B.VET TECH OSCE REVISION 2022
0.0(0)
Studied by 0 peopleCard Sorting
1/113
Earn XP
Description and Tags
Last updated 8:35 AM on 11/7/22
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
114 Terms
1
New cards
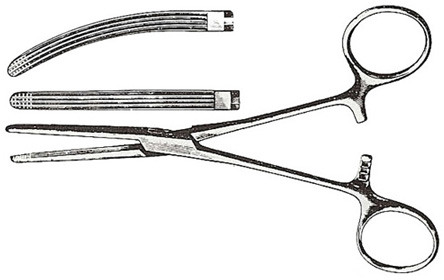
Mayo-Hegar Needle Holder/Driver
Used for suturing

2
New cards
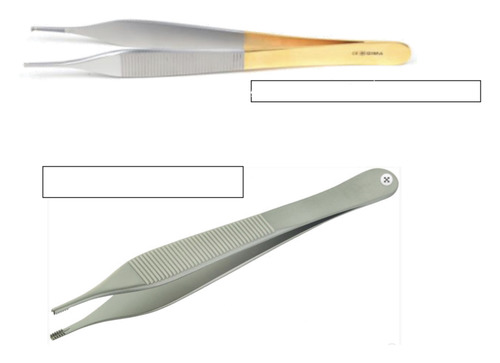
Adson Brown Tissue Forceps
Instrument with several small and delicate teeth that are used for light handling of delicate tissue
3
New cards
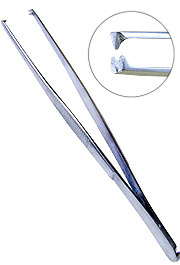
Rat Tooth Tissue Forceps
used to grasp skin and other dense tissue
teeth are generally bigger than those in the adson tissue, and the handle is skinnier than the adson tissue
teeth are generally bigger than those in the adson tissue, and the handle is skinnier than the adson tissue
4
New cards
Debakey tissue forceps
Vascular; grasping fine tissue; many lengths ; used in all types of surgery ; 1 x 2 rows of serrations

5
New cards
Metzenbaum Scissors
To blunt-dissect or cut soft fine tissues

6
New cards
Mayo Scissors
A heavy scissor used for cutting tough tissue; muscle/ fascia, blades may be straight or curved.

7
New cards
Suture Scissors
Used to cut sutures

8
New cards
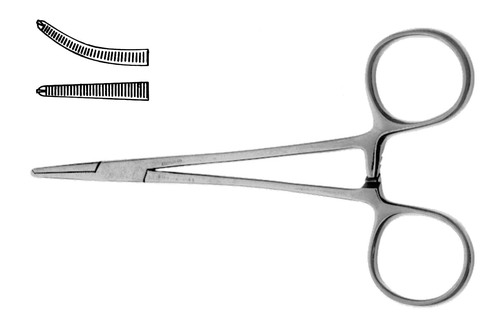
Mosquito Haemostats
Small delicate haemostatic forceps for small vessels.
9
New cards
Allis Tissue Forceps
Inward curving forcing toothed blades and a ratcheted handle designed for grasping fascia and tendons.
10
New cards
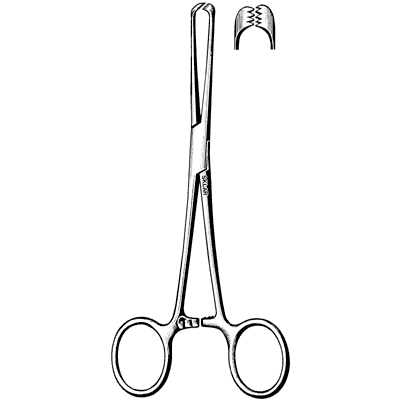
Backhaus Towel Clamps
used to attach towels and drapes to the px

11
New cards
Rochester Carmalt Forceps
Used to clamp and crush tissue bundles that contain blood vessels. Longitudinal grooves and cross grooves at the tip.
12
New cards
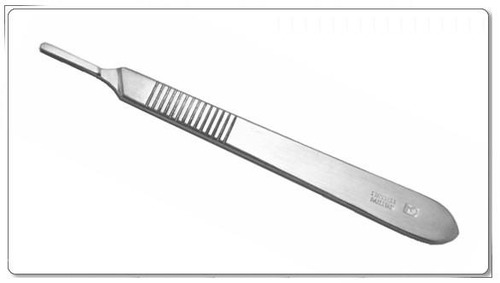
Scalpel Blade Holder
holds scalpel blade
13
New cards
Ovarian hysterectomy margins
cranial margins diaphragm & caudally brim of pubis/ vulva or 10-15cm either side of incision site which is caudal of the umbilicus
14
New cards
Castration margins
cranial margin prepuce & caudally the scrotum; then 10cm either side of the incision site
15
New cards
surgical clipper blade
size 40
16
New cards
tick clip- clipper blade
size 10
17
New cards
Cleaning instruments
Soak Medyzyme >5min
Scrub debris
Rinse in deionised water
Ultrasonic cleaner
Rinse in deionised water
Autoclave
**Cannot pack wet
Scrub debris
Rinse in deionised water
Ultrasonic cleaner
Rinse in deionised water
Autoclave
**Cannot pack wet
18
New cards
Surgical hand scrub
Removes as many microorganisms as possible Chlorhexidine 4% solution; minimum 5 min contact time
Hand scrubbing 5-10 min, chlorhex hand scrub, nails-pick, nail scrub- bristle side, soft foam= hand, breaking asepsis = minor= clean specific area, major = rescrub from the beginning
Hand scrubbing 5-10 min, chlorhex hand scrub, nails-pick, nail scrub- bristle side, soft foam= hand, breaking asepsis = minor= clean specific area, major = rescrub from the beginning
19
New cards
Gowning
1. Standing approximately 50cm from the sterile area*, pick up the gown by the *folded edges* and lift it directly up from the package. The gown is folded so that the outside faces away.
2. Stepping back from the table, make sure *no objects are near the gown*. Holding the gown at the *shoulders*, allow it to unfold gently. *Do not shake* the gown.
3. Place the hands inside the *armholes* and guide each arm through the sleeves by raising and spreading the arms.
4. For the *open gloving* technique, *pull the sleeves over the hands*. For the *closed gloving* technique, keep the hands and *fingers covered by the sterile gown*.
5. An *assistant fastens the back and waistband* of the gown.
2. Stepping back from the table, make sure *no objects are near the gown*. Holding the gown at the *shoulders*, allow it to unfold gently. *Do not shake* the gown.
3. Place the hands inside the *armholes* and guide each arm through the sleeves by raising and spreading the arms.
4. For the *open gloving* technique, *pull the sleeves over the hands*. For the *closed gloving* technique, keep the hands and *fingers covered by the sterile gown*.
5. An *assistant fastens the back and waistband* of the gown.
20
New cards
Open gloving method
1. hand washing
2. open the glove wrapper from the corner and peel back the sides
3. place the inner glove on a clean dry surface
4. place the package so the the right glove on your right side.
