Apex: Cardiovascular Anatomy & Physiology
1/221
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
222 Terms
Identify the statements that BEST describe ventricular myocytes (3)
A. Hyper K increases threshold potential
B. They contain more mitochondria than skeletal myocytes
C. T tubules spread the wave of depolarization through myocardium
D. RMP is -90mv
E. Na conductance is greater than potassium conductance at rest
F. Hypo K decreases RMP
B. They contain more mitochondria than skeletal myocytes
D. RMP is -90mv
F. Hypo K decreases RMP
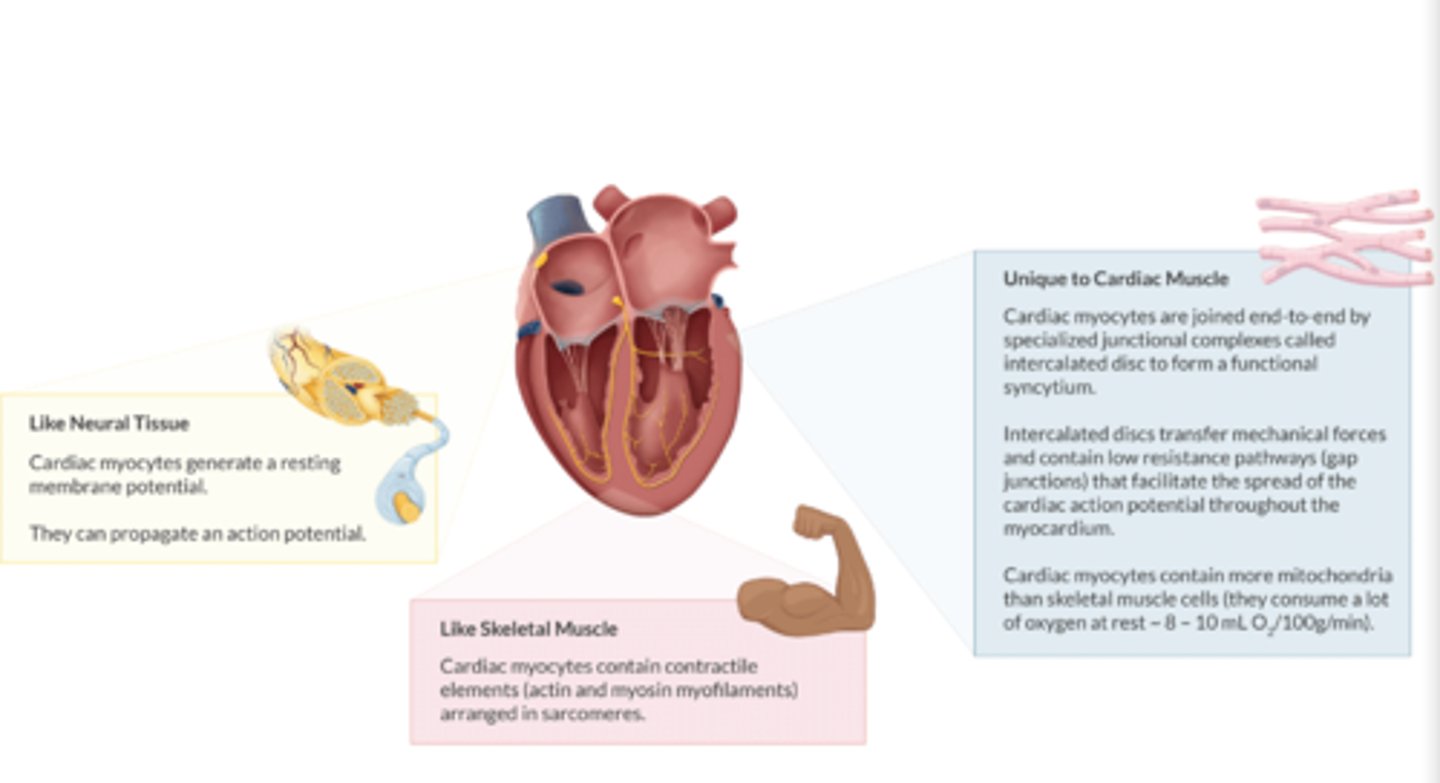
What is unique about cardiac myocytes:
1. How are they joined together?
2. do cardiac myocytes contain more or less mitochondria vs skeletal muscle cells?
3. How much O2 do cardiac myocytes consume at rest?
1. Joined by INTERCALATED DISCS & contain gap junctions to spread action potentials
2. More mitochondria than skeletal muscle cells.
3 O2 consumption at rest: 8-10 mL O2/100g/min.
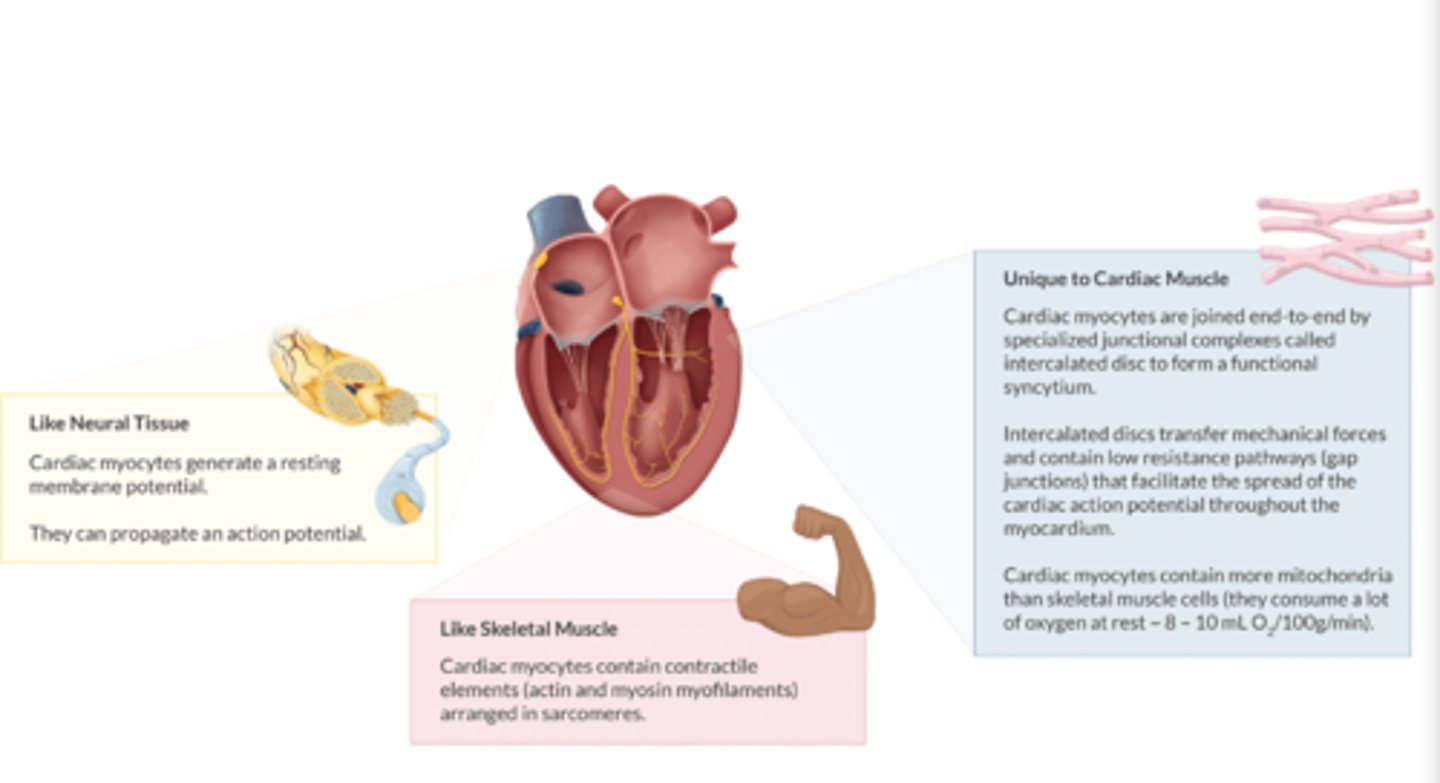
How are cardiac myocytes like neural tissue/myocytes? (2)
Both generate a resting membrane potential & propagate an action potential
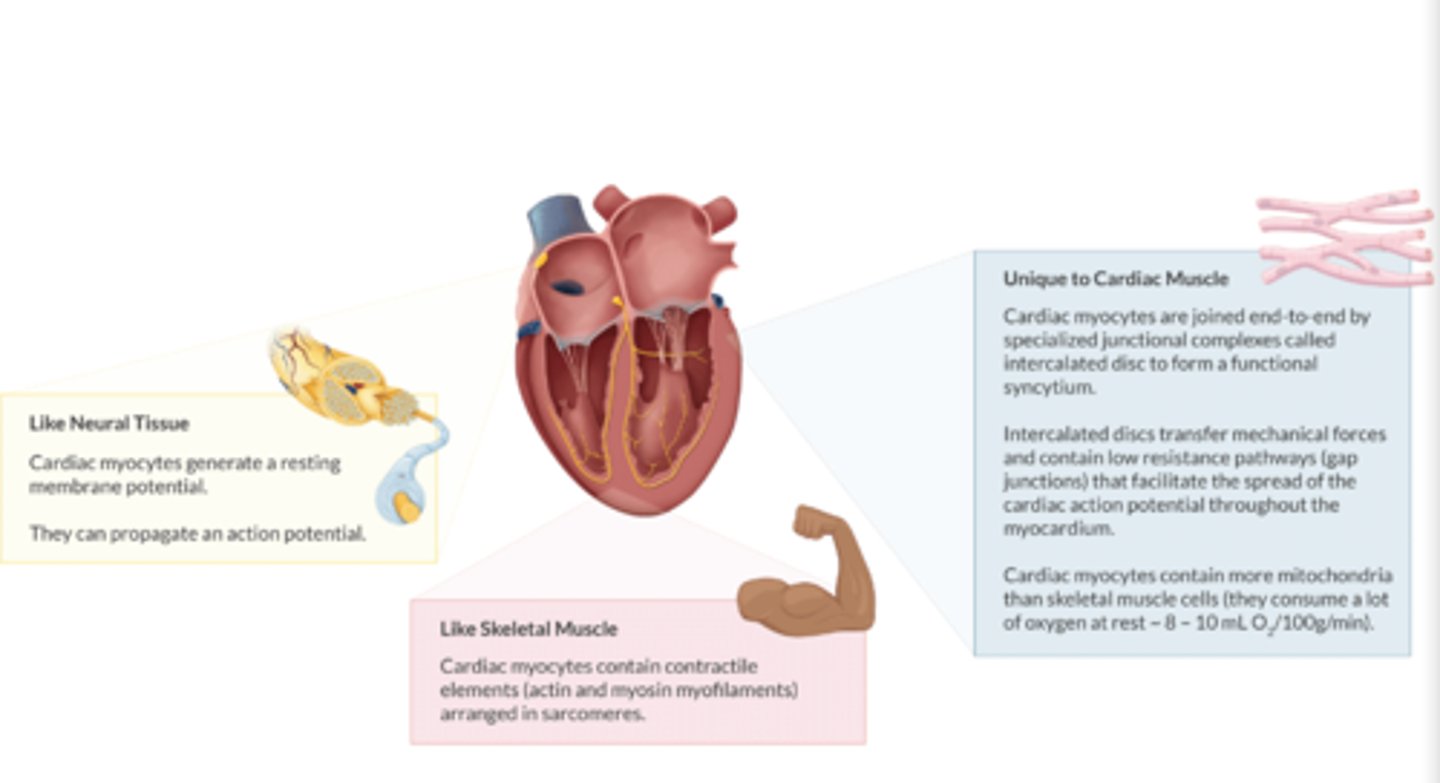
How are cardiac myocytes like skeletal tissue/myocytes? (2)
1. Both contain actin and myosin myofilaments (contractile elements)
2. arranged in sarcomeres
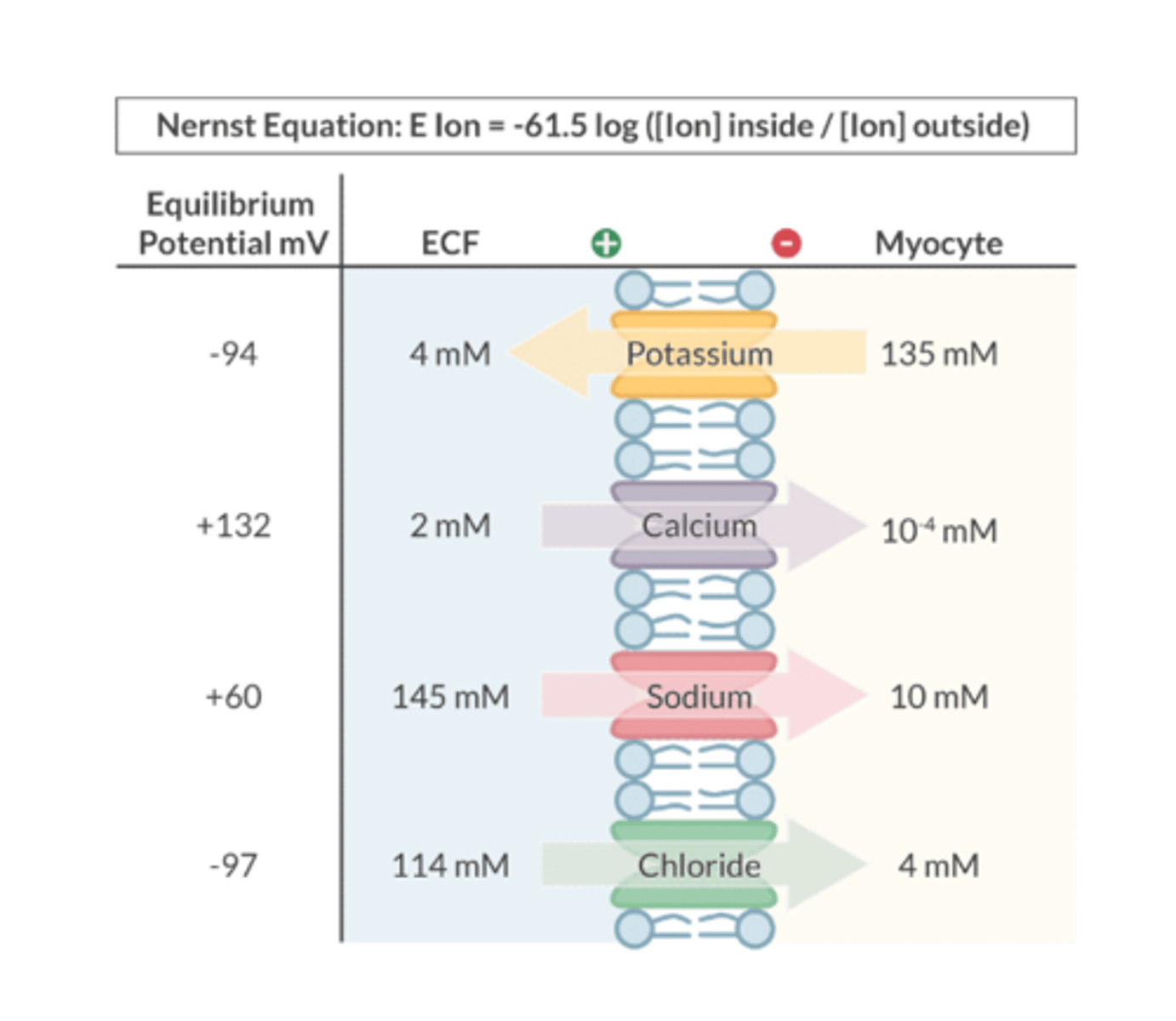
What is Equilibrium Potential?
Describes the situation where there is NO NET MOVEMENT of an ion across a cell membrane
-charge inside balances the charge on the outside
What can be used to predict an ion's equilibrium potential?
