Level 3 (Exam 4)- All Examplars
1/108
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
109 Terms
Pathophysiology
What is traumatic brain injury
an injury to the skull or the brain that is severe enough to interfere with normal function
Pathophysiology
What is coup and counter coup
a serious traumatic brain injury where the front of the brain is damaged from the direct impact and the opposite side hits the side of the skull
Pathophysiology
why is counter coup more severe than the initial site of impact
Rationale:
the jerking backwards of the brain hits the back part of the skull. MVA, falls and shaking infant syndrome are increase risk factors to counter coup
Rationale:
increases the risk for hemorrhage
Pathophysiology
What is the Monroe Kellie hypothesis and how is that connected to ICP
The cranial vault:
brain
blood
CSF
1/3 will increase in volume, then the other two must decrease in volume or there will be an increase in ICP
Complications
what are the two complications a skull fracture cause
cerebral hypoxia
ischemia
Nurse interventions
A nurse suspects a basal skull fracture and clear fluid is leaking from the pts ears. What diagnostics can the use to determine CSF possibility
check with a glucose monitor or halo test

Manifestation
A nurse assess bruising over the mastoid process of the ears, what is the condition called
battle sign
Diagnostic
A patient came in with a possible skull fracture and might have a consussion, what diagnostic tool might the nurse use to determine the extent of the fracture
A CT scan (first line)
MRI
Glasgow scale = 15 is best
Nurse Education
A patient that suffered a skull fracture is about to go home. What education should the nurse provide to the patient and the family
educate on the symptoms to watch out for
watch the patient for 24-48 hours after the brain injury
The patient can sleep but wake them every 3-4 hours in the first 24-48 hours
avoid screen time for a few days
avoid aspirin and ibuprofen (acetaminophen is okay)
avoid heavy weight lifting
Manifestations
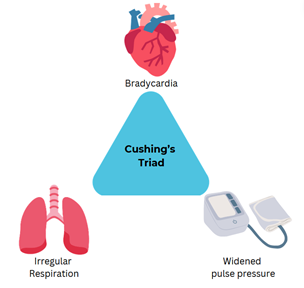
A patient had a head injury and is entering the late stages of the injury. The nurse suspects Crushing Triads. What would the nurse see upon presentation
widened pulse pressure (high systolic/low diastolic BP)
bradycardia (low heart rate)
irregular respiration
Manifestation
decorticate
Manifestations
decerebrate
Pathophysiology
what is a epidural hematoma
Manifestations
Rationale:
bleeding between the dura and the inner surface of the skull
unconscious with brief lucid intervals
headache
NV
Rationale:
these bleed is arterial in nature and bleeds FAST
Pathophysiology
what is a SUBDURAL hematoma
Manifestations
Rationale:
bleeding between the dura and the arachnoid layer of the meninges
decreased LOC
headache
ipsilateral pupil dilation
Rationale:
venous bleed and a slow bleed
Pathophysiology
what vertebra are mostly involved in spinal cord injuries
C1-C5
T12
L1
Pathophysiology
What are the two types of spinal cord injuries
Rationale
primary
secondary
Rationale:
Primary- is direct physical trauma to the spinal cord
secondary- after a primary injury, the injury becomes on going and progressive
Manifestation
what are the symptoms of a spinal cord injury that develops into spinal shock
↓ DTR
Spinal reflex and sensation
flaccid apparency below the level of injury
Nurse intervention
A nurse is caring for a patient who has
HR: 54
TEMP: 97 at 11 am , 99 11:30 am, 100 at 12 pm
BP: systolic of 87
How should should the nurse interpret these findings and what should she do
Rationale:
these are signs of neurogenic shock and should contact the HCP
Pathophysiology
Why is a secondary spinal cord injury dangerous
Rationale:
edema can form within 24 hours and create permeant tissue damage
Which action should the nurse recognize has the highest priority for a patient who was admitted 16 hours earlier with a C5 spinal cord injury?
