AP Psychology Final
1/955
Earn XP
Description and Tags
This took me about 4 days to make bruh. Pulled 2 all nighters just to do this. Good Luck on AP Exams. Wishing for a 5. We are in this together!
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
956 Terms
Schizophrenia
The most profound and devastating of all mental disorders, and it is the most prevalent disorder among all psychoses. Severe mental disorder characterized by disturbances in thought processes, perceptions, emotional regulation, and behavior. Common symptoms include hallucinations (hearing or seeing things that aren’t there), delusions (false beliefs), disorganized speech or thinking, and difficulty with motivation and daily functioning.
Psychosis
Refers to any disorder in which the affected person has lost contact with reality.
Positive symptoms
The presence of abnormal behaviors or experiences that are added to a person’s normal functioning. (Addition)
Negative symptoms
Refer to those with a marked decrease of normal functions. (Reduction)
Diminished emotional expression
A negative symptom of schizophrenia, where a person shows less facial expression, gestures, or vocal tone. It means the individual may appear less emotionally responsive or may not express feelings as strongly as others. This can make it harder for others to interpret the person's emotions and create difficulties in social interactions.
Delusions
The persistence of false beliefs, usually held by affected individuals as ideas about themselves in relation to the world around them.
Hallucinations
Sensory experiences that occur without any external sensory stimuli, meaning the individual is experiencing something that actually isn’t there. They are involuntary and cannot be controlled by the individual but are experienced as real as any other normal sensory perception.
Flat affect
Refers to a severe reduction in emotional expression. Individuals with flat affect show little or no facial expression, tone of voice, or gestures, even in situations that would typically provoke strong emotions.
Schizoaffective disorder
Is essentially schizophrenia plus periodic symptoms of disordered affect or mood. An individual diagnosed with this disorder will not only display two or more of the five psychosis- related symptoms described above but will also present a major mood episode of either pervasive depression or mania.
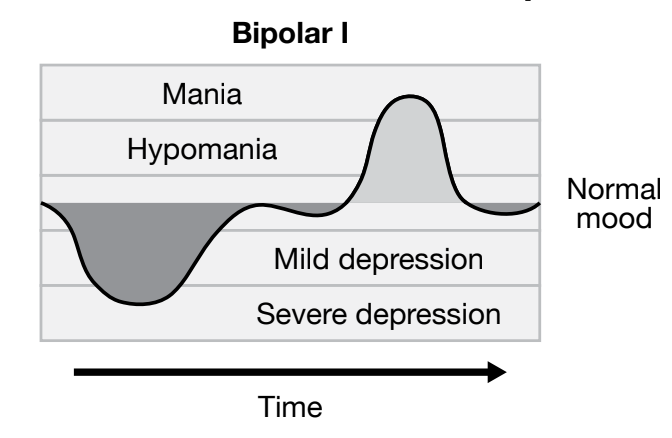
Bipolar I
Is a mood (or affective) disorder in which an individual had experienced at least one manic episode (mania) as well as episodes of major depression.
Major depression
A mental health condition characterized by persistent feelings of sadness, hopelessness, and a lack of interest or pleasure in activities that were once enjoyable.
Mania
A state of abnormally elevated mood and intensely high energy that disrupts daily life.
Manic episode
A period of abnormally high mood and energy; often characterized as either excessively euphoric, like “feeling on top of the world,” or extremely irritable and dysphoric, experiencing profound unease. People may also experience feelings of grandiosity and begin many projects that are often beyond their skills or talents. They may also require significantly less sleep.
Flight of ideas
People with bipolar I may display this in speech because their thoughts may race faster than they can express coherently.
Hypomania
An individual with bipolar I may also this, a condition that is similar to mania but less severe. It is characterized by a pattern of episodes alternating between hypomania and major depression.
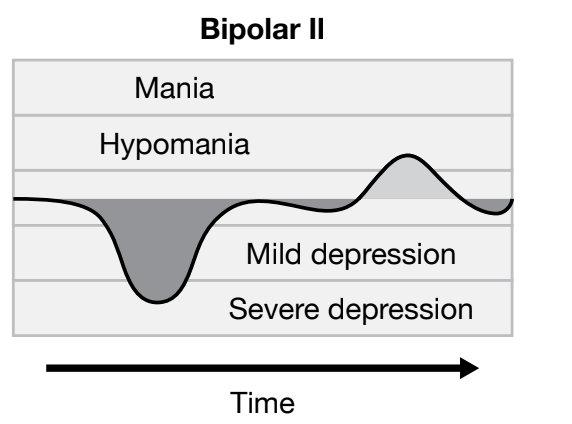
Bipolar II
An individual would have experienced a hypomanic episode but never a manic one.