Nernst equation
Automaticity is the ability to:
Ability for the heart to generate an action potential spontaneously (via the SA node- sets the heart rate)
Excitability is the ability
- Heart responds to electrical stimulus
- Depolarizes & fires action potential
Conductance is the ability to transmit:
the ability to transmit electrical current
-Because ions are charged, they do no freely pass through cell membranes. Instead, an ion requires an open channel to cross from one side of the membrane to the other
-An open ion channel INCREASES the conductance of that ion
-A closed ion channel REDUCES the conductance of that ion
Define Inotropy
the force of myocardial contraction during systole
Define Chronotropy
heart rate
Define Dromotropy
conduction velocity through the heart
(velocity= distance/time)
Define Lusitropy
relaxation during diastole
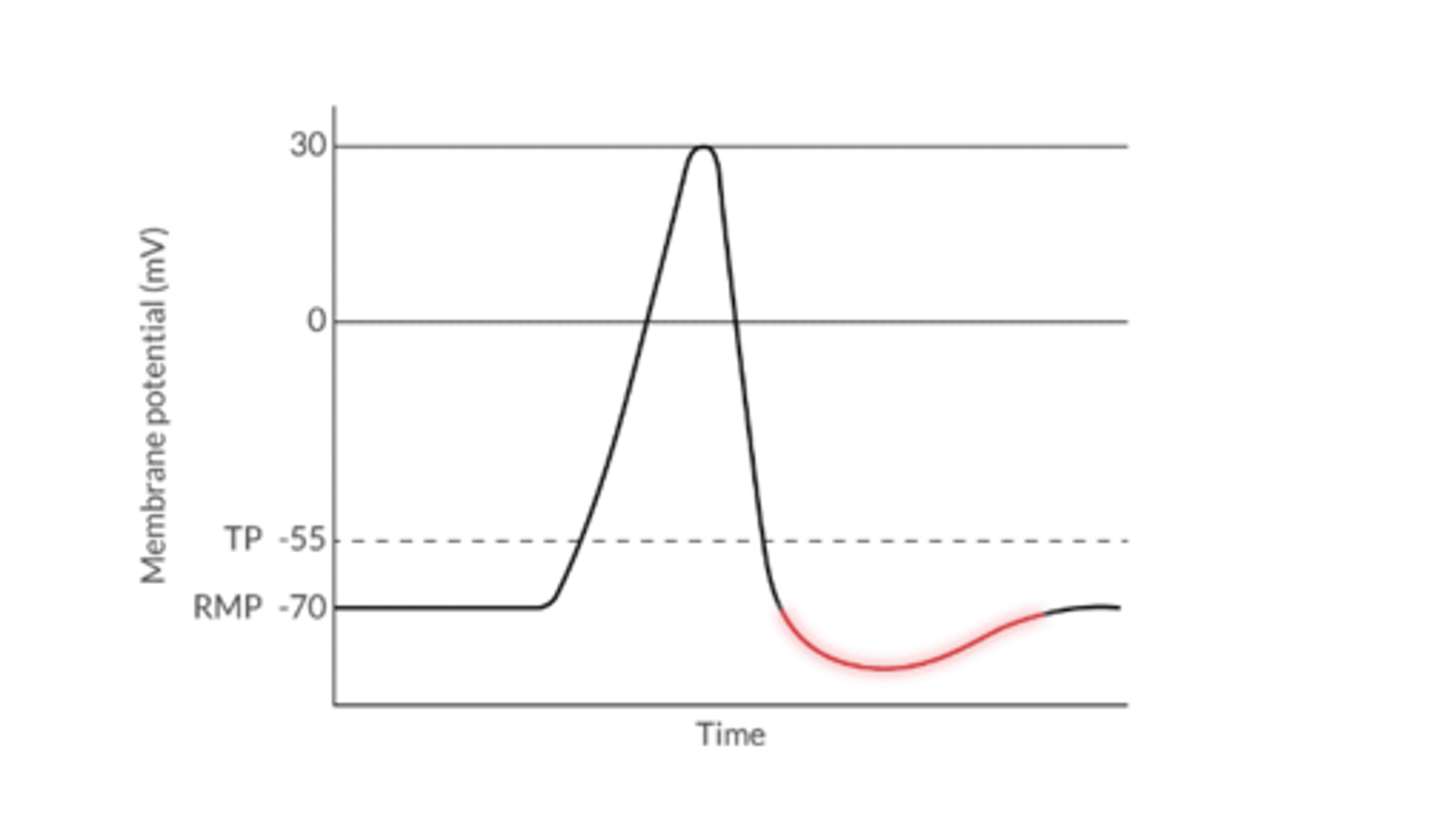
What is the Resting Membrane Potential of a Cardiac Myocyte?
The electrical potential across a cell membrane at rest (-70mV in cardiac myocyte)
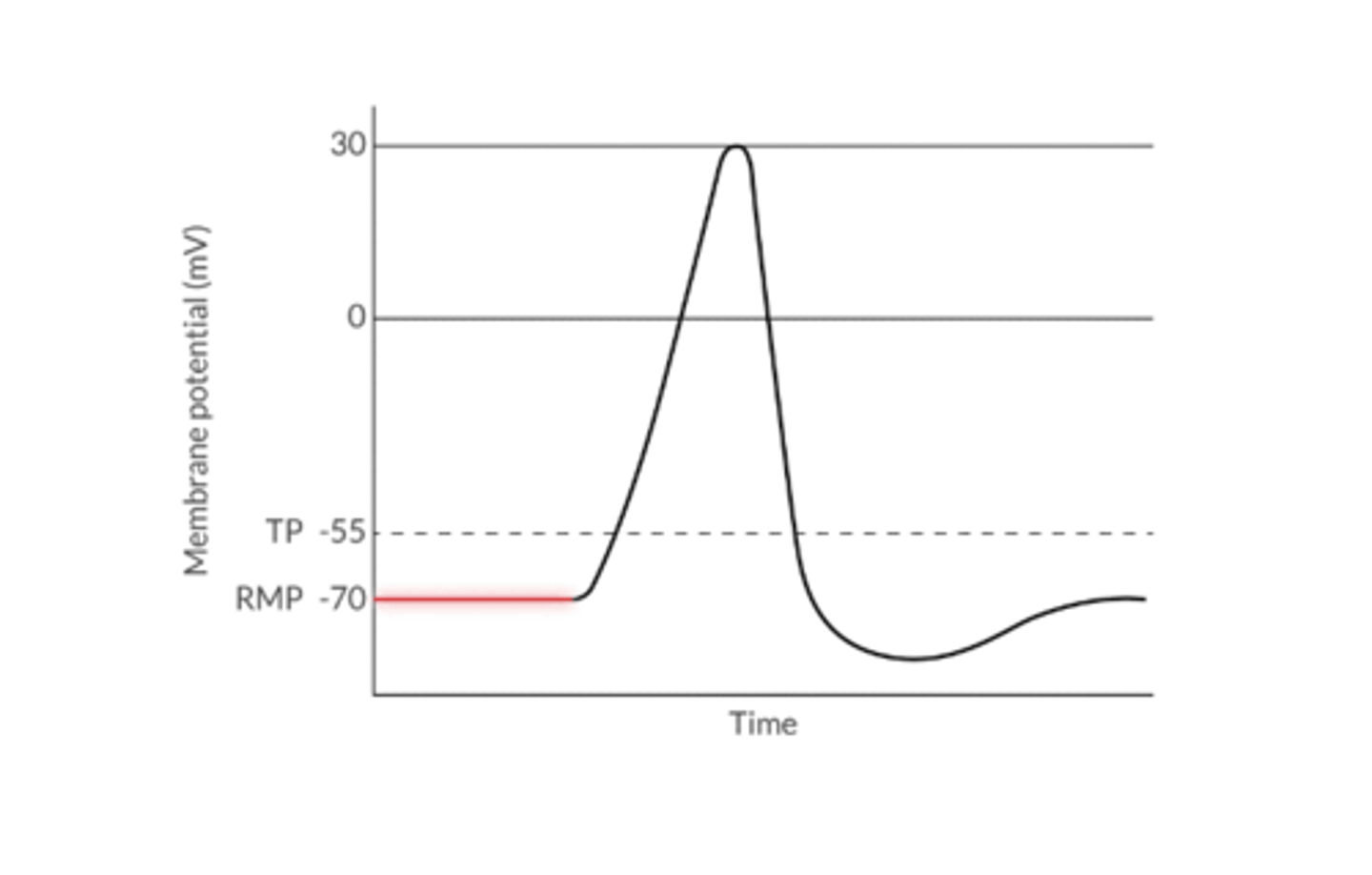
What 3 things determine the RMP?
1. Chemical force (concentration gradient)
2. Electrostatic counterforce
3. Sodium/potassium ATPase
What is the primary determinant of RMP?
SERUM K***
At rest the nerve cell continuously leaks ________
K+ (loses its positive charge)
DECREASED serum K+ --> RMP becomes more _________
NEGATIVE
INCREASED serum K+ --> RMP becomes more _________
POSITIVE
What is the Threshold Potential?
the voltage change that must occur to initiate depolarization (-55mv)
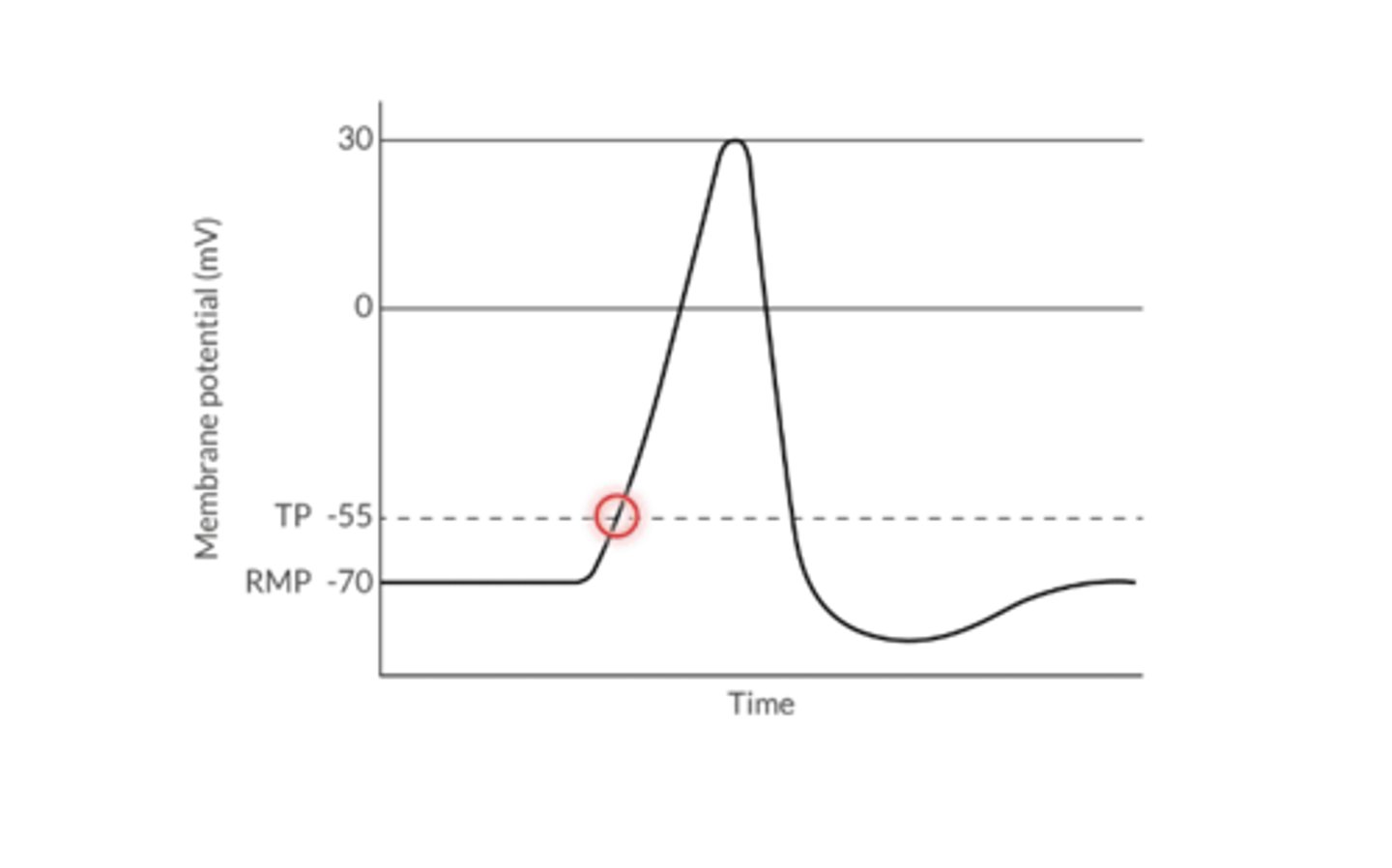
What is the primary determinant of threshold potential?
SERUM Ca+!!!
DECREASED serum Ca+--> TP becomes more ________
NEGATIVE
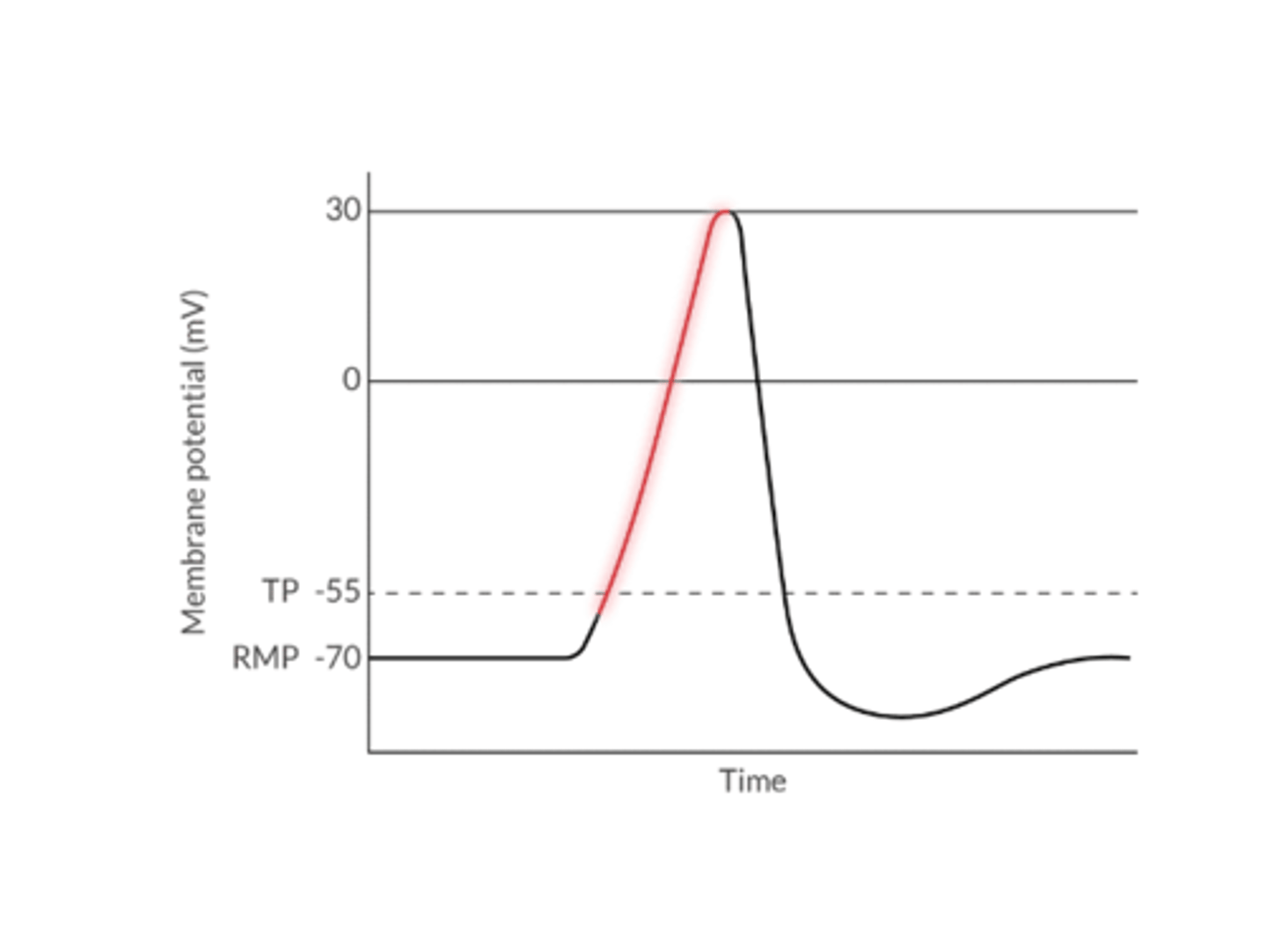
1. Depolarization describes:
2. What type of phenomenon
1. the movement of cell's membrane potential to a more positive value (less of a charge difference between inside and outside the cell)
Na+ or Ca+ enters the cell
2. All or nothing phenomenon
Results in an AP as long as the TP is achieved
What determines the ability of a cell to depolarize?