Assessment of respiratory rate and effort
Cardiac monitoring for bradycardia
Administration of low-molecular-weight heparin
Application of pneumatic compression devices to legs
Assessment of respiratory rate and effort
Edema around the area of injury may lead to damage above the C4 level, so the highest priority is assessment of the patient’s respiratory function
Manifestations
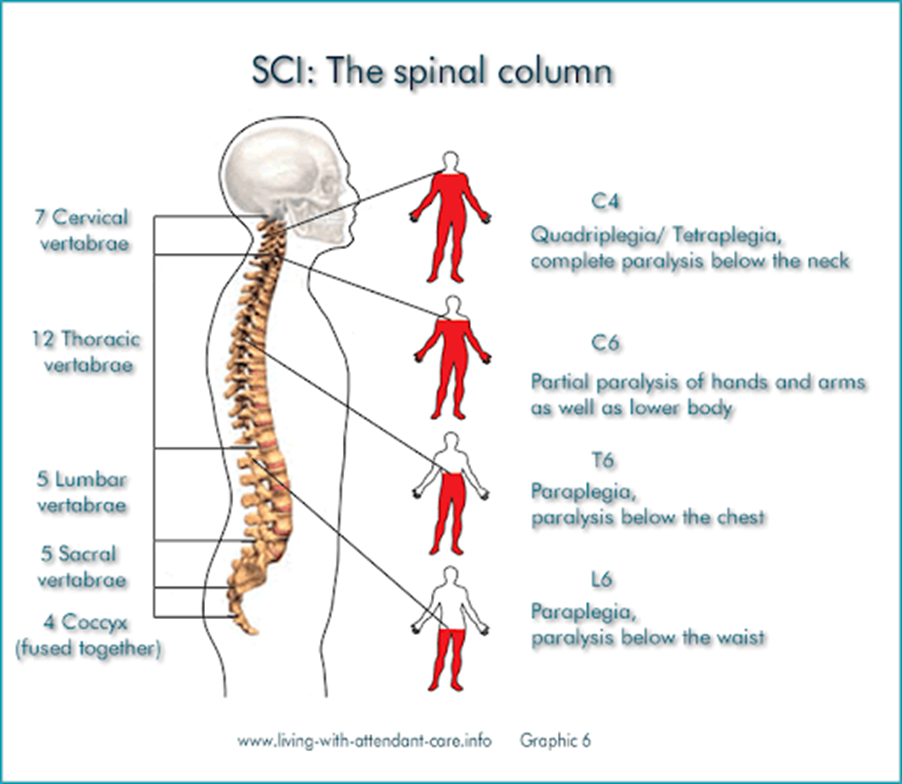
What type of paralysis can be noted if there is damage C4. C6, T6 areas of the spinal cord
C4 = complete paralysis below the neck
C6 = partial paralysis of hand and arms
T6 = paralysis below the neck
Treatment
What medications can be given to pts who have low HR and low RR and have a spinal cord injury
atropine
Nurse Interventions
A nurse is caring for a spinal cord injury patient and is using a Halo Brace. What should the nurse to reduce the risk of infection
provide pin care everyday
Rationale:
the screws are entering the skull via the skin. Break in skin and bone integrity can lead to infections. Care is needed to prevent this
Pathophysiology
what is autonomic dysreflexia
a life threatening condition that can result from spinal cord injuries that affect T6 or higher
Risk Factor
Why is damage to the T6 area of the spinal cord important to understand the triggers of autonomic dysreflexia
Rationale:
T6 is the area of the CNS the sends and receives info to signal to the body of full bladders or bowel impactions.
Rationale:
Damage to the T6 causes the body to not feel when the bladder is full or the bowels are impacted. Full bladder or bowels is the biggest trigger for autonomic dysreflexia
Nurse Interventions
A nurse is caring for a patient who has a T6 spinal cord injury. The nurse take a BP of 160/ 88, HR of 34 and assess the patients bladder- the bladder is hard and distended upon palpation. What is the primary intervention (3 steps)
Rationale:
raise the HOB 45'
Contact the HCP
Do a straight catherization
Rationale:
Damage to the T6 causes the body to not feel when the bladder is full or the bowels are impacted. Full bladder or bowels is the biggest trigger for autonomic dysreflexia. A straight catheterization with remove the built up urine reducing the risk that comes with a full bladder. Elevating the HOB helps reduce the pressure
A BP of 20-40 mm Hg above the baseline + bradycardia (30-40 bpm) + full bladder = autonomic dysreflexia S/S
Treatment
If a patient is experiencing automatic dysreflexia, what medications are given
Rationale:
Nitroglycerin Paste
Rationale:
Nitro will decrease the elevated blood pressure from the autonomic dysreflexia crisis
Manifestations
what are the manifestations of autonomic dysreflexia
hypertension
diaphoresis above the injury
bradycardia
Nurse Interventions
A nurse has assessed for bladder distension and bowel impaction. The nurse notes no distention and impaction. What other nursing interventions should the nurse do to determine triggers to autonomic dysreflexia
assess for skin breakdown, tight clothes and laying on the call light
Pathophysiology
what is a fracture and how are they classified
a disruption or break in bone continuity
Classification
Complete or incomplete
open or closed
stable or unstable
Pathophysiology
Describe the 6 types of fractures
transverse = straight across
spiral =
greenstick = split or bent
comminuted = crumbled
oblique = across / down the bone
pathologic = diseased bone fracture
Manifestations
what are the manifestations of a bone fracture
edema / swelling
pain
muscle spasm
deformities
confusion
Risk Factors
what are the risk factors to fractures
Rationale:
elderly
post menopause
high risk activities
Rationale:
post menopausal women are more at risk due to the development of osteoporosis. As a result, their bones are weaker and will break.
