Surgical Approaches (McIntyre)
1/64
Earn XP
Description and Tags
McIntyre
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
The patient is a 30 year old White male , who is a consultation from Thomas J. Lee MD for evaluation of infertility. The patient has been married for 4 years to a 32 year old female, Jess. Her doctor is Dr Lau. The patient has been trying unsuccessfully for a pregnancy for one year. She has not had children in the past. She has regular cycles. She has not yet had an HSG. She is not on meds for fertility. He has fathered no other children. He has not had testicular trauma. He has not been diagnosed with a varicocele in the past. He denies a history of undescended testicles, chemical exposures, radiation, post pubertal mumps, and chemotherapy. He has had no previous semen analysis. He has not had a hormone profile checked.
The couple has tried timed intercourse. They have intercourse intermittently around the time of ovulation. They do not use lubricants.
Testes : normal testes, vas deferens normal, Bilateral Grade I varicocele
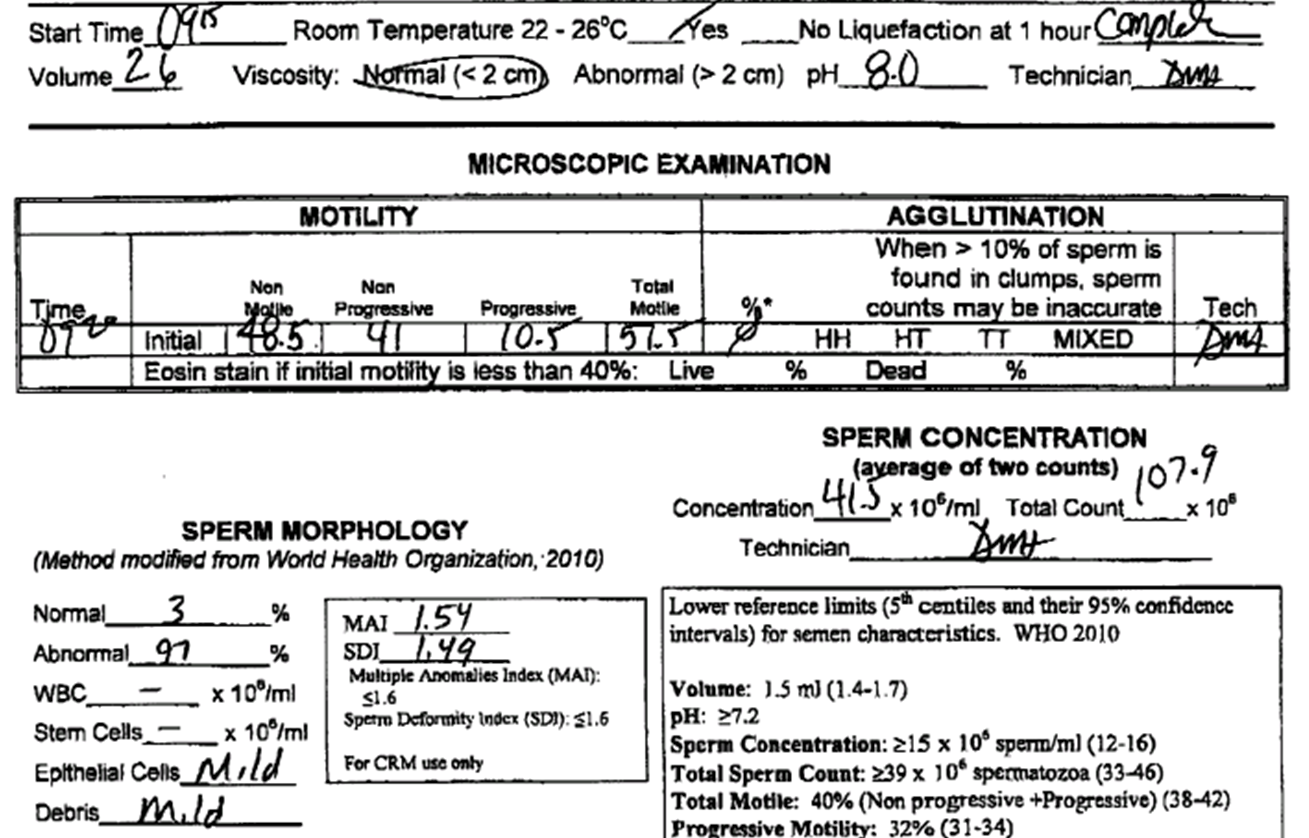
Varicocele
Progressive motility low
Post varicocelectomy: increased semen parameters
Incidence of varicocele in general population
20%
Incidence of varicocele in infertility space
40%
Most common surgically correctable cause for a male infertility
Varicocele
Different grades of varicocele
Grade 1 only palpable with Valsalva
Grade 2 palpable without Valsalva but gets bigger with
Grade 3 seen through skin
Layers of scrotum and spermatic cord
Skin, dartos, external spermatic fascia, cremaster, internal spermatic fascia, tunica vaginalis
To fix hydrocele, you have to remove the
tunica vaginalis
Contents of inguinal canal
Testicular artery, genital branch of genitofemoral nerve, and vas deferens
(also testicular vein and lymphatics)
Stay cephalad of the inguinal ligament because of ?
