CPR 3.2
0.0(0)
0.0(0)
Card Sorting
1/42
Earn XP
Description and Tags
Cardiac Rehabilitation (Part 1)
Study Analytics
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
43 Terms
1
New cards
Patients for Cardiac Rehabilitation
- Hypertensive
- Angina Pectoris
- Post-MI
- Cardiomyopathy
- Coronary Bypass Graft
- Coronary Angioplasty
- Coronary Atherectomy
- Pacemaker Implant
- Valvular Replacement
- Cardiac Transplant
- Elderlies
- Arryhtmias, CAD, Non-ischemic Heart disease, Pulmonary disease, PVD
- Healthy individuals who are at risk for CVD
- Angina Pectoris
- Post-MI
- Cardiomyopathy
- Coronary Bypass Graft
- Coronary Angioplasty
- Coronary Atherectomy
- Pacemaker Implant
- Valvular Replacement
- Cardiac Transplant
- Elderlies
- Arryhtmias, CAD, Non-ischemic Heart disease, Pulmonary disease, PVD
- Healthy individuals who are at risk for CVD
2
New cards
Goals of Cardiac Rehab
- Increase functional capacity
- Reduce pathophysiologic effects of heart disease or reverse pathological diseases leading to CVD
- Manage cardiac sx effectively
- Retard or reverse atherosclerosis
- Reduce mortality & morbidity
- Improve lipid profile
- Ameliorate high BP
- Counter obesity
- Control adult-onset diabetes
- Alleviate depression
- Improve QOL
- Reduce pathophysiologic effects of heart disease or reverse pathological diseases leading to CVD
- Manage cardiac sx effectively
- Retard or reverse atherosclerosis
- Reduce mortality & morbidity
- Improve lipid profile
- Ameliorate high BP
- Counter obesity
- Control adult-onset diabetes
- Alleviate depression
- Improve QOL
3
New cards
FITT Principle
Frequency, Intensity, Time/Duration, Type/Mode, Progression
4
New cards
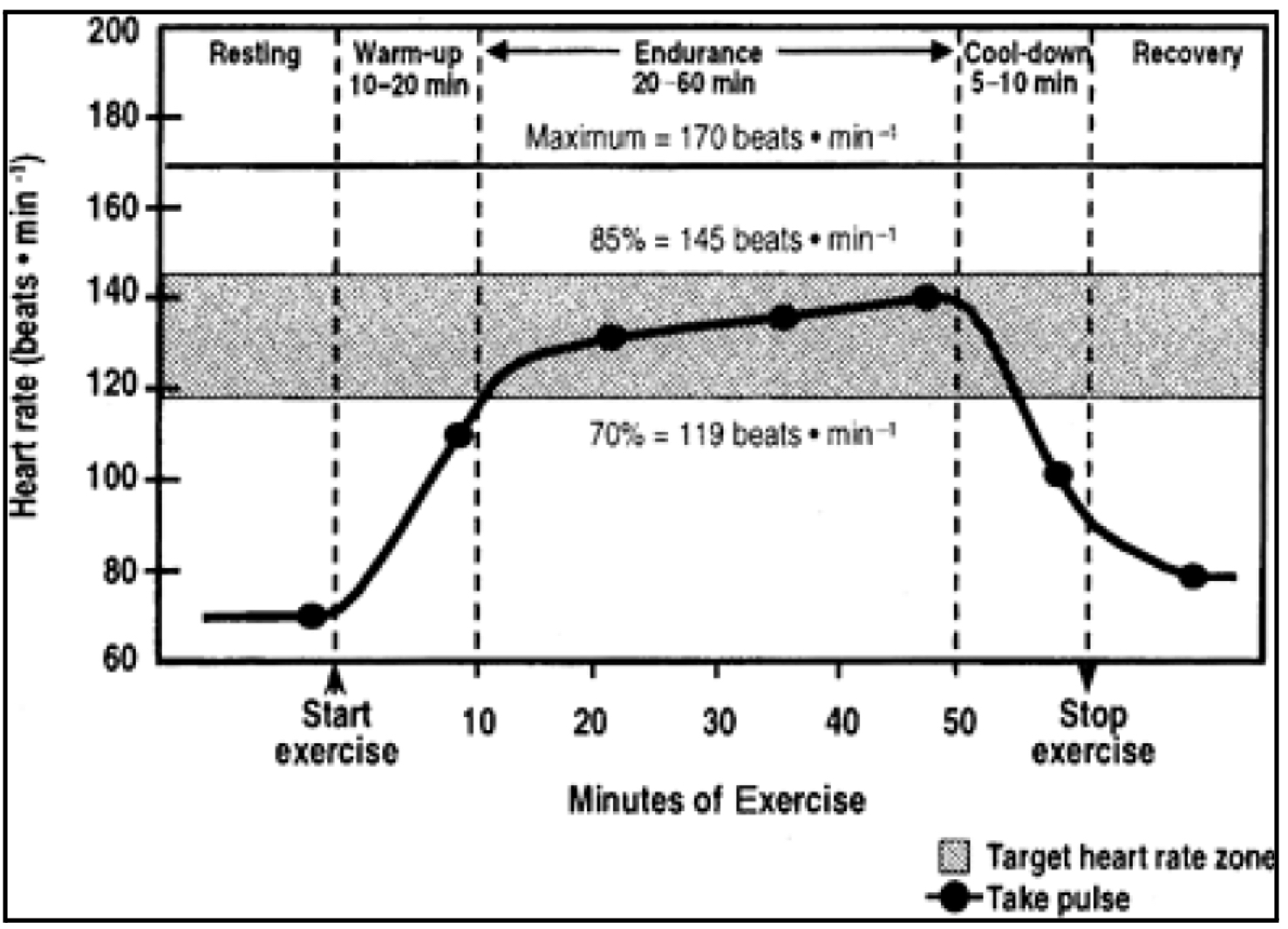
Components of Exercise Training
- Warm-up: 5-10 mins
- Conditioning: 20-60 mins
- Cool down: 5-10 mins
- Conditioning: 20-60 mins
- Cool down: 5-10 mins
5
New cards
What happens if pt immediately engages in endurance properly without performing warm-up?
Sudden rise/inc of HR
- not good as it is difficult to control already --> poses more risks
- not good as it is difficult to control already --> poses more risks
6
New cards
What happens when warm-up is done prior to endurance proper?
HR or VS will gradually inc intensity up until gray area is reached
Acute: focus on lower limit of gray area, aim for middle as progression
Chronic: focus on upper limit of gray area
In-pt: focus on white area below gray area
Acute: focus on lower limit of gray area, aim for middle as progression
Chronic: focus on upper limit of gray area
In-pt: focus on white area below gray area
7
New cards
TYPE/MODE: FLEXIBILITY EXERCISES