5.open
6. glove the dominant hand first grasp the glove by the cuff.
8. slip the first four finger of your dominant hand under the cuff
9. use the non dominant hand into the cuff of the dominant hand glove and open the cuff
2. open the glove wrapper from the corner and peel back the sides
3. place the inner glove on a clean dry surface
4. place the package so the the right glove on your right side.
5.open
6. glove the dominant hand first grasp the glove by the cuff.
8. slip the first four finger of your dominant hand under the cuff
9. use the non dominant hand into the cuff of the dominant hand glove and open the cuff
21
New cards
closed gloving method
1. with hands covered by gown sleeves, open inner sterile glove package. dominant hand picks up glove for non dominant hand by grasping folded cuff
2. extend nondominant forearm w/ palm up & place palm of glove against palm of non dominant hand. glove fingers point toward elbow
3. grasp back of glove cuff w/ covered dom. hand, turn glove cuff over end of nondom. hand & gown cuff
4. grasp top of glove & underlying gown sleeve w/ covered dom. hand & extend fingers into glove being sure glove's cuff covers gown's cuff
5. glove dominant hand in same manner, reversing hands. used glove nondom. to pull on glove. keep hand inside sleeve
6. be sure fingers are fully extended
2. extend nondominant forearm w/ palm up & place palm of glove against palm of non dominant hand. glove fingers point toward elbow
3. grasp back of glove cuff w/ covered dom. hand, turn glove cuff over end of nondom. hand & gown cuff
4. grasp top of glove & underlying gown sleeve w/ covered dom. hand & extend fingers into glove being sure glove's cuff covers gown's cuff
5. glove dominant hand in same manner, reversing hands. used glove nondom. to pull on glove. keep hand inside sleeve
6. be sure fingers are fully extended
22
New cards
Surgical preparation of patient
Confirm patient position for sx
Clip in prep room
Clip appropriate margins as confirmed by vet
No 40 size clipper blades
Vacuum loose hair
Px skin prep
Drape
Clip in prep room
Clip appropriate margins as confirmed by vet
No 40 size clipper blades
Vacuum loose hair
Px skin prep
Drape
23
New cards
Surgical scrub step 1
dilute 1:6, 100ml and 600ml h2O (700ml total); aqueous chlorhexidine 4% surgical scrub add gauze swabs; repeat a total 3 times after all debris removed 5 min contact time
24
New cards
Surgical scrub step 2
methylated/ alcohol scrub; soak swab in alcohol/ methylated spirits then wipe inscision site with concentric circles, until chlorhex is removed in prep and Sx. **ensure swabs do not go back over the cleaned surface/ incision site
25
New cards
Surgical scrub step 3
chlorhex- metho spray; 0.5% chlorhex- in 70% alcohol; light mist once moved to theatre, allow to air dry
26
New cards
Sx prep excretions
ensure the px has urinated pre sx, if not express bladder once anesthetised and place purse string if required
27
New cards
Sx prep Clip
confirm clip margins ; 15-20cm around incision site
clip with the hair, then against the hair
vacuum px and table to remove all hair prior to scrub
clip with the hair, then against the hair
vacuum px and table to remove all hair prior to scrub
28
New cards
Sx prep scrub other chemicals
PVP Iodine; 2.5mls iodine with 500ml distilled water used for sx scrub on mucous membranes -> eyes, mouth ears
Aqueous chlorhexidine; 40ml : 4L water, for flushing prepuce and vulva
Aqueous chlorhexidine; 40ml : 4L water, for flushing prepuce and vulva
29
New cards
Draping the patient
unfold, fold, tuck, place, clamp
lateral drape first
lateral drape first
30
New cards
Cleaning instruments and surgical kits
clean and rinse with distilled water, clean with medizyme, ultrasonic cleaning, lubricate, dry
31
New cards
When packing surgical kits; they require
sterile indicator strips and tape, label; name/ initials, date packed, kit type
32
New cards
Sterilisation of surgical kits
autoclave to destroy microorganisms via protein denaturing; heavy items on bottom chamber
33
New cards
Care and maintenance of clippers; non contaminated blades
- remove gross debris (remove blade, brush)
- clean with blade wash (small amount to cover blade, run 30 sec, dry with gauze)
- disinfect with alcohol chlorhexidine (2 min contact time, wipe dry)
- clipper oil
- wipe hand piece with F10
- Charge
- clean with blade wash (small amount to cover blade, run 30 sec, dry with gauze)
- disinfect with alcohol chlorhexidine (2 min contact time, wipe dry)
- clipper oil
- wipe hand piece with F10
- Charge
34
New cards
Care and maintenance of clippers; contaminated blades
- wear gloves remove gross debris (remove blade, brush)
- disinfect with F10 min 60 sec- if parvo >15 min, wipe dry with clean gauze
- surgistain; with gloves make solution 1:7 water, soak blades for 15 min, rinse in distilled water & dry
- clipper oil
- wipe hand piece with F10
- Charge
- disinfect with F10 min 60 sec- if parvo >15 min, wipe dry with clean gauze
- surgistain; with gloves make solution 1:7 water, soak blades for 15 min, rinse in distilled water & dry
- clipper oil
- wipe hand piece with F10
- Charge
35
New cards
Anaesthesia rebreathing system check
1. Attach oxygen hose
2. Attach scavenge hose to pendant
3. Turn scavenge on
4. Attach scavenge hose to spill valve
5. Check oxygen flush button
6. Turn flowmeter on full, then back to 2L/min
7. Flowmeter seal check
8. Vaporiser seal check
9. Check vaporiser full
10. Check vaporiser dial rotates all the way
11. Check vaporiser locked on if selectatec mount
12. Check soda lime canister
13. Attach fresh gas hose to Common Gas Outlet
14. Attach rebreathing system to soda lime canister
15. Attach Rebreathing Bag (RB)
16. Occlude breathing circuit with thumb
17. Close spill valve - for pressure/leak check
18. Pressurise circuit to 20cm H20 and ensure pressure does not drop
19. Check one-way valves
20. Open spill valve (very important patient will die if spill valve not opened)
21. Empty RB bag with y-piece occluded then unblock breathing circuit
2. Attach scavenge hose to pendant
3. Turn scavenge on
4. Attach scavenge hose to spill valve
5. Check oxygen flush button
6. Turn flowmeter on full, then back to 2L/min
7. Flowmeter seal check
8. Vaporiser seal check
9. Check vaporiser full
10. Check vaporiser dial rotates all the way
11. Check vaporiser locked on if selectatec mount
12. Check soda lime canister
13. Attach fresh gas hose to Common Gas Outlet
14. Attach rebreathing system to soda lime canister
15. Attach Rebreathing Bag (RB)