femoral artery and vein is close under
Theories of causes of varicoceles
Refluxing renal metabolites
Hormonal dysfunction
Hypoxia and ROS
Hyperthermia
Indications for varicocelectomy
Impaired semen quality
Testicular pain
Prevention of testicular atrophy in adolescents or if atrophy is present in adults
Techniques for varicocelectomy
Laparoscopic
Retroperitoneal
Inguinal
Subinguinal
Endovascular embolization
Postoperative care for varicocelectomy and post op follow up
Avoid strenous activity for 4 weeks
Standard wound care
Semen analysis around 12 weeks
Varicocelectomy improves _____ parameters which may improve changes of natural conception or help efforts of assisted reproduction
semen
form of surgical sterilization by which the vas deferens is divided or damaged to the point it will no longer transport sperm
Vasectomy
Vasovasostomy
Vasectomy reversal
Vasoepididymostomy
bypass epididymal obstruction
Presence of epididymal obstruction requires a
Vasoepididymostomy
Greatest predictor of epidymal obstruction is time since
Vasectomy
less than 3 years 97% will have successful vasovasostomy
greater than 3 years see specialist
Sperm can be preserved during vasectomy reversal for use in
IVF
Clear fluid with mostly normal motile sperm
Grade 1
Clear fluid with mostly normal non-motile sperm
Grade 2
Cloudier fluid with mostly sperm heads
Grade 3
cloudier with only sperm heads
Grade 4
paste like with no sperm
Grade 5
