Dyslipidemia-come back to memorize intensity
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
Distinguish between primary and secondary prevention of CVD
Primary: no history of ASCVD → preventing future events
Increased risk of a primary cardiovascular event
Secondary: established clinical ASCVD → already had an event + trying to prevent future events
Goal is to prevent a secondary cardiovascular event
* Clinical ASCVD = ACS, history of MI, stable or unstable angina, coronary or other revascularization, stroke, TIA, PAD
Identify modifiable and non-modifiable CV risk factors
Modifiable:
HTN (BP > 140/90)
“Dyslipidemia”
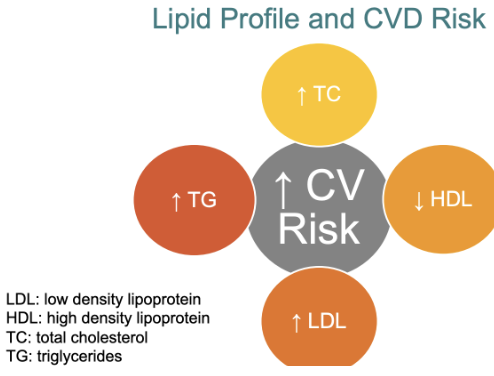
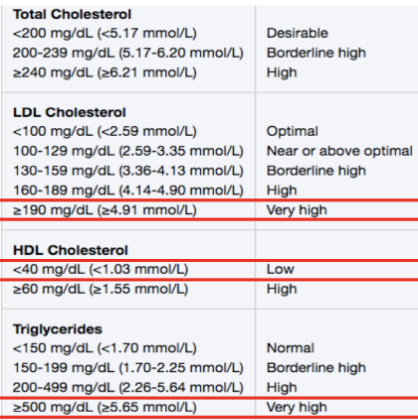
High TC, TG, or LDL
Only 15% is related to diet
Drug therapy not routinely indicated until Triglycerides (TG) > 500-1000 mg/dL
Also common in diabetes, so not often treated in these patients
Low HDL (< 40 mg/dL)
Exercise and diet is the best ways to increase HDL → no primary drug therapy
obesity/ inactivity
Diabetes
Metabolic syndrome
Smoking
Non-modifiable:
Age
Males > 45 yr
Females > 55 yr
Family hx/o CVD
Male first-degree relative < 55 yr
Female first degree relative < 65 yr
Other CV Risk factors - not LO
Carotid intima media thickness
Coronary calcium score
Apolipoprotein B (ApoB)
Lipoprotein A - Lp(a)
hsCRP
Lipid Profile and CVD Risk
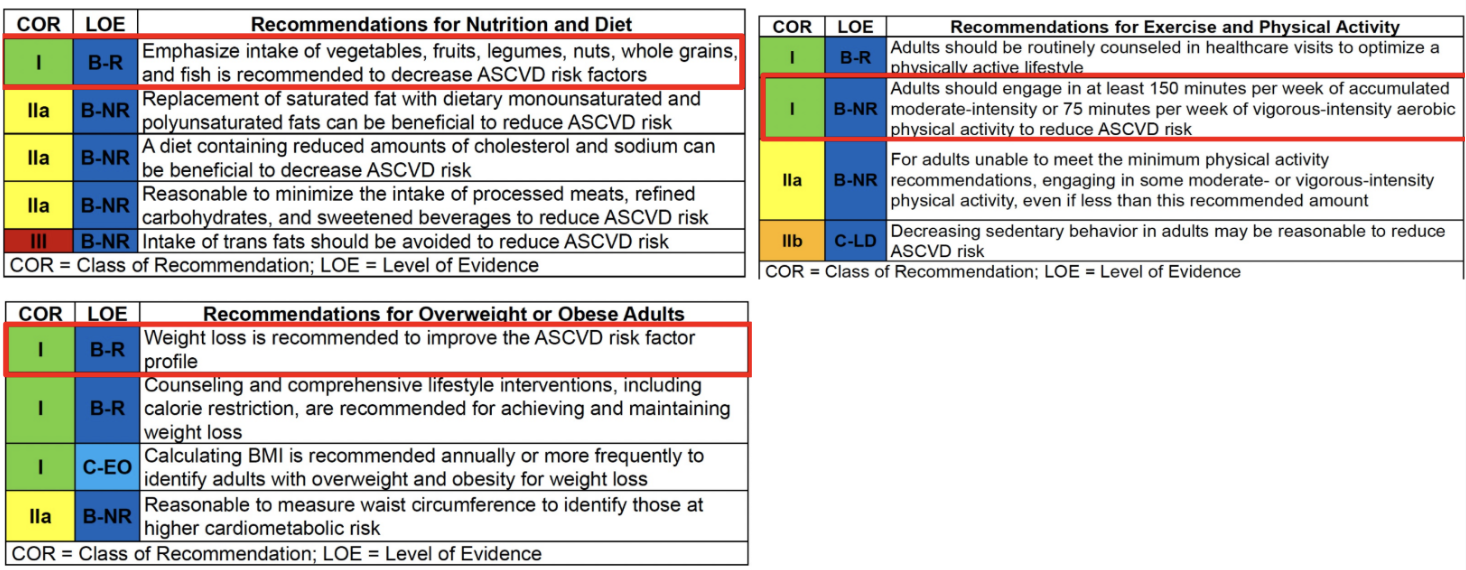
Recall key lifestyle (diet & physical activity) recommendations to reduce CV risk
Important to intake vegetables, fruits, legumes, nuts, whole grains, and fish is recommended to decrease ASCVD risk factors
Exercise for at least 150 minutes per week (moderate intensity) or 75 minutes per week( vigorous-intensity)
Weight loss
Alcohol consumption in moderation
1 drink for women or 2 drinks a day for men maximum
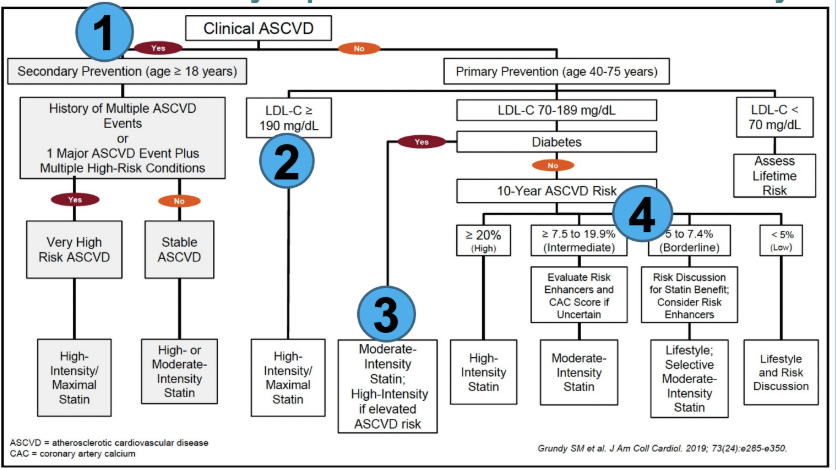
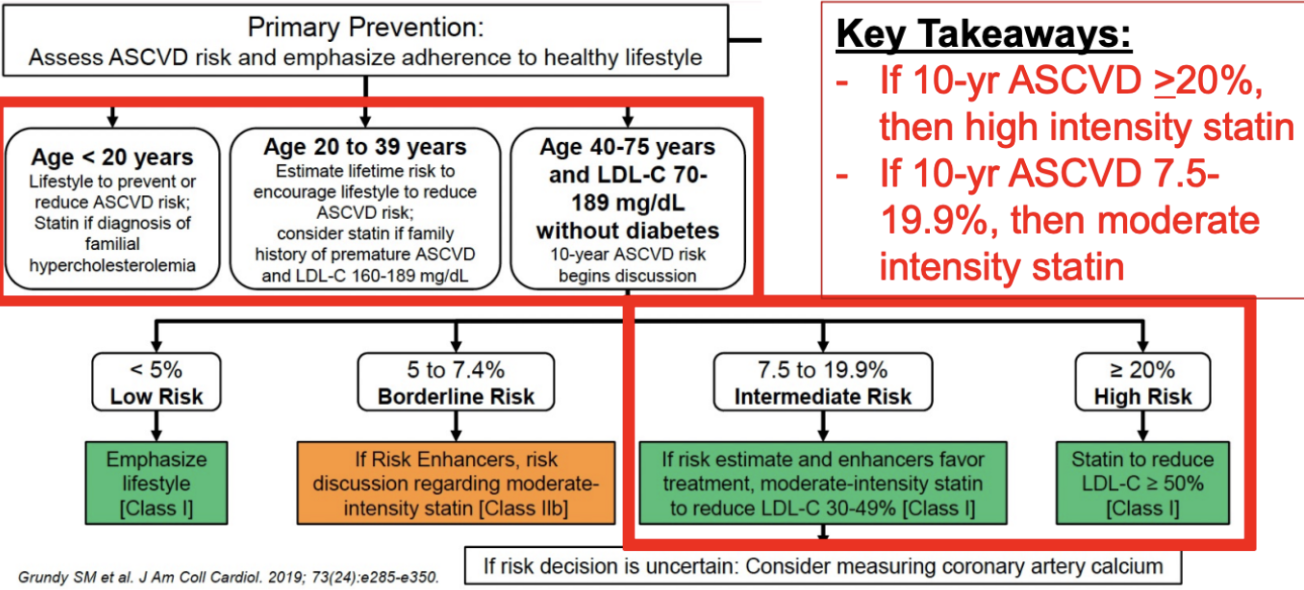
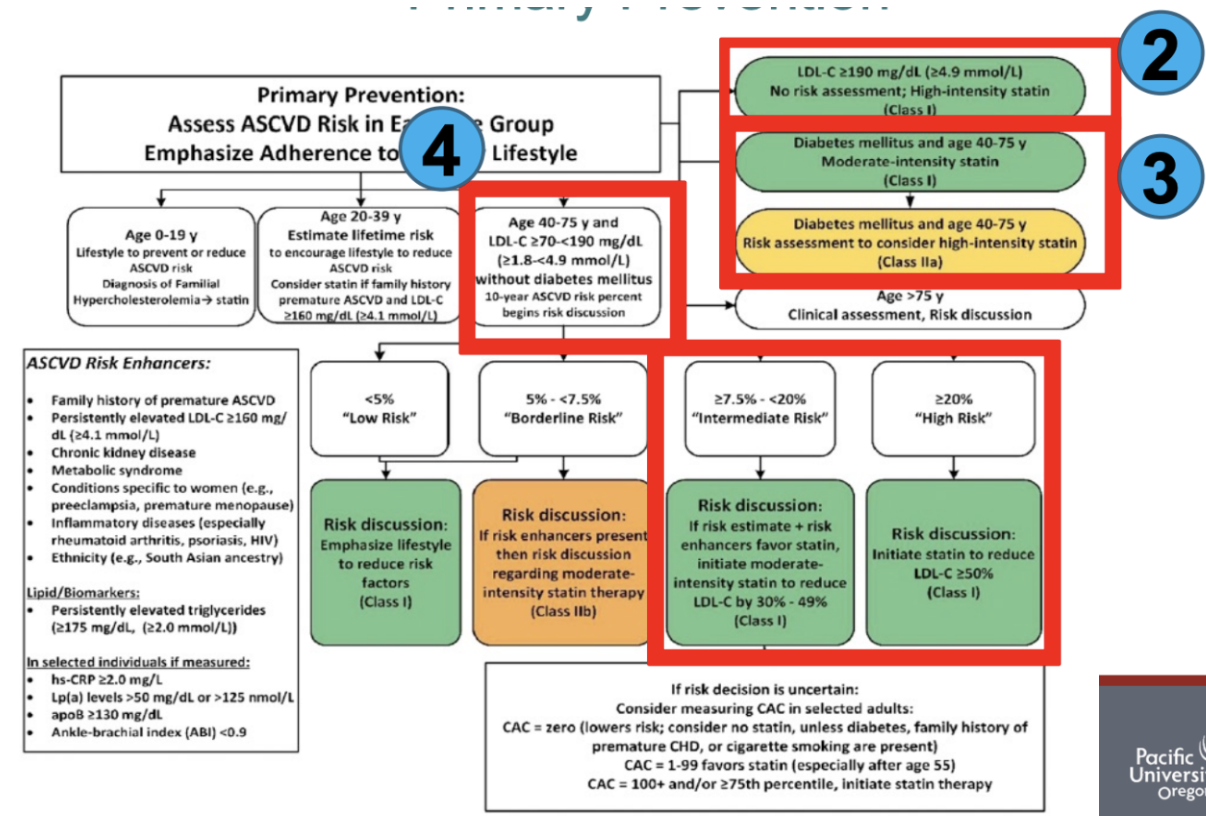
4 Statin Benefit Groups
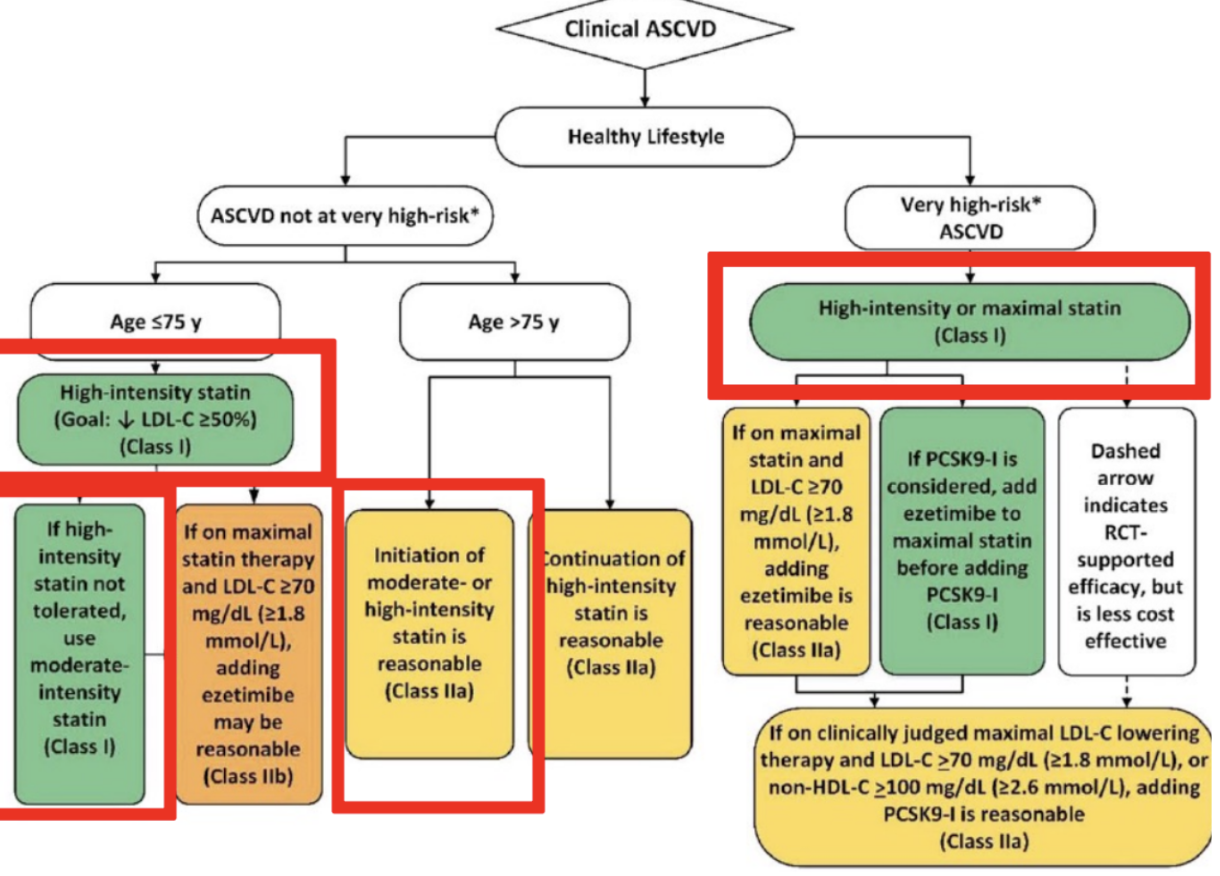
Clinical ASCVD “Secondary Prevention”
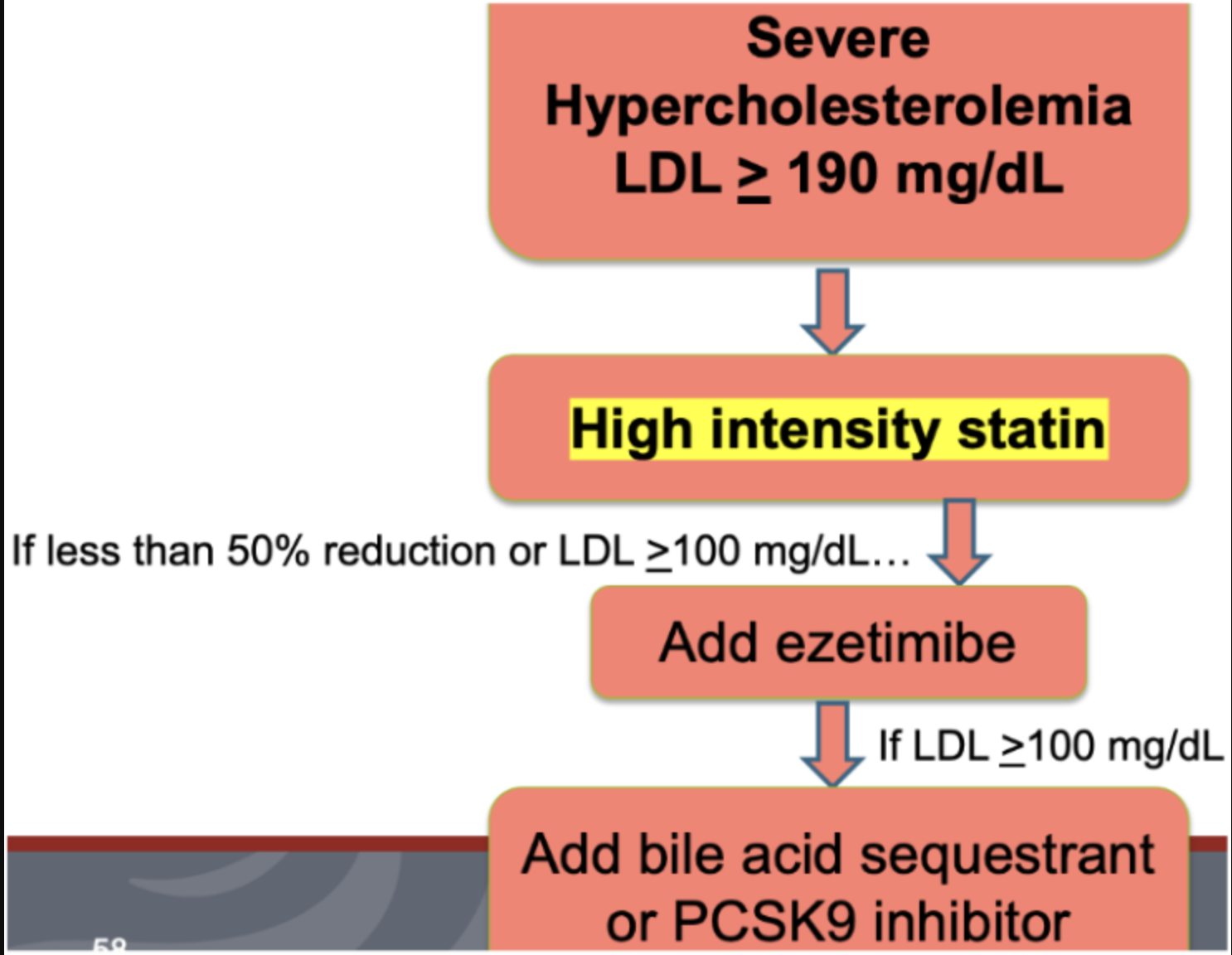
LDL > 190 mg/dL
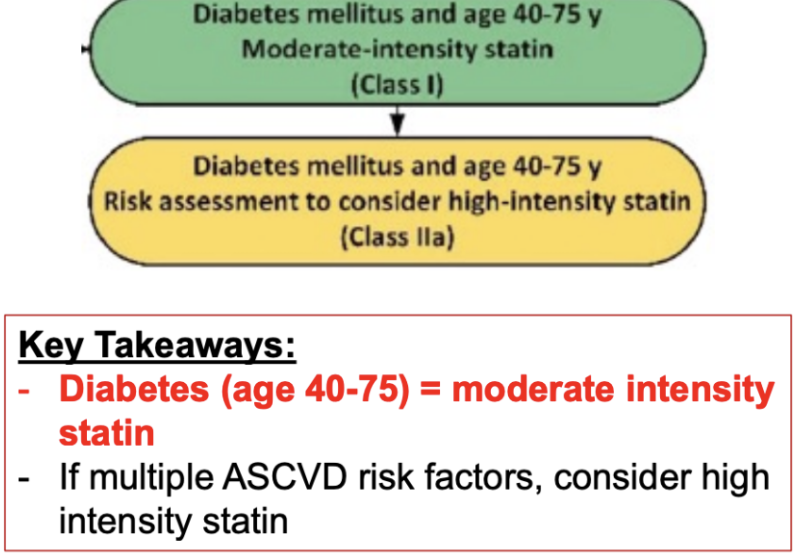