The difference between RMP and TP
When RMP is CLOSER to TP, the cell is ___________ to depolarize
EASIER
When RMP is FURTHER from TP, the cell is ___________ to depolarize
HARDER
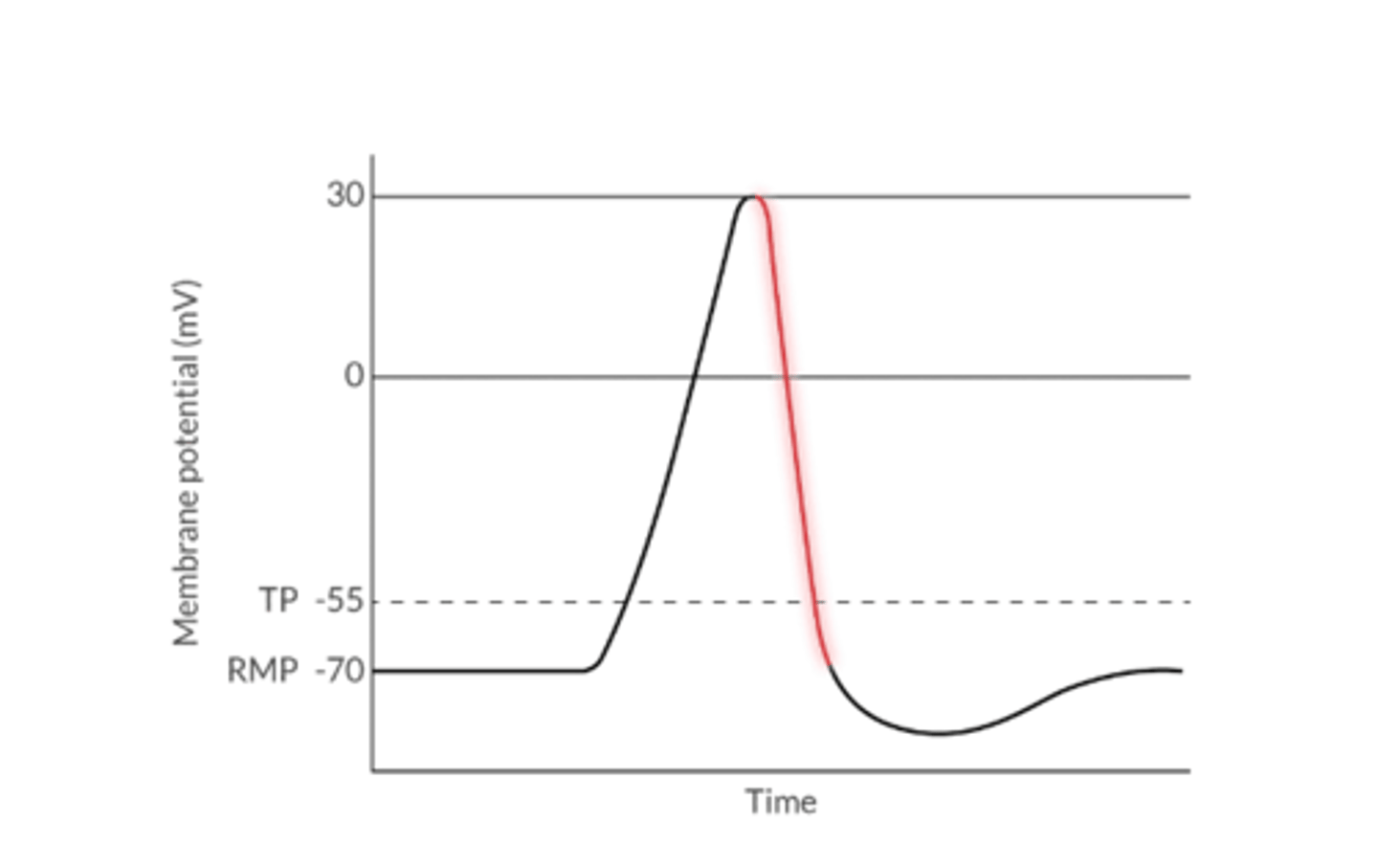
1. What is Repolarization?
2. Ion movement during this time?
3. resistant to what during this time?
1. The return of a cell's membrane potential towards a more negative value after depolarization
2. K+ leaves the cell of Cl- enters the cell
3. The cell is resistant to subsequent depolarization during the refractory period
Hyperpolarization describes what?
The movement of a cell's membrane potential to a more negative value beyond the RMP
Typically happens after repolarizations for a very short time
Because RMP is further from TP, it's more difficult to depolarize a cell that's hyperpolarized
What restores the ionic balance towards RMP in excitable tissue?
Sodium-potassium ATPase pump
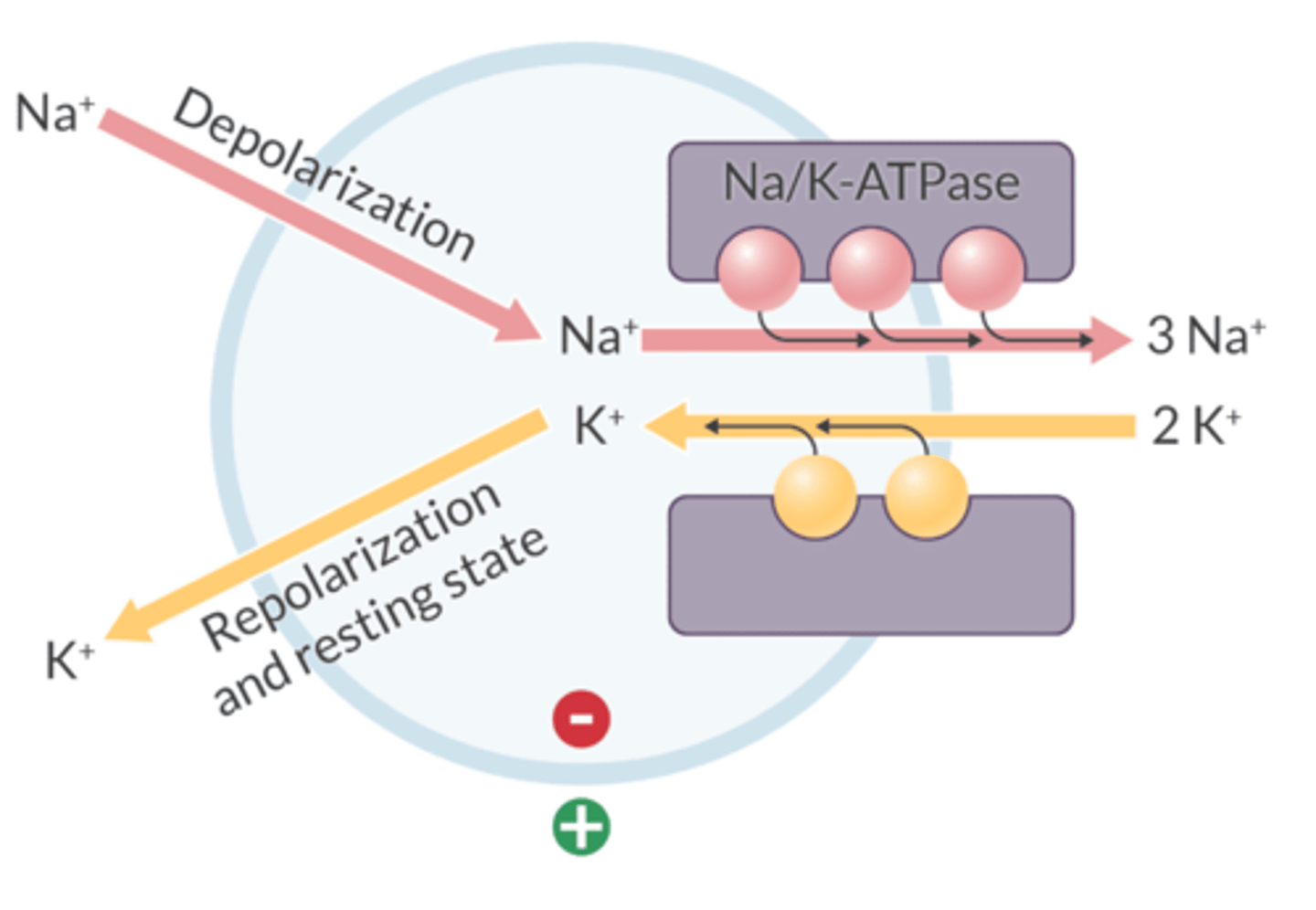
Sodium-potassium ATPase pump:
1. Ion movement with this pump?
2. Passive or active?
1. Removes 3 Na+ that enters the cell during depolarization
2. Returns 2 K+ that has left the cell during repolarization
1. For every 3 Na+ ions it removes, it brings 2 K+ into the cell
Always on
2. An ACTIVE TRANSPORT mechanism that requires ATP
What drug inhibits the Na/K-ATPase?
Digoxin
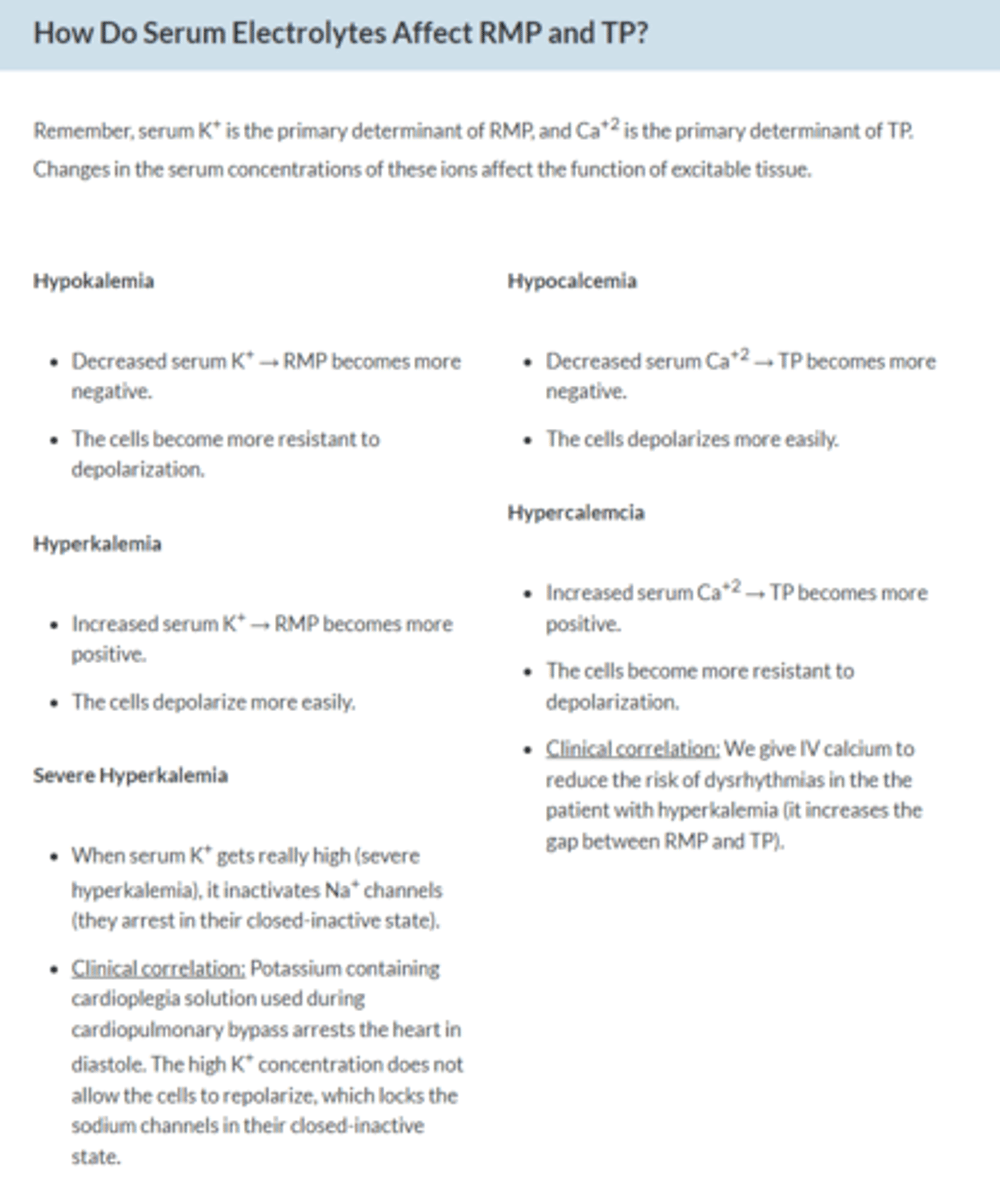
How do serum electrolytes affect RMP and TP?
1. Hypokalemia
2. Hyperkalemia
3. Hypocalcemia
4. Hypercalcemia
5.Severe hyper K
1. RMP more negative--> Cell resistant to depolarization
2. RMP more positive--> depolarize more easily
3. TP more negative--> depolarize more easily
4. TP more positive--> more resistant to depolarization
Inactivates Na channels (they arrest in their closed-inactive state) K containing cardioplegia solution used during CPB arrests the heart in diastole. The high K concentration does not allow cells to repolarize whh locks the Na channels in their closed-inactive state
Which phase of the ventricular action potentia is A/W greatest calcium conductance
A. 1
B. 2
C. 3
D. 4
B. 2
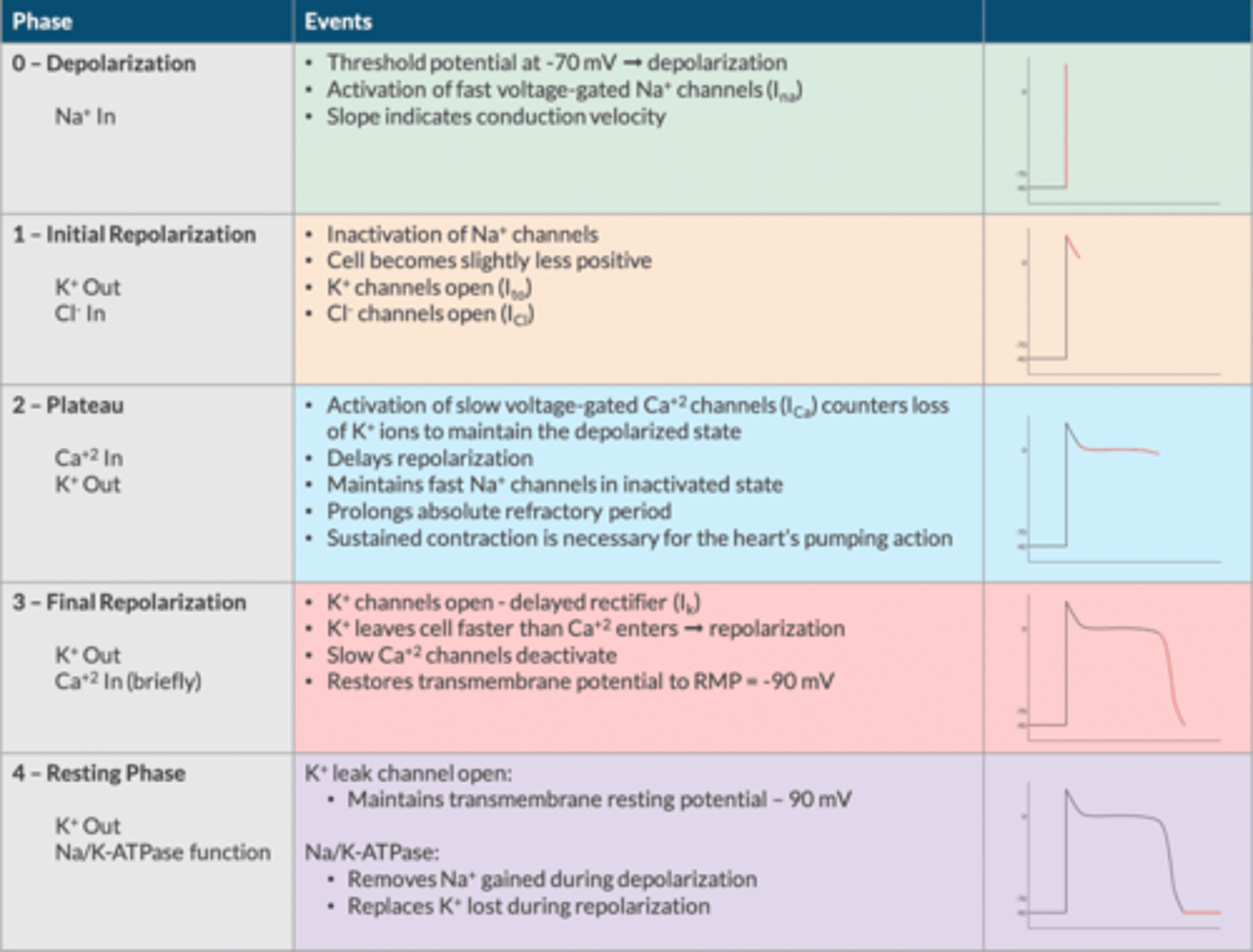
Myocyte Action Potential (The Bare Minimum):
What are the phases (5)?