(epididymal obstruction)
Fluid grade 1-3 has good outcomes using
Vasovasostomy
Grade 4 and 5 patients would benefit from
Vasoepididymostomy
Cutting tunica vaginalis exposes
epididymis
Post operative care for vasoepididymostomy
Scrotal support
Abstinence from intercourse
Restricted to light duty activities
first semen analysis at 6 weeks and regular intervals after
May takes months for sperm to return
_______ only ciliated portion of male reproductive tract
Efferent ducts
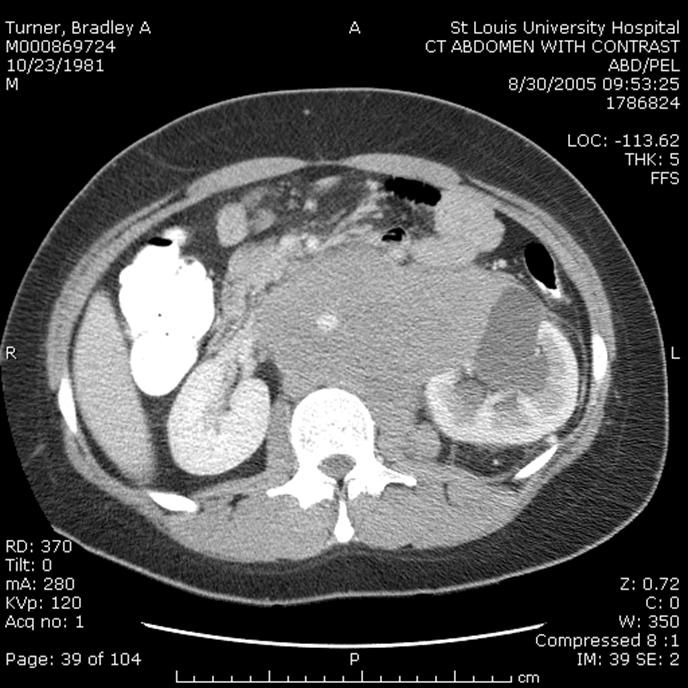
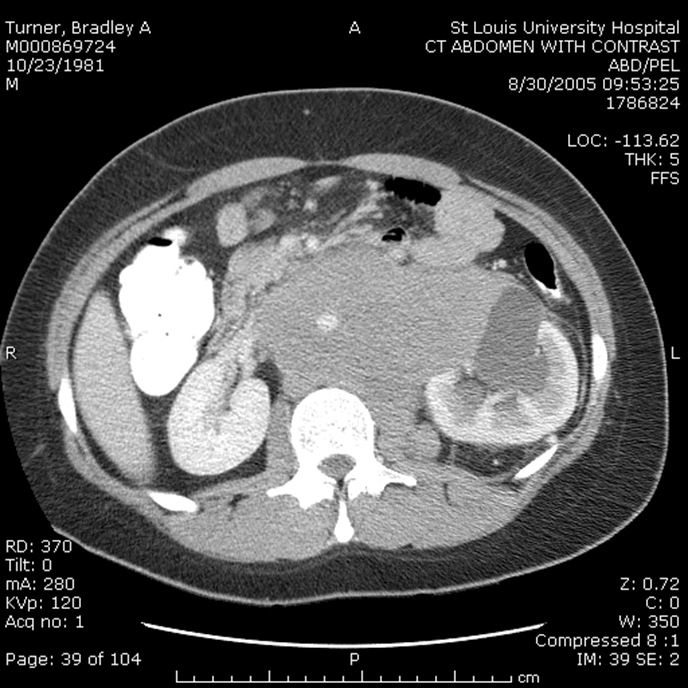
The patient is a 26 year old Caucasian/White male, who is a consultation from Dr. K for evaluation of infertility and azoospermia The patient has been married for 6 years to a 25 year old female, Dot. Her doctor is Dr. K . The patient has been trying unsuccessfully for a pregnancy for several years. She has not had children in the past. She has regular cycles. She has had a HSG which was normal. She is not on meds for fertility.
He has fathered no other children. He has not had testicular trauma. He has not been diagnosed with a varicocele in the past. Mr. Smithson denies a history of undescended testicles, chemical exposures, radiation, post pubertal mumps, and chemotherapy. He has had previous semen analysis. The results of the semen analysis were 0.3 Azoo x2.
The couple has tried timed intercourse. They have intercourse intermittently around the time of ovulation. They do not use lubricants.