16. Occlude breathing circuit with thumb
17. Close spill valve - for pressure/leak check
18. Pressurise circuit to 20cm H20 and ensure pressure does not drop
19. Check one-way valves
20. Open spill valve (very important patient will die if spill valve not opened)
21. Empty RB bag with y-piece occluded then unblock breathing circuit
36
New cards
Anaesthesia non-rebreathing system check
1. Attach oxygen hose
2. Attach scavenge hose to pendant
3. Turn scavenge on
4. Check oxygen flush button
5. Turn flowmeter on full, then back to 2L/min
6. Flowmeter seal check
7. Vaporiser seal check
8. Check vaporiser full
9. Check vaporiser dial rotates all the way
10. Attach NRB to Common Gas Outlet
11. Attach Rebreathing Bag (RB)
12. Attach scavenge hose to spill valve on NRB
13. Close spill valve - for pressure/leak check
14. Occlude breathing circuit with thumb
15. Pressurise circuit to 20cm H20 and ensure pressure does not drop
16. Open spill valve (very important patient will die if spill valve not opened)
17. Empty RB bag with breathing system occluded then unblock breathing circuit
18. Checking integrity of coaxial green Fresh Gas Tube in a Bain NRB
• Depress oxygen flush valve (the rebreathing bag should compress)
2. Attach scavenge hose to pendant
3. Turn scavenge on
4. Check oxygen flush button
5. Turn flowmeter on full, then back to 2L/min
6. Flowmeter seal check
7. Vaporiser seal check
8. Check vaporiser full
9. Check vaporiser dial rotates all the way
10. Attach NRB to Common Gas Outlet
11. Attach Rebreathing Bag (RB)
12. Attach scavenge hose to spill valve on NRB
13. Close spill valve - for pressure/leak check
14. Occlude breathing circuit with thumb
15. Pressurise circuit to 20cm H20 and ensure pressure does not drop
16. Open spill valve (very important patient will die if spill valve not opened)
17. Empty RB bag with breathing system occluded then unblock breathing circuit
18. Checking integrity of coaxial green Fresh Gas Tube in a Bain NRB
• Depress oxygen flush valve (the rebreathing bag should compress)
37
New cards
endotracheal tube cuff inflation
Inflate until you can no longer hear air escaping around the ET tube- have one person close the spill valve and give a breath between 10-20H2O depending on the size of the patient, slowly inflate, continue this process until there is no sound/ air escaping
38
New cards
drug calculations
dose = concentration x volume
39
New cards
A 40 kg dog requires antibiotics for a urinary tract infection. She needs 20 mg/kg of amoxicillin/clavulanic acid three times a day for three weeks.
How many 500 mg tablets does she require for each dose?
How many tablets do you need to send home with the owner?
How many 500 mg tablets does she require for each dose?
How many tablets do you need to send home with the owner?
Dose = Dose rate (mg/kg) x Weight (kg)
Dose = 20 mg/kg x 40kg = 800 mg
Volume = 800 mg/500 mg/tablet = 1.6 tablets
1.6 tablets per dose (will accept 1 1/2 tablets or 2 tablets)
1.5 x 3 x 21 = 95 tablets
or
2 x 3 x 21 = 126 tablets
Dose = 20 mg/kg x 40kg = 800 mg
Volume = 800 mg/500 mg/tablet = 1.6 tablets
1.6 tablets per dose (will accept 1 1/2 tablets or 2 tablets)
1.5 x 3 x 21 = 95 tablets
or
2 x 3 x 21 = 126 tablets
40
New cards
You are asked to prepare a drug label for a patient. The patient is a 6 kg cat that requires 5 days of meloxicam suspension (0.5 mg/ml) to be given per os once a day. The veterinarian wants the cat to have 0.1 mg/kg of meloxicam on the first day and 0.05 mg/kg per day after that. You have the choice of a 15 or 30 ml bottle.
S: Dose (1st day) = 6 kg x 0.1 mg/kg = 0.6 mg
Dose (subsequent days) = 6kg x 0.05mg/kg
Volume = 0.6 mg/0.5 mg/ml = 1.2 ml on the first day and 0.6 ml on subsequent days.
Volume required for total treatment = 1.2 + (0.6 x 4) = 3.6 ml so 15 ml bottle most appropriate.
Give X 1.2 ml meloxicam (0.5mg/ml) orally with food on the first day Give 0.6 ml ml once a day orally with food for subsequent 4 days. Do not treat past 5 days.
Dose (subsequent days) = 6kg x 0.05mg/kg
Volume = 0.6 mg/0.5 mg/ml = 1.2 ml on the first day and 0.6 ml on subsequent days.
Volume required for total treatment = 1.2 + (0.6 x 4) = 3.6 ml so 15 ml bottle most appropriate.
Give X 1.2 ml meloxicam (0.5mg/ml) orally with food on the first day Give 0.6 ml ml once a day orally with food for subsequent 4 days. Do not treat past 5 days.
41
New cards
You are asked to draw up 2 mg/kg of alfaxalone to be used to induce a 9 kg dog. The concentration of the afaxalone is 10 mg/ml.
a) What volume will you draw up?
b) The vet wants the alfaxalone diluted to 5 mg/ml. How much saline would you add?
c) If the vet was to add enough saline to the original volume (part a) to finish with a total of 5 ml what would be the concentration of alfaxalone?
a) What volume will you draw up?
b) The vet wants the alfaxalone diluted to 5 mg/ml. How much saline would you add?
c) If the vet was to add enough saline to the original volume (part a) to finish with a total of 5 ml what would be the concentration of alfaxalone?
S: a) Dose = 2 mg/kg x 9 kg = 18 mgVolume = 18mg / 10 mg/ml = 1.8 ml
b) There are two ways to work this out. The important thing to remember that the dose of 18 mg remains the same.
The way that you seemed to prefer is;
The new concentration = 5mg/ml. This is half the concentration of the original 10mg/ml. If we are going to use half the concentration we will need to give double the dose rate to get the same dose of 18 mg.
Therefore you will need a total of 3.6 mls of (5mg/ml alfaxalone) to provide 18 mg. You will need to draw up 1.8 mls of alfaxalone out of the bottle (10 mg/ml).
As the total volume needed is 3.6 mls and you have 1.8 mls of alfaxalone out of the bottle you will need 1.8 mls of saline
Eg. total volume 3.6ml = volume of alfaxalone 1.8ml + volume of saline 1.8ml
While the concentration and volumes change the dose does notC1 x V1 = C2 x V218 mg = 5 x V2V2 = 3.6 ml, 3.6 - 1.8 = 1.8 ml of saline
If we to work through the additional example in the tutorial
If you need to dilute 10 mg/ml alfaxalone to 2 mg/ml then
2 mg/ml is 1/5 of 10 mg/ml ie 2/10.
If the concentration is 1/5 of the original you will need 5 times the volume.
Therefore Volume = 5 x 1.8 ml (10mg/ml) = 9ml
Total volume = volume of alfaxalone + volume of saline
Therefore volume of saline = total volume - volume of alfaxalone = 9ml - 1.8 ml = 7.2 ml
c) C = dose/volume = 18 mg/5ml = 3.6 mg/ml
b) There are two ways to work this out. The important thing to remember that the dose of 18 mg remains the same.
