9.1 perio conditions
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
gingival color: reddish pink → more vascular
contour: rounded gingival margin
consistency: Softer and less fibrotic due to less dense connective tissue and fewer organized collagen fibers
surface texture: Smooth surface, stippling usually absent or minimal in early childhood
children
gingival color: coral pink
contour: knife edge gingival margin
consistency: firm and resilient
surface texture: stippling present
adults
features:
gingival inflammation
reversible
critically, features no loss of attachment or bone
plaque-induced gingivitis
prevalence:
low in early childhood
peaks during puberty
60% of teens exhibit gingival bop
plaque-induced gingivitis
etiology:
plaque dependent
steroid hormones (puberty, pregnancy, menstruation, oral contraceptives)
local factors: crowding, eruption, calculus
plaque-induced gingivitis
features:
enlargement of interdental papilla and/or marginal gingiva
appearance ranges from pale and fibrotic to red and friable
can be generalized or localized
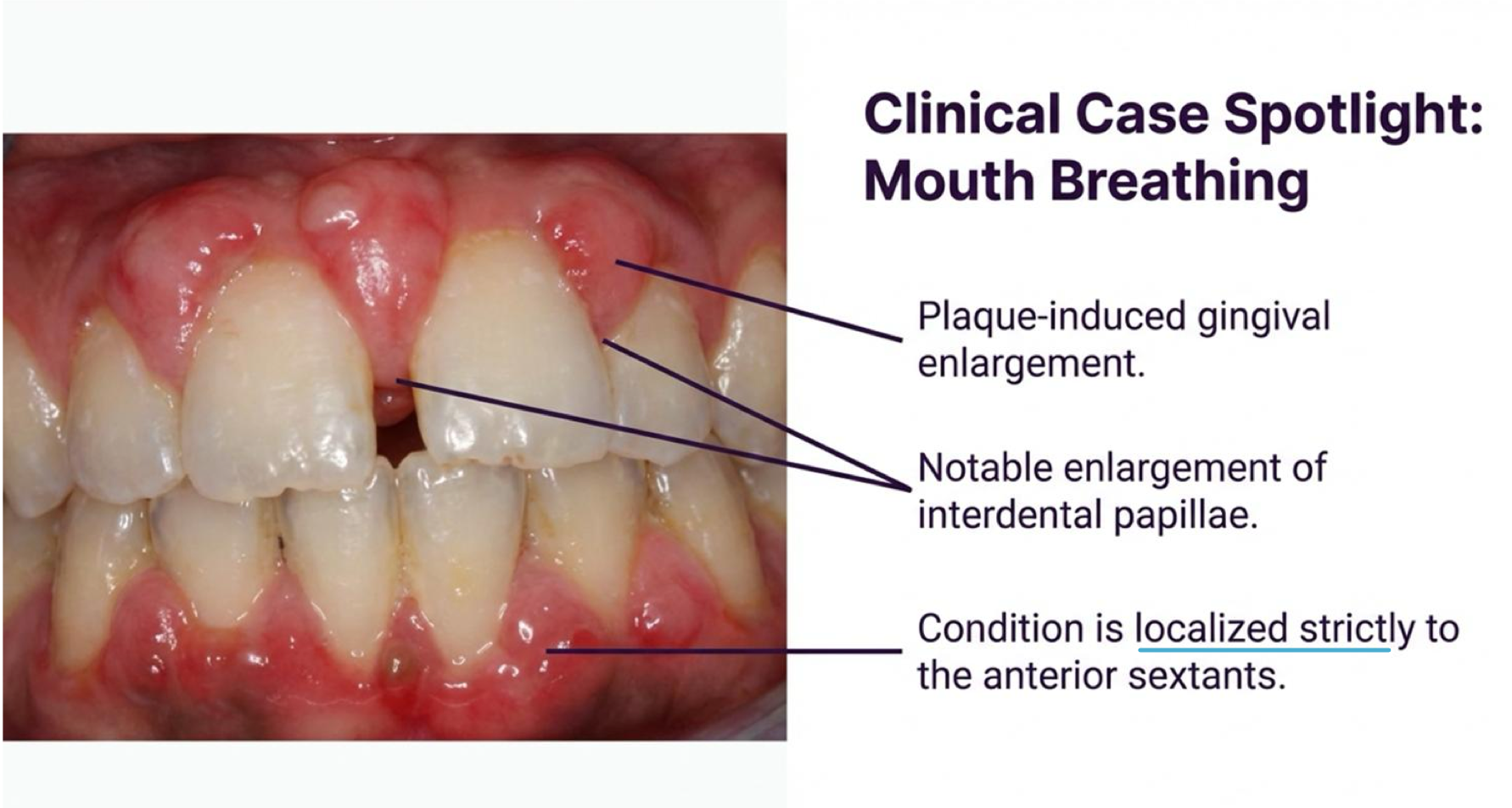
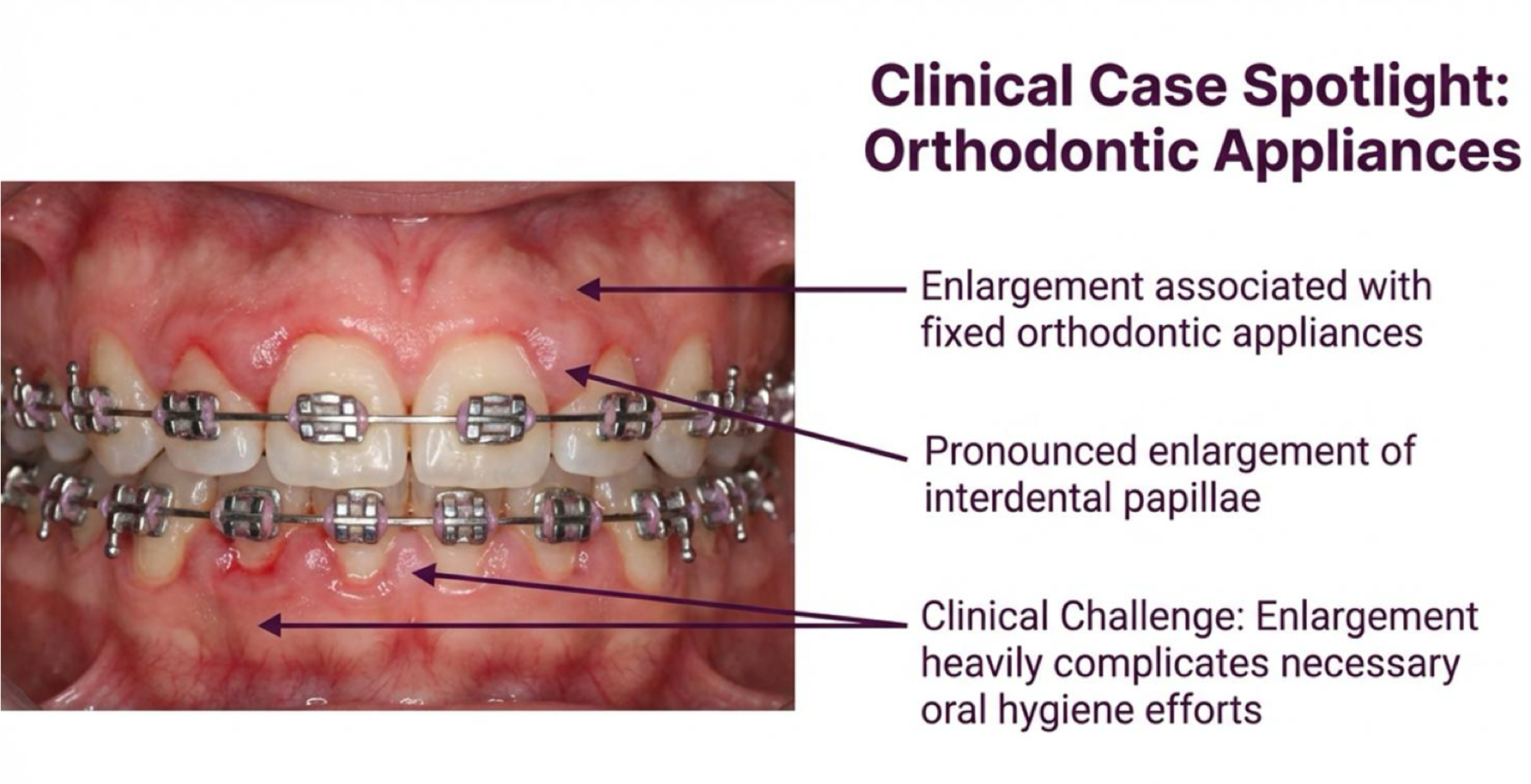
plaque-induced gingival inflammation
etiology:
caused by prolonged exposure to plaque
common local contributory factors - mouth breathing and orthodontic appliances
plaque-induced gingival inflammation
dental management:
requires thorough oral hygiene routines
in severe cases, gingivectomy or gingivoplasty may be required
plaque-induced gingival inflammation
mouth breathing may include presence of what three things?
orthodontic appliances may include presence of what three things?
what three drug types may induce DIGE?
anticonvulsants
immunosuppressants
calcium channel blockers
phenytoin, sodium valproate, phenobarbitone
anticonvulsants
