pathology + histology week 17
0.0(0)
Studied by 0 peopleCard Sorting
1/67
Earn XP
Description and Tags
Last updated 4:05 PM on 7/8/26
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
1
New cards
go over theme 1 for the skin
2
New cards
cell types of the skin
1. keratinised squamous epithelial cells = keratinocytes:
* held together by desmosomes
* secrete cytokines and defensins
2. melanocytes:
* produce melanin, absorb and protect against UV radiation
3. DCs:
* intraepidermal DCs = langerhans cells
* specialised dendrocytes are found in the dermis, similar functions to langerhans cells
* skins first line of defense (is mechanincal defense not the first line?)
* langerhans secrete factors that augment innate immune responses → migrate from the skin to regional lymph nodes to present their antigens = stimulate the adaptive immune system
4. lymphocytes:
* T cells stimulated by ^ express cutaneous lymphocyte associated antigen (CLA) and chemokines receptors (eg. CCR4/10) → leave the lymph node → go back to the dermis (process is caused by chemokines secreted by active keratinocytes)
* small numbers of B cells are found in the dermis → humoural response
5. skin microbiome → prevents colonisation by other organisms
6. nerves, sweat glands, muscles, hair follicles etc:
* merkel cells are found in the epithelial basal cell layer, may have neuroendocrine or mechanoreceptor functions
7. adnexal components:
* sweat glands → guard against variations of body temp.
* hair follicles → produce hair → protect epithelial stem cells (?)
3
New cards
disorders of pigmentation and melanocytes (names)
1. freckles
2. lentigo
3. melanocytic nevus (pigmented nevus, mole)
4. dysplastic nevi
5. melanoma
4
New cards
freckles
* most common pigmented lesions of childhood in lightly pigmented people
* histologically similar to cafe au lait spots seen in neurofibromatosis type 1 but they are larger, arise independently of sun exposure and contain aggregated melanosomes
* hyperpigmentation is due to increased amount of melanin pigment within basal keratinocytes, the __associated__ melanocytes may be slightly enlarged but are normal in density
* they fade and darken in a cyclic fashion during winter and summer, NOT due to a change in the number of melanocytes but due to a change in the degree of pigmentation
* histologically similar to cafe au lait spots seen in neurofibromatosis type 1 but they are larger, arise independently of sun exposure and contain aggregated melanosomes
* hyperpigmentation is due to increased amount of melanin pigment within basal keratinocytes, the __associated__ melanocytes may be slightly enlarged but are normal in density
* they fade and darken in a cyclic fashion during winter and summer, NOT due to a change in the number of melanocytes but due to a change in the degree of pigmentation
5
New cards
lentigo
* common benign localised hyperplasia of melanocytes
* occurs at all ages but most commonly in infants and children
* may involve mucous membranes as well as the skin
* small oval tan brown macules or patches, sharply circumscribed
* linear (nonnested) melanocytic hyperplasia restricted to the cell layer immediately above the BM that produces a hyperpigmented basal layer
* unlike freckles, they do not darken when exposed to sunlight
* occurs at all ages but most commonly in infants and children
* may involve mucous membranes as well as the skin
* small oval tan brown macules or patches, sharply circumscribed