The way that you seemed to prefer is;
The new concentration = 5mg/ml. This is half the concentration of the original 10mg/ml. If we are going to use half the concentration we will need to give double the dose rate to get the same dose of 18 mg.
Therefore you will need a total of 3.6 mls of (5mg/ml alfaxalone) to provide 18 mg. You will need to draw up 1.8 mls of alfaxalone out of the bottle (10 mg/ml).
As the total volume needed is 3.6 mls and you have 1.8 mls of alfaxalone out of the bottle you will need 1.8 mls of saline
Eg. total volume 3.6ml = volume of alfaxalone 1.8ml + volume of saline 1.8ml
While the concentration and volumes change the dose does notC1 x V1 = C2 x V218 mg = 5 x V2V2 = 3.6 ml, 3.6 - 1.8 = 1.8 ml of saline
If we to work through the additional example in the tutorial
If you need to dilute 10 mg/ml alfaxalone to 2 mg/ml then
2 mg/ml is 1/5 of 10 mg/ml ie 2/10.
If the concentration is 1/5 of the original you will need 5 times the volume.
Therefore Volume = 5 x 1.8 ml (10mg/ml) = 9ml
Total volume = volume of alfaxalone + volume of saline
Therefore volume of saline = total volume - volume of alfaxalone = 9ml - 1.8 ml = 7.2 ml
c) C = dose/volume = 18 mg/5ml = 3.6 mg/ml
42
New cards
The veterinarian you are working with wants to perform local blocks on a feline dental patient that weighs 5.5 kg. The maximal allowable dose rate of lignocaine in the cat is 6 mg/kg. The veterinarian wants you to calculate the volume of 2% lignocaine that corresponds to this dose rate. What is your answer?
Dose = Wt x dose rate = 5.5 kg x 6 mg/kg = 33 mg.
The concentration of lignocaine is 20 mg/ml.
Therefore the volume = 33/20 = 1.65 ml.
The concentration of lignocaine is 20 mg/ml.
Therefore the volume = 33/20 = 1.65 ml.
43
New cards
You are setting up gravity feed fluids for a cat spey. The cat weighs 3.8 kg. You will be using a burette which delivers 60 drops/ml. The veterinarian wishes Hartmans to be administered at a rate of 3 ml/kg/hr during the procedure.
How many drops per second do you need to give?
The spey lasts for 20 min. How much Hartmans should the cat have received in this time?
How many drops per second do you need to give?
The spey lasts for 20 min. How much Hartmans should the cat have received in this time?
Dose = Dose rate x Wt = 3.8 kg x 3 ml/kg/hr = 11.4 mls/hr
11.4 x 60 drops/hr = 684 drops per hr.As there are 60 min in a hour
684/60 = drops/min = 11.4
As there are 60 s in a minute11.4/60 = 0.2 drops/sec or 1 drop every 5 s
11.4 mls/hr = 0.19 ml/min
over 20 min = 0.19 x 20 = 3.8 mls
11.4 x 60 drops/hr = 684 drops per hr.As there are 60 min in a hour
684/60 = drops/min = 11.4
As there are 60 s in a minute11.4/60 = 0.2 drops/sec or 1 drop every 5 s
11.4 mls/hr = 0.19 ml/min
over 20 min = 0.19 x 20 = 3.8 mls
44
New cards
A 15 kg dog needs to be placed on a ketamine infusion at a rate of 5 microg/kg/min. If the concentration of the infusion is 1 mg/ml, what rate in mls/hr would you write on the chart?
Dose = dose rate x Wt = 15 kg x 5 microg/kg/min = 75 microg / min
As there are 60 min in hour = 4,500 micog / hr
As there were 1000 micrograms in a ml
4,500/1000 mg/hr = 4.5 mg/hr
Volume = Dose/concentration = 4.5/1 mg/ml = 4.5 ml/hr.
As there are 60 min in hour = 4,500 micog / hr
As there were 1000 micrograms in a ml
4,500/1000 mg/hr = 4.5 mg/hr
Volume = Dose/concentration = 4.5/1 mg/ml = 4.5 ml/hr.
45
New cards
A 7 kg dog requires a fentanyl infusion to be administered at 4 microg/kg/hr for 24 hours. How many vials of fentanyl 500 microg in 10 ml would be needed to make this infusion?
Dose = dose rate x Wt = 4microg x 7kg x 24hr = 672 microg for the 24 hours
Volume = dose/concentration = 672microgr/500microg per vial = 1.34 vials of fentanyl
Volume = dose/concentration = 672microgr/500microg per vial = 1.34 vials of fentanyl
46
New cards
A 26 kg dog requires a dopamine infusion to be administered at 7 microg/kg/min. How many mls per hour does this dog need? You need to make the dopamine solution first by injecting a 5 ml ampule of dopamine which contains 200 mg into a 500 ml bag of 0.9% NaCl.
Dose = dose rate x Wt = 7 microg x 26 kg = 182 microg per minute.
As the rate will be in hours we need to work out how many microg/hour
Dose = 182 microg x 60 min per hour = 10,920 microg/hour.
This is a large number so we will convert it to mg. Remember 1000 microg in a milligram
Dose = 10,920 microg/1000 = 10.92 mg
To work out our hourly rate we need the concentration of the solution. We need to make this up
If we add 200 mg into a 500 ml bag (after removing 5 ml of saline) the
Concentration = amount of solute/volume = 200 mg/500 ml = 0.4 mg/ml
Dose = Dose rate/concentration = 10.92 mg/hr / 0.4mg/ml = 27.3ml/hr
As the rate will be in hours we need to work out how many microg/hour
Dose = 182 microg x 60 min per hour = 10,920 microg/hour.
This is a large number so we will convert it to mg. Remember 1000 microg in a milligram
Dose = 10,920 microg/1000 = 10.92 mg
To work out our hourly rate we need the concentration of the solution. We need to make this up
If we add 200 mg into a 500 ml bag (after removing 5 ml of saline) the
Concentration = amount of solute/volume = 200 mg/500 ml = 0.4 mg/ml
Dose = Dose rate/concentration = 10.92 mg/hr / 0.4mg/ml = 27.3ml/hr
47
New cards
A 8 kg fox terrier has been kicked in the head by a horse. You want to administer mannitol at 1g/kg over 20minutes. In a 500 ml bag of Osmitrol there is 100 g of mannitol. What volume/percent is the solution and what rate in ml/hr does the dog need?
Dose = dose rate x Wt = 1 g x 8 kg = 8 g. We usually work in mg so this would be = 8000 mg
Volume = dose rate/concentration
Concentration = amount of solute/volume = 100 g/500ml = 0.2 g/ml
As we are used to working in mg this would = 200 mg/ml (20% w/v)
Volume = dose rate/concentration = 8000mg/200 mg/ml = 40 ml.
The mannitol needs to be given over 20 mlnutes.
The rate of administration would be 2 mg/min which works out to be 120 mls per hour.