Describe ion movement during each phase:
Phase 0= Depolarization: Na+ IN
Phase 1= Initial Repolarization: Cl- IN and K+ OUT
Phase 2= Plateua: Ca+ IN and K+ OUT
Phase 3= Repolarization: K+ OUT
Phase 4= Maintenance of TMP: K+ OUT and Na/K-ATPase function
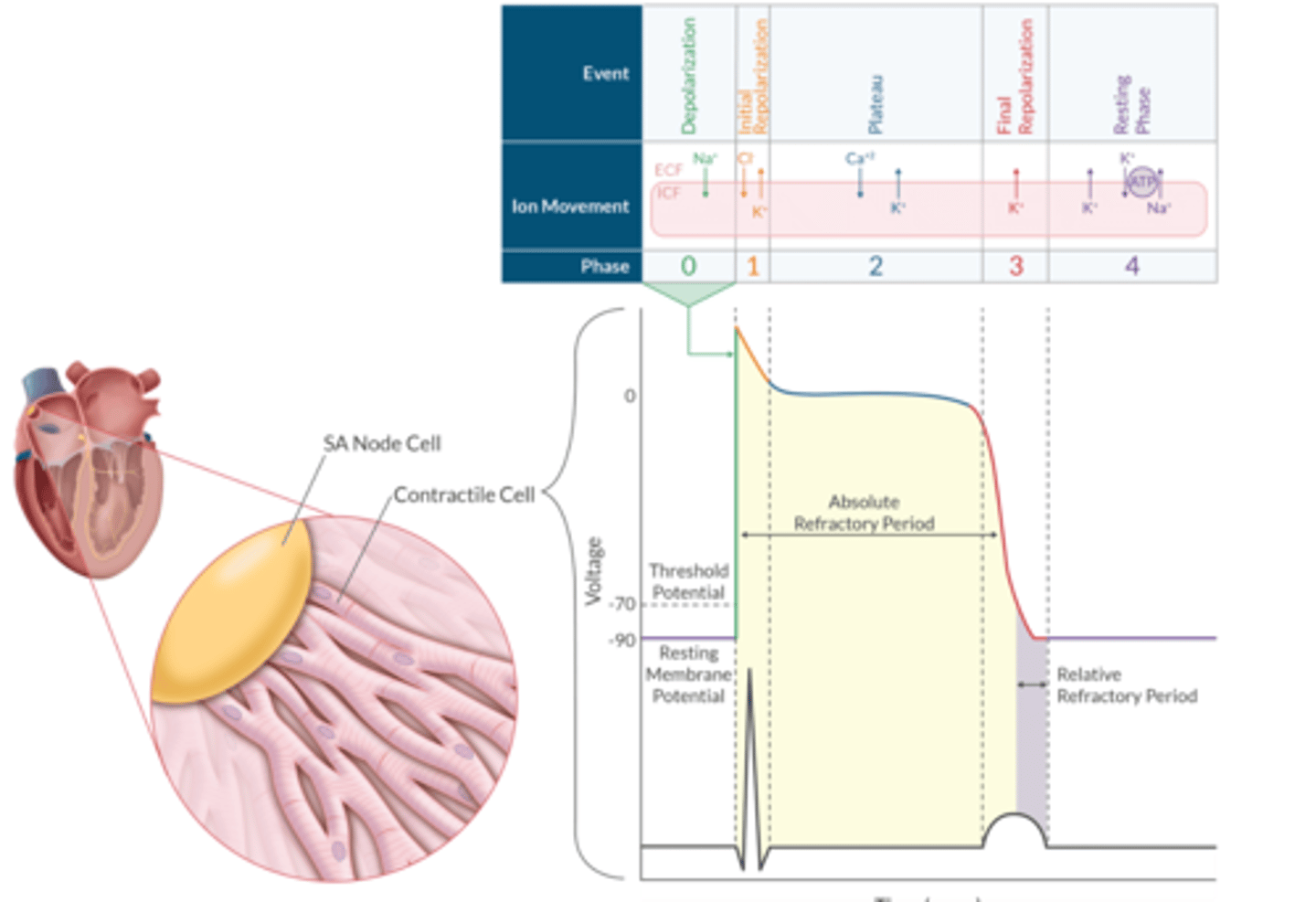
Myocyte Action Potential (Apex Chart)
Which current is responsible for spontaneous phase 4 depoloarization in SA node
A. I-Na
B. I-K
C. I-Ca
D. I-f
D. I-f
The funny current is primary determiniants of pacemaker’s intrinisc HR
Describe the Conduction Tissue AP Pathway through the Heart
SA Node--> Internodal Tracts --> AV node --> Bundle of His --> Left and Right BB --> Purkinje Fibers
SA Node Action Potential contains how many phases?
3 ( Phase 4, 0, 3)
What is the RMP for the SA node AP?
-60 mV (HIGHER!!)
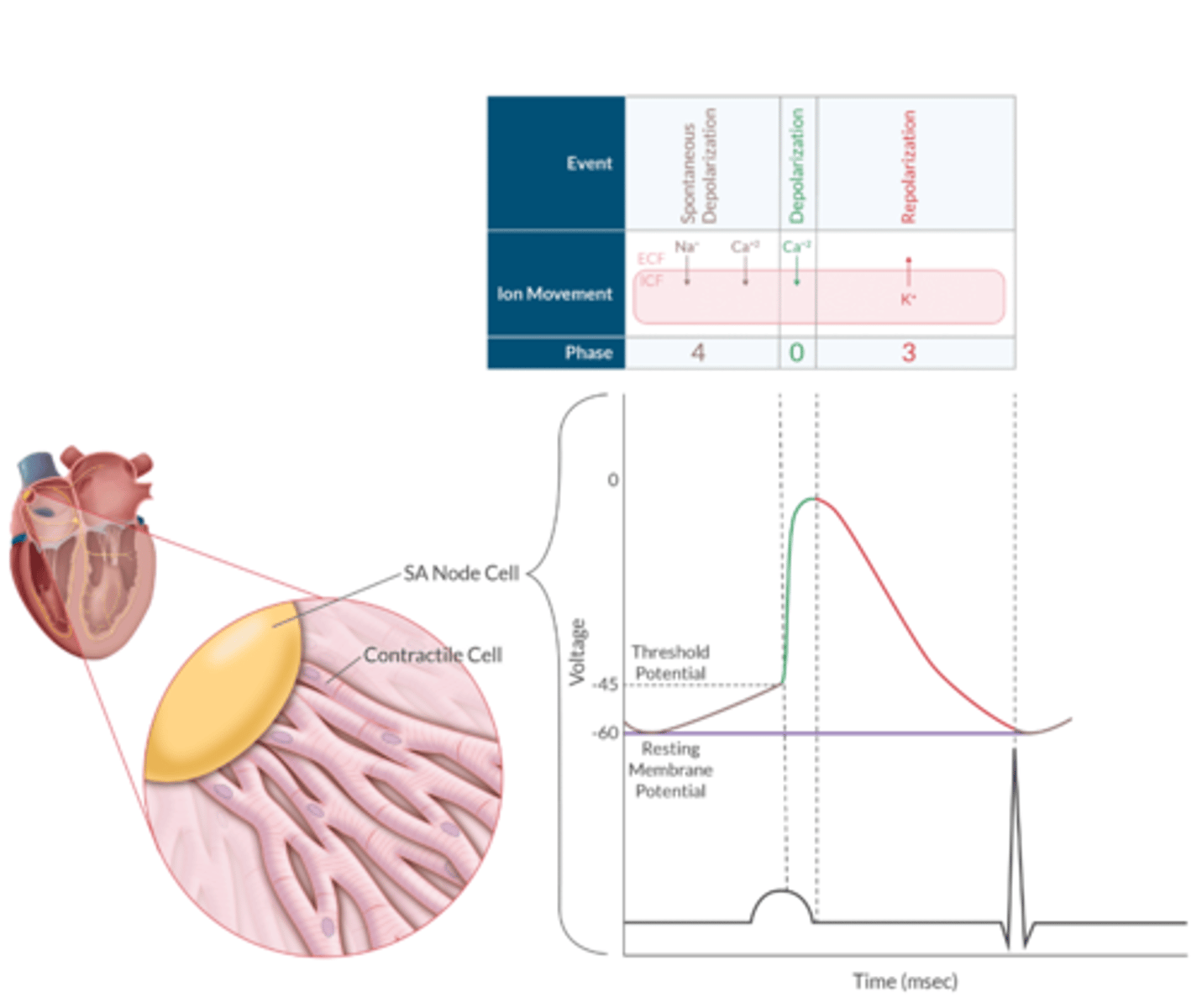
SA Node AP Apex Chart
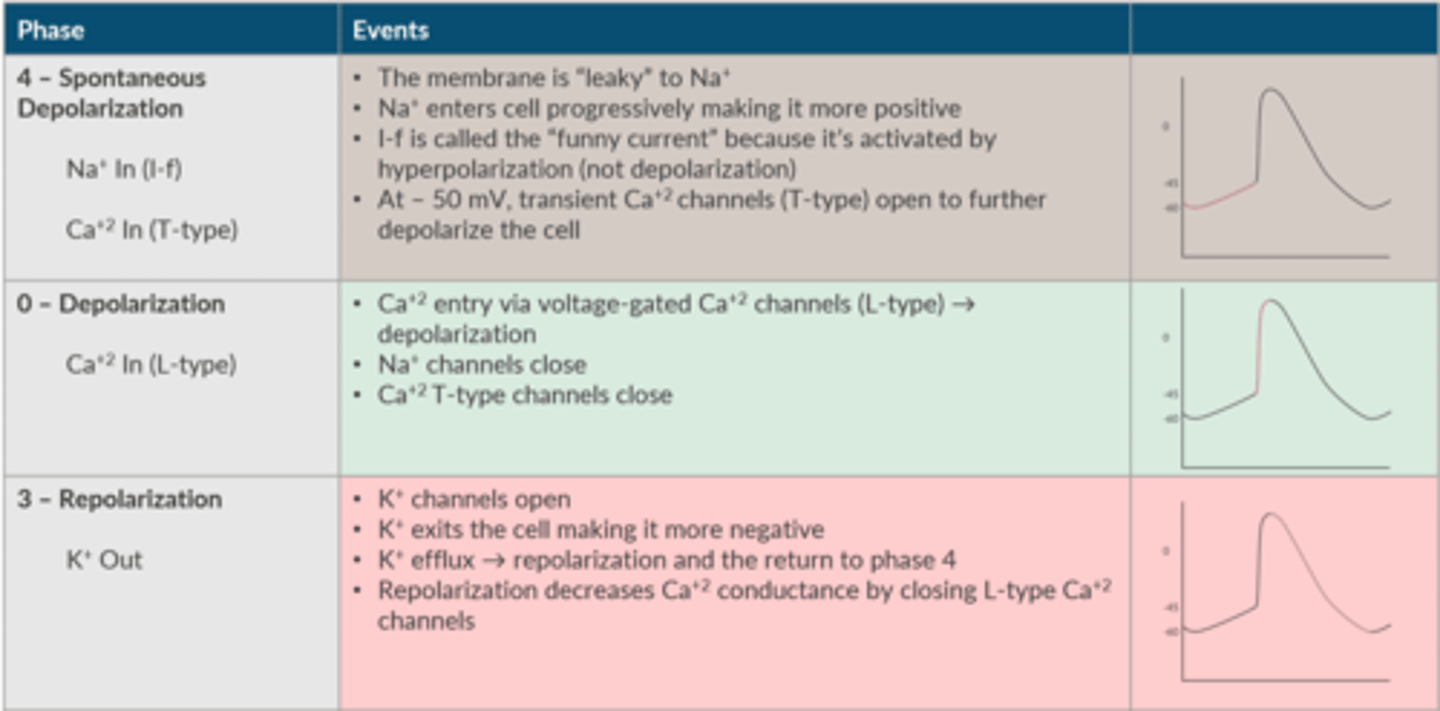
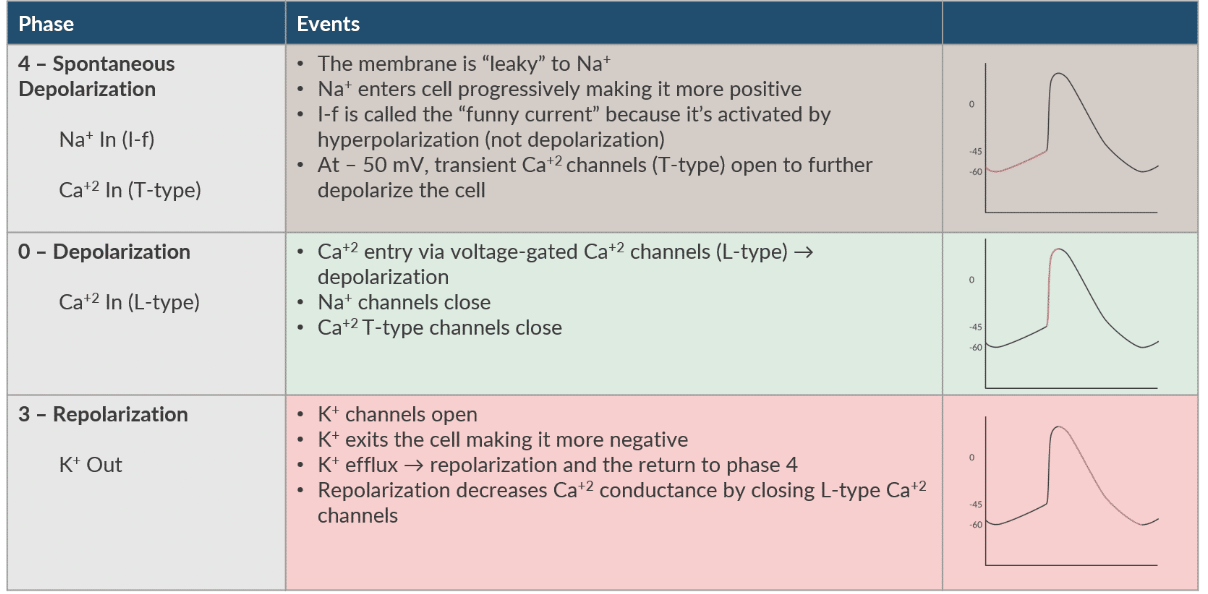
Phase 4 of SA AP is termed what?
Ion movement during this phase?
Spontaneous Depolarization ( Na+ in (I-f), Ca+ In (T-type))
- the membrane is "leaky" to Na+
-Na+ enters cell progressively making it more positive
-I-f is called the "funny current" because it's activated by hyperpolarization (NOT depolarization)
-At -50mV, transient Ca+2 channels (T-type) open to further depolarize the cell
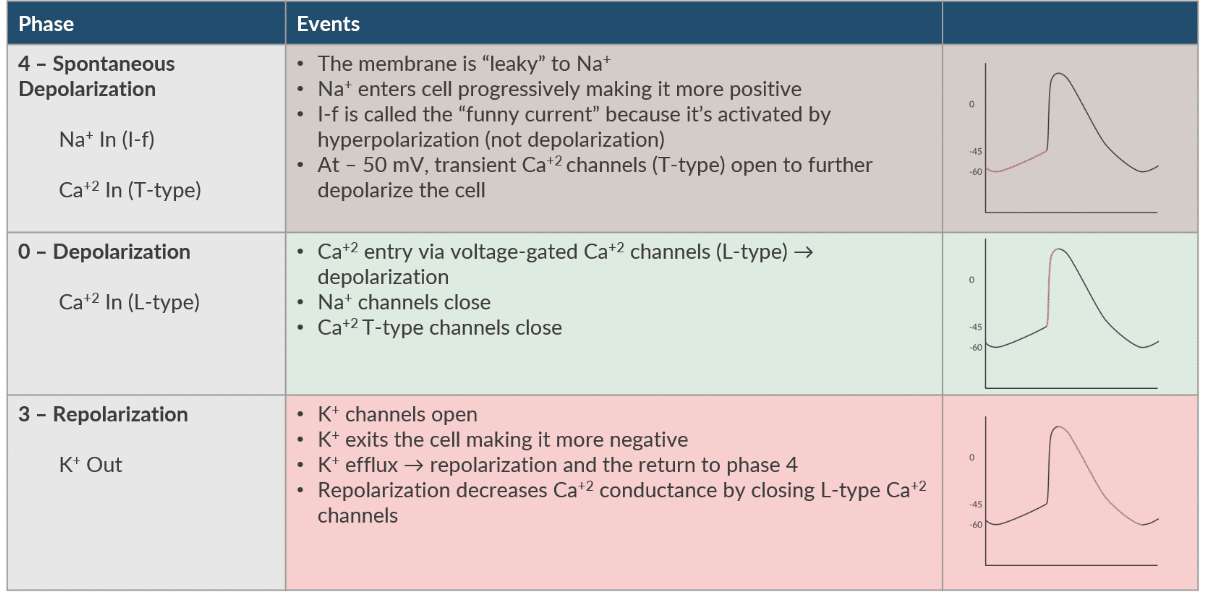
Phase 0 of SA AP?
Ion movement?
Depolarization- Ca+ In (L- type)
-Ca+2 entry via VG- Ca+2 channels (L-type)--> DEPOLARIZATION
-Na+ channels close
-Ca+2 T-type channels close
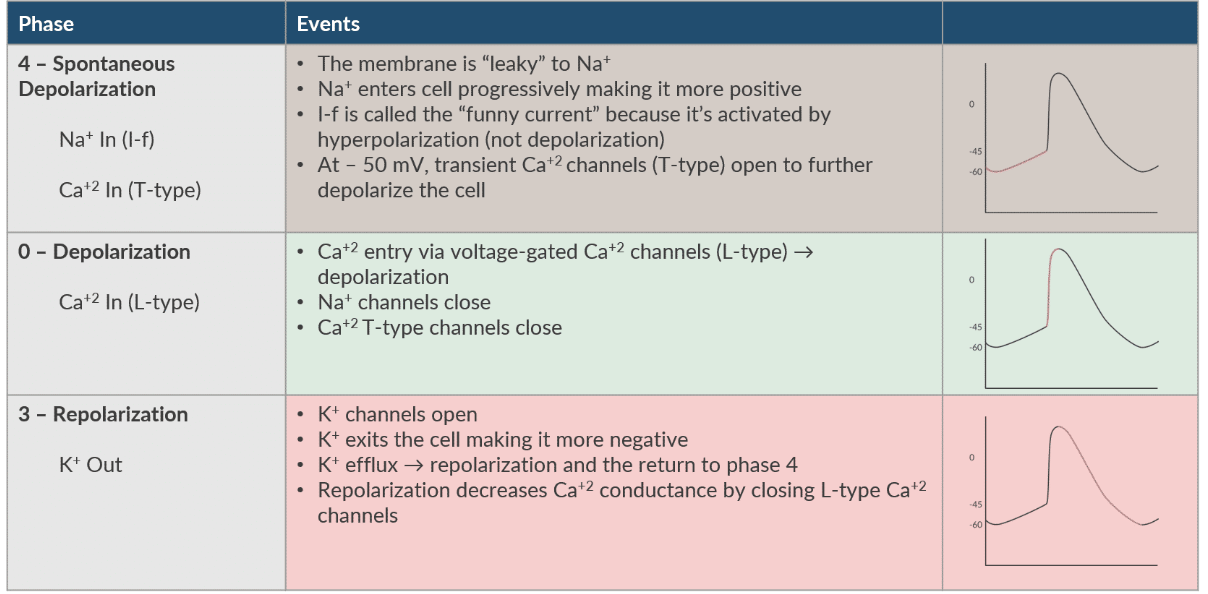
Phase 3 of SA AP
ion movement
Repolarization
-K+ channels open
-K+ exits the cell making ti more negative
-K+ efflux --> repolarization and the return to phase 4
-Repolarization decreases Ca+2 conductance by closing L-type Ca_2 channels
What helps re-establish the SA node AP gradient after repolarization?