Diabetes Mellitus Age 40-75
No Diabetes Mellitus Age 40-75; LDL 70-189
Clinical ASCVD “Secondary Prevention”
LDL > 190 mg/dL
Diabetes Mellitus Age 40-75 ( primary prevention)
No Diabetes Mellitus Age 40-75; LDL 70-189
Groups 2-4 (LDL, Non/Diabetics)
Atorvastatin 40-80 mg
High-Intensity Statin
Rosuvastatin 20-40 mg
High-Intensity Statin
Atorvastatin 10-20 mg
Moderate-Intensity Statin
Rosuvastatin 5-10 mg
Moderate-Intensity Statin
Simvastatin 20-40mg
Moderate-Intensity Statin
Pravastatin 40-80mg
Moderate-Intensity Statin
Lovastatin 40mg
Moderate-Intensity Statin
Simvastatin 10mg
Low-Intensity Statin
Pravastatin 10-20mg
Low-Intensity Statin
Lovastatin 20mg
Low-Intensity Statin
1st line treatment for LDL reductions and primary and secondary prevention of CV events
Clinical effects: decrease LDL, TG; maintenance or increase of HDL
Monitoring
Fasting Lipid panel
Baseline
4-12 weeks after starting/changing dose to assess for % LDL reduction
CK
Baselines and if experiencing myotoxicity
Liver Function
Baseline and if clinically indicated
Pregnancy
Category x, teratogenic