Volume = dose rate/concentration
Concentration = amount of solute/volume = 100 g/500ml = 0.2 g/ml
As we are used to working in mg this would = 200 mg/ml (20% w/v)
Volume = dose rate/concentration = 8000mg/200 mg/ml = 40 ml.
The mannitol needs to be given over 20 mlnutes.
The rate of administration would be 2 mg/min which works out to be 120 mls per hour.
48
New cards
A 2 kg puppy needs to be placed on a 2.5% dextrose solution. How much of a 50% dextrose solution would you need to add to a 100 ml of hartmans to make a 2.5% solution?
A 2.5% w/v solution is equivalent to 25 mg/ml.
To make up 100 ml of this solution
Amount = Concentration x volume = 25 mg/ml x 100 ml = 2500 mg
A 50% solution contains 500 mg/ml
Volume = Dose/concentration = 2500/500 = 5 mls of dextrose
To make up 100 ml of this solution
Amount = Concentration x volume = 25 mg/ml x 100 ml = 2500 mg
A 50% solution contains 500 mg/ml
Volume = Dose/concentration = 2500/500 = 5 mls of dextrose
49
New cards
Calculate the flow rate for a 32kg at the beginning of anaesthesia (100 ml/kg/min) and for maintenance (40 ml/kg/min)
A:100 ml x 32kg/min = 3200 ml/min = 3.2 L/min
A: 40ml x 32kg/min = 1280 ml/min = 1.28L/min
A: 40ml x 32kg/min = 1280 ml/min = 1.28L/min
50
New cards
Acepromazine
Use: Sedation- Tranquilizer; causes hypotension and vasodilation
Dose: 0.01- 0.05mg/kg
Concentration: 2mg/ml
Dose: 0.01- 0.05mg/kg
Concentration: 2mg/ml
51
New cards
Alfaxalone (Alfaxan)
Use: induction agent; can cause tachycardia & apnoea
Dose: D 1-2mg/kg C 2-4mg/kg
Concentration: 10mg/ml
Duration: 5-10min
Dose: D 1-2mg/kg C 2-4mg/kg
Concentration: 10mg/ml
Duration: 5-10min
52
New cards
Atipamozole
Alpha 2 antagonist; medetomidine reversal agent
53
New cards
Atropine
Use: anticholinergic; increases HR and contractility of the heart
Duration: 20 min
Duration: 20 min
54
New cards
Butorphanol
Use; partial Mu antagonist and kappa agonist- more pain relief then sedation
Dose: 0.1-0.2 mg/kg
Duration: 2-4hr
Dose: 0.1-0.2 mg/kg
Duration: 2-4hr
55
New cards
Diazapam
Use: anticonvulsant, anxiolytic- muscle relaxant & antiseizure
Dose: 0.5-2mg/kg
Duration: ~8hr
Dose: 0.5-2mg/kg
Duration: ~8hr
56
New cards
Dopamine
Use: positive inotrope, to increase HR, Blood pressure from severe hypotension
Dose: 5-20mg/kg/min (IV CRI)
Dose: 5-20mg/kg/min (IV CRI)
57
New cards
Fentanyl (transdermal)
Use: pure mu/ opioid analgesia
Onset: 12hr post placement
Duration: ~2-3 days
Onset: 12hr post placement
Duration: ~2-3 days
58
New cards
Fentanyl
Use: pure mu/ opioid analgesia
Dose: 1-5mcg/kg
Duration: 20 min
Dose: 1-5mcg/kg
Duration: 20 min
59
New cards
Glyccopyrrolate
Use: anticholinergic; increase HR & BP, inhibit salivary secretions
Dose: 0.011mg/kg
Longer duration
Dose: 0.011mg/kg
Longer duration
60
New cards
Lignocaine (Lidocaine)
Use: Anaesthetic (local block), Antiarrhythmic- VPCs
Dose: 0.5-1mg/kg
Dose: 0.5-1mg/kg
61
New cards
Medetomidine/Dexmedetomidine
Use: alpha 2 agonist sedation & pain relief; can cause initial hypertension then decreased cardiac output; low HR & BP
Dose: 1-10mcg/kg
Concentration: 1mg/ml
Dose: 1-10mcg/kg
Concentration: 1mg/ml
62
New cards
Meloxicam
Use- NSAID
63
New cards
Methadone
Use: pure mu, opioid, provides analgesia
Dose: 0.1-0.5mg/kg
Concentration: 10mg/ml
Duration: 4-6hr
Dose: 0.1-0.5mg/kg
Concentration: 10mg/ml
Duration: 4-6hr
64
New cards
Midazolam
Use: pre-med twilight anaesthesia; anticonvulsant, anxiolytic- muscle relaxant & antiseizure
Dose: 0.2-0.5mg/kg
Dose: 0.2-0.5mg/kg
65
New cards
Naloxone
Use: opioid reversal/ mu antagonist
66
New cards
Propofol
Use: induction agent; can cause apnoea, hypotension and bradycardia
Dose: 4mg/kg
Concentration: 10mg/ml
Effects: 30-60sec
Duration: 20min
Dose: 4mg/kg
Concentration: 10mg/ml
Effects: 30-60sec
Duration: 20min
67
New cards
Radiology; PALACE
P- Positioning of your animal; legs pulled in correct direction
A- Anatomy- included anatomical structures
L- Labelling- appropriate position
A- artifacts; obvious artifact; microchip, ecg lead, motion, sandbags, gloves, positioning aids
C- collimation- centrepoint, don't have excessive anatomy included
E- exposure- is it appropriate; lung; good contrast between soft tissue and gas
A- Anatomy- included anatomical structures
L- Labelling- appropriate position