Cyclothymic disorder
A mood disorder that involves elevated moods similar to hypomania but not as severe. The depressive episodes in this disorder are also not as severe. Chronic, quick-cycling mood changes that are less severe than bipolar disorder
Depressive disorders
Significant feelings of sadness, emptiness, or irritability that are accompanied by somatic and cognitive disruptions that significantly affect daily function. There are 8 types; The three most common disorders are disruptive mood dysregulation disorder, major depressive disorder, and persistent depressive disorder.
Disruptive mood dysregulation disorder (DMDD)
A childhood psychological condition characterized by extreme irritability, anger, and intense and sometimes frequent temper outbursts.
Major depressive disorder
Also known as unipolar depression, involves severe symptoms such as fatigue, sustained depressed mood, diminished interest or pleasure in activities, decreased appetite, weight loss, sleep disturbances, feelings of worthlessness, guilt, diminished ability to concentrate, and persistent thoughts of death or suicide. Combination of symptoms that interfere with the ability to work, study, sleep, eat, and enjoy once pleasurable activities.
Persistent depressive disorder
A depressed mood that has lasted for at least two years. It is considered a milder form of depression with no suicidal thoughts. Someone with this disorder may experience two or more of the characteristic symptoms: poor appetite or overeating, sleep disturbances, fatigue, low self-esteem, poor concentration, feelings of hopelessness, and a lack of interest in activities they had previously found interesting. (dysthymia)
Personality disorder
People with personality issues that are so problematic, abnormal, and enduring that they lead to distress or impaired interactions with others suffer from this disorder. Characterized by enduring patterns of internal experiences & behavior that are deviant from one’s culture; pervasive & inflexible; begin in adolescence/early adulthood; stable over time and lead to personal distress or discomfort.
Cluster A
“Odd, Suspicious, and Eccentric” disorders include disorders that show patterns of paranoia, social isolation, cognitive or perceptual distortions, and eccentric behaviors.
Paranoid personality disorder
It is a pattern of distrust and suspiciousness about other people’s motives, and usually those motives are considered malevolent.
Cluster B
“Dramatic, Emotional, Erratic” disorders, as their name implies, are disorders that cause significant disruption and even harm to self and others.
Borderline personality disorder
Marked by a significant and disruptive pattern of instability in interpersonal relationships, mood, self-image, and impulse control. Characterized by instability in relationships and moods. Tend to have a poor self-image and are very impulsive and unpredictable.
Histrionic personality disorder/Narcissistic personality disorder
Attention-seeking and self-centeredness are characteristic of these disorders.
Antisocial personality disorder (APD)
Most frequently associated with criminal behavior. A person with this disorder often is unable to feel any empathy or guilt, and that inability leads to a pattern of disregard for the rights and well-being of others and rampant manipulative behavior.
Cluster C
“Anxious and Fearful” disorders include avoidant, dependent, and obsessive-compulsive personality disorders.
Obsessive-compulsive personality disorder
Involves a disruptive preoccupation with orderliness, perfectionism, and personal and interpersonal control.
Neurocognitive disorders (NCD)
Refer to a group of disorders in which the primary problem is in cognitive function, but it is an acquired disorder rather than a developmental one.
Alzheimer’s disease
Progressive neurodegenerative disorder that causes memory loss, confusion, and changes in behavior.
Lewy body-related dementia
Causes neurocognitive impairment but also includes hallucinations as a symptom. Protein deposits
Delirium
The central features include cognitive dysfunction in attention or awareness, limited attention span, and confusion. Additionally, memory deficit, disorientation, and perceptual disturbance may be caused by a direct physiological or medical condition; tends to be transient—it comes and goes.