Scrotum : I can not palpate either vas adequately to be convinced that they are present
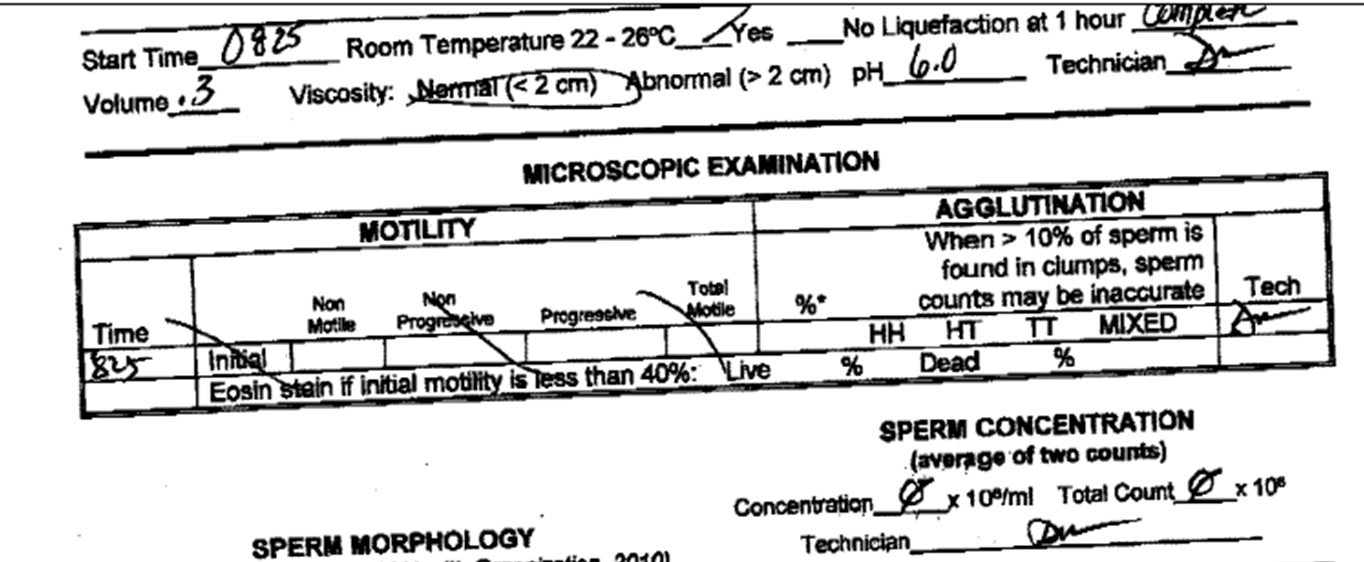
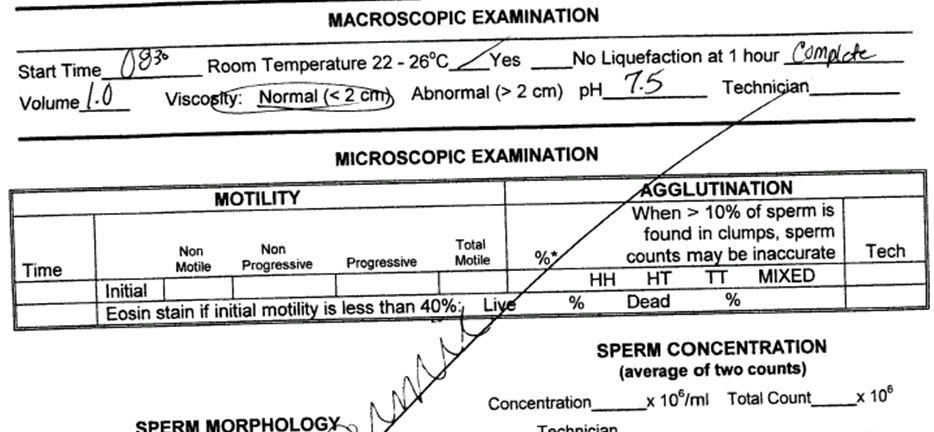
Look at volume and pH
CF
Seminal vesicles are also atretic in
CF
Bulbourethral glands <_%
Prostate ___-___%
Seminal vesicles ___-____%
Vas deferens/epididymis ___-___%
5
20-30
60-70
6-10
1.5 cc LLN and 7-8 ULN
For volume of ejaculate
Patients with CBAVD have _______ azoospermia
obstructive
Sperm retrieval in OA
percutaneous approach (need 8-10 good sperm) of epididymis
Biopsy gun from testicle
FNA of testicle
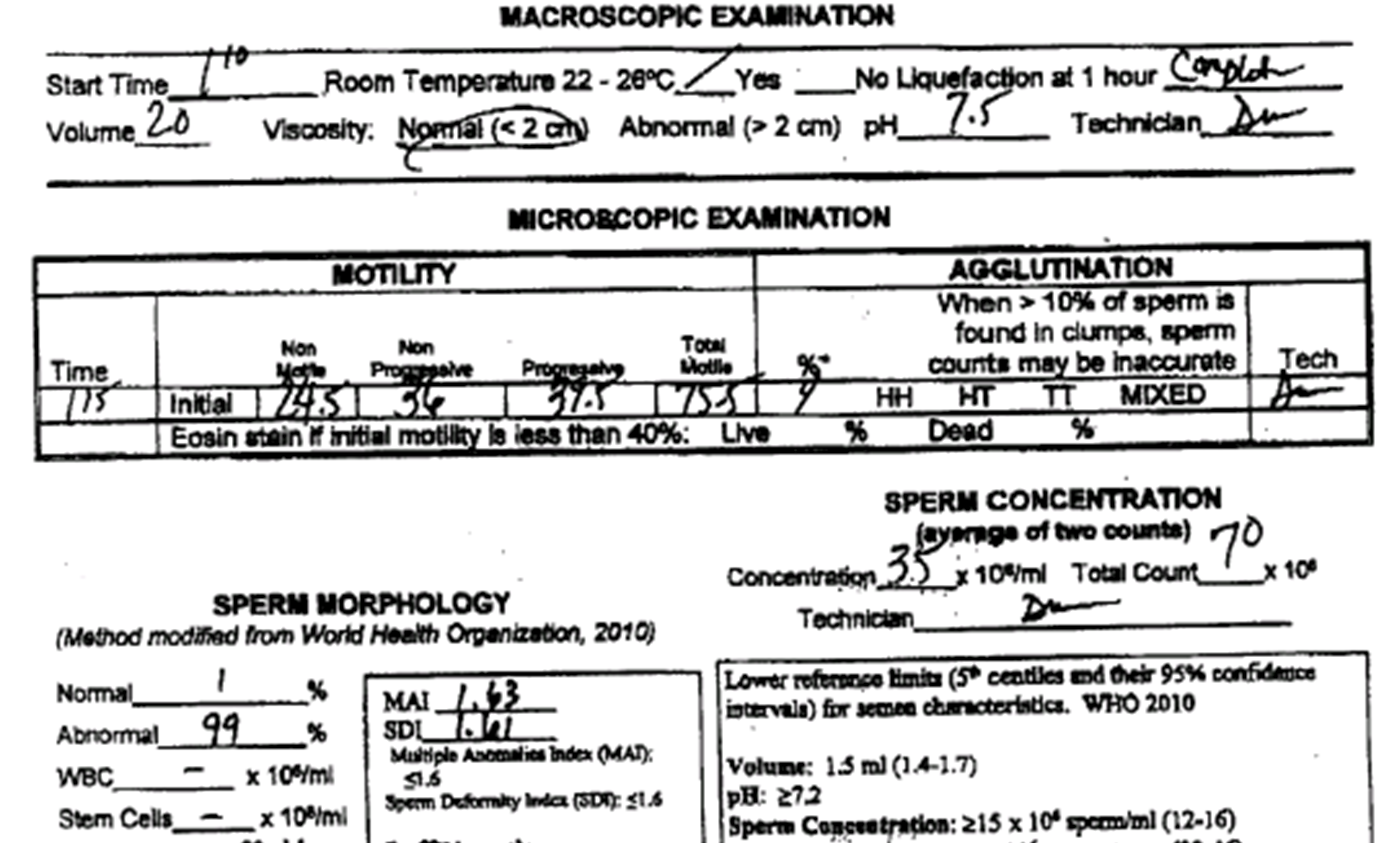
The patient is a 36 year old African American/Black male, who is a consultation from Thomas Meyrs for evaluation of infertility. The patient has been married for 6 years. To a 34 year old female, Sally. Her doctor is Dr Ringler. The patient has been trying unsuccessfully for a pregnancy for one year. She has not had children in the past. She has regular cycles. She has had a HSG which was normal. She is not on meds for fertility. He has fathered no other children. He has not had testicular trauma. He has not been diagnosed with a varicocele in the past. Mr. Mathers denies a history of chemical exposures, radiation, and post pubertal mumps. He has had no previous semen analysis. He has not had a hormone profile checked.
