ch 7 culture of the population in communities
1/65
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
culturally sensitive care
the practice of recognizing and attending to the unique cultural needs and beliefs of patients in a healthcare setting.
race
primarily a social classification that relies on physical markers such as skin color to identify group membership
culture
a set of beliefs, values, and assumptions about life that is widely held among a group of people and that is transmitted across generations
culture is also defined as
a learned world view shared by a population or group and transmitted socially that influences values, beliefs, customs and behaviors, and is reflected in the language, dress, food, materials and social institutions of a group.
cultural artifacts
physical items that represent the beliefs, values, and practices of a specific culture.
cultural competence
a combination of culturally congruent behaviors, practice attitudes, and policies that allow nurses to work effectively in cross- cultural situations. The term competence refers to performance that is sufficient and adequate.
racial classification
a social categorization based on physical features such as skin color and hair texture, which has limited relevance in clinical settings due to the vast differences among individuals within the same racial group.
ethnicity
a shared sense of identity and belonging, often marked by common cultural elements such as language, religion, and historical narratives that unite a group despite individual differences.
“peoplehood”
cultural awareness
the conscious self-reflection and exploration of one’s own cultural beliefs, values, and biases. it involves understanding how these factors influence one’s behavior and interactions with clients of different cultures.
learning cultural dimensions of clients
understanding our own behavior and how it impacts competant care
health is expressed differently across cultures which affects patient’s response
cultural knowledge
the process of gaining insights and information about the lifestyles, traditions, and health practices of various cultural and ethnic groups, emphasizing an understanding of the client’s perspective.
cultural skill
the ability to effectively incorporate cultural awareness and knowledge when gathering cultural data and performing appropriate physical assessments, including appropriate communication and interaction methods.
cultural encounter
the process by which healthcare providers engage in cross-cultural interactions, both directly with patients and indirectly with colleagues, to enhance understanding and prevent stereotypes.
cultural desire
the intrinsic motivation to provide culturally competent care, stemming from a genuine eagerness to learn and engage rather than an obligation imposed by others.
cultural preservation
the act of supporting and facilitating practices that are culturally significant for patients alongside conventional biomedical care.
supporting the use of acupuncture or the traditional Korean dish Mi-Yuk Kook (seaweed soup) for postpartum recovery.
cultural accommodation
a nursing intervention allowing the patient to maintain their cultural practices that do not pose a health risk, thus enhancing trust and compliance in care.
e.g., warm v. cold drinks, turning a bed to face Mecca for a bedbound patient, home burial of the placenta
cultural brokering
the role of healthcare providers in negotiating, advocating and mediating between the patient’s culture and the healthcare system to enhance understanding and access to needed care.
cultural repatterning
the process through which healthcare providers collaborate with patients to modify or change cultural practices that may be harmful to health.
e.g., using an herb tea that is causing HTN
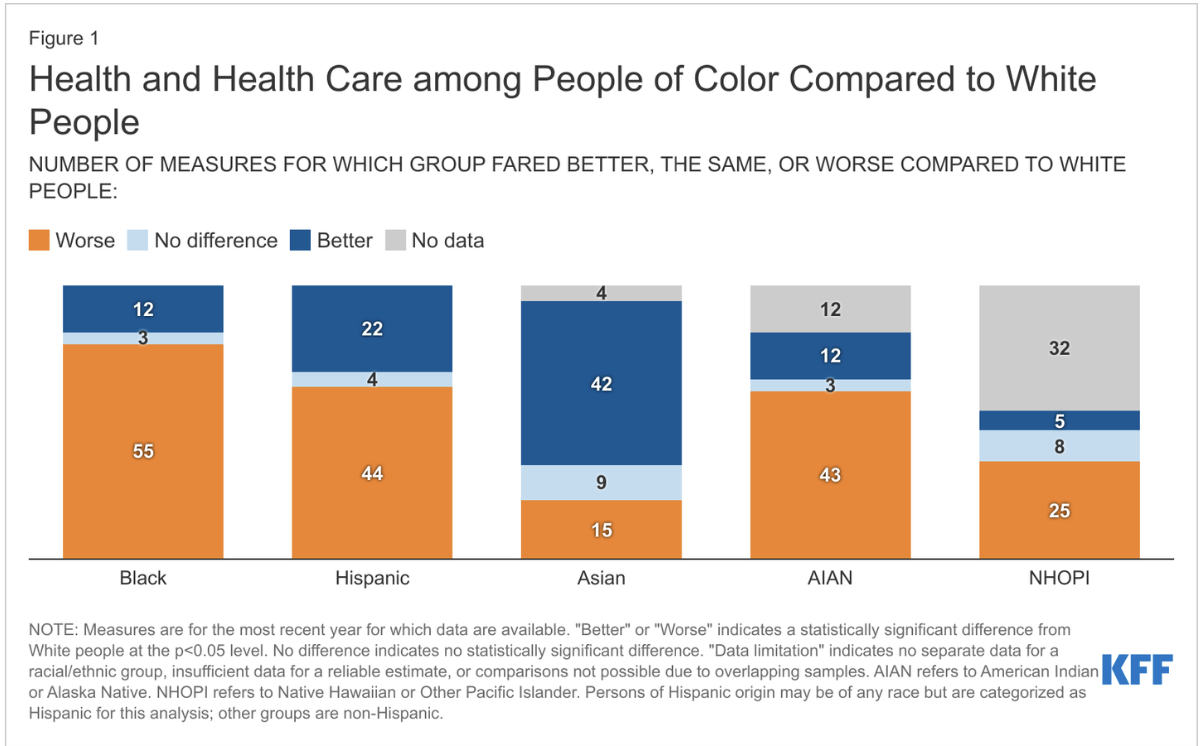
health disparities
differences in health outcomes and access to healthcare services among varied populations, primarily influenced by socioeconomic factors rather than biological aspects.