* linear (nonnested) melanocytic hyperplasia restricted to the cell layer immediately above the BM that produces a hyperpigmented basal layer
* unlike freckles, they do not darken when exposed to sunlight
6
New cards
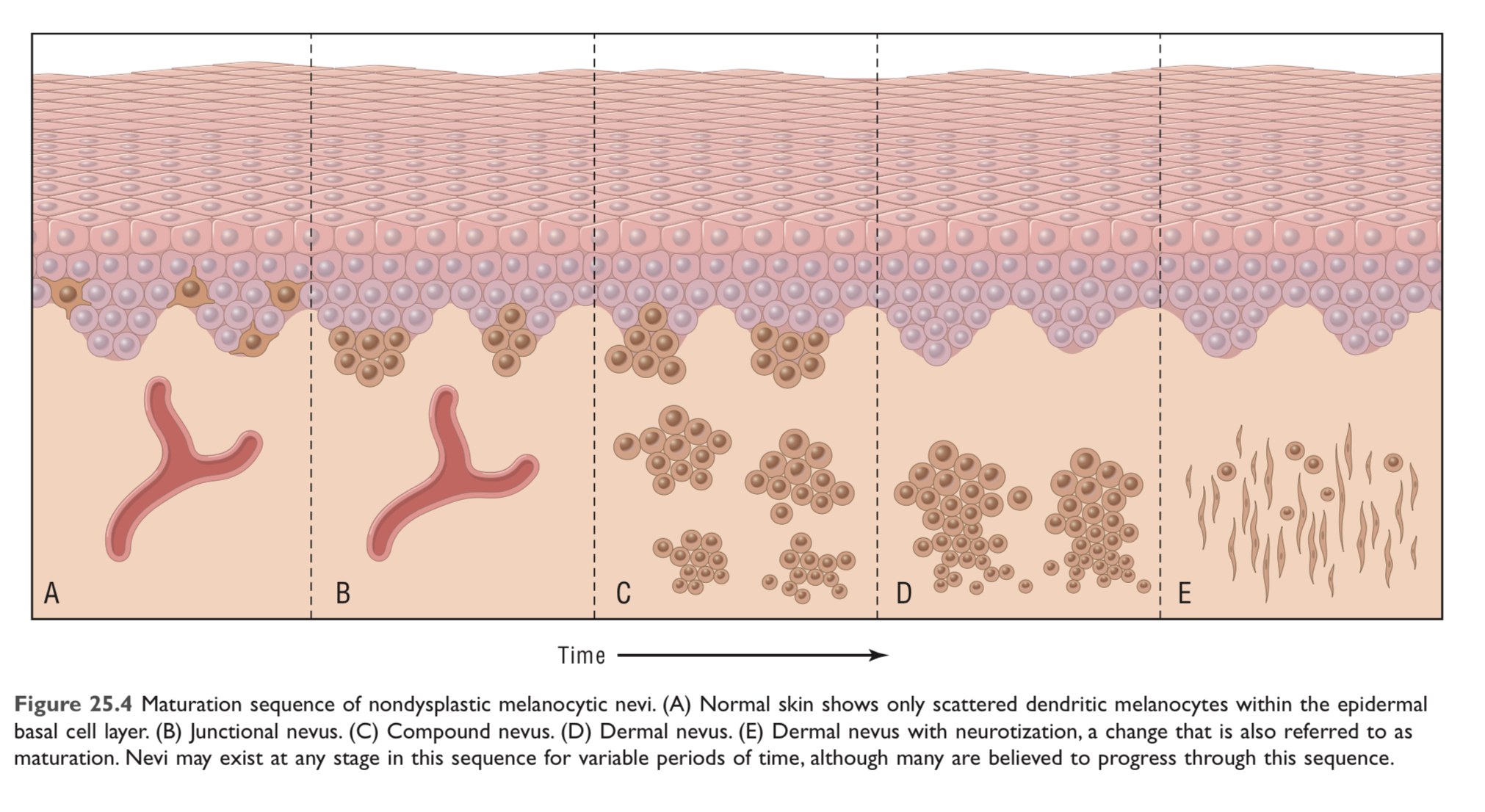
melanocytic nevus (pigmented nevus, mole)
* common benign neoplasms (non dysplastic)
* usually caused by acquired mutations in components of the RAS signalling pathway (eg. activation of RAS or BRAF)
* they rarely give rise to melanomas, may be due to oncogene induced senescence (+ RAS/BRAF → accumulation of p16/INK4a → growth arrest)
* uniformly pigmented, small, relatively flat
* may become more prominent during pregnancy → some level of hormone sensitivity
* thought to progress through a series of morphologic changes over time
1. junctional nevi: aggregated or nests of round cells that grow along the dermoepidermal junction
nevus cells are uniform and rounded, contain small nuclei and show little to no mitotic activity
2. compound nevi: ^ grow into the underlying dermis
3. intradermal nevi: epidermal nests are lost, melanocytes acquire fusiform contours and grow in fascicles resembling neural tissue (= neurotisation) → figure E
* 2 and 3 are usually more elevated than junctional nevi
* usually caused by acquired mutations in components of the RAS signalling pathway (eg. activation of RAS or BRAF)
* they rarely give rise to melanomas, may be due to oncogene induced senescence (+ RAS/BRAF → accumulation of p16/INK4a → growth arrest)
* uniformly pigmented, small, relatively flat
* may become more prominent during pregnancy → some level of hormone sensitivity
* thought to progress through a series of morphologic changes over time
1. junctional nevi: aggregated or nests of round cells that grow along the dermoepidermal junction
nevus cells are uniform and rounded, contain small nuclei and show little to no mitotic activity
2. compound nevi: ^ grow into the underlying dermis
3. intradermal nevi: epidermal nests are lost, melanocytes acquire fusiform contours and grow in fascicles resembling neural tissue (= neurotisation) → figure E
* 2 and 3 are usually more elevated than junctional nevi
7
New cards
nevus cells and their types
* a variant of melanocytes
* larger than typical melanocytes, don’t have dendrites, have more abundant cytoplasm with coarse granules
* usually located at the dermoepidermal junction or in the dermis of the skin
\
1. superficial nevus cells → larger, tend to produce melanin, grow in nests
2. deeper nevus cells → smaller, produce little to no pigment, appear as cords and single cells
* larger than typical melanocytes, don’t have dendrites, have more abundant cytoplasm with coarse granules
* usually located at the dermoepidermal junction or in the dermis of the skin
\
1. superficial nevus cells → larger, tend to produce melanin, grow in nests
2. deeper nevus cells → smaller, produce little to no pigment, appear as cords and single cells
8
New cards
forms of melanocytic nevi\*\*\*
9
New cards
oncogene induced senescence
a robust and sustained antiproliferative response brought about by oncogenic signaling resulting from an activating mutation of an oncogene, or the inactivation of a tumor-suppressor gene
10
New cards
what causes neurotisation
enzymatic changes = progressive loss of tyrosine kinase activity and acquisition of cholinesterase activity
11
New cards
how to distinguish benign nevi from melanomas
melanomas dont have the changes associated with neurotisation (?)