HMGCoA-Reductase Inhibitors (Statins)
prevents the absorption or cholesterol from the intestine
acts act the brush bored of the small intestine to inhibit cholesterol absorption
Clinical effects: decreases LDL, decreases/maintains TG, increases and maintains HDL
When added to statin, can further reduce LDL by 13-20%
Group 1 and 2 high risk groups → added to statin to decrease LDL low
Ezetimibe
(more expensive - usually last because of cost)
PCSK9 binds to LDL receptors and target them for lysosomal degradation
Too much PCSK9 activity leads to fewer LDL receptors on surface and increases LDL levels in blood
Clinical effects: big decrease in LDL, maintenance HDL and TG
Highest efficacy in LDL response
Place in therapy:
Addition to max-tolerated statin if unable to achieve adequate LDL response
Very costly, brand name
Injectable
When added to statin, can further reduce LDL by 43-64%
PCSK9-Inhibitor
Clinical effects: decrease in LDL/TG; increase in HDL
Place in therapy:
ACC/AHA guidelines make no formal recommendation for use
Evidence does not suggest additional benefit is already taking statin
Adverse effects:
Flushing and Pruritus
Hyperuricemia
Hyperglycemia
Niacin
Clinical effects: decrease LDL, increase/maintain HDL and TG
Place in therapy:
when added to statin can further reduce LDL by 15-30%
Second line after ezetimibe or PCSK9
Counseling:
GI intolerance, many drug interactions, fat-soluble vitamin deficiency
Administer 2 hours before or 4-6 hours other scheduled meds
Bile Acid Sequestrants
Indicates as adjunctive therapy to lifestyle modification and statine therapy for treatment of primary hyperlipidemia in adults with heterozygous familial hypercholesterolemia (HeFH) or ASCVD who require additional LDL lowering
Lowers LDL cholesterol levels by about 23% compared with placebo
Bempedoic acid
Indicated as adjective therapy to lifestyle modification and statin therapy for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or ASCVD who require additional LDL lowering
SQ injection given every 3-6 months
Lowers LDL cholesterol levels by about 50-55% compared with placebo
Inclisiran
Indicated as adjective therapy to lifestyle modification and statin therapy for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or ASCVD who require additional LDL lowering
Monthly IV infusion
Lowers LDL cholesterol levels by about 47-50% compared with placebo
Evinacumab
Clinical effects: decrease/maintain LDL, increase HDL, major decrease in TG
Place in therapy:
Target lowering of TG
Not for LDL lowering
Fibrates
Clinical effects: maintain LDL, increase HDL, major decrease TG
Place in therapy:
Targeted lowering of TG
Not for LDL lowering
Requires 2-4 g/day of EPA + DHA
OTC “fish oil”
Evidence support in decreased CV events with Vascepa
Inconsistent evident for general C benefits with OTC fish oil
Omega-3 Fatty Acids
Treatment for Hypertriglyceridemia
If TG >500 mg/dL
Treat lifestyle and secondary causes first
Consider statin therapy is ASCVD risk > 7.5%
Consider omega-3 fatty acids or fibrate
If TG > 1000 mg/dL
Start omega-3 fatty acids or fibrate to prevent acute pancreatitis
Takes prior over statin recommendations
Treatment options
Omega-3 fatty acids
Lovaza
Vascepa
Fenobrate
Gemfibrozil