NA/K-ATPase pump
What determines the heart rate? (2)
1. Intrinsic firing rate of the dominant pacemaker (usually the SA node)
2. Autonomic tone (At rest, PNS exceed SNS tone)
Where does the SA node reside?
in the right atrium
What is another name for the SA node?
Keith-Flack node
The rate of ___________________________ of the SA node determines the intrinsic HR
spontaneous PHASE 4 DEPOLARIZATION
What happens if disease or hypoxia of the SA node impairs it's ability to fire?
The cell with the next highest rate of spontaneous phase 4 depolarization will assume the pacemaker responsibility.
This explains why a junctional rhythm is slow and does not have a P wave. Volatile anesthetics depress SA node automaticity, which explains why these agents can cause a junctional rhythm
What innervates the SA node?
RIGHT vagus (CN 10)
What innervates the AV node?
LEFT vagus nerve
What are the cardiac accelerator fibers for SNS tone?
T1-T4
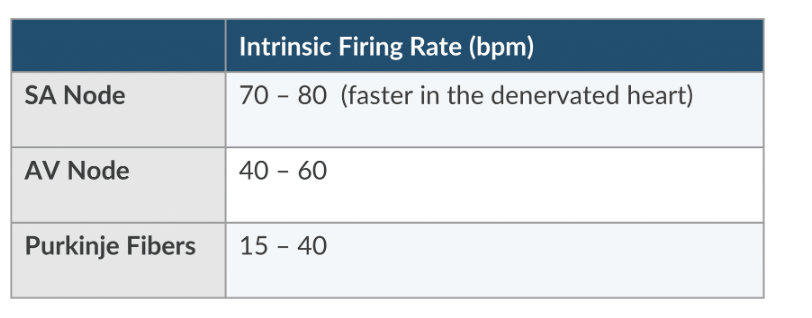
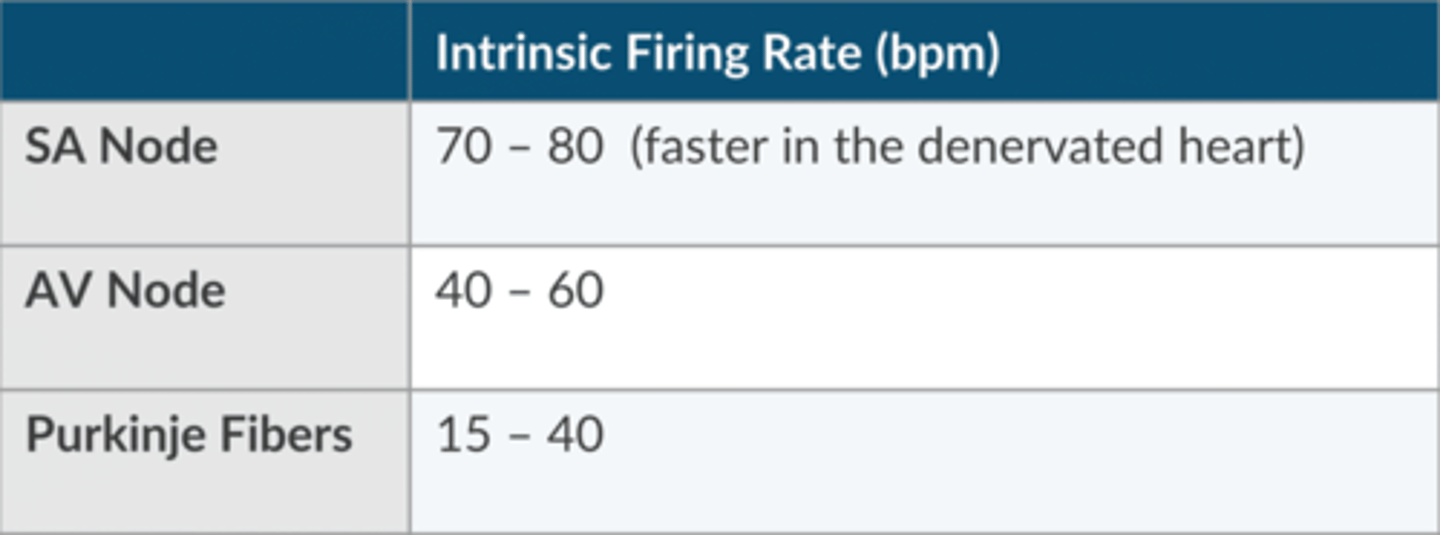
What is the normal intrinsic firing rate of the SA node?
70-80 (faster in the denervated heart) bpm
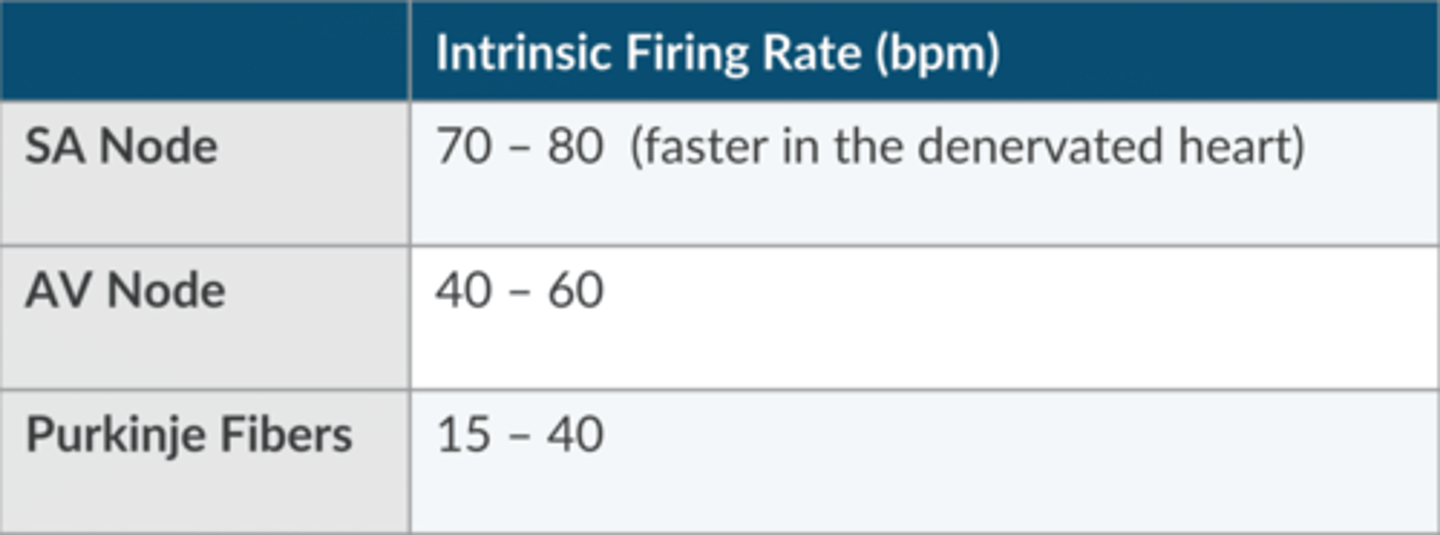
What is the normal intrinsic firing rate of the AV node?
40- 60 bpm
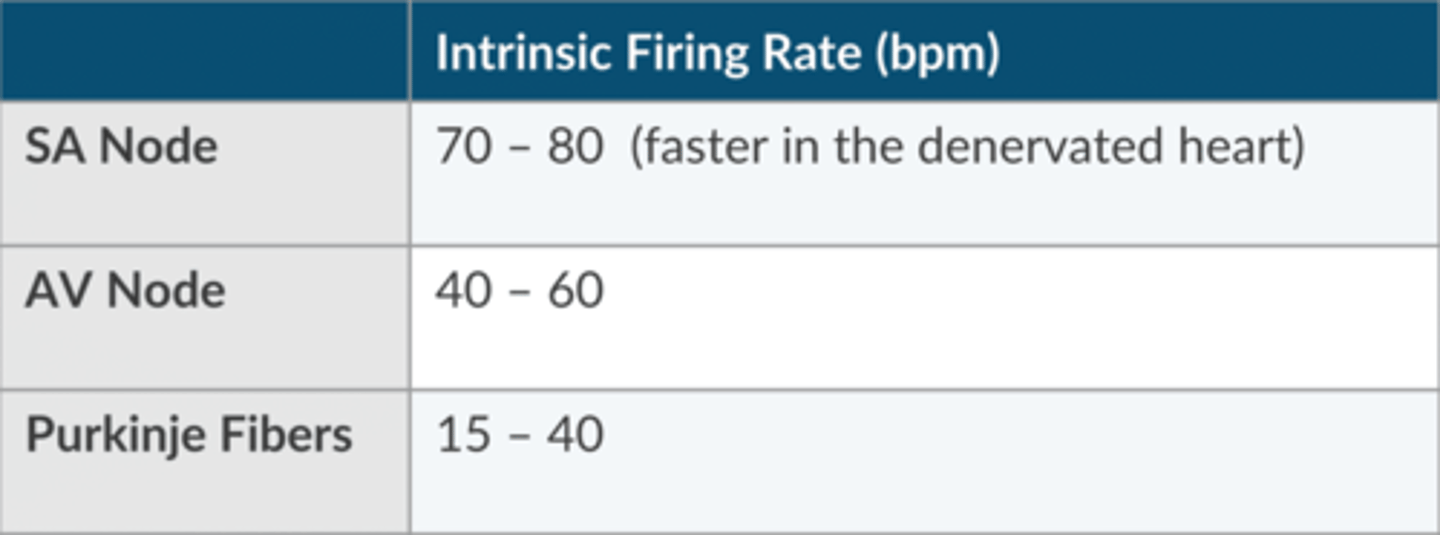
What is the normal intrinsic firing rate of the Purkinje Fibers?
15-40 bpm
What 3 variables can be manipulated to change the sinus node rate?
1. the rate of spontaneous phase 4 depolarization
2. Threshold potential
3. RMP
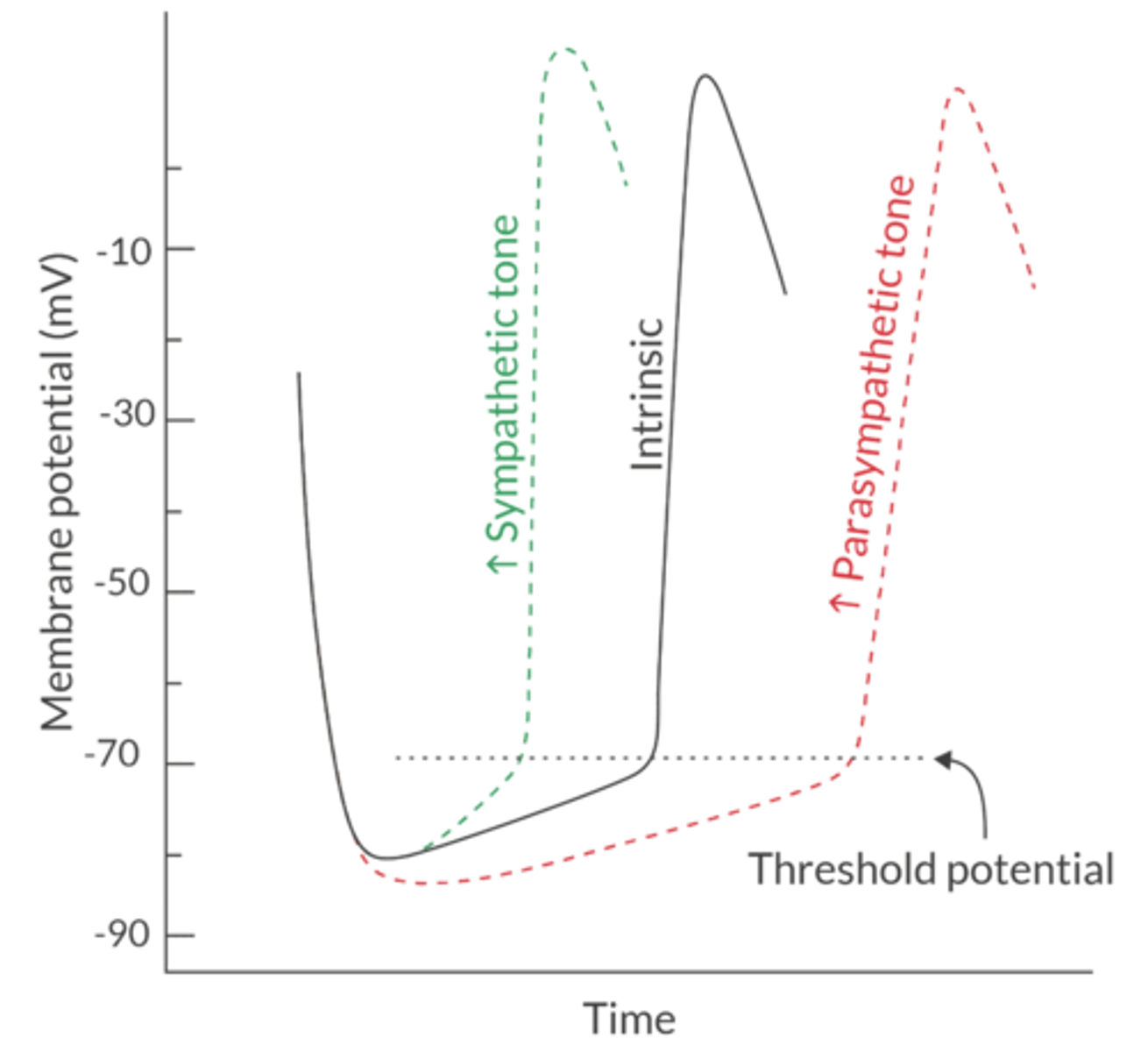
How does SNS autonomic tone affect HR?
NOREPINEPHRINE stimulates beta-1, which INCREASES HR by increasing NA+ and Ca+ conductance
This increases the slope of spontaneous phase 4 depolarization
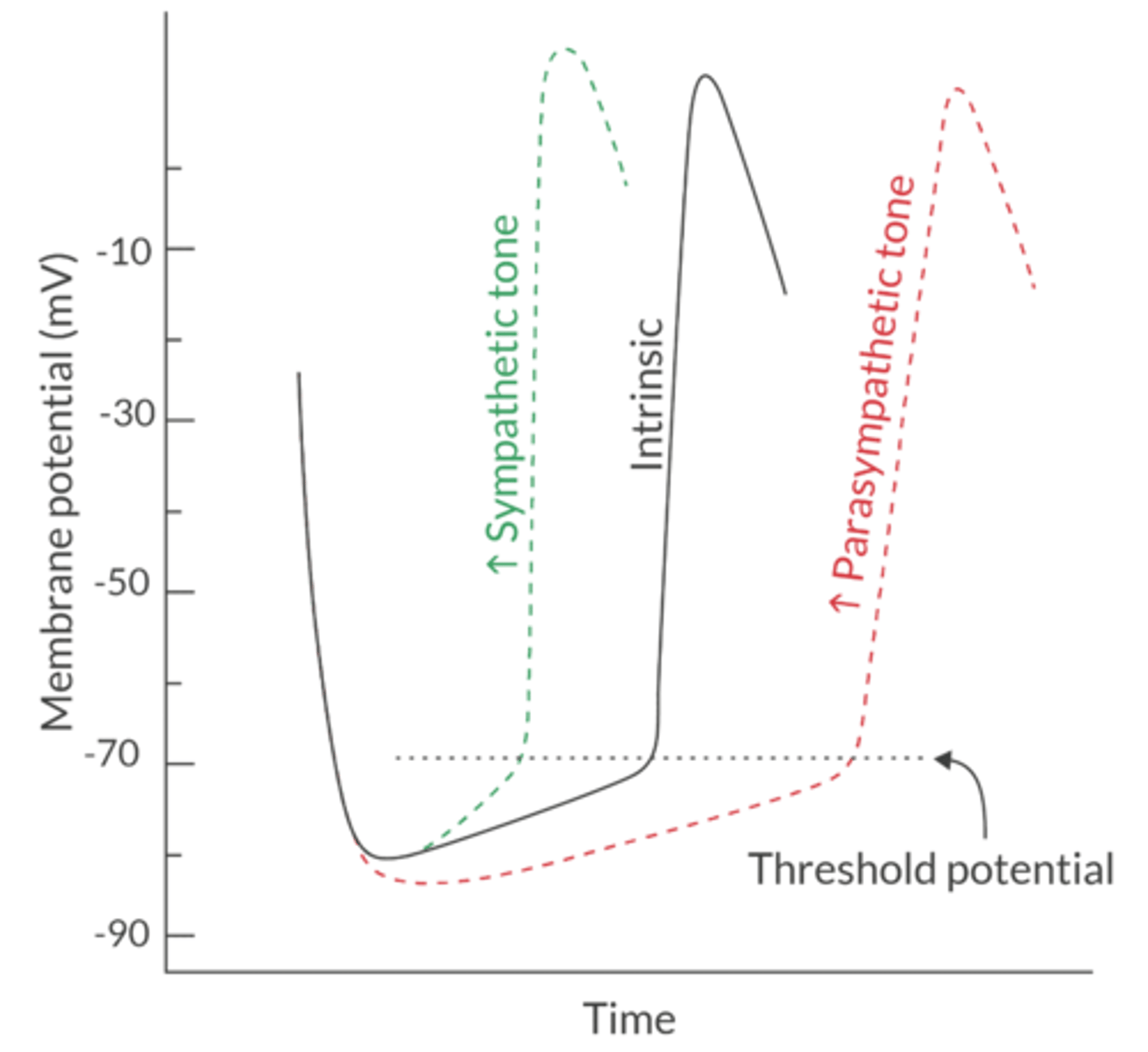
How does PNS autonomic tone affect HR?