health disparities statistics
Hx of medical racism & violence
Tuskegee syphilis study - 40 years study with un consenting Black men
Henrietta Lacks - cervical cancer cells used in research without her consent
Dr. James Sims - “father” of modern gynecology -experimented on enslaved women without anesthesia
Forced sterilizations of Black, Native American and Puerto Rican women under 20th century eugencis laws
social determinants of health
the social, economic, and environmental factors that affect health outcomes and often contribute to health inequities, especially among culturally diverse groups.
stereotyping
the act of attributing generalized beliefs or characteristics to individuals based solely on their group identity without recognizing personal differences.
ex. asian people are good at math
prejudice
a prejudgment or negative attitude toward individuals from different groups, often rooted in stereotypes.
racism
a form of prejudice that involves the belief that certain racial groups are inherently inferior, leading to discrimination and unequal treatment in various aspects of life.
ethnocentrism
the belief that one's own culture or ethnic group is superior to others, which can lead to biased evaluations of other cultures.
documented (lawful permanent resident)
non-citizens who have been granted lawful status to reside and work in the united states but typically face a waiting period for access to public benefits.
refugee
individuals who flee their home country due to a well-founded fear of persecution and are often granted immediate eligibility for benefits such as medicaid upon arrival.
immigrants and barriers to care
factors that lead many immigrants to postpone seeking healthcare, including fear of deportation and unfamiliarity with the healthcare system, as well as specific health risks prevalent among certain immigrant populations.
cultural blindness
the practice of ignoring cultural differences and treating all individuals uniformly, which may overlook their unique cultural needs.
cultural imposition
the act of one culture forcing its values, beliefs, and practices onto members of another culture.
cultural conflict
a situation where differing cultural expectations lead to misunderstandings or perceived threats between healthcare providers and patients when either group is not aware of cultural differences
cultural shock
the disorienting experience of adapting to a culture that is significantly different from one’s own.
implicit bias
unconscious negative stereotypes or attitudes toward a particular group that can influence perceptions and behaviors toward individuals from that group.
project implicit
take the implicit association test to help address implicit biases
strategies to develop cultural competence and eliminate health disparities
an array of approaches including enhancing cultural awareness, acquiring knowledge and skills, fostering multiple cultural encounters, nurturing cultural desire, using frameworks to guide interventions, and addressing systemic issues.
cultural assessment
the systematic evaluation of a patient's cultural background to guide healthcare decisions and improve patient experiences.
ethnic model
a comprehensive framework for conducting culturally competent care that includes assessing a patient’s explanations of illness, treatments sought, alternative healers engaged, negotiation preferences, interventions, and collaborative approaches.
ethnic model “e”
questions that explore the patient's perspective on their health concerns, including personal interpretations and community input.
Why do you think you have these symptoms?
What do friends, family, or others say about these symptoms?
Do you know anyone else who has had this kind of problem?
Have you heard about, read about, or seen this problem on television, on the radio, or in the newspaper? (If patients cannot offer explanations, ask what most concerns them about the problem).
ethnic model “t”
queries related to past treatments and remedies the patient has utilized for their health issues.
What kinds of medicines, home remedies, or other treatments have you tried for this illness?
Is there anything that you eat, drink or do or avoid on a regular basis to stay healthy? Tell me about it.
What kind of treatment are you seeking from me?
ethnic model “h”
inquiries about any advice the patient has received from non-medical sources, such as folk healers or community members.
Have you sought any advice from alternative/folk healers, friends, or other people (non-doctors) for help with your problems? Tell me about it
ethnic model “n”
questions aimed at finding acceptable treatment options from both the patient’s and healthcare provider’s perspectives.
What options are acceptable to both you and me? Make sure these options incorporate your patient’s beliefs, not contradict them.