The couple has tried timed intercourse. They have intercourse intermittently around the time of ovulation. They do not use Lubricants
He does have a history of Lupus and has received cytoxan for some time in the past. Currently he is on prednisone for treatment.
Testosterone 504 ng/ml (above 350 good)
LH 14 (1.5-9.3)
FSH 40 (1.6-8)
Azoospermia
Cytoxan- chemotherapy wiped out primordial germ cells
Testicular failure/ primary hypogonadism (no inhibin)
Men of reproductive age should not have an FSH over
7.5
Treatment for non-obstructive azoospermia
Micro Testicular sperm extraction and in vitro fertilization
Micro Tese (look for more opaque tubules)
Pt is a 25 yr old male present after pulling groin 2 weeks ago playing kickball.
Noted a knot come up and thinks it is getting bigger
Never had this before was not red or tender, is getting in the way when sitting

What type of cancer does he have?
LD 953 (80-210)
Beta HCG 11.1 (less than 1)
AFP 1.1 (less than 15)
Choriocarcinoma
Work Up of Testicular Mass
•History and Physical Exam
•Labs*
–bHCG
–LDH
–AFP
•Radical Orchiectomy
•Ct Scan
______ incision makes it radical orchectomy instead of simple
Inguinal
bulk tumor marker, how much is there
Lactate dehydrogenase
Check after to removal to see if there is anything left. After 4 half life’s
AFP 7 days longest so check 4 weeks after removal.
In pure seminoma only ___ will be elevated
LDH
What is the most common GCT ?
Mixed
Most common pure tumor is?