> General body stretching
- (+) tightness, spasm
- dependent on age, condition
> ROM
- (+) tightness, spasm
- dependent on age, condition
> ROM
8
New cards
TYPE/MODE: CALISTHENICS
> Gross motor movements
> Generalized big/large movements of the body
- provides general flexibility & general CV endurance
> Rhythmical
- incorporate muscle so pts can follow rhythm
> Generalized big/large movements of the body
- provides general flexibility & general CV endurance
> Rhythmical
- incorporate muscle so pts can follow rhythm
9
New cards
Cardiopulmonary Exercises - Group A
> Endurance activities (minimal skill and fitness)
> Adults (sedentary)
> Walking leisurely, cycling, aqua-aerobics, slow dancing (Zumba)
> Adults (sedentary)
> Walking leisurely, cycling, aqua-aerobics, slow dancing (Zumba)
10
New cards
Cardiopulmonary Exercises - Group B
> Vigorous intensity endurance activities requiring minimal skill (advanced)
> Physically active adults
> Jogging, running, aerobics, fast dancing (more diff Zumba, ballroom)
> Physically active adults
> Jogging, running, aerobics, fast dancing (more diff Zumba, ballroom)
11
New cards
Cardiopulmonary Exercises - Group C
> Endurance activities requiring skill (advanced)
> Adults with acquired skill (under training)
> Swimming, skating
> Adults with acquired skill (under training)
> Swimming, skating
12
New cards
Cardiopulmonary Exercises - Group D
> Recreational sports (advanced)
> Adults with regular exercise (if athletes, engage them to actual compet)
> Basketball, soccer, hiking
> Adults with regular exercise (if athletes, engage them to actual compet)
> Basketball, soccer, hiking
13
New cards
Determinants of Intensity/Parameters/Methods
> HR Method
> Oxygen Consumption
> Oxygen Consumption
14
New cards
Heart Rate Method
> Monitor pulse
> Compute THR using Karvonen's Formula
> [rHR + intensity % (HRmax - rHR)]
> HRR = HRmax - rHR
> Training SBP = %(SBPmax - SBPrest) + SBPrest
*Some pts HR is inaccurate (pts taking betablockers), use training SBP
> Compute THR using Karvonen's Formula
> [rHR + intensity % (HRmax - rHR)]
> HRR = HRmax - rHR
> Training SBP = %(SBPmax - SBPrest) + SBPrest
*Some pts HR is inaccurate (pts taking betablockers), use training SBP
15
New cards
O2 Consumption Method
> Determine VO2max
- requires gas analysis, pts wear O2 masks
> 60-70% of VO2max
> Equivalent to HRmax
> 60-70% VO2max = HRmax
- requires gas analysis, pts wear O2 masks
> 60-70% of VO2max
> Equivalent to HRmax
> 60-70% VO2max = HRmax
16
New cards
Maximum HR
> age dependent
> HRmax = 220 - age
> 60-80%(HRmax): normal indivs
>
> HRmax = 220 - age
> 60-80%(HRmax): normal indivs