A- artifacts; obvious artifact; microchip, ecg lead, motion, sandbags, gloves, positioning aids
C- collimation- centrepoint, don't have excessive anatomy included
E- exposure- is it appropriate; lung; good contrast between soft tissue and gas
68
New cards
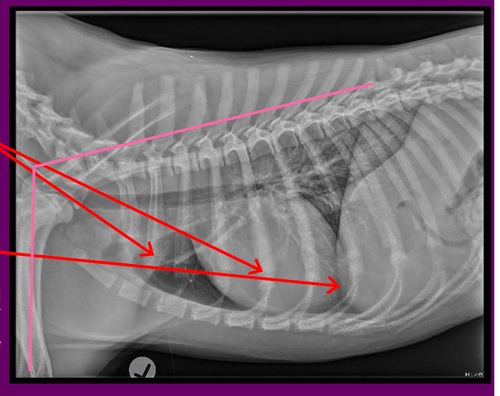
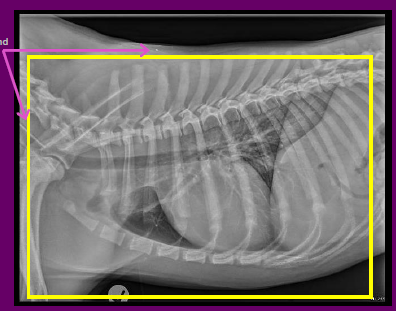
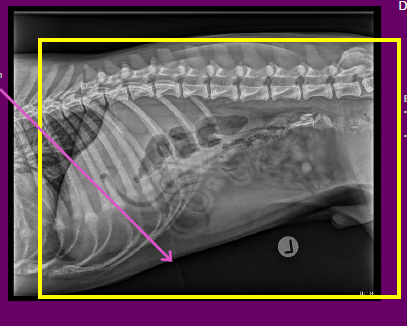
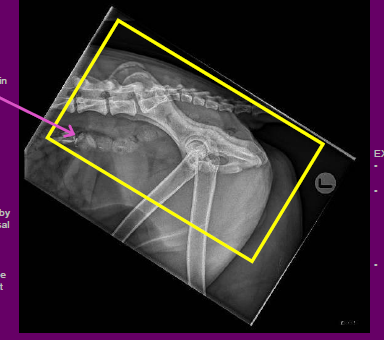
Left lateral thorax X-ray positioning
POSITIONING
Minimal rotation evidenced by costochondral junctions being nearly superimposed
Poor inspiration evidenced by superimposition of diaphragm over the heart
Forelimbs adequately extended Jade's rule of thumb: 90 degrees or more in relation to thoracic spine (pink angle)
Minimal rotation evidenced by costochondral junctions being nearly superimposed
Poor inspiration evidenced by superimposition of diaphragm over the heart
Forelimbs adequately extended Jade's rule of thumb: 90 degrees or more in relation to thoracic spine (pink angle)
69
New cards
Left lateral thorax x-ray anatomy & labelling
ANATOMY
All required anatomy is included
CRANIAL Thoracic Inlet
CAUDAL Diaphragm
VENTRAL Sternum skin margin
DORSUM Vertebral bodies
LABELLING
Correct marker
Placed in an appropriate location
All required anatomy is included
CRANIAL Thoracic Inlet
CAUDAL Diaphragm
VENTRAL Sternum skin margin
DORSUM Vertebral bodies
LABELLING
Correct marker
Placed in an appropriate location
70
New cards
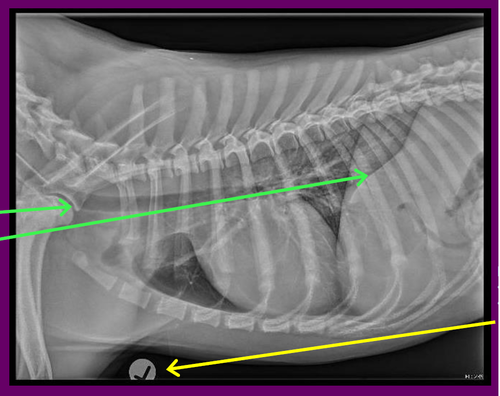
Left lateral thorax x-ray artefacts, collimation & exposure
ARTEFACTS
No unexpected artefacts
You can note the presence of ETT and Microchip COLLIMATION
Could be improved- See yellow box
EXPOSURE EI: 239 indicates underexposed
Lung markings themselves look adequately exposed
Good
No unexpected artefacts
You can note the presence of ETT and Microchip COLLIMATION
Could be improved- See yellow box
EXPOSURE EI: 239 indicates underexposed
Lung markings themselves look adequately exposed
Good
71
New cards
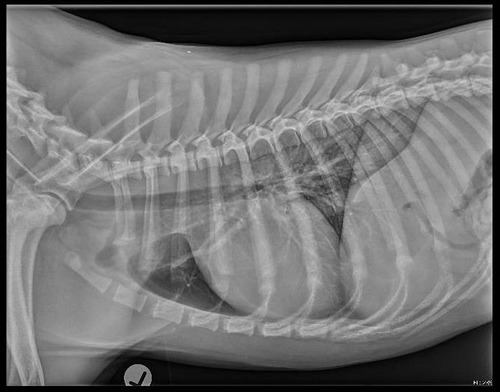
Left lateral thorax x-ray repeat?
Yes • Better inspiration required to become diagnostic quality • Note: Under a full GA peak inspiration is achieved by performing a breath hold. Under sedation you need to observe the rise and fall of the chest - timing is crucial!
72
New cards
Non-diagnostic radiographs
Poorly positioned and/or exposed radiographs cannot be accurately interpreted by the requesting veterinarian or radiologist
73
New cards
Diagnostic quality xrays
Images that are of an acceptable quality and can be accurately interpreted
74
New cards
Image viewing conventions: lateral
Lateral projections should always be orientated so that the patients nose is on the left, tail to the right
75
New cards
Image viewing conventions: Ventro-dorsal (VD/DV)
Ventro Dorsal (VD)/ Dorso Ventral (DV) views should be viewed as thought the patient is standing on their hindlimbs . The left should be on the right, and right on the left
76
New cards
Image viewing conventions: Caudal Cranial (CdCr)
Caudo Cranial ( CdCr) often preferred to be
viewed with the lateral aspect on the right
viewed with the lateral aspect on the right
77
New cards
Exposure Index (EI)
EI Value = 300
< 300-underexposed
> 300-overexposed
< 300-underexposed
> 300-overexposed
78
New cards
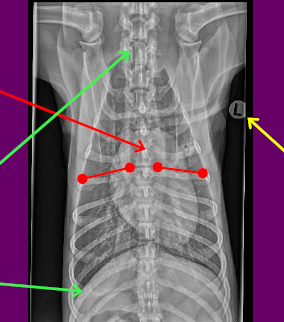
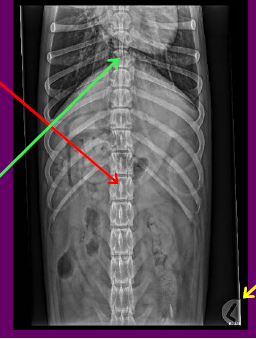
Ventro Dorsal (VD) Thorax xray: positioning anatomy labelling
POSITIONING
•No rotation evidenced by sternum being superimposed over the spine
•You can also assess this by the spinous processes sitting in the middle of the vertebral bodies or symmetry in the length of the ribs
ANATOMY
•All required anatomy is included
•CRANIAL Thoracic Inlet
•CAUDAL Diaphragm
•LATERALLY Skin margins
LABELLING
•Correct marker
•Placed in appropriate location
•No rotation evidenced by sternum being superimposed over the spine
•You can also assess this by the spinous processes sitting in the middle of the vertebral bodies or symmetry in the length of the ribs
ANATOMY
•All required anatomy is included
•CRANIAL Thoracic Inlet
•CAUDAL Diaphragm
•LATERALLY Skin margins
LABELLING
•Correct marker
•Placed in appropriate location
79
New cards
Ventro Dorsal (VD) Thorax xray: artefacts collimation exposure repeat?