Pathophysiology
what are the stages of bone healing
Rationale:
fracture hematoma- a blood clot forms at the fracture
granulation tissue-
callus formation- C.T. forms a callous at the end parts of the fracture
ossification- the bone hardens
consolidation and remodeling- the callous is reformed and the bone has shape again
Nurse Interventions
why is fracture reduction like manipulation, reduction and traction devices important nursing interventions for fractures
these intervention keep the bone aligned properly
Nurse Interventions
Give examples of fracture immobilization tools / interventions
external cast = a physical cast placed over the fracture
internal or external fixation = using pins to immobilize the fracture
maintenance traction = (bucks traction) used in the hospital to immobilize the fracture
Nurse Interventions
What interventions are needed if a patient has open fractures
Rationale:
surgical detriment
tetanus / antibiotics
Rationale:
fractures that have open wounds are at increase risk for infection. Cleaning and admin of drug therapy early reduce the risk of infection development.
Nurse Interventions
After a fracture has be immobilized. what should nurse do to prevent complications
Rationales
The nurse should do neuro checks every hour
turn every 2 hours
keep the cast dry
elevate above the head
Rationale:
to make sure they don’t have nerve damage and have good blood flow
to reduce pressure injuries risk
protect skin integrity / infection
Treatment
what is a skin traction boot
Rationale:
A skin traction boot is a immobilization device were weights are hanging off the end of the bed.
Rationale:
the weights must never touch the ground because the tension is what helps immobilize and align the fracture to heal properly
it also helps reduce muscle spasms
Treatment
A nurse just finished obtaining report on a patient who fell 6 stories. The patient has a fracture on the right femur. The nurse is notified that the patient is on a Skeletal Traction Bed Frame. An order is placed for 10lbs to hang from the traction device. The nurse notes that the patient’s device only has 2lbs. What should the nurse do?
Rationale:
Contact the HCP
Rationale:
In order for the traction device to work, tension must be created. Improper weight will reduce said tension and prevent the immobilization/ alignment needed to heal the fracture. Contact the HCP to correct the weight.
Nurse Intervention
If a patient is on alignment devices to correct the fracture, what should the nurse do to reduce infection
Rationale:
pin care everyday
Rationale:
pins are breaking skin integrity. Break in skin integrity can lead to infection at the points of entry
Nurse Education
what education should the nurse provide to the patient who has a cast
Rationale:
DO NOT
get it wet
remove padding
insert objects
put lotion in the cast
bear weight
cover it with plastic
Rationale:
adding water to the internal section of the cast / objects can increase the risk for infection due to breaks in skin integrity
DO
keep it dry
cover it before showering
use a blow dryer to dry the cast after showering
elevate above the heart for the first 48 hours
move the extremities
report odor, drainage, pain, swelling, discoloration of finger/toes, tingles
educate the patient to do their cast and fracture appointment follow ups
Rationale:
Keeping the inside of the cast reduces the risk of infection
Risk Factors
what are the risk factors to have an amputation for
middle / older adults = PVD, atherosclerosis, DM
young adults = trauma (vets)
osteomyelitis
frostbite
Diagnostics
What are the diagnostics needed to determine if a patient might need an amputation
Rationale:
X ray
CT or MRI
vascular studies
Rationale:
CT and X rays can help determine if osteomyelitis is present. The disease increase the risk for amputation
vascular studies show how far down the blood travels and help the doctor determine how much to cut
Nurse Interventions
A nurse is caring for a patient who will undergo surgery to amputate his left leg. What should the nurse educate / tell the patient prior to the start of the surgery
get consent prior to start of the surgery
explain the reason for the amputation
Nurse Intervention
A nurse is caring for a patient post-op from surgery. The patient underwent a left leg amputation. The nurse assess the incision site and notes lots of bright red blood saturating the gauze. What should the nurse do first.