12
New cards
dysplastic nevi
* can be direct precursors of melanoma + multiple lesions are a marker of an increased risk for ^
* most are acquired rather than congenital
* dysplastic nevus syndrome/familial atypical mole/melanoma syndrome → autosomal dominant disorder → tendency to develop multiple dysplastic nevi and melanoma are co inherited
__!! not all melanomas in individuals with dysplastic nevus syndrome arise from dysplastic nevi → these lesions are best viewed as indicators of increased melanoma risk__
\
* regardless, the vast majority are clinically stable and never progress
* starts off with RAS/BRAF then CDKN2A or CDK4 mutations
* not all patients with germline mutations in CDKN2A or CDK4 have dysplastic nevi and not all familial dysplastic nevi are associated with mutations in these genes
* patients may have hundreds
* flat macules, slightly raised plaques with a pebbly surface or target like lesions with a darker raised center and irregular flat periphery
* recognised by their large size, variability in pigmentation and irregular borders
* occur on both sun exposed and protected skin (unlike moles)
* usually involve the epidermis and dermis, nevus cell nests within the epidermis may be enlarged and often fuse with adjacent nests
* single nevus cells begin to replace the normal basal cell layer along the dermoepidermal junction → lentiginous hyperplasia
* other features → (in the superficial dermis) lymphocytic infiltrates, release of melanin from dead nevus cells into the dermis where it is phagocytosed by macrophages, linear fibrosis surrounding the epidermal rete ridges
==__check histology pictures and label them!!!!!!!__==
* most are acquired rather than congenital
* dysplastic nevus syndrome/familial atypical mole/melanoma syndrome → autosomal dominant disorder → tendency to develop multiple dysplastic nevi and melanoma are co inherited
__!! not all melanomas in individuals with dysplastic nevus syndrome arise from dysplastic nevi → these lesions are best viewed as indicators of increased melanoma risk__
\
* regardless, the vast majority are clinically stable and never progress
* starts off with RAS/BRAF then CDKN2A or CDK4 mutations
* not all patients with germline mutations in CDKN2A or CDK4 have dysplastic nevi and not all familial dysplastic nevi are associated with mutations in these genes
* patients may have hundreds
* flat macules, slightly raised plaques with a pebbly surface or target like lesions with a darker raised center and irregular flat periphery
* recognised by their large size, variability in pigmentation and irregular borders
* occur on both sun exposed and protected skin (unlike moles)
* usually involve the epidermis and dermis, nevus cell nests within the epidermis may be enlarged and often fuse with adjacent nests
* single nevus cells begin to replace the normal basal cell layer along the dermoepidermal junction → lentiginous hyperplasia
* other features → (in the superficial dermis) lymphocytic infiltrates, release of melanin from dead nevus cells into the dermis where it is phagocytosed by macrophages, linear fibrosis surrounding the epidermal rete ridges
==__check histology pictures and label them!!!!!!!__==
13
New cards
probability of developing melanoma in a person with dysplastic nevus syndrome is…
>50% by the age of 60
14
New cards
tumour progression in dysplastic nevi (photo)
15
New cards
if melanocytic nevi and dysplastic nevi start out the same, what differentiates them?
both start off with acquired activating mutations in NRAS and BRAF genes but dysplastic nevi (in dysplastic nevus syndrome) often have inherited loss of function mutations in CDKN2A (codes for p16 → inhibits CDK4/6), others have mutations that make CDK4 resistant to inhibition by p16
\
not all patients with germline mutations in CDKN2A or CDK4 have dysplastic nevi and not all familial dysplastic nevi are associated with mutations in these genes
\
not all patients with germline mutations in CDKN2A or CDK4 have dysplastic nevi and not all familial dysplastic nevi are associated with mutations in these genes
16
New cards
melanoma
* check theme 2 (?)
* most deadly of all skin cancer, strongly linked to acquired mutations caused by UV
* relatively common neoplasm, most are cured surgically but their reported incidence is increasing
* in 10-15%, the risk of melanoma is inherited as an autosomal dominant trait with variable penetrance
* most common mutation → BRAF,
* repair of UV radiation induced DNA damage is imperfect so UV exposure leads to accumulation of mutations
* high rate of point mutations
* irregular and often notched borders
* melanoma cells have a ‘characteristic’ appearance
* most deadly of all skin cancer, strongly linked to acquired mutations caused by UV
* relatively common neoplasm, most are cured surgically but their reported incidence is increasing
* in 10-15%, the risk of melanoma is inherited as an autosomal dominant trait with variable penetrance
* most common mutation → BRAF,
* repair of UV radiation induced DNA damage is imperfect so UV exposure leads to accumulation of mutations
* high rate of point mutations
* irregular and often notched borders
* melanoma cells have a ‘characteristic’ appearance
17
New cards
melanoma cells
* larger than normal melanocytes or those in melanocytic nevi
* enlarged nuclei with irregular contours
* chromatin clumped at the periphery of the nuclear membrane
* prominent red (eosinophilic) nucleoli
* appearance is similar in radial/vertical growth
* enlarged nuclei with irregular contours
* chromatin clumped at the periphery of the nuclear membrane
* prominent red (eosinophilic) nucleoli
* appearance is similar in radial/vertical growth
18
New cards
most frequent driver mutations in melanoma
1. affecting cell cycle control:
* CDKN2A → 40% of autosomal dominant melanomas
* CDKN2A codes for p15/16 and ARF → in melanomas, p16 is affected (ARF might also be affected)
2. pro-growth pathways:
* in sporadic melanoma → increases in RAS (15-20%) and PI3K/AKT
* activation of BRAF (usually combined with loss of PTEN → increased PI3K/AKT) → seen in 40-50% MOST COMMON MUTATION
* PTEN loss is seen in 20% of non sun-exposed areas
* loss of NF1 may also be seen (negative regulator of RAS)
3. telomerase:
* mutations in the promoter of TERT in sporadic melanoma, rarely inherited
19
New cards
most important risk factor for melanoma
periodic severe sunburns early in life \n personal or family history of melanoma or atypical nevi
20
New cards
benign nevi vs melanoma
melanoma → variation in colour, zones of hypopigmentation may also appear due to focal regression of the tumour, borders are not smooth/regular
21
New cards
mucosal lentiginous melanoma
* patient usually in 50s to 60s
* 2/3 of patients are male
* 80% on hard palate or maxillary alveolus
* similar in clinical characteristics to other melanomas
* may show "moth-eaten" bone destruction
* 2/3 of patients are male
* 80% on hard palate or maxillary alveolus
* similar in clinical characteristics to other melanomas
* may show "moth-eaten" bone destruction
22
New cards
types of melanoma
1. superficial spreading:
* most common form (70%)
* usually from a benign mole
* usually in sun exposed areas
2. nodular:
* 15% of melanomas
* starts as a raised spot (light or dark)
* grows vertically and rapidly
3. lentigo maligna:
* indolent lesions of the face of older men, mistaken for an age spot
* may remain in the radial growth phase for several decades
* sun exposed area
4. acral lentiginous:
* unrelated to sun exposure
* common in dark skin
23
New cards
growth phases of melanoma
1. radial → horizontal along epidermis and superficial dermis (low risk of metastasis) = lentigo, superficial and acral/mucosal
2. vertical → growth into the deep dermis (increased risk of metastasis) = nodule
24
New cards
pathological variables of melanoma to predict outcome
1. tumour depth of invasion (breslow thickness)
2. number of mitoses
3. evidence of tumour regression (may be due to host immune response) → no regression has better prognosis
4. ulceration of overlying skin
5. presence and number of tumour infiltrating lymphocytes → less = better prognosis
6. location (central body or extremity)
(also do sentinel lymph node biopsy)
25
New cards
ABCDE of melanoma
**A**symmetry
irregular **B**order
variegated **C**olour
increasing **D**iameter
**E**volution or change over time
irregular **B**order
variegated **C**olour
increasing **D**iameter
**E**volution or change over time
26
New cards
best markers for melanoma risk are…
sporadic dysplastic nevi
27
New cards
benign epithelial tumours (names)
* derived from the keratinising stratified squamous epithelium of the epidermis and hair follicles in the ductular epithelium of cutaneous glands
* often recapitulate the structures from which they arise
* may rarely be telltale signs of life threatening visceral tumours
1. seborrhoeic keratosis
2. acanthosis nigricans
3. fibroepithelial polyp
4. epithelial or follicular inclusion cyst (wen)
* often recapitulate the structures from which they arise
* may rarely be telltale signs of life threatening visceral tumours
1. seborrhoeic keratosis
2. acanthosis nigricans
3. fibroepithelial polyp
4. epithelial or follicular inclusion cyst (wen)
28
New cards
seborrhoeic keratosis
* common
* occur most frequently in middle ages or older people
* spontaneous, numerous on the trunk (other areas may be involved)
* round flat coin like waxy plaque, uniformly tan to dark brown, __velvety/granular surface__
* ==__small round pore like ostia impacted with keratin__== → not found in melanoma
* dermatosis pupulosa nigra → multiple small seborrhoeic keratoses on the face, present in up to 35% of african american adults
* many sporadic cases have activating FGFR3 mutations
* may suddenly appear in large numbers as part of a paraneoplastic syndrome (leser-trelat sign), might be due to stimulation of keratinocytes by TGF-alpha produced by tumour cells, __most commonly carcinomas of the GI tract__
* exophytic, sharply demarcated from the adjacent epidermis, composed of sheets of small cells that resemble basal cells
* characteristic → hyperkeratosis at the surface + small keratin filled cysts (horn cysts) and invaginations of keratin into the main mass (invagination cysts) ==__**INSERT PHOTO FIGURE 25.9**__==
* occur most frequently in middle ages or older people
* spontaneous, numerous on the trunk (other areas may be involved)
* round flat coin like waxy plaque, uniformly tan to dark brown, __velvety/granular surface__
* ==__small round pore like ostia impacted with keratin__== → not found in melanoma
* dermatosis pupulosa nigra → multiple small seborrhoeic keratoses on the face, present in up to 35% of african american adults
* many sporadic cases have activating FGFR3 mutations
* may suddenly appear in large numbers as part of a paraneoplastic syndrome (leser-trelat sign), might be due to stimulation of keratinocytes by TGF-alpha produced by tumour cells, __most commonly carcinomas of the GI tract__
* exophytic, sharply demarcated from the adjacent epidermis, composed of sheets of small cells that resemble basal cells
* characteristic → hyperkeratosis at the surface + small keratin filled cysts (horn cysts) and invaginations of keratin into the main mass (invagination cysts) ==__**INSERT PHOTO FIGURE 25.9**__==
29
New cards
acanthosis nigricans
* may be an important cutaneous sign of underlying benign and malignant conditions
* thickened, hyperpigmented skin, velvet like texture, mostly on flexural areas
* epidermis and underlying enlarged dermal papillae undulate sharply to form numerous repeating peaks and valleys
* variable hyperplasia, hyperkeratosis and slight basal cell layer hyperpigmentation (but no melanocytic hyperplasia)
* 2 types depending on the underlying condition
1. 80% → associated with benign conditions and develops gradually usually during childhood or puberty