cyclosporine, sirolimus, tacrolimus
immunosuppressants
nifedipine, nitrendipine, diltiazem, amlodipine
calcium channel blockers
clinical features of DIGE?
Painless fibro-epithelial growth of interdental papillae/marginal gingiva
May cover crowns
Related to plaque control (does not occur in edentulous areas)
Regresses after drug cessation
treatment for DIGE
Replace drug if possible
Professional prophylaxis
Azithromycin (beneficial post-debridement for cyclosporine patients)
Chlorhexidine rinse
Gingivectomy/gingivoplasty
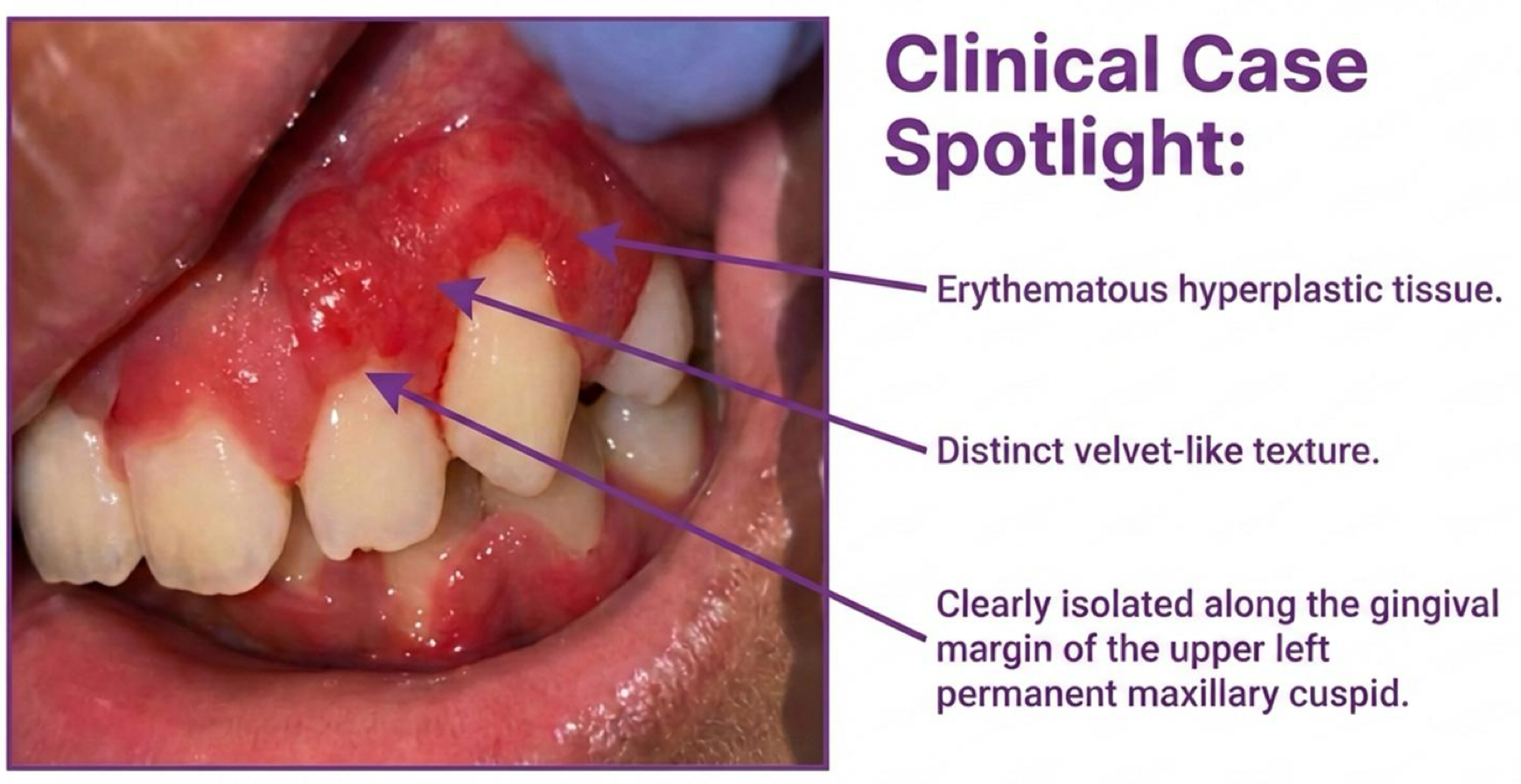
presentation of localized juvenile spongiotic hyperplasia
Red hyperplastic lesion with a highly vascular appearance and velvet-like texture
Involves marginal and/or attached gingiva
Not associated with plaque or calculus
Typically, asymptomatic but poses esthetic concerns. May resolve spontaneously
management of localized juvenile spongiotic hyperplasia