Acetylcholine stimulates the muscarinic-2 receptor, which slows the HR by increasing K+ conductance and hyperpolarizing the SA node
This decreases the RMP and reduces the slope of spontaneous phase 4 depolarization (notice the less steep curve in the picture)
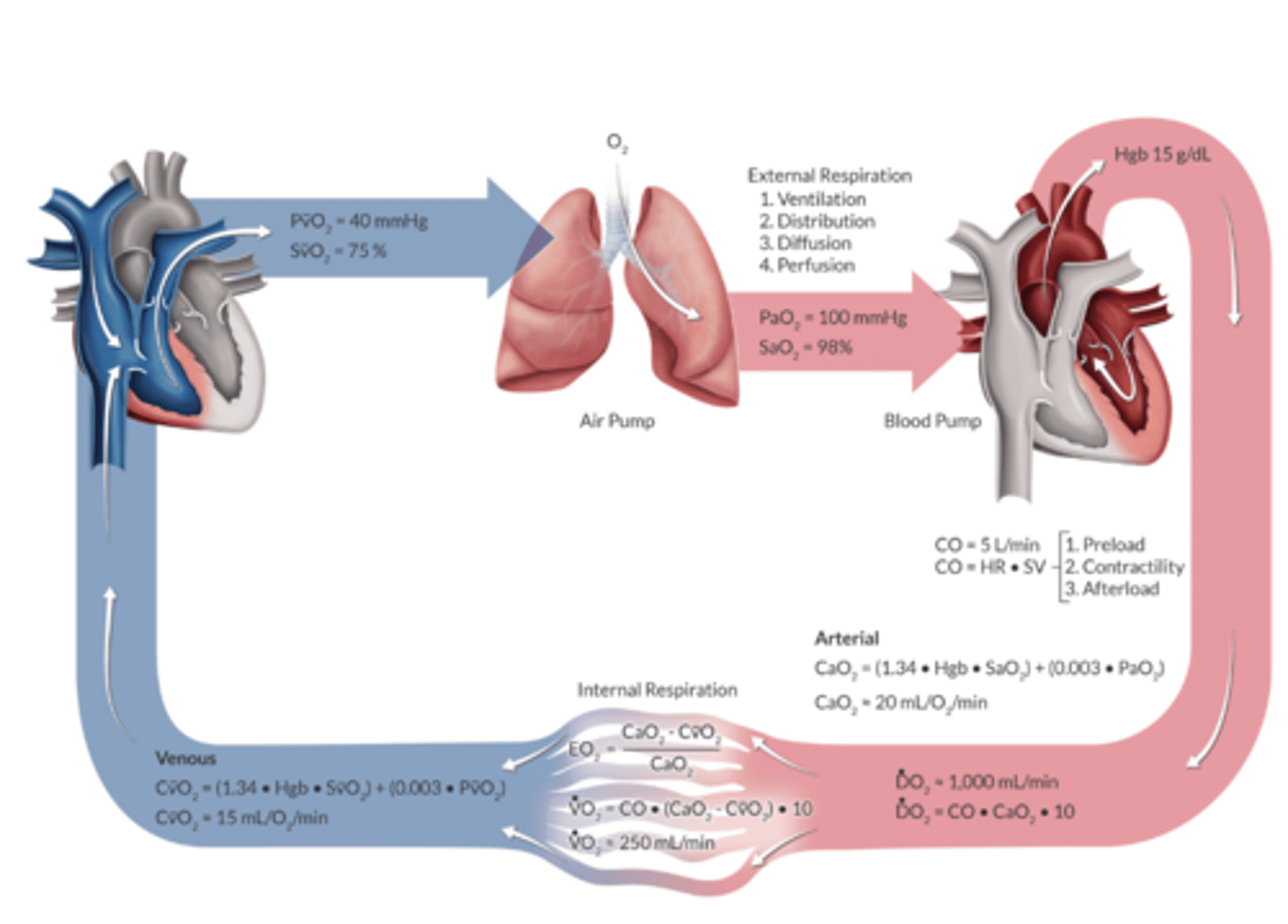
What is the expected O2 delivery in 70kg adult
A. 20ml/dl
B. 1,000ml/min
C. 250 ml/min
D. 15 mL/dL
B. 1,000ml/min
What does CaO2 tell us?
O2 carrying capactiy- tells us how many grams of O2 are contained in a deciliter of arterial blood
What is the CaO2 equation
CaO2= (Hgb x SaO2 × 1.34) + (PaO2 × 0.003)
Normal CaO2 value
20 mL/dL
DO2 describes what?
How much O2 is carried in arterial blood & how fast it’s being delivered to the tissues
What is the DO2 Equation?
DO2= CO x [(hgb x SaO2 × 1.34) + (PaO2 × 0.003)] x 10
which is basically CO x (CaO2 x 10)
What is a Normal DO2
DO2= CO x CaO2 x 10
1000 mL
What is EO2?
Oxygen extraction ratio
how much oxygen is exttracted by the tissues
EO2 Equation
CaO2- CvO2. = EO2
CaO2
25% (whole-body)
VO2 describes the bodies?
Oxygen Consumption= how much O2 is consumed by the tissues
What is the VO2 normal value
250 mL/min or 3.5 mL/kg/min
CVO2 is the?
Venous Oxygen Content- tells us how much oxygen is carried in venous blood
CvO2 equation
(Hb x 1.34 x SvO2) + (PvO2 x 0.003)
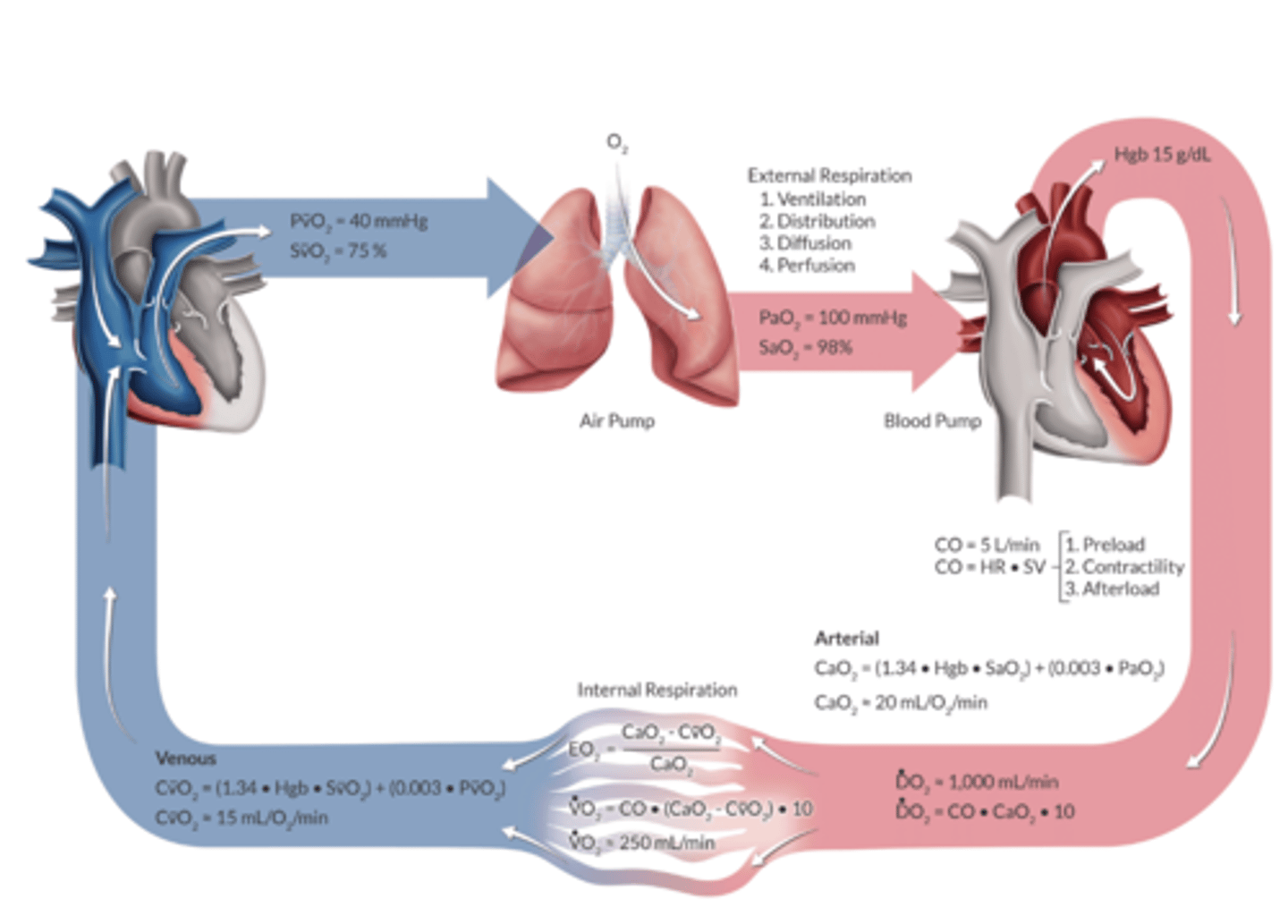
Venous Oxygen Content Normal Value
15 mL/dL
Blood flow is inversely proportional to:
A. Body temperature
B. Vessel diameter
C. AV pressure difference
D. Hct
D. Hct
PaO2 is the?
The amount of oxygen dissolved in blood
PaO2 follows what law?
Henry's
Ohm's Law
Current= Voltage Difference/ Resistance
OR
Flow=Pressure Gradient/Resistance
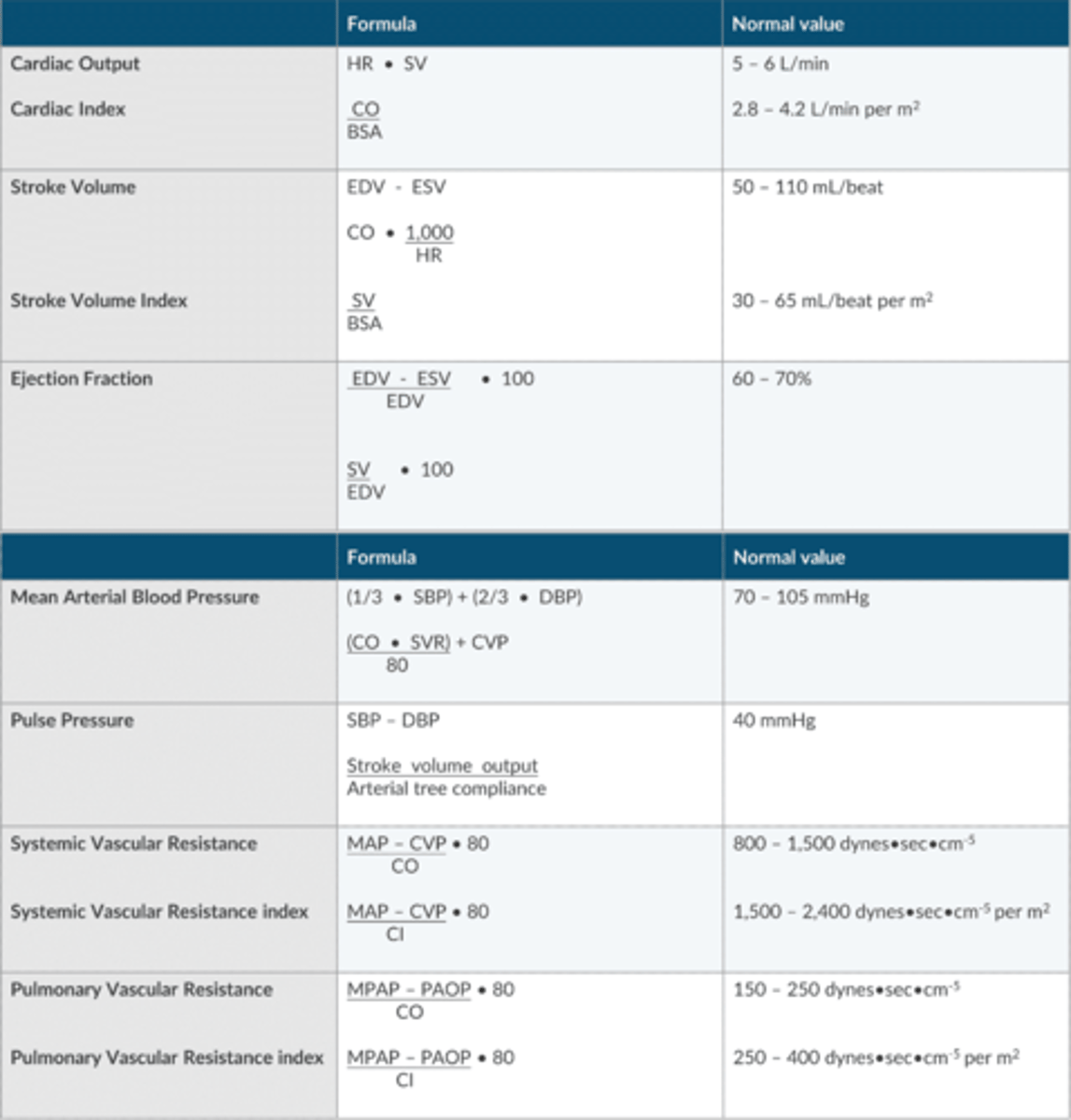
Apex Table for Ohm's Law Variables

MAP Equation using SVR
(CO x SVR)/ 80 + CVP
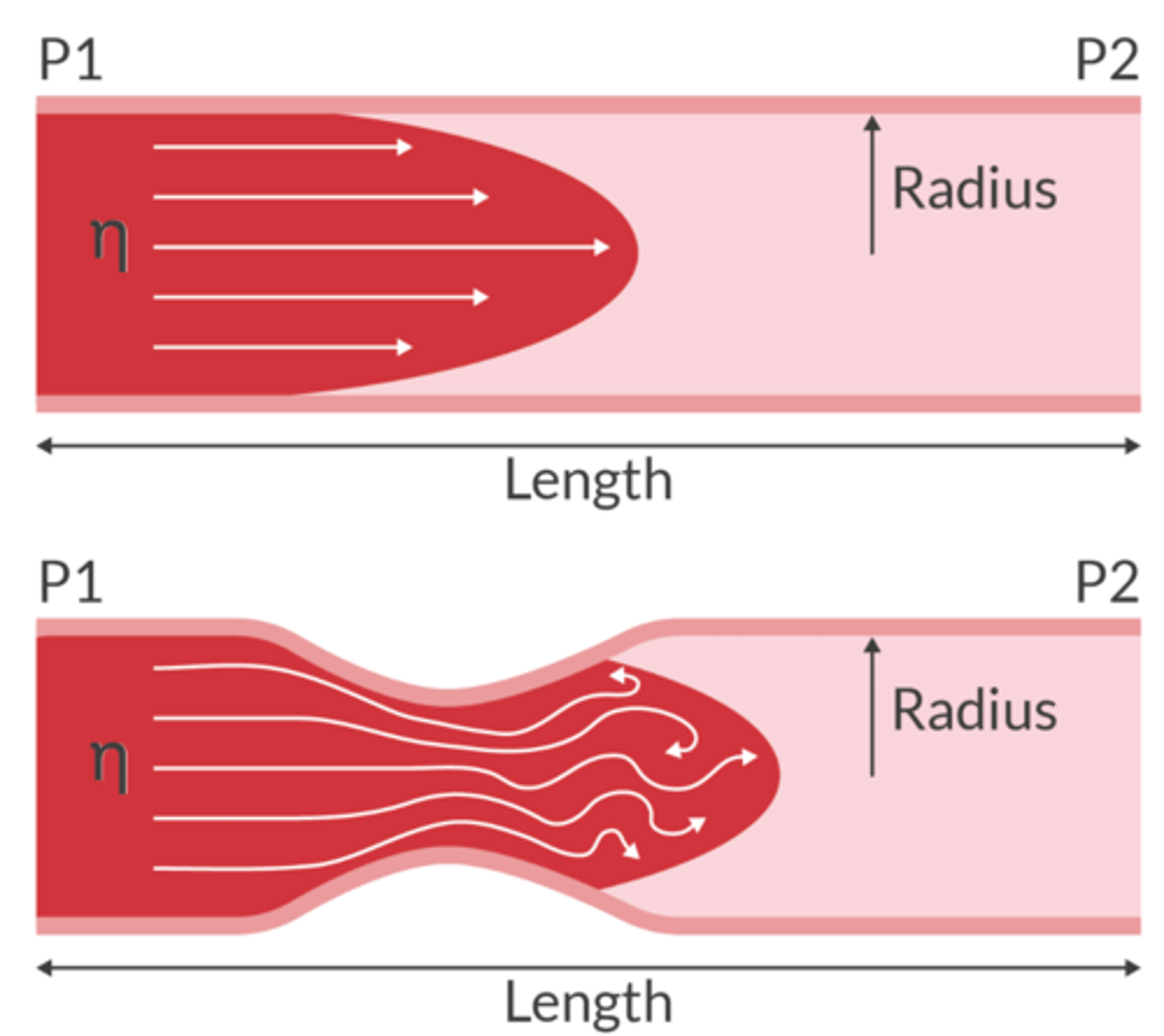
What is Poiseuille's Law?