>
17
New cards
Heart Rate Reserve
> HRR = HRmax - HRrest
- HRrest (baseline HR): while pt is NOT doing exercise
> 40-60%(HRR): cardiac pts
> 60-80%(HRR): normal indivs
- HRrest (baseline HR): while pt is NOT doing exercise
> 40-60%(HRR): cardiac pts
> 60-80%(HRR): normal indivs
18
New cards
Target Heart Rate
> Normal: 60-80% (HRR) + HRrest
> Athletes: 80-95% (HRR) + HRrest
> Cardiac pts: 40-60% (HRR) + HRrest
> Athletes: 80-95% (HRR) + HRrest
> Cardiac pts: 40-60% (HRR) + HRrest
19
New cards
Metabolic Equivalent
> Amt of O2 consumed by the body to perform physical activity at a given time
> 1 MET = 3.5 ml of O2 / kg of BW / min
> Cardiac pt = 50-60%
> 1 MET = 3.5 ml of O2 / kg of BW / min
> Cardiac pt = 50-60%
20
New cards
MET of Lying Quietly
1.0
21
New cards
MET of sitting at ease
1.2-1.6
22
New cards
MET of sitting, writing
1.9-2.2
23
New cards
MET of standing at ease
1.4-2.0
24
New cards
MET of walking at 1 mph
2.3
25
New cards
MET of light housework
1.7-3.0
26
New cards
MET of heavy housework
3.0-6.0
27
New cards
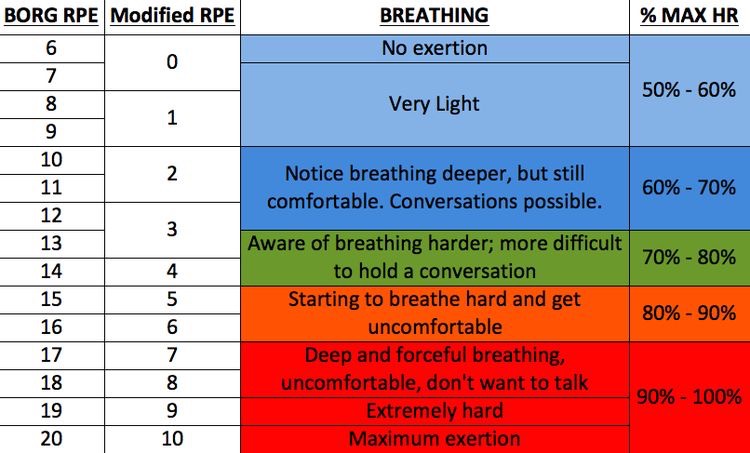
Rate of Perceived Exertion
> acute: 11-13 (60-70%)
> progress: 14-16 (70-90%)
> athletes: 17-20 (90-100%)
> progress: 14-16 (70-90%)
> athletes: 17-20 (90-100%)
28
New cards
FREQUENCY - In patient
> daily (usually BID)
> daily intervention but shorter duration
> 2x/day (20-30 mins, AM & PM)
> pt c advanced conditions (severely impaired CV endurance)
> daily intervention but shorter duration
> 2x/day (20-30 mins, AM & PM)
> pt c advanced conditions (severely impaired CV endurance)
29
New cards
FREQUENCY - out patient
3-5x/week
30
New cards
FREQUENCY - > 5 METS
3-5x/week
31
New cards
FREQUENCY - < 5 METS
Multiple daily sessions (usually bid)
32
New cards
Progression
> Duration inc first before intensity
33
New cards
Progress intensity if
- HR is lower than THR
- RPE is lower
- Sx of ischemia do not appear
- RPE is lower
- Sx of ischemia do not appear
34
New cards
Phases of Cardiac Rehab
I - acute, in pt care
II - home-based recuperation
III - out pt program
IV - indep self care
II - home-based recuperation
III - out pt program
IV - indep self care
35
New cards
Phase 1 - duration
upon admission until discharge (7-14 days)
36
New cards
Phase 1 - goals
> offset deleterious physiologic & psychological effects of bed rest
> provide medical surveillance/monitoring
> evaluate and prepare pts to safely return to ADLs within the limits imposed by their conditions
> prep the pt and support system at home or in a transitional setting
> facilitate physician referral and pt entry into an outpt cardiac rehab program
> provide medical surveillance/monitoring