What are the most important results that you hope to achieve from this treatment?
ethnic model “i”
requests for the best intervention that aligns with the patient’s cultural practices and includes alternate treatment methods.
What is the best intervention for you?
Have we considered alternative treatments, spirituality, and healers as well as other cultural practices (e.g., foods eaten or avoided in general when sick)?
ethnic model “c”
questions that focus on collaboration between the patient, family, healthcare providers, and community resources to ensure comprehensive support.
How can the patient, family members, other health care team members, healers, and community resources collaborate?
arthur kleinman’s questions
a set of questions designed to elicit a patient’s conceptualization of their illness, including personal, cultural, and contextual factors influencing their health.
What do you call your problem? What name does it have?
What do you think caused your problem?
Why do you think it started when it did?
What does your illness do to you? How does it work?
How severe is it? Will it have a long or short course?
What do you fear most about your illness?
What are the chief problems that your illness has caused for
you?
What kind of treatment do you think you should receive?
What are the most important results you hope to receive from
treatment?
organizational factors
increase awareness of healthcare disparities
ensure payor systems don’t limit minority access to care
improve interpretation/language services
increase diversity among healthcare professionals
add cross-cultural education early in healthcare training
collect and use data to identify gaps
allow adequate time for patient care
follow guideline-driven care
provide a consistent “medical home” (primary care provider) to reduce disparities
interpreter selection
choose qualified interpreters (medical knowledge, dialect awareness) and avoid family or same-community interpreters when possible
consider factors like age, gender, and socioeconomic/education differences
speak slowly, clearly, and avoid medical jargon
introduce roles and monitor nonverbal cues during communication
confirm accuracy by checking understanding, using the patient’s exact words, and reviewing information with the patient
communication barriers
a range of challenges that impede effective communication in healthcare settings, potentially leading to misunderstandings.
mohammad kochi summary
an overview of the challenges faced by afghan refugees, especially from the nomadic kochi community, in accessing healthcare amidst cultural and systemic barriers.
why might information be withheld? (mohammad kochi)
reasons such as protecting the patient's emotional state, adherence to cultural norms where family decisions prevail, or concerns about provoking despair regarding treatment options.
is it ever acceptable to withhold information? (mohammad kochi)
withholding information may be justified if it aligns with the patient’s cultural values, although generally, honesty and transparency are prioritized in healthcare.
noorzia vs her father
a contrast between noorzia's preference for clear medical information and her father's traditional reliance on family and cultural perspectives.
why are interpreters important?
interpreters play a crucial role in minimizing communication errors, enhancing understanding, and ensuring patient safety through accurate translation of information.
takeaways from mohammad kochi
insights about diverse decision-making processes among patients, the impact of cultural disparities within the same community, and the critical role of effective communication in healthcare.
alicia mercado summary
a narrative highlighting how chronic illness can be complicated by socio-emotional factors, emphasizing the importance of understanding patient unique contexts to enhance care.
why did mrs. mercado not follow through with treatment?
reasons include stress and depression, concerns about medication side effects, cultural beliefs, and logistical challenges like appointment access.
reasons why other patients may not adhere
various factors such as high costs, lack of understanding of treatment, cultural preferences for alternative medicine, and complacency once feeling better.
role as mrs. mercado’s nurse
to engage empathetically, address barriers to care, provide clear education, establish manageable treatment plans, and offer appropriate supports.
mrs. mercado’s attitude towards medications
characterized by hesitation and fear, likely stemming from past experiences and cultural beliefs regarding the safety of treatments.
complementary/alternative medicine
non-conventional therapeutic approaches that can sometimes benefit patients, but should be openly discussed for safety and efficacy.
key takeaways for alicia mercado
acknowledgment that non-adherence is multifaceted, emphasizing the necessity of addressing mental health and personal stressors while fostering trust.
robert phillips summary
the story of a patient with severe kidney disease exploring the compounded challenges of mistrust and fear influenced by racial disparities in healthcare.
mr phillip’s interpretation of his illness
robert views his medical condition as life-altering and tied to deeper themes of identity and survival, contrasting with the clinical focus of healthcare providers.
why are there disparities in transplants? (robert phillips)
systemic inequities contribute to unequal access to organ transplants for african-americans, influenced by socioeconomic factors and biases in referral patterns.
how can stereotyping impact care? (robert phillips)
stereotypes can lead healthcare providers to make incorrect assumptions about patient behaviors, resulting in substandard care and diminished trust.
patient mistrust due to mistreatment (robert phillips)
mistrust in healthcare often arises from historical patterns of discrimination and negative experiences, influencing patients’ willingness to seek treatment.
robert phillips key takeaways
highlights the necessity for healthcare professionals to consider the patient's personal experiences, avoid stereotypes, advocate for equitable treatment, and build trust.