* most commonly associated with obesity and DM (or other endocrine abnormalities)
* may occur as an autosomal dominant trait with variable penetrance
* as part of several rare congenital syndromes
2. 20% → associated with cancer, most commonly GI carcinoma
* in all types, there is a disturbance that leads to increased growth factor receptor signalling in the skin
* familial form → germline activating mutations in FGFR3 (same as in seborrhoeic keratosis)
* may be seen with skeletal deformities depending on the mutation
* hyperinsulinaemia (in type II DM) is thought to provoke IGFR-1 which activates the same signalling pathways for FGFR3
* some cases have high levels of TGF-alpha which may result in activation of EGFR
* thickened, hyperpigmented skin, velvet like texture, mostly on flexural areas
* epidermis and underlying enlarged dermal papillae undulate sharply to form numerous repeating peaks and valleys
* variable hyperplasia, hyperkeratosis and slight basal cell layer hyperpigmentation (but no melanocytic hyperplasia)
* 2 types depending on the underlying condition
1. 80% → associated with benign conditions and develops gradually usually during childhood or puberty
* most commonly associated with obesity and DM (or other endocrine abnormalities)
* may occur as an autosomal dominant trait with variable penetrance
* as part of several rare congenital syndromes
2. 20% → associated with cancer, most commonly GI carcinoma
* in all types, there is a disturbance that leads to increased growth factor receptor signalling in the skin
* familial form → germline activating mutations in FGFR3 (same as in seborrhoeic keratosis)
* may be seen with skeletal deformities depending on the mutation
* hyperinsulinaemia (in type II DM) is thought to provoke IGFR-1 which activates the same signalling pathways for FGFR3
* some cases have high levels of TGF-alpha which may result in activation of EGFR
30
New cards
fibroepithelial polyp
* one of the most common cutaneous lesions
* middle aged and older people, neck, trunk, face and intertriginous areas
* vast majority are sporadic, very rarely associated with birt hogg dube syndrome
* soft, flesh coloured bag like tumours, often attached to the surrounding skin by a slender stalk
* consist of fibrovascular cores covered by benign squamous epithelium
* polyps may undergo ischaemic necrosis due to torsion
* often become numerous during pregnancy
* usually inconsequential
* middle aged and older people, neck, trunk, face and intertriginous areas
* vast majority are sporadic, very rarely associated with birt hogg dube syndrome
* soft, flesh coloured bag like tumours, often attached to the surrounding skin by a slender stalk
* consist of fibrovascular cores covered by benign squamous epithelium
* polyps may undergo ischaemic necrosis due to torsion
* often become numerous during pregnancy
* usually inconsequential
31
New cards
epithelial or follicular inclusion cyst (wen)
* common lesions caused by invagination and cystic expansion of the epidermis or more commonly a hair follicle
* when large, they may undergo traumatic rupture → spills keratin into the dermis → extensive and often painful granulomatous inflammatory response
* when large, they may undergo traumatic rupture → spills keratin into the dermis → extensive and often painful granulomatous inflammatory response
32
New cards
adnexal (appendage) tumours
* some are benign and may be confused with cutaneous cancers such as basal cell carcinoma
others are associated with germline mutations in tumour suppressor genes
* malignant forms are more common than benign
* nondescript flesh coloured solitary or multiple papules and nodules
1. eccrine poroma → predominantly on the palms and soles where sweat glands are numerous
2. cylindroma → ductal (apocrine or eccrine) differentiation, usually forehead or scalp, nodules may coalesce. may be dominantly inherited (associated with inactivation of the tumour suppressor CYLD which encomes an enzyme that negatively regulates NF-kB)
mutations of CYLD are associated with 2 other genetic syndromes marked by the occurrence of multiple adnexal tumours
→ islands of cells resembling the normal epidermal or adnexal basal cell layer (basaloid cells)
3. syringoma → eccrine differentiation, multiple small tan papules around the lower eyelids
4. sebaceous adenoma → can be associated with internal malignancy in Muir Torre syndrome and a subset of lynch syndrome = germline defects in DNA mismatch repair genes
5. pilomatricoma → shows hair follicle differentiation, activating mutations in CTNNB1 (encodes beta catenin which WNT signalling occurs through)
6. adnexal tumours can also show apocrine differentiation
\
==__**histology???????**__==
others are associated with germline mutations in tumour suppressor genes
* malignant forms are more common than benign
* nondescript flesh coloured solitary or multiple papules and nodules
1. eccrine poroma → predominantly on the palms and soles where sweat glands are numerous
2. cylindroma → ductal (apocrine or eccrine) differentiation, usually forehead or scalp, nodules may coalesce. may be dominantly inherited (associated with inactivation of the tumour suppressor CYLD which encomes an enzyme that negatively regulates NF-kB)
mutations of CYLD are associated with 2 other genetic syndromes marked by the occurrence of multiple adnexal tumours
→ islands of cells resembling the normal epidermal or adnexal basal cell layer (basaloid cells)
3. syringoma → eccrine differentiation, multiple small tan papules around the lower eyelids
4. sebaceous adenoma → can be associated with internal malignancy in Muir Torre syndrome and a subset of lynch syndrome = germline defects in DNA mismatch repair genes
5. pilomatricoma → shows hair follicle differentiation, activating mutations in CTNNB1 (encodes beta catenin which WNT signalling occurs through)
6. adnexal tumours can also show apocrine differentiation
