Physio 6102 Respiratory System
1/206
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
207 Terms
Functions of Respiratory System (6)
provides body with O2
eliminates CO2
regulates pH [H+] in blood
speech via vocal cords
defense against microbes
influences chemical messengers in blood
components of respiratory system
tubes into lungs, right and left lungs, alveoli, chest + diaphragm moves air into/out of lungs
respiratory cycle
one inspiration, one expiration
pathway of air during inspiration
upper airways to conducting zone to respiratory zone
upper airways
nose/mouth and pharynx
air into larynx, food into espohagus
upper airway diseases
inflammation from common cold/rhinitis
upper airway constriction (adenotonsillar hypertrophy- obstructive sleep apnea or choking)
air flow in conducting zone
bulk flow into trachea to 2 bronchi
into bronchioles (shorter/smaller tubes)
bronchi diameter controlled by
cartilage
bronchiole diameter controlled by
smooth muscle
respiratory zone composed of
alveoli (like tree)
3 functions of conducting zone
1, low-resistance pathway for airflow
warms + moistens air
defense against microbes/foreign particles
three defense mechanisms against foreign matters in conducting zone
surrounding cells have cilia, beat toward pharynx
cells secrete mucus to trap particles → pharynx
macrophages engulf foreign particles
conducting zone dysfunctions
cystic fibrosis + asthma
respiratory zone contains
7 branchings of tree: increases surface area for gas exchange
bronchioles + alveoli
gas exchange in respiratory zone
diffusion
cystic fibrosis
genetic CFTA Cl- channel mutation
mucus secretion dehydrated, thickens
causes obstructive blockages in breathing and bacterial accumulation
histology of respiratory zone
terminal bronchiole → respiratory bronchioles → alveoli
conducting zone doesn’t do
gas exchange
blood vessels and airway relationship
pulmonary artery and vein out of/into heart
pulmonary pressure LOW as compared to systemic
pulmonary artery hypertension
narrows, hypoxia, smooth muscle around artery constricts, difficult for right heart to pump into lungs
structure of alveolus
hollow sac open to airways
one cell-thick walls, secrete surfactant
two types of alveoli
type I: squamous epithelia alveolar: flat
type II: surfactant-secreting alveolar cells: cubical
oxygen must diffuse through 4 layers
thin layer of fluid lining alveolus
alveolar epithelium
alveolar and blood capillary basement membranes + interstitial connective tissues
blood capillary endothelium
air travel sequence in inhalation
pharynx → larynx → trachea → bronchi → alveoli
alveoli dysfunction
ARDS (acute respiratory distress syndrome) and sepsis
cytokine release, neutrophil infiltration, alveolar-capillary leak, edema
ARDS caused by
inhaled pathogens (COVID/bacteria)
lungs to chest wall relationship
thorax: closed compartment separated from abdomen by diaphragm
thoracic cage: spinal column, ribs, sternum, internal/external intercostal muscles
lungs to pleural sac relationship
lung surrounded by pleural sac
attached to lung by connective tissue and thoracic wall/diaphragm muscle
pleural sac
contains thin layer of intrapleural fluid (lubricates surfaces)
pressure changes in fluid causes changes in lung volume
how to lung surface and thoracic wall move
in/out together
ventilation
exchange of air between atmosphere and alveoli (high to low pressure)
air flow proportional to, inversely prop. to
pressure difference, resistance to flow
change in pressure: which two points
alveoli - atmosphere pressures
air flow equation
change in P/resistance
inspiration pressures
Palv < Patm
expiration pressures
Palv > Patm
P atm (relative)
760 mmHg, considered to be 0
what causes pressure change in alveoli
change in lung volume
which gas law underscores change in lung volume
Boyle’s law: constant temperature, volume and pressure are inverse
this drives air flow into/out of lungs
when lung volume increases, what happens to alveolar pressure
decreases (and vice versa)
what determines lung volume
compliance/ease of lung stretching
difference in pressure inside vs outside lungs
pressure inside lungs is, outside is
alveolar pressure, intrapleural pressure (in pleural sac)
transpulmonary pressure
alveolar P - intrapleural P
determinant change in lung volume: across the lung
trans-chest-wall pressure
Pip - Patm
intrapleural pressure is always
-4: subatmospheric
chest and pleural pressures are
opposing
three pressure changes in respiratory cycle
between breaths: Ptp is 4 to expand lungs
inspiration: Ptp increases to increase lung volume
expiration: Pip increases, Ptp decreases to passively recoil lungs
positive TP means
lungs contain some air (ALWAYS)
rupture of lung/chest wall results in
pneumothorax: Pip = 0 so Ptp = 0
lung collapses, rip cage expands
diaphragm + rib cage movement in respiration
inspiration: diaphragm descends, intercostal muscles elevate
expiration: diaphragm ascends, intercostals depress
inspiration events
diaphragm + intercostals contract
thorax expands
Pip decreases
Ptp increases
Palv decreases to move air inside
is there muscle connected directly to lungs?