Rationale:
Contact the HCP
Rationale:
the sutures may have opened up and caused hemorrhage. Circulation is being compromised . The patient needs to return to the operating room to fix the sutures. Life threatening
Nurse Intervention
What should the nurse assess after an amputation surgery
Rationale:
do circulation checks
do neuro checks
Rationale:
circulation checks establish good perfusion or lack there of
to monitor for neuro damage or compartment syndrome
Pathophysiology
Compartments syndrome is a decrease in pressure within a compartment that decompresses blood vessels, nerves, and/or tendons in the leg, arm, and shoulder.
True
False
Rationale:
False
Rationale:
Compartment syndrome is an increase in pressure directly related to tissue swelling.
Pathophysiology
What is phantom leg syndrome
Rationale:
Pain in a missing body part
Rationale:
the nerves are severed at the site of amputation. The brain is still sending signals to that area indicating pain
Treatment
A patient states “i got my amputation surgery 3 weeks ago, but I’m feeling pain where my leg use to be” What should the nurse do?
Give the pain medication
Risk Factor
what increases the risk to develop compartment syndrome
trauma
tight dressing or cast
hemorrhage into compartment
Manifestations
What are the 6 Ps of compartment syndrome
pain
pallor
pressure
paresthesia
paralysis
pulseless
Rationale:
If a patient complains of any of these signs, then they are at risk for compartment syndrome. Notify the provider ASAP.
Diagnostic
what test is used before and after exercise to determine compartment syndrome risk
intercompartment pressure test
Treatment
A patient is at risk for compartment syndrome. What surgical treatment must be done
Rationale:
fasciotomy
Rationale:
this procedure relieves pressure caused by the syndrome. If not done, then the patient might need an amputation
Treatment
Name:
Mannitol
MOA:
Treatment
Name:
Mannitol
MOA:
used to decreased the high blood pressure when a pt has increased ICP
Pathophysiology
what are tonic-clonic seizures
the most common type of seizures. Involuntary miscle contractions and loss of consciousness.
Manifestations
what are the two most common symptoms of tonic clonic seizures
muscle rigidity
jerking movements
lasts 1-2 mins
Nurse intervention
During the Seizure
>5 mins →
Place them on seizure precautions
Monitor LOC and keep airway
If the seizure lasts more than 2 mins
During the Seizure
>5 mins → emergency → call 911 → keep track of duration and start time of seizure
Assess if the patient has had a head strike → to determine further damage.
