crash. On physical exam you note bruising under the right eye, and an inability to move the eye upwards. What is your gameplan?
Malignant Otitis Externa
A complication of otitis externa that usually occurs despite 2-3 weeks of topical antimicrobial therapy
Confirm by CT/MRI, IV abx
Gameplan for Malignant Otitis Externa
CT/MRI, IV abx, myringotomy, tympanocentesis
78 y/o male presents to the ED for ear pain, he states that he is currently on antibiotics for an ear infection but he hasn’t been taking them. On physical exam you note postauricular erythema with tenderness and swelling - the auricle is protruding and there is no postauricular crease. What is your gameplan?

Anesthetize, I and D, pack all the grooves, wrap the head civil war wound style
Okay so if Connor Mcgregor comes in to the ER for an auricular hematoma - what are we doing?
Pour in some lidocaine, remove with forceps/flush it out, look at the canal and TM, Abx drops
Gameplan for an insect in the ear
Afrin (oxymetazoline), Lido w/ epi covered packing, chemical cautery w/ silver nitrate, Rhino Rocket (must be left in place)
Gameplan for Anterior Epistaxis
Rhino rockets/foley catheters to apply posterior pressures
Gameplan for Posterior Epistaxis - difficult to control
Refer to ENT w/in 6-10 days (Emergent if severe), PO abx (Pro tip from Paquette)
Gameplan for nasal fractures
Nasal septal hematoma
What must be r/o in all facial and nasal trauma?
incise/drain, Abx, ENT f/u
Gameplan for Nasal septal hematoma
Attempt to remove (forceps, mouth-mouth negative pressure from parents, foley cath trick), Abx if it was something organic
Gameplan for Nasal Foreign body
Purulent nasal secretions, severe symptoms for 7+ days, Double-worsening, unilateral pain
What are the rules for prescribing abx for sinusitis?
Abx resistance, very severe infection
When should a CT w/ Contrast be ordered for sinusitis?
Meningitis, sinus cavernosum infection,
Complications of bacterial sinusitis
X-ray/CT to identify, regional anesthesia, incise and drain, Pen VK or amoxicillin, dental followu-p
Gameplan for Dental Abscesses
Dental Abscesses
What is characterized by dental pain followed by local swelling that spreads to the facial planes?
Ludwig Angina
What is characterized by an oral infection that spreads into bilateral submandibular spaces that crosses midline and is swollen, red, and indurated?
AIRWAY!, IV abx, CT face and neck w/contrast, emergent surgical punt
Gameplan for Ludwig Angina
Enamel-Dentin Fracture
What is characterized by tooth sensitivity to hot/cold stimuli as well as air passing over the exposed surface during breathing
Seal in the ED, Abx (open fracture), punt to the dentist
Gameplan for Enamel-Dentin Fracture
Stabilize (front and back splint), dental follow up w/in 24-48 hours, abx
Gameplan for Crown-root fractures
Splint in place, f/u with dental, Abx
Gameplan for tooth luxation injuries
Rinse tooth for 10 sec with sterile saline and tap water, replace tooth, splint in place, abx
Gameplan for tooth avulsion (girl bye) injuries
Drainage - Prep suction, inject local anesthesia, needle aspiration in the lateral tonsil, IV steroid (1 dose), Abx (10 days)
16 y/o male presents to the ED for a severe sore throat and he can’t really talk. On physical exam you note a contralateral deflection of the swollen uvula and inferior/medial displacement of the right tonsil. What is your treatment plan?
5-10 days post-op
The most significant post-tonsillectomy hemorrhage occurs
ENT consult immediately, Apply direct pressure with a bleeding tonsillar bed with a pack or 4×4 gauze
Gameplan for post-tonsillectomy hemorrhage
PMHX of depression, previous SI, or attempt, missing time in parents Hx, reports of accidental ingestion, reports of intentional ingestion
Risk factors for TI
Odynophagia, dysphagia, N/V, Abd tenderness/tenderness, hematemesis, coffee-ground emesis, hematochezia, melena, wheezing, cough, SOB, stridor, respiratory distress/arrest, AMS
Signs and symptoms for ingestion-related esophagitis - depends on the amount of damage
CXR for respiratory problems, Acute abdominal xrays (r/o perf, possible battery ingestion), upper endoscopy
Diagnostics for ingestion-related esophagitis
Emergent airway stabilization PRN, remove the battery ASAP, NEVER induce vomiting or use neutralizing agents
Treatment plan for ingestion-related esophagitis
Increase the risk of the formation of esophageal strictures and esophageal cancer
Prognosis for ingestion-related esophagitis