NO: connected to pleural wall
when does inspiration end?
when Palv = Patm
what also contracts in large inspiration
other accessory muscles like scalenes
events during expiration
diaphragm + intercostals relax
chest wall recoils
Pip increases, Ptp decreases (return to preinspiration values)
lungs passively recoil to original dimensions
alveoli compress, Palv increases
air flows from lungs → atmosphere
air flows in expiration until
Palv = Patm
in expiration Pip is always, Ptp is always
subatmospheric, positive
so some air left in lungs
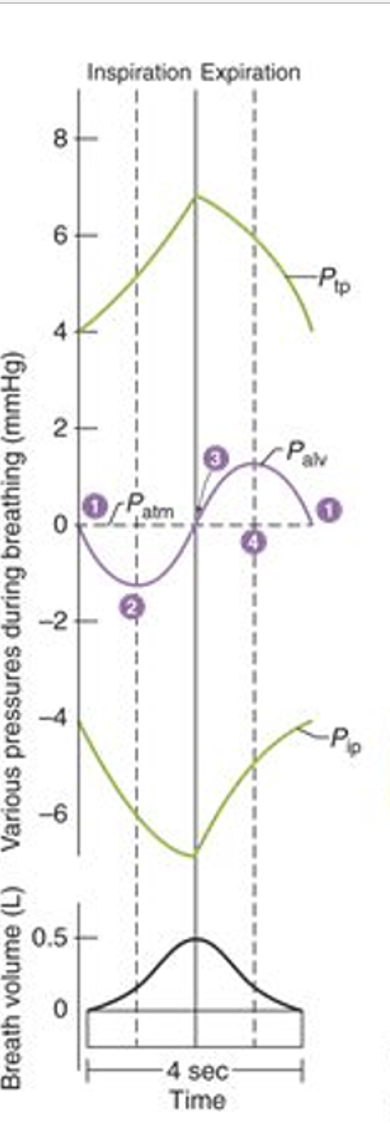
explain this diagram
talk about changes in each pressure
lung compliance definition
magnitude of the change in lung volume produced by a given change in Ptp
change in volume/Ptp
inverse of stiffness
lower lung compliance resilts in _ increase in volume for given increase in Ptp
less
patients with low compliant lungs:
breathe more shallowly, more rapidly for adequate ventilation
factors determining lung compliance
elasticity of connective tissue, surface tension at air-water interface in alveoli
clinical significance of lung connective tissue
pulmonary fibrosis
atelectasis/pneumothorax
emphysema/COPD
pulmonary fibrosis
ECM accumulation, scarring, decreased elasticity and compliance (more work to inflate rigid alveoli)
atelectasis/pneumothorax
decreased lung compliance
emphysema/COPD
elastic recoil property damage, high compliance, hard to exhale excess air
air sacs of the lungs damaged/enlarged, can be caused by smoking
surface tension
attractive force: pulls surface molecules together at air-liquid interface: maximize surface area
surface tension of PURE water in alveoli
difficult to expand, collapse: more energy to overcome surface tension + elastic lung tissue properties
purpose of surfactant
reduces surface tension to pull water molecules together, reduces surface tension too increase compliance
secreted by type II cells lining alvelo
what is surfactant
phospholipid/protein mixture, forms monolayer between air and water
mechanism of surfactant production
deep breath stretches type II cells, induces surfactant secretion
law of laplace
pressure = 2(surface tension)/radius
pressure prop. to ST, inverse to alveolus radius
why is surfactant important
stabilization of differently-sized alveoli to prevent collapse of small or over-expansion of large alveoli
based on radius size
respiratory-distress syndrome of newborn
surfactant deficiency, low compliance, increase work of breathing
mechanical ventilation + artificial surfactant administration
main determinant of airway resistance
tube radius (resistance inversely prop. to 4th power of airway radius)
physical factors that affect airway radius
transpulmonary pressure distends bronchioles