Place them on seizure precautions
Protect pt- don't restrain them and place them on their side → to prevent aspiration
Have padded side rails
Monitor LOC and keep airway
Make sure suction and Ambu bag are at bedside
If the seizure last more than 2 mins
call 911 and note the start and duration of the seizure
Pathophysiology
what will a patients post ictal state be after a tonic clonic seizure
they will be hard to arouse and allow them to sleep
Nurse Interventions
what are common interventions a nurse can obtain when a pt is at risk of an active seizure
document the start and duration of the seizure
know which body parts are moving
Diagnostics
what are the diagnostics for generalized seizures
Rationale:
EEG
MRI
SPECT
Rationale:
EEG show the seizure type
MRI show lesions on the brain
SPECT show which part of the brain is causing the seizure
Pathophysiology
what is a and absent / petite mal seizure
Manifestations
they space out and stare and don’t respond
Manifestations
lasts seconds
automatisms- sudden and repetitive motions (knee pats)
Pathophysiology
what is a and atonic seizure
Manifestations
Rationale:
when there is a lack of muscle tone and they completely pass out
Manifestations
slump over
Rationale:
the sudden slump over increase the risk for head trauma
Risk Factor
what is the biggest risk factor for someone to develop seizures
Not compliant anti-seizure meds
Pathophysiology
what is a focal seizure and what are its subtypes
Complications
originate in one area of the brain
simple partial- their conscious will stay intact
complex partial- impaired conscious
Complication
the focal seizure can go from simple to complex
Pathophysiology
what are febrile seizures. They have a rapid recovery of the post ictal state
tonic clonic seizures but with a high fever
Risk Factors
what are the risk factors for febrile seizures
6 months - 5 years
history of febrile seizures
fever and infection
Treatment
A child has febrile seizures and being given rectal diazepam PRN. What are the considerations the nurse should be aware of when giving this drug
Rationale:
Nurse consideration:
given when the child has 3 or more seizures
can be given every 8 hours
watch for sedation
Rationale:
diazepam is a a benzodiazepine. these classes of drugs have a adverse effect of sedation and should be monitored when given to a child. A safety risk
Nurse Interventions
what questions should a nurse ask when working with children who experience febrile seizures
do they have a Hx of seizures
have they experienced trauma
Nurse Education
what education should the nurse give to the parents of the child who has experienced febrile seizures
teach the signs of seizure in the child
seek medical attention ASAP if the seizure is recurrent
Pathophysiology
what is status epilepticus
a repeated seizure that had no recovery and lasts for 30 mins
Diagnostic
what are the labs and diagnostics for status epilepticus
Rationale:
EEG
Glucose
Electrolytes
Phenytoin level
Rationale:
hypoglycemia can occur in status epilepticus. May need dextrose to correct low levels
low level of phenytoin can indicate that the pt is not taking enough and causing the seizure to return.
Nurse Interventions
A pt is experiencing status epilepticus, what should the nurse do first before the admin of IV benzodiazepines
Rationale:
asses the IV access
Rationale:
the IV site needs to be patent so the IV medication can flow into the pt and treat the status epilepticus
Treatment
what are the three drugs given for status epilepticus and which one is first line
IV Benzodiazepines (first line)
lorazepam, diazepam
Phenytoin
Dextrose
Nurse Interventions
A nurse is caring for a patient who has a history of seizures. The patient experienced an episode of status epilepticus, and now is recovering. What should the nurse assess first
Rationale:
Assess if they are on anti-convulsant meds and if they are taking the meds or have stopped them abruptly
Rationale:
stopping anti-convulsant drugs abruptly or discontinuing can increase the risk of seizure episodes to occur or re-occur.
Nurse Education
What education should be provided to seizure patients
Rationale:
wear medical ID bracelet
Educate about meds (phenytoin)
constantly monitor your labs
educate about oral or dental care
educate parents about seizure care steps
educate pts to not change or stop drugs abruptly
contact HCP if needed
Educate about contraceptive and anticonvulsant drugs
Rationale:
phenytoin level need to be monitored to make sure there is enough in the body to create a desired effect
phenytoin can cause gingival hyperplasia
it can increase infection risks
they need to brush their teeth to prevent the side effect
mixing anticonvulsants and contraceptives can increase pregnancy
make sure HCP is contacted if they want to get pregnant
Treatment
what diet can a seizure pt be on
Rationale:
Keto diet- high carb and low fat
Rationale:
a keto diet can reduce seizure frequency
Pathophysiology
what is a stroke
infarction (death) of specific portions of brain tissue due to poor blood supply
Pathophysiology
why is 4-6 mins of interrupted blood flow to the brain deadly
that is how long it takes for infarction of brain tissue to occur and create irreversible damage