\
==__**histology???????**__==
33
New cards
WNT signalling through beta catenin is essential for…
early hair development, regulates hair growth and maintenance
34
New cards
premalignant and malignant epidermal tumours (names)
1. actinic keratosis
2. squamous cell carcinoma
3. basal cell carcinoma
35
New cards
actinic keratosis
* occurs on sun damaged skin and exhibits hyperkeratosis
* precursors to squamous cell carcinoma
* high incidence of TP53 mutations
* tan brown, red or skin coloured, rough, some lesions produce so much keratin that a cutaneous horn develops
* lips may also develop similar lesions → actinic cheilitis
* hyperplasia of basal cells or atrophy that results in thinning of the epidermis
* dyskeratosis of basal cells → pink or reddish cytoplasm
* ==__in contrast to basal cell carcinoma__==, intercellular bridges are present
* elastosis of the superficial dermis
* __thickened stratum corneum and they retain their nucleus (parakeratosis)__
* topical imiquimod (activates TLRs) eradicates up to 50% of lesions
* freezing (?) may also work
* precursors to squamous cell carcinoma
* high incidence of TP53 mutations
* tan brown, red or skin coloured, rough, some lesions produce so much keratin that a cutaneous horn develops
* lips may also develop similar lesions → actinic cheilitis
* hyperplasia of basal cells or atrophy that results in thinning of the epidermis
* dyskeratosis of basal cells → pink or reddish cytoplasm
* ==__in contrast to basal cell carcinoma__==, intercellular bridges are present
* elastosis of the superficial dermis
* __thickened stratum corneum and they retain their nucleus (parakeratosis)__
* topical imiquimod (activates TLRs) eradicates up to 50% of lesions
* freezing (?) may also work
36
New cards
squamous cell carcinoma
* second most common tumour on sun exposed sites (most common = basal cell carcinoma)
* higher incidence in men than women except for lesions on the lower legs
* metastasis = <5%, lesions are deeply invasive and involve the subcutis
* most important cause = DNA damage caused by UV (tumour incidence is proportional to lifetime sun exposure)
2nd most common association = immunosuppression (esp. if chronic eg. due to chemotherapy or organ transplantation)
* immunosuppression may contribute to carcinogenesis by reducing host surveillance and increasing susceptibility of keratinocytes to infection and transformation by viruses, esp. HPV 5 and 8
* UV damages DNA but also causes a transient defect in cutaneous innate immunity
* there are other risk factors
* precursors may be actinic keratosis or xeroderma pigmentosum
actinic → TP53 (added mutations of RAS are common to cause scc)
xeroderma → inherited mutations in genes in the nucleotide excision repair pathway
* if not invasive → sharply defined, red scaling plaques
if invasive → nodular, show variable keratin production and may uclerate
* higher incidence in men than women except for lesions on the lower legs
* metastasis = <5%, lesions are deeply invasive and involve the subcutis
* most important cause = DNA damage caused by UV (tumour incidence is proportional to lifetime sun exposure)
2nd most common association = immunosuppression (esp. if chronic eg. due to chemotherapy or organ transplantation)
* immunosuppression may contribute to carcinogenesis by reducing host surveillance and increasing susceptibility of keratinocytes to infection and transformation by viruses, esp. HPV 5 and 8
* UV damages DNA but also causes a transient defect in cutaneous innate immunity
* there are other risk factors
* precursors may be actinic keratosis or xeroderma pigmentosum
actinic → TP53 (added mutations of RAS are common to cause scc)
xeroderma → inherited mutations in genes in the nucleotide excision repair pathway
* if not invasive → sharply defined, red scaling plaques
if invasive → nodular, show variable keratin production and may uclerate
37
New cards
UV damages DNA and…
causes a transient defect in cutaneous innate immunity
38
New cards
DNA damage caused by sunlight is sensed by…
ATM and ATR → cause upregulation of p53 → arrests the G phase → repair or elimination of cells
39
New cards
basal cell carcinoma
* locally aggressive cutaneous tumour
* associated with mutations that activate the Hedgehog signalling pathway
* most common invasive cancer in humans
* slow growing, rarely metastasises, most are recognised at an early stage and excised, <0.5% are locally aggressive and potentially disfiguring
* occurs at sun exposed sites in slightly pigmented elderly
* incidence is increased in immunosuppression and disorders of DNA repairs such as xeroderma pigmentosum (as with SCC)
* present as pearly papules with telangiectasias, some tumours contain melanin and superficially resemble melanocytic nevi or melanomas
* advanced tumours may ulcerate
* superficial basal cell carcinoma (a variant) present as erythematous occasionally pigmented plaques that may resemble early forms of melanoma
* tumours cells resemble those in the normal basal cell layer
* 2 patterns are seen
1. multifocal growths: originate from the epidermis
2. nodular lesions: grow into the dermis, have basophilic cells with hyperchromatic nuclei embedded in a mucinous matrix often surrounded by fibroblasts and lymphocytes
* ==__**palisading?**__==
\
NBCCS = nevoid basal cell carcinoma syndrome
* autosomal dominant
* characterised by the development of multiple basal cell carcinomas often before 20, accompanied by various other tumours
* germline loss of function of one allele of PTCH, the other allele is inactivated in tumours by an acquired mutation usually caused by exposure to mutagens (esp. UV)
1/3 consist of C→T transitions = hallmarks of UV damage
* associated with mutations that activate the Hedgehog signalling pathway
* most common invasive cancer in humans
* slow growing, rarely metastasises, most are recognised at an early stage and excised, <0.5% are locally aggressive and potentially disfiguring