flow rate = ΔP(πr^4 / 8Lη)
Q = dP/R
flow rate depends on pressure difference, and radius, length, and viscosity of liquid
increased resistance can be caused by increased length, increased viscosity, or decreased radius
Q= BF
R= Radius
Delta P= AV pressure gradient (Pa-Pv)
n= viscority
L= length of tube
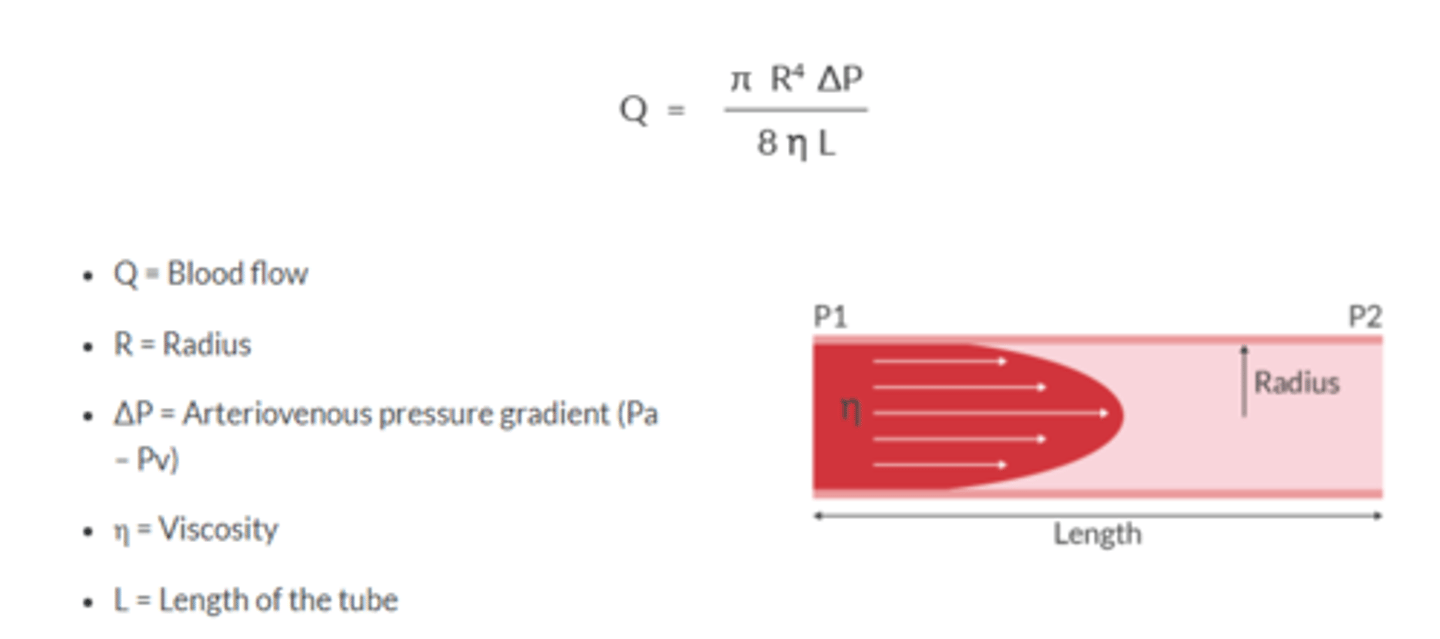
Vascular resistance is determined by ___ of artierioles
Radius
Doubling radius —> flow increases 16 fold
Tripling the radius—> flow increases 81 fold
Quadrupling the radius—> flow increases 256 fold
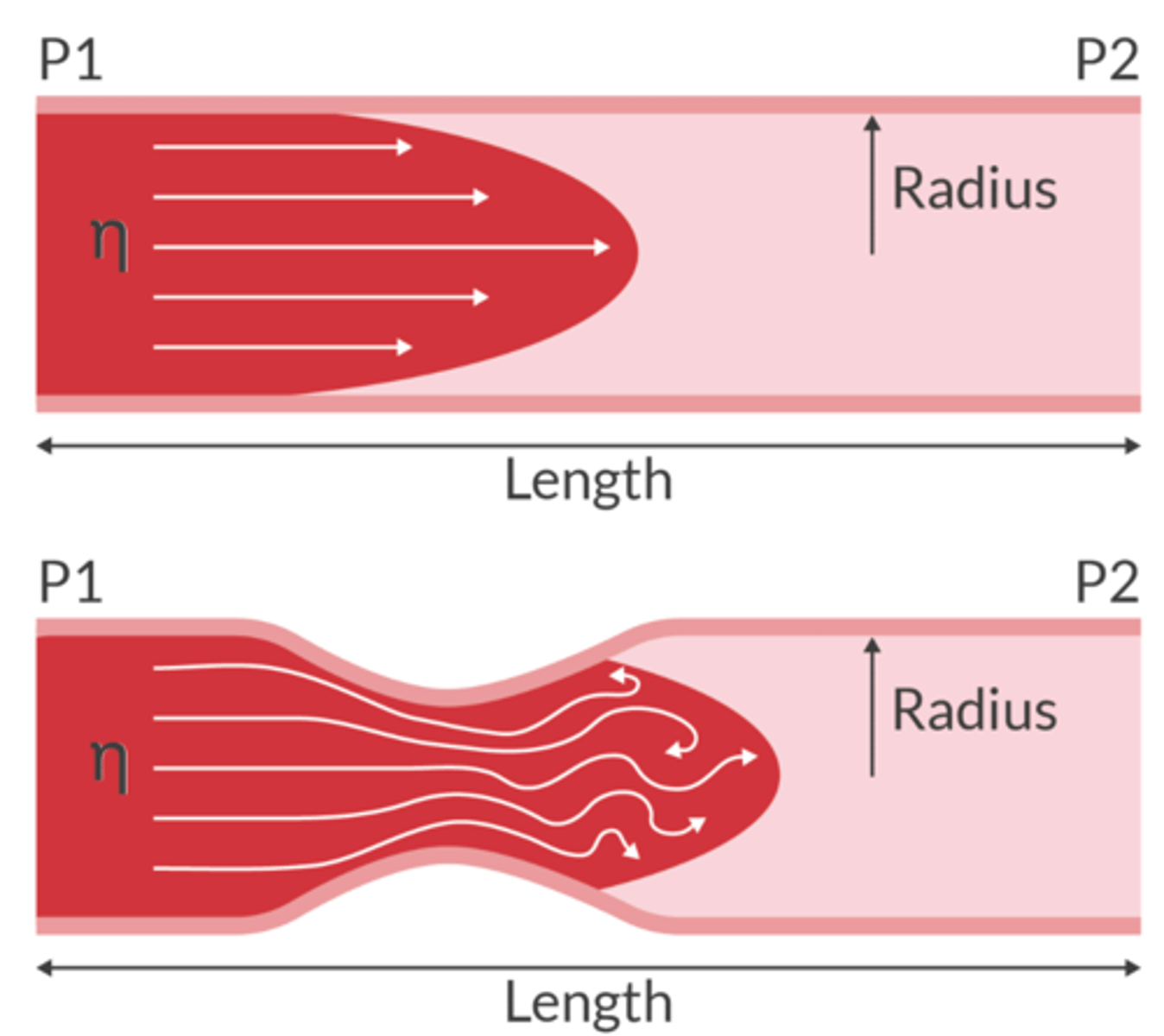
Laminar Flow
molecules travel in a parallel path through the tube
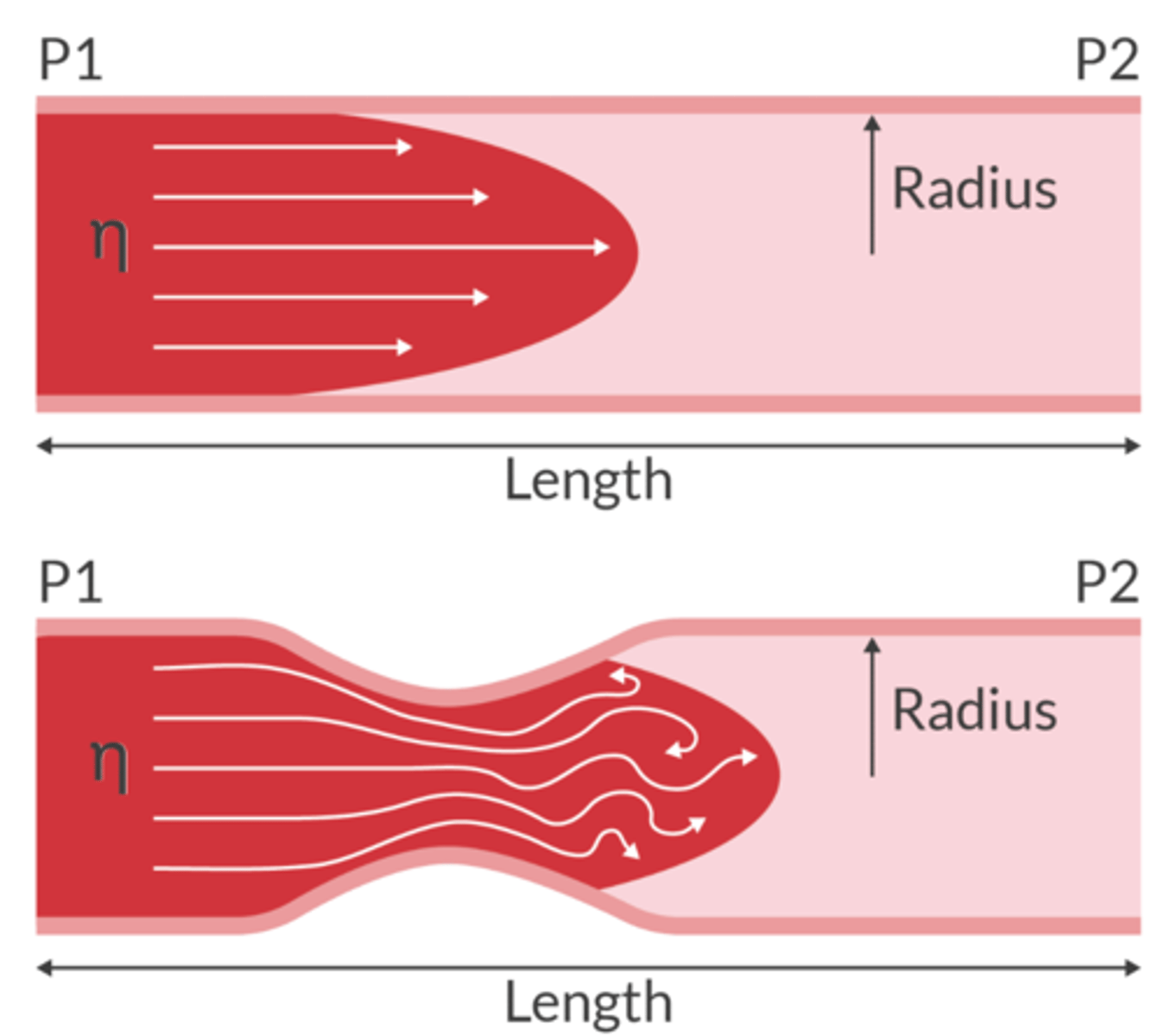
Turbulent Flow
molecules travel in a non-linear path and will create eddies
When flow is turbulent, lots of neergy is lost to heat and virbrations. (can produce a mumur)
Transitional Flow
Laminar flow along the vessel walls with turbulent flow in the center
Reynold's Number tells us what about flow?
used to predict if the flow will be laminar or turbulent
-Re <2000 = flow will be mostly laminar
-Re >2000 = flow will be mostly turbulent
- Re = 2,000-4,000 suggests transitional flow
The result of friction from the intermolecular forces as a fluid passes through a tube
Viscosity
What is blood viscosity determined by in the human body?