Psychology student syndrome
A condition mentioned in the context of the DSM-5, where students studying psychology may start to worry that they have a particular psychological disorder after learning about its symptoms. This happens when certain symptoms described in the course material resonate with the student, leading them to wonder if they might have that disorder. However, these feelings are typically temporary and may not reflect an actual mental health issue.
International Classification of Diseases (ICD)
The latest edition of the DSM that has attempted to harmonize with another classification tool. Published by the World Health Organization (WHO) and classifies an extensive range of medical conditions and also includes a comprehensive classification system for mental disorders.
Comorbidity
The presence of two or more disorders at the same time.
Intellectual development disorder
Refers to deficits of general mental abilities such as intellectual functioning and adaptive behaviors.
Autism spectrum disorder
A developmental disorder that centers on repetitive behaviors and impairments of social communication and interaction.
Tic disorder
A condition characterized by involuntary, repetitive movements or sounds called tics. These tics can be motor (e.g., blinking, head jerking) or vocal (e.g., grunting, throat clearing). The tics may be brief or occur in longer bursts, and they can vary in severity. Tic disorders are often seen in children and may improve with age.
Intellectual functioning
Refers to learning ability, problem-solving, and reasoning.
Adaptive behavior
Refers to social, practical, and conceptual skills such as the ability to follow rules and/or avoid being victimized (social), upkeep of personal hygiene and use of money or a telephone (practical), and the ability to apply literacy, number concepts, and self-direction (conceptual).
Anxiety
A feeling of unease, fear, or worry that something bad is about to happen, is a part of everyday life.
Generalized anxiety disorder (GAD)
Defined as prolonged (six months or longer) feelings of unspecified worry and unease. Individuals with this disorder are unable to stop the constant feelings of dread without a clear cause, and these feelings disrupt their daily lives. Other specific symptoms may include fatigue, restlessness, irritability, sleep disturbances, and muscle tension. Physical symptoms associated with heightened levels of distress, including headache, gastrointestinal problems, or diarrhea, are common in people with this disorder.
Panic disorder
Described as an acute, or sudden and severe, feeling of extreme anxiety or fear that something terrible will happen at any minute.
Derealization
A feeling of unreality.
Depersonalization
A feeling of being detached from oneself.
Specific phobia disorder
An anxiety disorder encompassing an overwhelming, unreasonable, and persistent sense of fear of a phobic stimulus, which can be an object or situation that provokes the fear response and sometimes a panic attack.
Agoraphobia
A fear of open, crowded, or enclosed spaces such as shops or movie theaters. May also include a fear of being outside the safety of one’s home or a fear of standing in line in a crowd. Many people diagnosed with phobia have a history of panic attacks. The fear of being in situations where escape might be difficult or help unavailable if needed.
Social anxiety disorder
(social phobia) causes some people to become overwhelmed with anxiety and fear when in social situations. They have an intense fear of being criticized or embarrassed so they avoid such social situations as large events or parties, public speaking, being on stage, or using public restrooms.
Obsessive-compulsive disorder
A mental health condition characterized by persistent, unwanted thoughts (obsessions) and repetitive behaviors or rituals (compulsions) that a person feels compelled to perform. These actions are often done to reduce the anxiety caused by the obsessions, but they provide only temporary relief. This disorder can involve specific obsessions, such as hoarding, obsessive skin picking, obsessive hair pulling (trichotillomania), or a preoccupation with one’s appearance (body dysmorphia). These behaviors can significantly interfere with daily life and functioning.
Hoarding disorder
A mental health condition characterized by persistent difficulty in discarding or parting with possessions, regardless of their actual value. Individuals with this disorder feel a strong emotional attachment to objects, and the thought of discarding them leads to intense anxiety. A woman with this disorder, for example, knows it is ridiculous to refuse to throw away used bandages, but inside her mind is the obsessive thought that something profoundly important is connected to that used bandageand throwing it away could lead to tragedy. The thought of throwing it away sends her anxiety soaring. So she saves it, along with everything else—used teabags, price tags from purchased items, and shoes beyond repair. One woman saved all the hair that accumulated in her hairbrush.
Body dysmorphic disorder
A condition related to OCD in which the affected person has an obsessive preoccupation with his or her physical appearance. In this disorder, the anxiety-reducing compulsive behavior may include compulsive grooming or frequent checking of one’s appearance in mirrors or window reflections.
Anhedonia
The inability to experience any pleasure.