ARTEFACTS
• No unexpected artefacts
•You can note the presence Microchip
COLLIMATION
•Could be improved
•See yellow box
EXPOSURE
•EI: 169 indicates underexposed
•Lung markings themselves look adequately exposed
•Good
REPEAT
No
•This image is of acceptable radiographic quality
• No unexpected artefacts
•You can note the presence Microchip
COLLIMATION
•Could be improved
•See yellow box
EXPOSURE
•EI: 169 indicates underexposed
•Lung markings themselves look adequately exposed
•Good
REPEAT
No
•This image is of acceptable radiographic quality

80
New cards
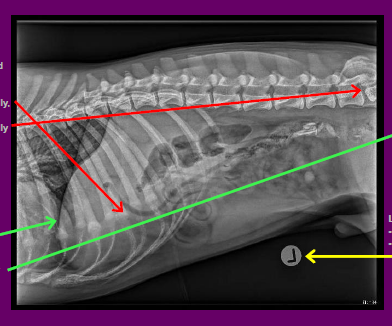
Left lateral abdomen xray positioning anatomy labelling
POSITIONING
•No rotation evidenced by the costochondral
junctions being superimposed cranially, and wings of ilium superimposed caudally
ANATOMY
•Not all required anatomy is included
•CRANIAL Diaphragm
•CAUDAL Greater Trochanter **missing**
•VENTRAL Skin margins
•DORSAL Spine
LABELLING
•Correct marker
•Placed in appropriate location
•No rotation evidenced by the costochondral
junctions being superimposed cranially, and wings of ilium superimposed caudally
ANATOMY
•Not all required anatomy is included
•CRANIAL Diaphragm
•CAUDAL Greater Trochanter **missing**
•VENTRAL Skin margins
•DORSAL Spine
LABELLING
•Correct marker
•Placed in appropriate location
81
New cards
Left lateral abdomen xray artefacts collimation exposure repeat?
ARTEFACTS
•Slight artefact from positioning foam
•Not detrimental to image quality
COLLIMATION
•If possible, collimate to include greater trochanter
•If dog is larger than the size of the imaging plate, two
exposures are required
EXPOSURE
•EI: 120 indicates underexposure
•Good abdominal serosal detail
REPEAT?
•Yes
•This image is of acceptable radiographic quality, BUT, we need another radiograph to include the full abdomen (ie, greater trochanter at the caudal portion of the image)
•Slight artefact from positioning foam
•Not detrimental to image quality
COLLIMATION
•If possible, collimate to include greater trochanter
•If dog is larger than the size of the imaging plate, two
exposures are required
EXPOSURE
•EI: 120 indicates underexposure
•Good abdominal serosal detail
REPEAT?
•Yes
•This image is of acceptable radiographic quality, BUT, we need another radiograph to include the full abdomen (ie, greater trochanter at the caudal portion of the image)
82
New cards
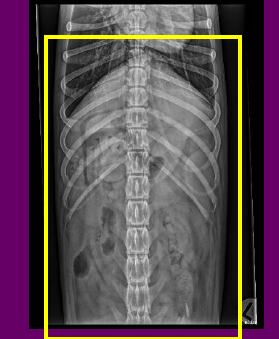
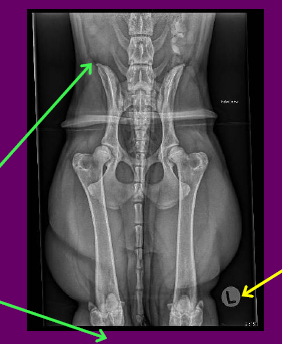
Ventro Dorsal (VD) Abdomen P.A.L.
POSITIONING
•No rotation cranially evidenced by the spinous process of the cranial lumbar vertebrae being central in the vertebral bodies
ANATOMY
• Not all required anatomy is included
• CRANIAL Diaphragm
• CAUDAL Greater Trochanter
• VENTRAL Skin margins
• LATERALLY Skin Margins
LABELLING
• Correct marker
• Placed in appropriate location
•No rotation cranially evidenced by the spinous process of the cranial lumbar vertebrae being central in the vertebral bodies
ANATOMY
• Not all required anatomy is included
• CRANIAL Diaphragm
• CAUDAL Greater Trochanter
• VENTRAL Skin margins
• LATERALLY Skin Margins
LABELLING
• Correct marker
• Placed in appropriate location
83
New cards
Ventro Dorsal (VD) Abdomen A.C.E.R?
ARTEFACTS
•None present
COLLIMATION
•If possible, collimation should be adjusted to include the greater trochanters
EXPOSURE
•EI: 413 indicates overexposure
•Good abdominal serosal detail
REPEAT?
•Yes
•This image is of acceptable radiographic quality, BUT,
we need another radiograph to include the full abdomen (ie, greater trochanter and caudal border of the image)
•None present
COLLIMATION
•If possible, collimation should be adjusted to include the greater trochanters
EXPOSURE
•EI: 413 indicates overexposure
•Good abdominal serosal detail
REPEAT?
•Yes
•This image is of acceptable radiographic quality, BUT,
we need another radiograph to include the full abdomen (ie, greater trochanter and caudal border of the image)
84
New cards
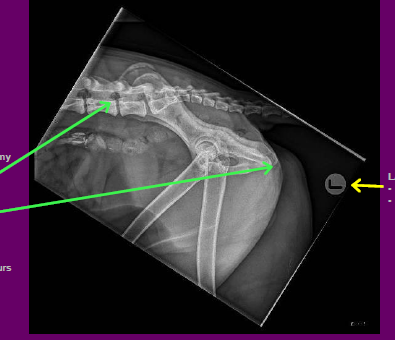
Left lateral pelvis xray P.A.L.
POSITIONING
•Slight rotation evident by lack of superimposition of the
acetabulum
ANATOMY
•All required anatomy is included
•CRANIAL Ilium
•CAUDAL Ischium
•DORSAL Skin margins
•VENTRAL 1/3 Proximal Femurs
LABELLING
•Correct marker
•Placed in appropriate location
•Slight rotation evident by lack of superimposition of the
acetabulum
ANATOMY
•All required anatomy is included
•CRANIAL Ilium
•CAUDAL Ischium
•DORSAL Skin margins
•VENTRAL 1/3 Proximal Femurs
LABELLING
•Correct marker
•Placed in appropriate location
85
New cards
Left lateral pelvis xray A.C.E.R?
ARTEFACTS
•No Unexpected artefacts
• Can make note of radiopaque shards in
the colon likely ingested bones
COLLIMATION
• Could be improved by centering more dorsal
over the palpable greater trochanters and reducing
collimated field in the dorso /ventral aspect
•See yellow box
EXPOSURE
• EI: 113 indicates underexposed
•Slight grainy appearance through the acetabulum, though joints are visible and detail is preserved
•Good, though slightly underexposed
REPEAT?
•No
•This image is of acceptable radiographic
quality
•It is not perfect, but it is diagnostic
•No Unexpected artefacts
• Can make note of radiopaque shards in
the colon likely ingested bones
COLLIMATION
• Could be improved by centering more dorsal
over the palpable greater trochanters and reducing
collimated field in the dorso /ventral aspect
•See yellow box
EXPOSURE
• EI: 113 indicates underexposed
•Slight grainy appearance through the acetabulum, though joints are visible and detail is preserved
•Good, though slightly underexposed
REPEAT?