Pathophysiology
what is affected when the frontal lobe experiences a stroke
speech
thinking
memory
movement
Pathophysiology
what is affected when the parietal lobe experiences a stroke
language
touch
space perception
Pathophysiology
what is affected when the temporal lobe experiences a stroke
hearing
learning
feelings
Pathophysiology
what is affected when the occipital lobe experiences a stroke
vision
color perception
Pathophysiology
what is affected when the cerebellum experiences a stroke
balance
coordination
Pathophysiology
what is affected when the brain stem experiences a stroke
a disruption in HR, RR, and temp control
Common Manifestations of Stroke
F =
A =
S =
T =
F = face / facial droop
A = arms / arm droop
S = speech / slurred speech
T = time / call 911
Types of Strokes
what is a TIA
Risk Factors
Nurse Education
Rationale:
Not a stroke, but temp decrease in blood flow that resolves in 24 hours with no brain cell damage
Risk Factors
signs of an impending stroke
Nurse Education
pts need education and to prevent reoccurrence
educate the pt to get frequent imaging and lab tests done
Rationale:
the more TIA a person has, the more their stroke risk increases
Types of Strokes
what is an ischemic stroke
Manifestations
Motor
Sensory
Psych (due to frontal lobe damage)
Risk Factors
there is a block in the cerebral blood vessels → ischemia of brain tissue → infarction of tissue
Manifestations
Motor
loss of voluntary movement
left brain damage = poor right sided movement
Sensory
visual disturbances
loss of balance coordination and proprioception
Psych
poor memory, attention span, frustrated and depressed
Risk Factors
A-Fib- the vents cant move the blood and clots form in the atrium
hypertension
Peds Congenital heart defects
Covid 19 + D dimer
Types of Strokes
what is an hemorrhagic stroke
Manifestations
Sensory
Risk Factors
Types of Strokes
a rupture of a vessel inside the brain due to hypertension not being controlled
Manifestations
Sensory
severe headache
decreased LOC (early sign of deuteriation)
Vision loss
diplopia
tinnitus
photophobia
Risk Factors
uncontrolled hypertension
Diagnostic
what are the diagnostics for a ischemic stroke
Rationale:
CT w/o contrast within 20 mins of arrival
Rationale:
to determine if the stroke is hemorrhagic or ischemic
Diagnostic
what are the diagnostics for a hemorrhagic stroke
Rationale:
CT w/o contrast
Lumbar puncture
Rationale:
CT to determine stroke type
Lumbar if the CT come back negative
do not do it if ICP is detected, due to increase pressure on the brain stem and brain. Leads to increase hemorrhage
Treatment - THROMOLYTICS
Name:
MOA:
Side Effects:
Nurse Consideration:
Name:
tPA
MOA:
dissolves blood clots and restores blood flow
Side Effects:
bleeding
Nurse Consideration:
must be given within 3 hours of onset stroke symptoms
don’t give to hemorrhagic stokes
don’t give if the the INR >1.7 on anticoagulants
don’t give anticoagulant drugs for 24 hours
give if their PT is < 15
give if their platelets are >100k
No if they have head injuries or surgeries in the past 3 months
no if their BP is greater than 180/110
admin labetalol to lower the BP
monitor BP every 5 mins
no if they had GI bleeds
monitor IV sites
get a swallow study
Treatment
what drug can be given to hemorrhagic stroke patients if they cant take the tPA
Heparin
Treatment
what drug can a hemorrhagic stroke patient take if they are at risk for ICP
Rationale:
Mannitol
Rationale:
decreases the ICP by urinating the extra fluid and relieving pressure off the brain
Treatment
A patient is taking TPA IV for their ischemic stroke and is starting to show signs of lethargy, what is the nurses priority intervention?
STOP the IV
call a rapid
give O2
Rationale:
their ischemic stroke has turned hemorrhagic. Lethargy ( ↓ LOC) is the first sign of deterioration of hemorrhagic strokes
Nurse Interventions
What nursing interventions are needed when a hemorrhagic stroke pt has ICP
Rationale:
admin mannitol + monitor for low BP
elevate the HOB 30-45 degrees
watch for hypoglycemia
Give stool softener
Rationale:
mannitol decreases / reduces the ICP
monitoring a low blood pressure is important to reduce the risk of brain ischemia
elevation of the head of the bed decreases the ICP
hypoglycemia makes stroke worse
a stool softener reduces straining, which can elevate the BP and make the ICP worse
Pathophysiology
what are the two neurotransmitters being affected in parkinsons disease
Pathophysiology
Parkinson's disease is associated with decreased levels of dopamine resulting from destruction of pigmented neuronal cells in the substantia nigra in the basal ganglion region. The loss of dopamine stores results in more excitatory neurotransmitters (acetylcholine) than inhibitory transmitters (dopamine). Serotonin and norepinephrine are not involved.
Manifestations
What are the 4 cardinal signs of parkinsons
Tremor
Rigidity
Bradykinesia- slow acting movement
Posture instability
Manifestations
when a patient has postural instability, what can you see and why is it bad
Posture instability
Stand with their head or have a propulsive gait
Can cause the loss of balance
increases the risk for falls