* occurs at sun exposed sites in slightly pigmented elderly
* incidence is increased in immunosuppression and disorders of DNA repairs such as xeroderma pigmentosum (as with SCC)
* present as pearly papules with telangiectasias, some tumours contain melanin and superficially resemble melanocytic nevi or melanomas
* advanced tumours may ulcerate
* superficial basal cell carcinoma (a variant) present as erythematous occasionally pigmented plaques that may resemble early forms of melanoma
* tumours cells resemble those in the normal basal cell layer
* 2 patterns are seen
1. multifocal growths: originate from the epidermis
2. nodular lesions: grow into the dermis, have basophilic cells with hyperchromatic nuclei embedded in a mucinous matrix often surrounded by fibroblasts and lymphocytes
* ==__**palisading?**__==
\
NBCCS = nevoid basal cell carcinoma syndrome
* autosomal dominant
* characterised by the development of multiple basal cell carcinomas often before 20, accompanied by various other tumours
* germline loss of function of one allele of PTCH, the other allele is inactivated in tumours by an acquired mutation usually caused by exposure to mutagens (esp. UV)
1/3 consist of C→T transitions = hallmarks of UV damage
40
New cards
PTCH protein
* a receptor for sonic hedgehog (SHH, a component of the hedgehog signalling pathway) which controls polarity and CNS development during embryogenesis, also regulates hair follicle formation and hair growth
* when ‘off’ it is in a complex with another transmembrane protein called SMO, when SHH binds to PTCH, SMO is released which in turn activates the transcription factor GLI1 → expression of genes that support tumour cell growth and survival
* when ‘off’ it is in a complex with another transmembrane protein called SMO, when SHH binds to PTCH, SMO is released which in turn activates the transcription factor GLI1 → expression of genes that support tumour cell growth and survival
41
New cards
tumours of the dermis (names)
1. benign fibrous histiocytoma (dermatofibroma)
2. dermatofibrosarcoma protuberans
42
New cards
benign fibrous histiocytoma (dermatofibroma)
* = a heterogenous family of benign dermal neoplasms of uncertain lineage
* most common form = dermatofibroma → benign spindle shaped cells, may extend into the subcutaneous fat
there may also be overlying epidermal hyperplasia characterised by downward elongation of hyperpigmented rete ridges (pseudoepitheliomatous hyperplasia)
* usually seen in adults, often occur on the legs of young and middle aged women
* lesions are asymptomatic and tender and may increase and decrease slightly in size over time
* fusion genes including those of the tyrosine kinase ALK have been identified
* seem to be composed at least partially of dermal dendritic cells
* firm, tan brown papules
* most common form = dermatofibroma → benign spindle shaped cells, may extend into the subcutaneous fat
there may also be overlying epidermal hyperplasia characterised by downward elongation of hyperpigmented rete ridges (pseudoepitheliomatous hyperplasia)
* usually seen in adults, often occur on the legs of young and middle aged women
* lesions are asymptomatic and tender and may increase and decrease slightly in size over time
* fusion genes including those of the tyrosine kinase ALK have been identified
* seem to be composed at least partially of dermal dendritic cells
* firm, tan brown papules
43
New cards
dermatofibrosarcoma protuberans
* well differentiated primary fibrosarcoma of the skin
* slow growing, locally aggressive, can recur but rarely metastasise
* protuberant nodules often on the trunk within a firm plaque that may sometimes ulcerate
* closely packed fibroblasts arranged radially → storiform
* the overlying epidermis is generally thinned unlike dermatofibroma
* frequently seen → extension into the subcutaneous fat and forming a characteristic honeycomb pattern
* may extend down to the subcutis
* translocation involving the genes encoding collagen 1A1 and platelet derived growth factor beta → overexpression and secretion of PDGFB → tumour cell growth through an autocrine loop
* usually treated with wide local excision, if not → PDGFB inhibitors
withdrawal of inhibitors leads to regrowth so it must be lifelong
* slow growing, locally aggressive, can recur but rarely metastasise
* protuberant nodules often on the trunk within a firm plaque that may sometimes ulcerate
* closely packed fibroblasts arranged radially → storiform
* the overlying epidermis is generally thinned unlike dermatofibroma
* frequently seen → extension into the subcutaneous fat and forming a characteristic honeycomb pattern
* may extend down to the subcutis
* translocation involving the genes encoding collagen 1A1 and platelet derived growth factor beta → overexpression and secretion of PDGFB → tumour cell growth through an autocrine loop
* usually treated with wide local excision, if not → PDGFB inhibitors
withdrawal of inhibitors leads to regrowth so it must be lifelong
44
New cards
dermal papillae
fingerlike projections of the dermis that may contain blood capillaries or Meissner corpuscles (of touch) \n Irrefukar connection between the epidermis ans dermis → interdigitatw with epidermal ridges → dermatoglyphs → finger and foot prints
45
New cards
epidermal layers (superficial to deep)
1. stratum corneum
2. stratum lucidum
3. stratum granulosum
4. stratum spinosum
5. stratum basale
46
New cards
stratum corneum
* outermost layer, 20-30 layers
* squamous keratinised cells
* glycolipids act as cement
* dead keratinocytes → release defensins
* the layer that is shed
* squamous keratinised cells
* glycolipids act as cement
* dead keratinocytes → release defensins
* the layer that is shed
47
New cards
stratum lucidum
* only found in thick skin (2-3 layers)
* clear layer of eosinophilickeratinisedcells
* no nuclei or organelles → ==dead==
* cytoplasm contains packed keratin filaments