•No
•This image is of acceptable radiographic
quality
•It is not perfect, but it is diagnostic
86
New cards
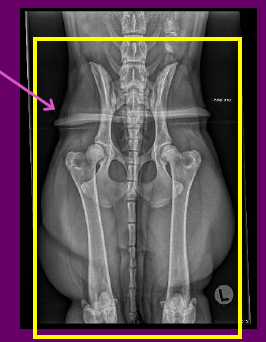
Extended Ventro Dorsal (VD) Pelvis P.A.L.
POSITIONING
•No rotation of the pelvis evident by symmetry of the ilium and obturator foramen
•The left femur is extended well with the patella nicely centred over the distal femur
• The right femur is slightly adducted and internally rotated as the patella is sitting medially over the distal femur
ANATOMY
•Not all anatomy required is included
•CRANIAL Ilium
•CAUDAL Stifle joint **MISSING*
•LATERALLY Skin margins
LABELLING
•Correct marker
•Placed in appropriate location
•No rotation of the pelvis evident by symmetry of the ilium and obturator foramen
•The left femur is extended well with the patella nicely centred over the distal femur
• The right femur is slightly adducted and internally rotated as the patella is sitting medially over the distal femur
ANATOMY
•Not all anatomy required is included
•CRANIAL Ilium
•CAUDAL Stifle joint **MISSING*
•LATERALLY Skin margins
LABELLING
•Correct marker
•Placed in appropriate location
87
New cards
Extended Ventro Dorsal (VD) Pelvis A.C.E
ARTEFACTS
•Artefact present from our tying technique
and foam underpad
COLLIMATION
•Could be improved by centring more distal to
include the entire field of interest
•See yellow box
EXPOSURE
•EI: 151 indicates under exposed
• Some grainy tissue can be seen in the caudal
abdomen but his is not our region of interest
•Good bony detail
•Good
REPEAT?
•Yes
•We need to include the stifle joints and abduct
and externally rotate the right femur
•Artefact present from our tying technique
and foam underpad
COLLIMATION
•Could be improved by centring more distal to
include the entire field of interest
•See yellow box
EXPOSURE
•EI: 151 indicates under exposed
• Some grainy tissue can be seen in the caudal
abdomen but his is not our region of interest
•Good bony detail
•Good
REPEAT?
•Yes
•We need to include the stifle joints and abduct
and externally rotate the right femur
88
New cards
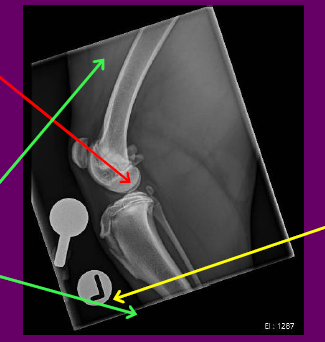
Lateral left stifle P.A.L.
POSITIONING
•Minimal rotation of the femur evidenced by the lateral and medial condyles not being entirely superimposed
ANATOMY
• All required anatomy is included
• DORSAL Distal 1/3 Femur
• VENTRAL Proximal 1/3 Tibia/Fibula
• CRANIAL Skin Margins
• CAUDAL Skin margins
LABELLING
•Correct marker
•Appropriate position
•Minimal rotation of the femur evidenced by the lateral and medial condyles not being entirely superimposed
ANATOMY
• All required anatomy is included
• DORSAL Distal 1/3 Femur
• VENTRAL Proximal 1/3 Tibia/Fibula
• CRANIAL Skin Margins
• CAUDAL Skin margins
LABELLING
•Correct marker
•Appropriate position
89
New cards
Lateral left stifle A.C.E.R.
ARTEFACTS
•None present
•Can note presence of ball bearing. It is 25mm in diameter and is used to calibrate measuring tools for accurate surgical measurements
COLLIMATION
•Appropriate centring, could include slightly less femur
•See yellow box
EXPOSURE
•EI: 1287 indicates large overexposure
• Good bony cortical and medullary detail
•Good soft tissue detail
•Good
• Very high EI number could be explained by the amount of 'black' in the image throwing off the calculation
REPEAT?
•No
•This is image is of acceptable radiographic quality
•Note: If this were pre op for surgical
intervention ( eg , TPLO) the full Tibia/Fibula needs to
be included, the angle of the stifle joint needs to be
90degrees (or 135 for other surgeries) and the rotation of the femoral condyles would need to be addressed
•None present
•Can note presence of ball bearing. It is 25mm in diameter and is used to calibrate measuring tools for accurate surgical measurements
COLLIMATION
•Appropriate centring, could include slightly less femur
•See yellow box
EXPOSURE
•EI: 1287 indicates large overexposure
• Good bony cortical and medullary detail
•Good soft tissue detail
•Good
• Very high EI number could be explained by the amount of 'black' in the image throwing off the calculation
REPEAT?
•No
•This is image is of acceptable radiographic quality
•Note: If this were pre op for surgical
intervention ( eg , TPLO) the full Tibia/Fibula needs to
be included, the angle of the stifle joint needs to be
90degrees (or 135 for other surgeries) and the rotation of the femoral condyles would need to be addressed

90
New cards
flow meter
a device used to control the rate of oxygen being delivered in liters per minute

91
New cards
Vapourisers
Add inhalant, to maintain anaesthesia in the patient

92
New cards
Common Gas Outlet (CGO)
The o2 and inhalant exit through here towards the patient, and is where we attach our breathing system

93
New cards
Rebreathing system
Anesthetic breathing circuits in which the exhaled gas is recirculated to the patient with CO2 removed.
94
New cards
Y-piece rebreather
most common type of rebreathing circuit
95
New cards
Soda lime canister
Contains soda lime which absorbs the carbon dioxide and water vapour expired by the patient.

96
New cards
Spill valve
The valve in an anesthesia ventilator that allows excess gases in the breathing system to be sent to the scavenging system after the bellows or piston has become fully filled during exhalation.

97
New cards
Non-rebreathing system
Anesthetic breathing circuits in which exhaled gases are discharged to the environment and do not pass back to the patient. co2 is removed by a high flow rate
98
New cards
Radiation dosemeter
A badge that is worn under your PPE lead gown to measure the dosage of radiation you are receiving
99
New cards
Radiation PPE
Only protects from scatter and never the primary beam; Lead apron, gloves, thyroid cover.
Time, distance, sheilding
Time, distance, sheilding
100
New cards
Xray Positioning- Abdo DV
Centre: Umbilicus, Midway
between last rib and pelvic inlet
Collimate:
Cranial: Last rib/ diaphragm
Caudal: Greater trochanter of
femur
Lateral: Skin edges
Trough/Sandbags to prevent
rotation
Forelimbs secured with sandbags
between last rib and pelvic inlet
Collimate:
Cranial: Last rib/ diaphragm
Caudal: Greater trochanter of
femur
Lateral: Skin edges
Trough/Sandbags to prevent
rotation
Forelimbs secured with sandbags