Surgical excision must be approached with caution due to the risk of gingival recession (recurrence rate is around 25%)
Insufficient evidence exists to prove the effectiveness of alternative treatments (cryotherapy, laser ablation, surface cauterization, topical steroids)
three presentations of localized juvenile spongiotic hyperplasia
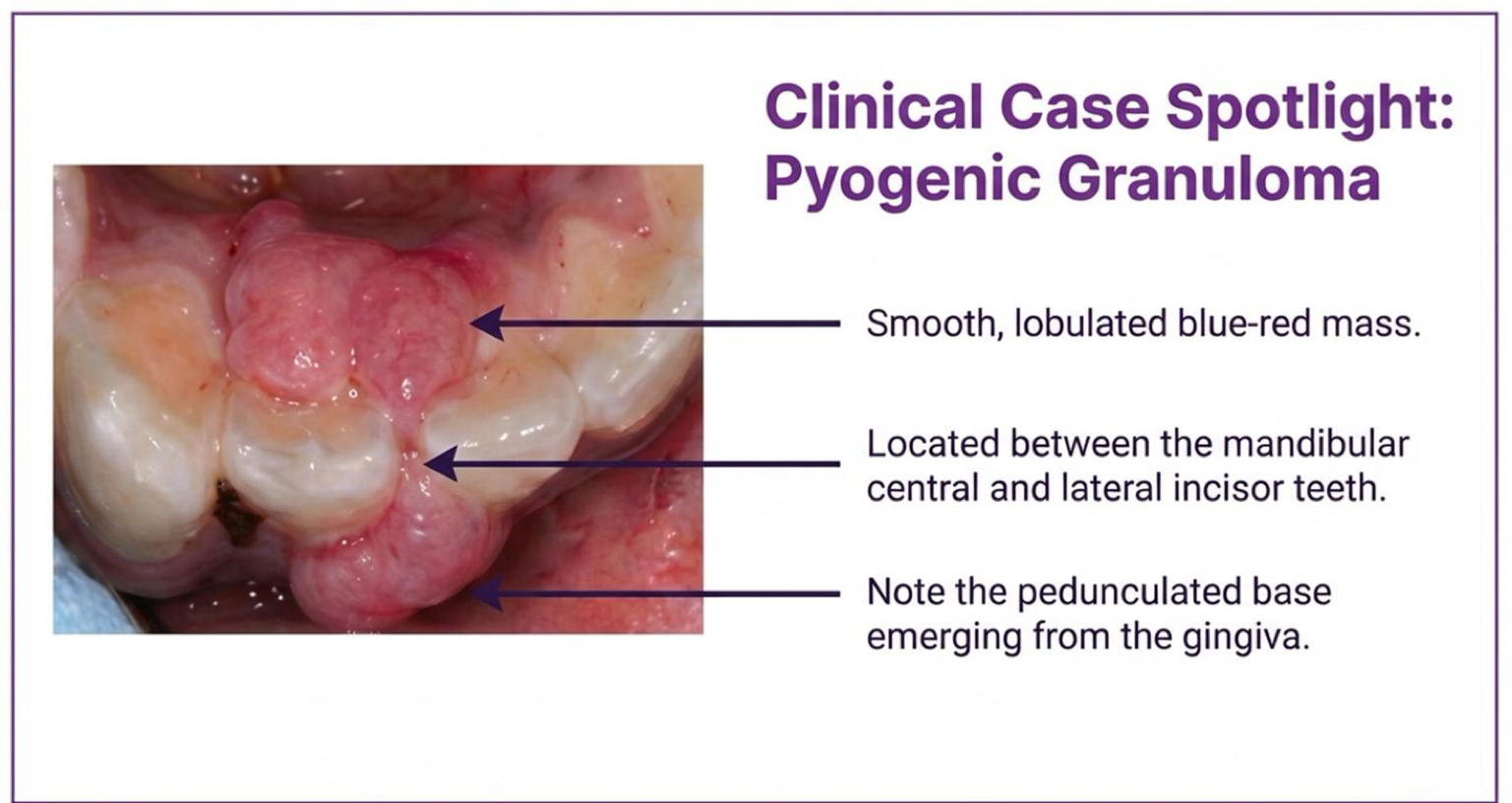
what is a pyogenic granuloma?
benign, reactive hyperplasia of CT. responds to trauma, chronic irritation, or elevated estrogen/progesterone. bleeds easily upon stimulation.
appearance and location of pyogenic granuloma
painless, smooth, lobulated blue-red colored mass
features a pedunculated base that commonly involves the gingiva
treatment of pyogenic granuloma
complete surgical excision coupled with the removal of underlying irritant
three features of pyogenic granuloma

Localized, painful sudden onset
Bacterial infection post-trauma (e.g., embedded popcorn, fingernail)
Managed via debridement, irrigation, drainage
(no PARL, no adj caries, etc)
gingival abscess

Inflammation of flap covering partially erupted molar (mostly 3rd molars)
Food trap leads to bacterial growth. Very painful due to occlusal trauma
Managed via debridement, antibiotics, chlorhexidine, extraction
pericoronitis

Edematous, spongy gingiva with non-specific appearance
Spontaneous bleeding, impaired wound healing
Managed by treating deficiency and plaque control
vitamin C - deficiency gingivitis

Rapid, painful onset. Soft tissue necrosis/ulceration with malodor
Linked to spirochetes, Prevotella Intermedia, stress, smoking. Peak in late teens/20s
Managed via ultrasonic debridement, NSAIDs, penicillin/metronidazole
ANUG (Acute Necrotizing Ulcerative Gingivitis)
what are the three distinct forms of perio disease?