Dysphoria
An intense state of unease.
Acute stress disorder (ASD)
Characterized by symptoms that begin to develop shortly after people experience or witness a traumatic event. They may include uncontrollable flashback memories and nightmares, dissociative symptoms, sleep disturbances, hypervigilance, and problems processing the traumatic event.
Post-traumatic stress disorder (PTSD)
A mental health condition that can develop after an individual experiences or witnesses a traumatic event, such as a natural disaster, serious accident, war, or assault. Symptoms include flashbacks, nightmares, severe anxiety, and avoidance of situations or places that remind the person of the trauma. People with PTSD may also feel detached or numb, and experience heightened emotional responses like irritability or difficulty sleeping. The condition can significantly impact daily life and functioning.
Dissociative amnesia
The inability to remember parts of the past as a result of trauma. The loss of these memories is triggered psychologically rather than by physical damage and is often associated with traumatic events such as rape or child abuse.
Localized amnesia
The inability to remember events during a specific stretch of time, such as the period of childhood from age five to age seven—is the most common type of memory loss.
Selective amnesia
Involves the loss of only certain specific memories. For example, a soldier may remember what he was doing before and after an explosive device blew up near him and killed his fellow soldier and friend, but he cannot remember the actual event.
Generalized amnesia
The total loss of memory of one’s life, including learned skills and acquired knowledge—is rare. People with this amnesia are often referred to law enforcement and psychiatric care because they are found to wander aimlessly.
Dissociative fugue
Refers to the complete loss of awareness of one’s identity and the assumption or development of another identity.
Dissociative identity disorder
Formerly called multiple personality disorder, is the presence of at least two distinct identities (alters) that appear in a host’s behavior along with impaired memory beyond mere forgetfulness. The mind partitions itself into two or more distinct personalities that may or may not know about each other.
Somatic symptom disorder
Characterized by extreme anxiety about physical symptoms that are interpreted as evidence of illness. Occurs when a person manifests a psychological problem (generally stress) through a physiological symptom. (Formerly Hypochondriasis)
Illness anxiety disorder (IAD)
A severe obsession with having or getting a serious illness despite no indication of illness following a medical exam. Previously known as hypochondriasis or hypochondria.
Conversion disorder
(functional neurological symptom disorder) is “con- version” of extreme anxiety into a physical disorder. The physical symptoms are real but no neurological or medical cause can be identified clinically. This disorder are characterized by motor symptoms such as weakness or paralysis, abnormal movements, limp, and tremors. Sensory symptoms include reduced or absent sense of touch, vision, or hearing. In extreme cases, non-epileptic (psychogenic) seizures may occur, as well as inability to speak and even coma.
Factitious disorder
If a person falsely reports, or deliberately creates or exaggerates symptoms to get medical attention, that person is exhibiting symptoms of this disorder.
Factitious disorder imposed on another
Another more harmful type of factitious disorder; (previously known as Munchausen syndrome by proxy), which involves the deliberate falsification of physical or psychological symptoms or actually inducing these symptoms in someone else in order to gain emotional attention and sympathy.
Anorexia nervosa
(often referred to as anorexia) is a life-threatening eating disorder that involves intense fear of weight gain or becoming overweight, a distorted perception of one’s weight or body shape, and persistent restriction of caloric intake leading to extreme weight loss and increasing damage to physical health. It affects more females than males and occurs more frequently in young adults. Typical symptoms of this include abrupt and profound weight loss coupled with exercise and constant weighing, compulsive and covert checking of one’s body in mirrors or reflective surfaces, and increased verbalization of the fear of weight gain or being fat.
Bulimia nervosa
(commonly referred to as bulimia) is a potentially life- threatening eating disorder that involves secretive binging—eating large or excessive amounts of food in a short period of time.
Binging/Purging
Self-induced vomiting, misuse of laxatives or diuretics (medications that increase urination to remove excess fluid from the body), and fasting or excessive exercise to compensate for the high calorie intake.
Awfulizing
(cognitive perceptions that things are much worse than they really are) and rigid thinking.
Binge-eating disorder
Is the most common eating disorder and involves recurrent episodes of eating excessive amounts of food in a short period of time accompanied by an intense sense of lack of control over the eating behavior.