elastic connective tissue link outside of airways to alveloar tissue (lateral traction)- stretched during inspiration
neural + chemical factors that affect airway radius
control smooth muscle contraction/relaxation
epinephrine relaxes, leukotrienes contract
abnormal airway resistance in asthma
inflammation of airways (allergy), smooth muscle hypersensitive to environmental changes
asthma treatments
leukotriene inhibitors/ glucocorticoids for anti-inflammation
bronchodilator drugs for epinephrine to relax
chronic bronchitis
xs mucus in bronchi, chronic inflammation in airways to decrease diameter, increase resistance
lung volume measures
tidal volume:
inspiratory reserve volume
expiratory reserve volume
residual volume
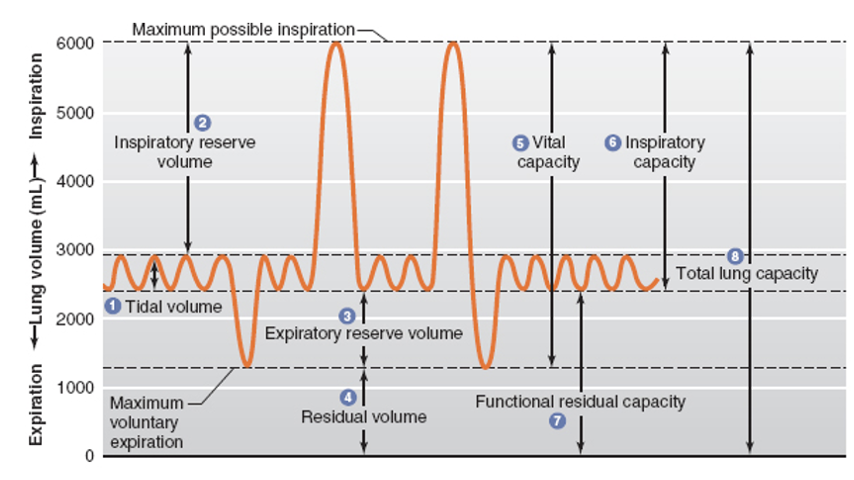
lung capacities
tidal volume (Vt)
volume entering/leaving lungs per breath (500 mL)
inspiratory reserve volume (IRV)
max air above TV in deepest inhalation (3000 mL)
expiratory reserve volume (ERV)
max air exhaled beyond Vt (1200 mL)
residual volume (RV)
air in lungs after max exhalation (1200 mL)
lung capacities
vital capacity, functional residual capacity, total lung capacity
vital capacity (VC)
max air a person can expire after maximal inspiratory (4700 mL)
Vt + IRV + ERV
functional residual capacity (FRC)
volume of air remaining in lungs after quiet expiration
ERV + RV
total lung capacity (TLC)
max amount of air lungs can contain
RV + IRV + ERV + Vt
forced expiratory volume in 1 sec
fraction of forced VC exhaled in one sec, 80% FVC
FEV1 in obstructive long diseases
decreased FEV1/FVC, increased resistance to expiration
FEV1 in restrictive lung diseases
decreased VC
normal or increased FEV1/FVC
respiratory minute ventilation
TV x respiratory rate
Ve = Vt x f
500 mL/breath x 12 breaths/min = 6000 mL/min
not ALL inhaled air for blood-gas exchange due to dead space
how much new atmospheric air reaches alveoli/breath
350 mL
alveolar ventilation
total volume of fresh air entering alveoli per minute
(TV - dead space) x respiratory rate
Va = (Vt - Vd) x f
4200 mL/min
to increase alveolar ventilation, what is more effective?
increase TV more effective than increase in respiratory rate
same minute ventilation, different alveolar ventilation
because dead space increases
two types of dead space
alveolar dead space: alveolar air that does not exchange with blood
physiologic dead space: anatomical + alveolar dead space
steps in respiration
ventilation: exchange of air b/w atmosphere and alveoli (bulk flow)
exchange of O2 and CO2 b/w alveolar air and blood in lung capillaries: diffusion
transport of O2 and CO2 through pulmonary and systemic circulation by air flow
exchange of O2 and CO2 b/w tissue capillary blood and cells in tissues by diffusion
cells use O2, produce CO2
pressure exerted by gas proportional to
temperature and gas concentration