> evaluate and prepare pts to safely return to ADLs within the limits imposed by their conditions
> prep the pt and support system at home or in a transitional setting
> facilitate physician referral and pt entry into an outpt cardiac rehab program
37
New cards
Phase 1 - indications for modified program
> pt presents c clinical sx
> need to lower intensity
> indicated but c caution (relative contraindication)
> large infarction (stable after 2-3 days )
> resting tachycardia (> 100 bpm) or inappropriate hR inc c self-care ADLs
> BP failing to rise or dec c self care ADLs (expected response is for BP to inc)
> ECG revealing >6-8 PVC/min or progressive heart block c self care ADLs
> angina or undure fatigue c self-care ADLs
> need for prolonged bed rest (> 4 days)
> complicated MI
> need to lower intensity
> indicated but c caution (relative contraindication)
> large infarction (stable after 2-3 days )
> resting tachycardia (> 100 bpm) or inappropriate hR inc c self-care ADLs
> BP failing to rise or dec c self care ADLs (expected response is for BP to inc)
> ECG revealing >6-8 PVC/min or progressive heart block c self care ADLs
> angina or undure fatigue c self-care ADLs
> need for prolonged bed rest (> 4 days)
> complicated MI
38
New cards
Complicated MI (McNeer Criteria)
> poor ventricular function
> significant ischemia c low-level activity
> cardiogenic shock
> ventricular tachycardia and/or fibrillation
> 2nd or 3rd AV block
> persistent sinus tachycardia (HR > 100 bpm at rest)
> persistent systolic hypotension (
> significant ischemia c low-level activity
> cardiogenic shock
> ventricular tachycardia and/or fibrillation
> 2nd or 3rd AV block
> persistent sinus tachycardia (HR > 100 bpm at rest)
> persistent systolic hypotension (
39
New cards
Phase 1 - Contraindications for program
> severe pump failure
> high risk subset:
- recurrent malignant arryhtmias
- angina at rest
- 2nd-3rd degree block
- persistent hypotension (
> high risk subset:
- recurrent malignant arryhtmias
- angina at rest
- 2nd-3rd degree block
- persistent hypotension (
40
New cards
Phase 1 - General Exercise Guidelines
> low intensity exercises (2-3 METs) --> 5 METs by discharge
> RPE: fairly light
> HR inc of 10-20 bpm above HRrest
> short exercise sessions c freq of 2-3x daily
> exercise tolerance test
> RPE: fairly light
> HR inc of 10-20 bpm above HRrest
> short exercise sessions c freq of 2-3x daily
> exercise tolerance test
41
New cards
Defining factor for Phase 1 discharge
5 METs
42
New cards
Exercise tolerance test
determines max capacity of pt and prescribed amt of exercise intensity
43
New cards