Seminoma
Yolk sac tumor
AFP
Choriocarcinoma
βHCG
Seminoma with mets to retroperitoneum
Chemo/ radiation
NSGCT with mets to retroperitoneum
Surgery/ Chemo
Right sided landing zone nodes
Paracaval
Interaortocaval
Preaortic
Left sided landing zone nodes
Interaortocaval
Preaortic
Paraortic
Sympathetic
Ejaculation
Preganglionic neurons innervate the epididymis, vas deferens, seminal vesicles, prostate, and penis
Intermediolateral nucleus at the T12-L2 level
Preganglionic fibers travel through the sympathetic chain
Exit through lumbar splanchnic nerves
Synapses in the inferior mesenteric ganglion
Pass through hypogastric plexus
Parasympathetic
Erection
Preganglionic neurons innervate the corpora cavernosa
IML at the S2-S4 level.
Exit through pelvic nerves
Pass through the hypogastric plexus
Internal pudendal artery ends in the ____
penis as dorsal nerve of the penis
Nerve that causes ______ runs on top of the prostate
erection
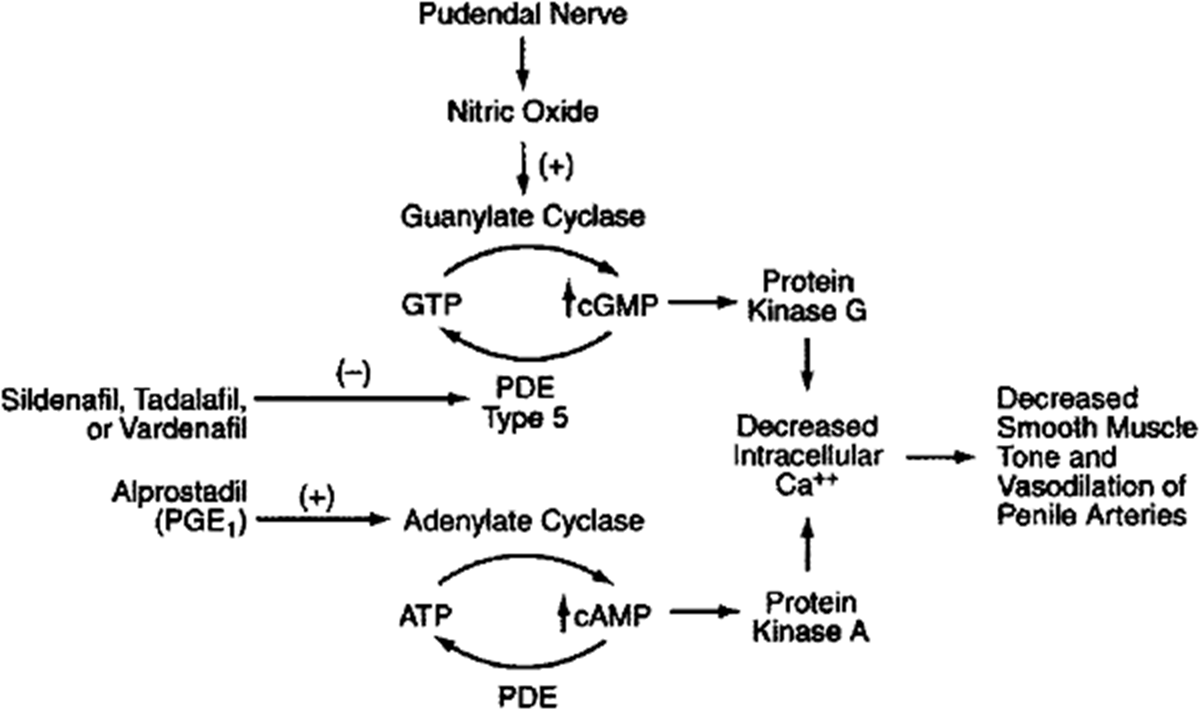
NO stimulates smooth muscle guanylate cyclase, upregulating synthesis of ____
cGMP
____ hydrolyzes cGMP to 5'-GMP
PDE5
ED can be treated by inhibiting ____
PDE5
Main physical causes of ED
Vascular
Diabetes
Medication
(heart disease, smoking, long term HTN)
Pelvic surgery, radiation, trauma (prosectomy)
Sildenafil was first approved from
primary pulmonary HTN
Half life of ____ is longer can take it daily 5 mg (get aroused for it) or on demand
cialis
Self-injections for ED
If you are failing oral medication including dual therapy but do not want to do the vacuum device
Daily Cialis + on demand Viagra or Levitra for dual therapy
Injection main ingredient is alprostadil which is a
PGE1 agonist