Social Cognition
How we think about ourselves/others in social situations.
Social Situations
Influence on even controls behavior; refers to a group of two or more people or may also describe an individual alone who thinks that others are observing him or her.
Social Influence
How we are influenced by others; how we are influenced by others in a social situation.
Social Psychology
The scientific study of how we think about, influence and relate to one another; a branch of psychology that uses a scientific approach to understand how and why social groups influence individual behavior and attitudes and how, in turn, individual attitudes and behaviors affect social groups.
Social Behavior
How we behave in social situations.
Schema
A cognitive filter through which we view the world and interpret information.
Self-Schema
A construct about himself and his experiences.
Possible Selves
Aspects of ourselves that we either aspire to be or could conceivably be.
Self-Serving Biases
Tendencies to perceive ourselves in a positive light; the tendency to attribute success to internal factors while blaming failure on external situations.
Attribution
The process of explaining why a person behaves a certain way, as a way of understanding how and why individuals explain their own behaviors, as well as the behaviors of others.
Internal Attribution
An assumption that behavior is driven by such internal characteristics as traits or feelings; Behavior that is explained as a result of personal characteristics.
External Attribution
The assumption that a person's behavior is influenced by external factors, such as the environment, other people, or situational circumstances, rather than their personal traits or characteristics; Behavior is explained as the result of unavoidable factors.
Stable Attribution
Refers to the belief that a cause of behavior is consistent and unchanging over time. For example, if a student gets an A on an exam and you assume it's because they are naturally smart, that is a stable attribution because intelligence is seen as a lasting trait.
Unstable Attribution
Refers to the belief that the cause of behavior is temporary and can change. For example, if a student gets an A and you attribute it to them studying hard for that particular exam, that is an unstable attribution because effort can vary from one situation to another.
Attribution Theory
Was first developed by Fritz Heider (1896–1988) and was later expanded by other researchers who, even into the 21st century, have used attribution theory as an investigative tool to determine the causes of behavior. Attribution theory suggests that causes of behaviors comprise two dimensions: (1) internal vs. external and (2) stable vs. unstable.
Consensus
Refers to the level of agreement among people regarding a particular opinion or behavior.
Distinctiveness
Refers to how unique or specific a person’s reaction is to a particular situation.
Consistency
Refers to how regularly a person behaves the same way in similar situations over time.
Just-World Hypothesis
Is the belief that the world is fair and that people get what they deserve. This viewpoint leads people to assume that victims must have done something to deserve their fate, reducing their perceived connection to the victim. It is a defensive and biased attribution that helps people feel safe by maintaining the illusion that bad things won’t happen to them.
Correspondent Interference Theory
Social psychologists Edward E. Jones (1926–1993) and Keith Davis of Duke University introduced the idea; This theory explains why people make internal or external attributions. It suggests that people tend to attribute others' behaviors to internal, stable traits rather than external circumstances.
Actor-Observer Bias
The tendency to attribute others' behaviors to internal factors (e.g., personality) but to explain our own behaviors using external factors (e.g., the situation). For example, if someone else is late, we might think they are irresponsible, but if we are late, we blame traffic. Attribute behaviors to situational effects when we are the actor, but attribute behavior to disposition factors when we are the observer.
Fundamental Attribution Error
The tendency to overemphasize internal traits and ignore external factors when explaining other people’s behaviors. For example, if we see someone hitting another person, we assume they are aggressive rather than considering possible external reasons (e.g., self-defense). Tendency for observers, when observing others, to underestimate the impact of the situation and overestimate the impact of personal disposition.
Ultimate Attribution Error
The tendency to apply the fundamental attribution error to entire groups rather than individuals. For example, if one member of a minority group commits an act of aggression, people may assume the entire group is aggressive, reinforcing stereotypes. Applying to an entire group, like gender or ethnic group.
Attitudes
Represent how you feel toward various objects; how you feel about something.
Cognitive Dissonance
A theory introduced by Leon Festinger (1919–1989) in 1957, identifies the discomfort felt when we hold two contradictory views simultaneously or act in a way that conflicts with our beliefs.
Leon Festinger
Introduced the cognitive dissonance theory.
Overjustification Effect
Refers to the phenomenon where providing external rewards for an activity that someone already enjoys reduces their intrinsic motivation for that activity.