* clear layer of eosinophilickeratinisedcells
* no nuclei or organelles → ==dead==
* cytoplasm contains packed keratin filaments
48
New cards
what do keratinocytes produce
* keratin
* glycolipids
* cytokines
* cholesterol precursors which change UVB to vitamin D
* glycolipids
* cytokines
* cholesterol precursors which change UVB to vitamin D
49
New cards
keratohyaline granules
keratin precursor proteins + pro filaggrin and other proteins \n They aggregate and cross link → bundles of keratin
50
New cards
why do keratinocytes flatten out
inner organelles disintegrate
51
New cards
stratum granulosm
* flattened cells, 3-5 layers
* cells undergoing terminal differentiation of keratinisation → cells flatten out and die + keratohyaline granules → basophilic layer
* lamellar granules → lipids + glycolipids → exocytosed when the cell dies → lipid rich layer → impermeable to H2O
* transition between the metabolically active strata and the dead cells of the more superficial strata
* cells undergoing terminal differentiation of keratinisation → cells flatten out and die + keratohyaline granules → basophilic layer
* lamellar granules → lipids + glycolipids → exocytosed when the cell dies → lipid rich layer → impermeable to H2O
* transition between the metabolically active strata and the dead cells of the more superficial strata
52
New cards
stratum germivatum
cells that are still dividing from the basal layer
53
New cards
stratum spinosum
* thickest layer (3-10)
* has the stratum germinavitum
* contains langerhan cells and DCs
* keratin filaments assemble to form tonofibrils → converge → terminate at desmosomes
* have spines (cells extending around tonofibrils to anchor themselves)
* cytoplasm is actively synthesising keratin types
* has the stratum germinavitum
* contains langerhan cells and DCs
* keratin filaments assemble to form tonofibrils → converge → terminate at desmosomes
* have spines (cells extending around tonofibrils to anchor themselves)
* cytoplasm is actively synthesising keratin types
54
New cards
stratum basale
* singe cell layer → cuboidal or columnar
* intense mitotic activity of stem cells → produce new keratinocytes
* connected to basement membrane through hemidesmosomes and anchoring fibers
* also contains melanocytes
* intense mitotic activity of stem cells → produce new keratinocytes
* connected to basement membrane through hemidesmosomes and anchoring fibers
* also contains melanocytes
55
New cards
from what cell layer are keratinocytes dead
lucidum
56
New cards
keratin formation
* starts in the stratum granulosum
* tonofibrils cross link with filaggrin
* keratohyaline granules and lysozomes break down cellular components into keratin
* tonofibrils cross link with filaggrin
* keratohyaline granules and lysozomes break down cellular components into keratin
57
New cards
squames
dead flattened skin cells that are normally shed from the epidermis as new skin cells emerge. Squames can be laden with potentially pathogenic bacteria
58
New cards
melanocytes
* stratum basale
* processes that extend into spinous layer
* 1 melanocyte for 5 keratinocytes
* not attached to neighbouring keratinocytes
* contain mitochondria, RER and golgi
* processes that extend into spinous layer
* 1 melanocyte for 5 keratinocytes
* not attached to neighbouring keratinocytes
* contain mitochondria, RER and golgi
59
New cards
how can you differentiate between langerhans and melanocytes
langerhans are located more superficially (spinosum)
60
New cards
melanin formation
1. tyrosinase synthesis in RER → converts tyrosine into dopa → transformed + polymerised into different forms of melanin
2. go to Golgi → melanin deposited into parallel filaments in the matrix → accumulates into vesicles
3. melanin accumulates
4. melanosome
Melanosome moves through processes into keratinocytes using dynein → shade DNA from UV
61
New cards
dermis layer
1. papillary layer:
* fibroblasts → collagen I and II → arranged in papillae → contain blood vessels and nerve endings (contain meissner corpuscles and free nerve endings)
* macrophages
* type IV anchoring fibrils attach it to the epidermis
2. reticular layer:
* thicker
* fibroblasts → tighter collagen + elastin
* macrophages
* oil and sweat glands, hair follicles, nerves (pacinian corpuscle etc), blood and lymphatic vessels
* regulates temperature
62
New cards
what type of innervation does the dermis have
sympathetic only
63
New cards
types of sensory receptors
1. Unencapsulated:
* tactile receptors/merkel cells → tonic, sustained light touch + texture
* free nerve endings → high/low temp, pain and itch
* root hair plexus
2. Encapsulated:
* meissner corpuscle → light touch or low frequency stimuli when temporarily deformed
* lamellated (pacinian) corpuscles → coarse touch, pressure and vibrations
* krause end bulbs
* ruffini corpuscles → stretch or twisting
64
New cards
types of skin glands
1. sebaceous glands:
* usually part of pilosebacous unit → sebum
* open directly into the epidermal surface if no hair
* branched acinar glands
* holocrins secretion
2. eccrine sweat glands:
* cholinergic fibers
* thermoregulatory
* mostly on foot soles
* have 3 types of cells in the secreting portion
* have 2 types of cells in ducts
3. apocrine sweat glands:
* adrenergic fibers
* more protein rich sweat
* merocrine secretion
* larger lumens than ^
* open into hair follicles
65
New cards
types of cells in the secreting portion of eccrine sweat glands
1. Myoepithelial cells
2. Dark cells
3. Columnar/cuboidal cells
66
New cards
function of sebum
collects dirt; softens and lubricates hair and skin \n weak antimicrobial properties + maintains stratum corneum
67
New cards
skin repair
1. blood vessels broken
2. blood clots
3. vasoconstriction
4. scab and inflammation - erythema, heat, edema, and pain
5. granulation tissue - made of fibroblasts and new capillaries form in the new area
6. scab is sloughed
68
New cards
immunotherapy chapter\*\*\*\*\*\*\*\*\*\*