hematocrit and body temperature
Viscosity of blood is ________________ proportionate to temperature
INVERSELY PROPORTIONATE
— cool temp. increases viscosity & resistance
Match each hemodynamic variable with its equation
SV
MAP
SVR
EF
SV= CO x (1000/HR)
MAP= [(CO x SVR) /80] + CVP
SVR= [(MAP- CVP)/ CO] x 80
EF[(EDV-ESV)/ EDV x 100
Apex table for Hemodynamic Formulas/Variables
Interrelationship between hemodynamic variables
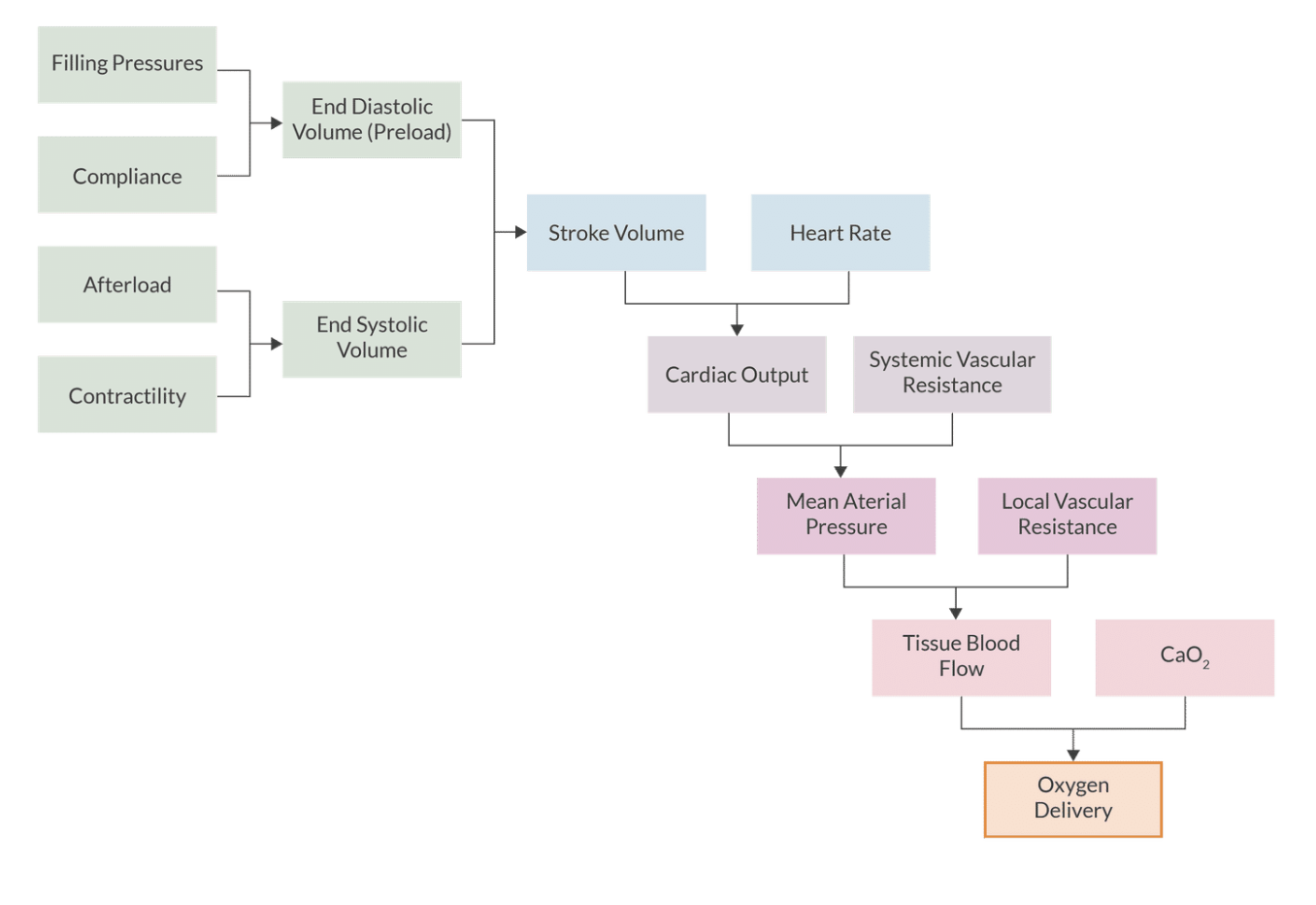
Which variables are related by the frank starling mechanism
A. LVEDP and SVR
B. contracility and CO
C. PAOP & SV
D. CVP and MAP
C. PAOP & SV
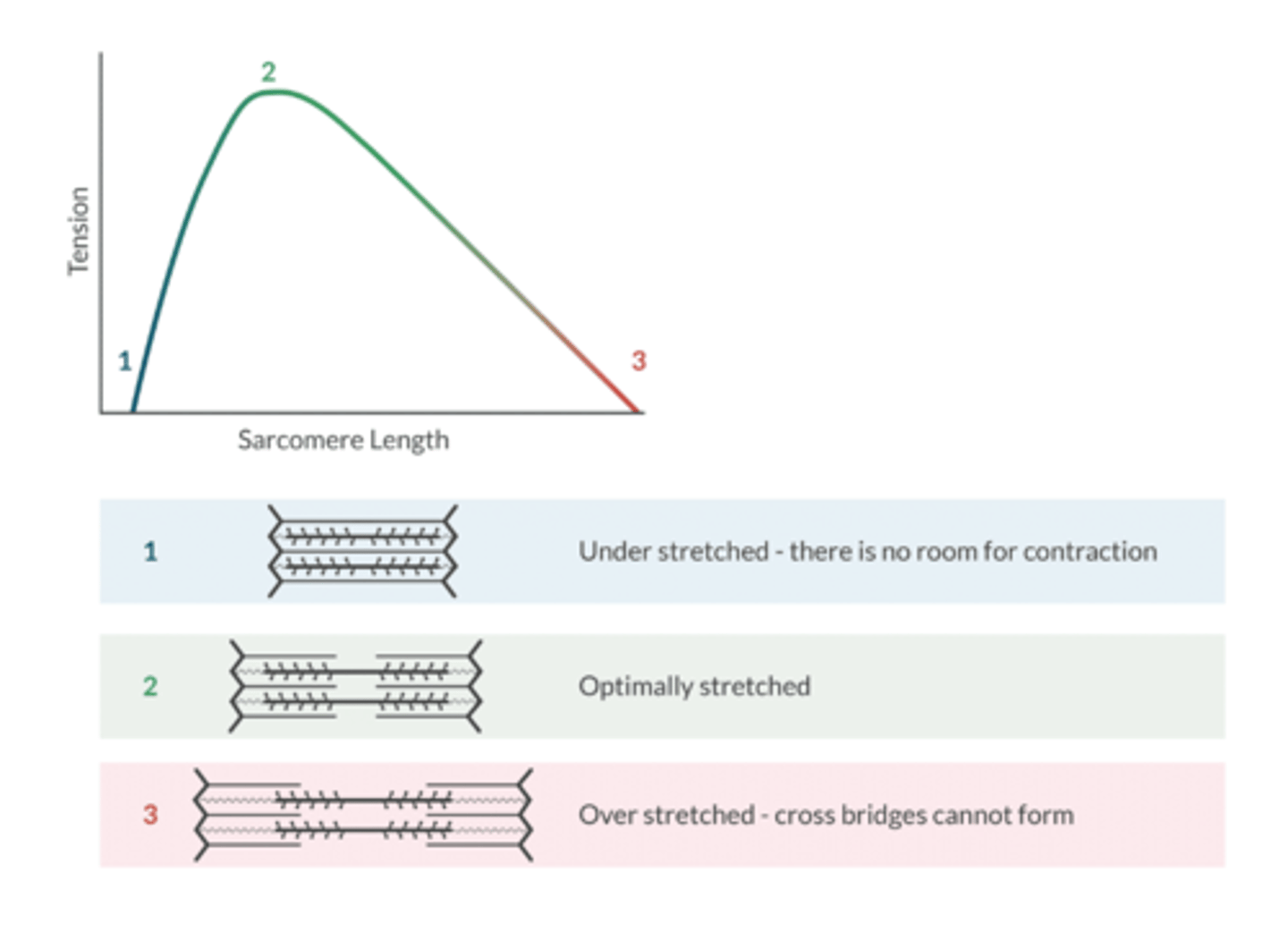
What is the functional unit of the contractile tissue in the heart?
sarcomere
Factors that influence preload: (7)
Blood volume- hypovolemia reduces preload
Atrial kick- atrial fib reduces preload
Venous tone- sympathectomy reduces preload
Intrapericardial pressure- pericardial tamponade reduces preload
Intrathoracic pressure- dynamic hyperinflation reduces preload
Body position- reverse Trendelenburg reduces preload
Valvular Regurgitation- aortic or mitral insufficiency INCREASES preload
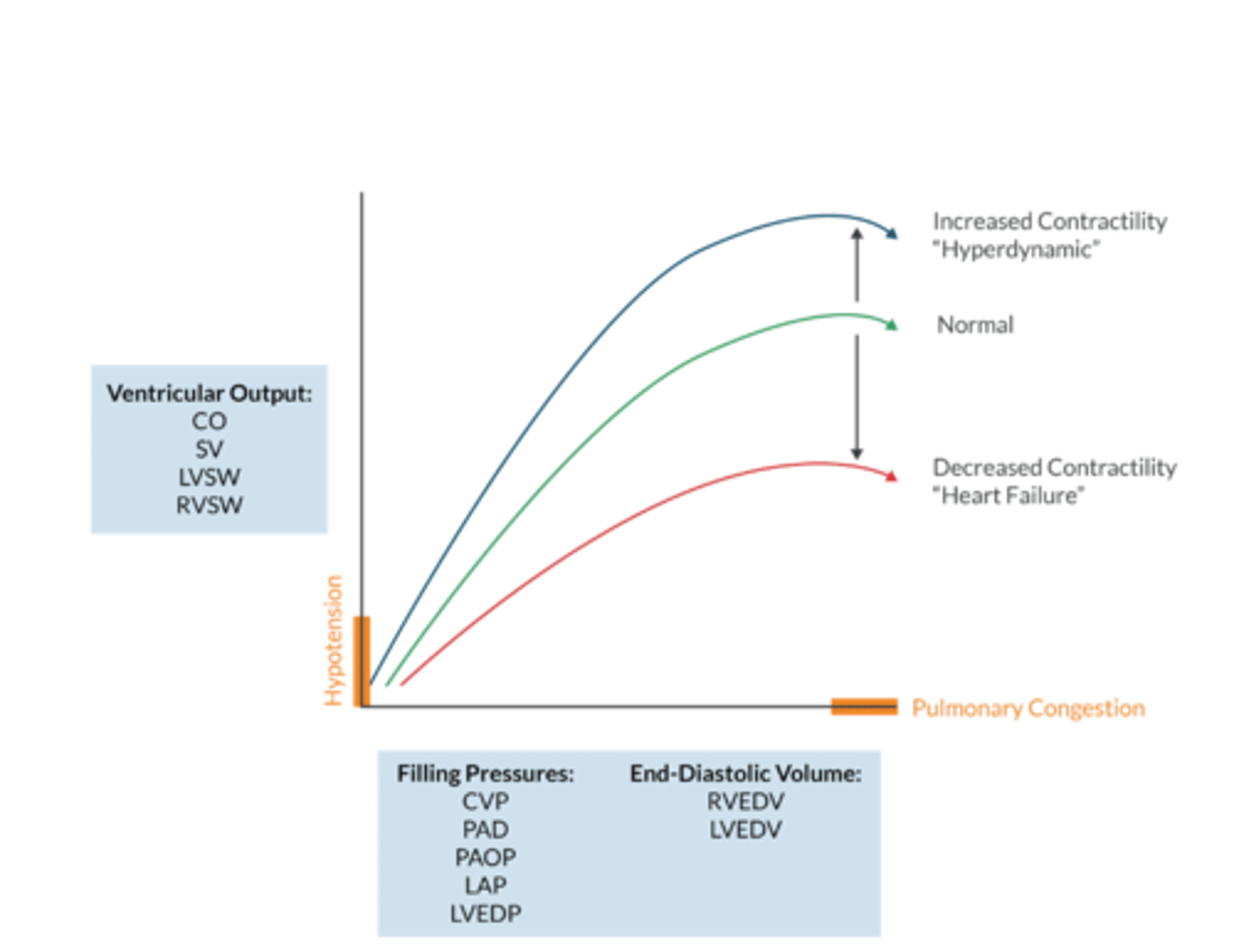
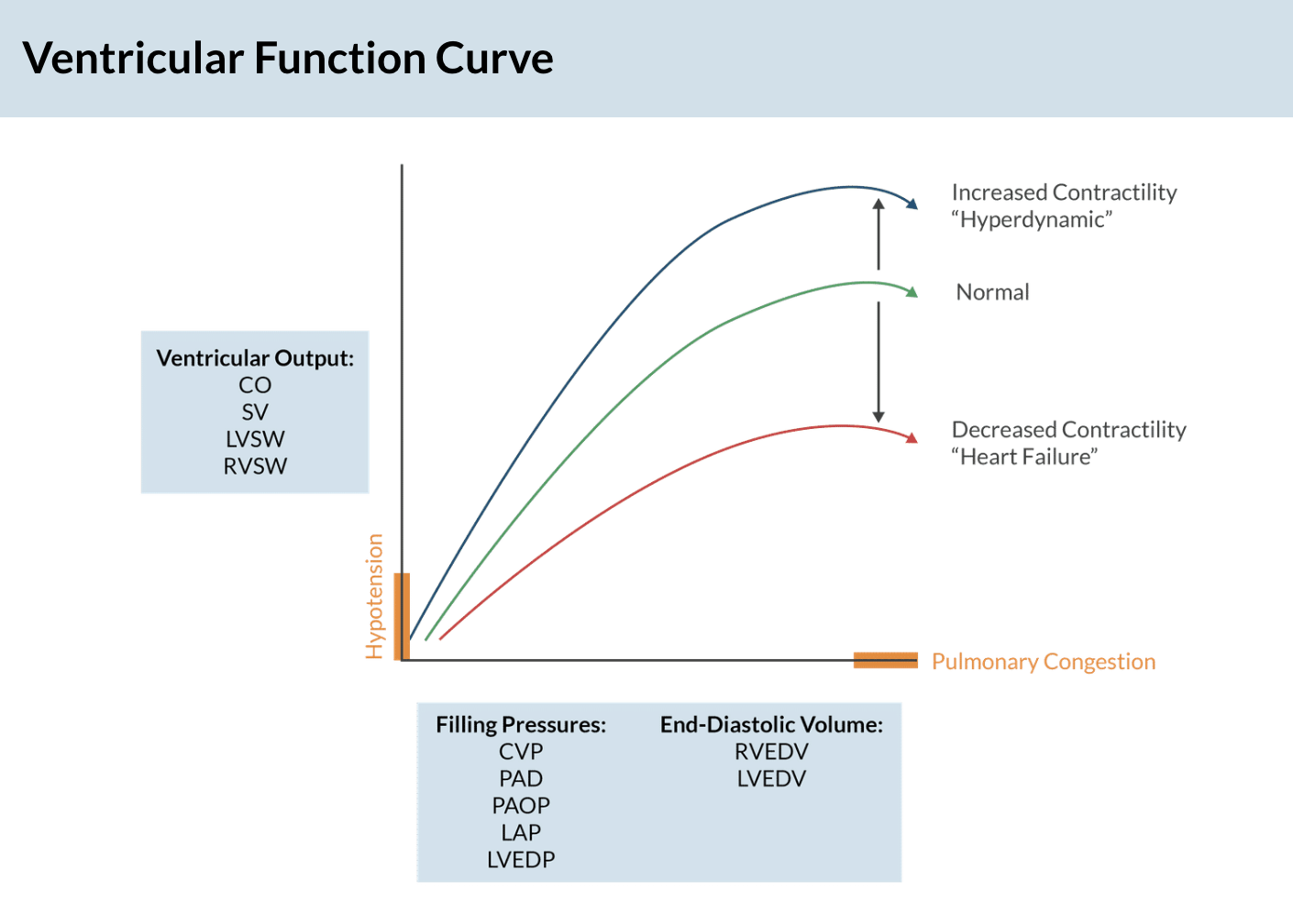
Ventricular Function Curve (apex )
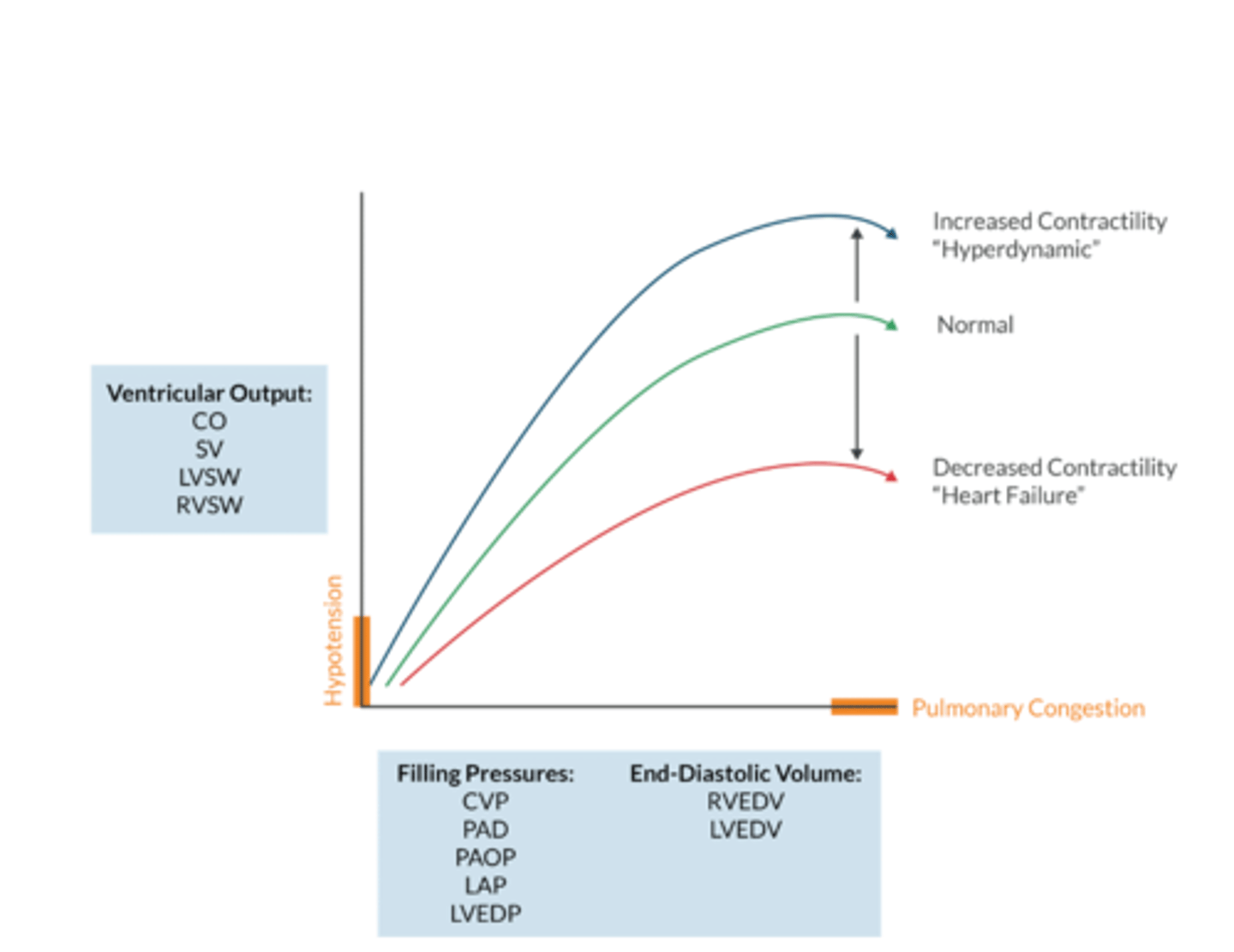
What does the ventricular function curve represent?
The Frank-Starling Mechanism- an increased ventricular volume produces a larger Cardiac output (to a point)
this occurs up to the plateau, after additional volume overstrestched ventricular sarcomers, decreases number of cross bridges that can be formed and decreases CO
Contractility (inotropy) is _________________ of preload and afterload
INDEPENDENT
- an increase preload increases the force of contraction (Starlings Law) but this is NOT the same as contractility
Contracility is the absility of the myocardial sarcomeres to perfrom work (shorten & produce force)
Whats on the Y axis of the ventricular function curve? (4)
Ventricular output:
CO
SV
LVSW
RVSW
what's on the x axis of the ventricular function curve? (2)
Filling Pressures:
-CVP
-PAD
-PAOP
-LAP
-LVEDP
End Diastolic Volume:
-RVEDV
- LVEDV
What % does atrial kick contribute to LVEDV (aka CO by extention)
20-30%
W/ a-fib, CO declines as a result
Conditions associated with reduced myocardial compliance include...(4)
1. hypertrophy
2. HF with preserved EF (diastolic failure)
3. fibrosis
4. aging
-these pts are more likely to experience a reduction in CO with cardiac rhythm disturbances, such as a-fib and junctional