periodontitis, necrotizing perio, perio as manifestation of systemic condition
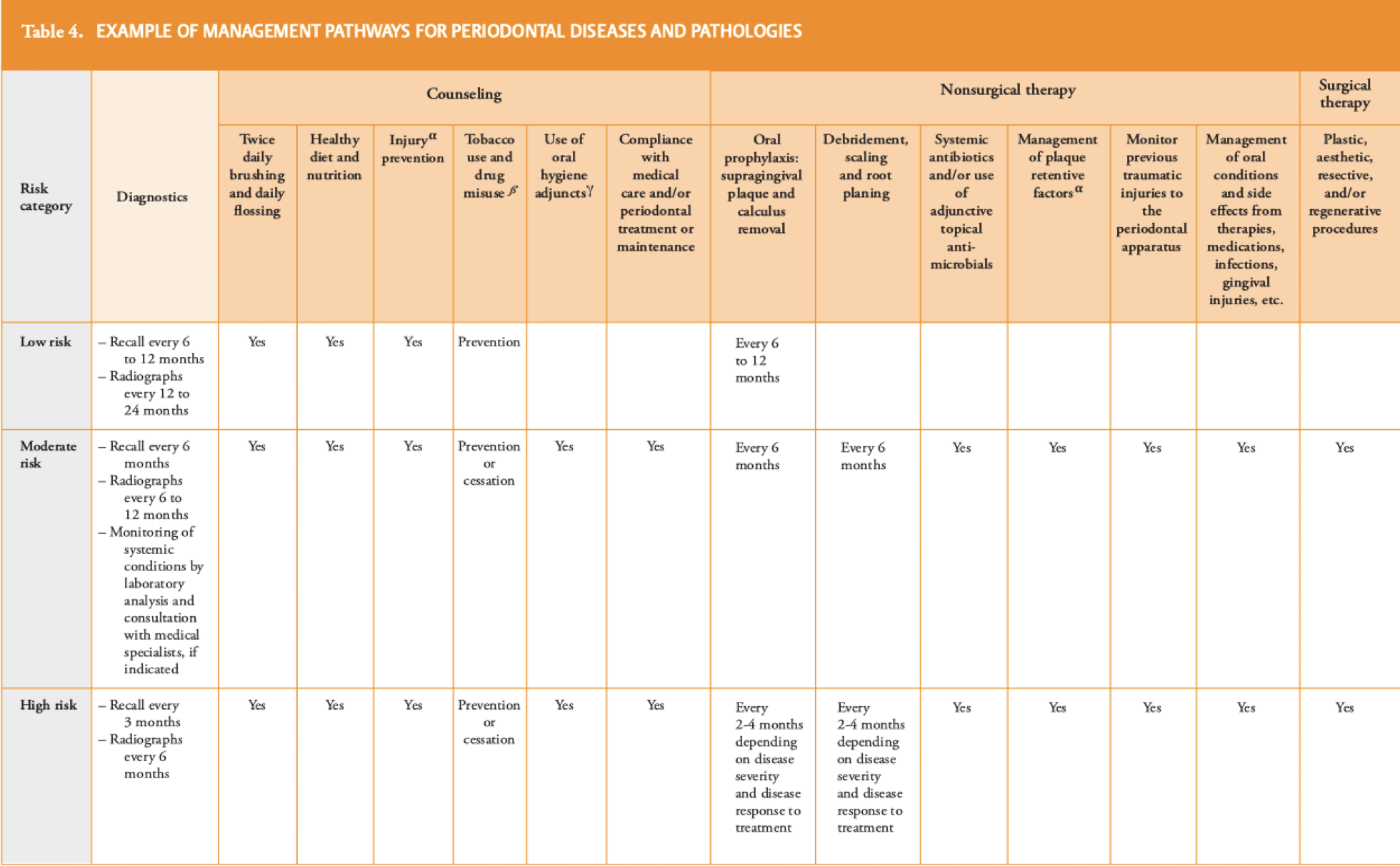
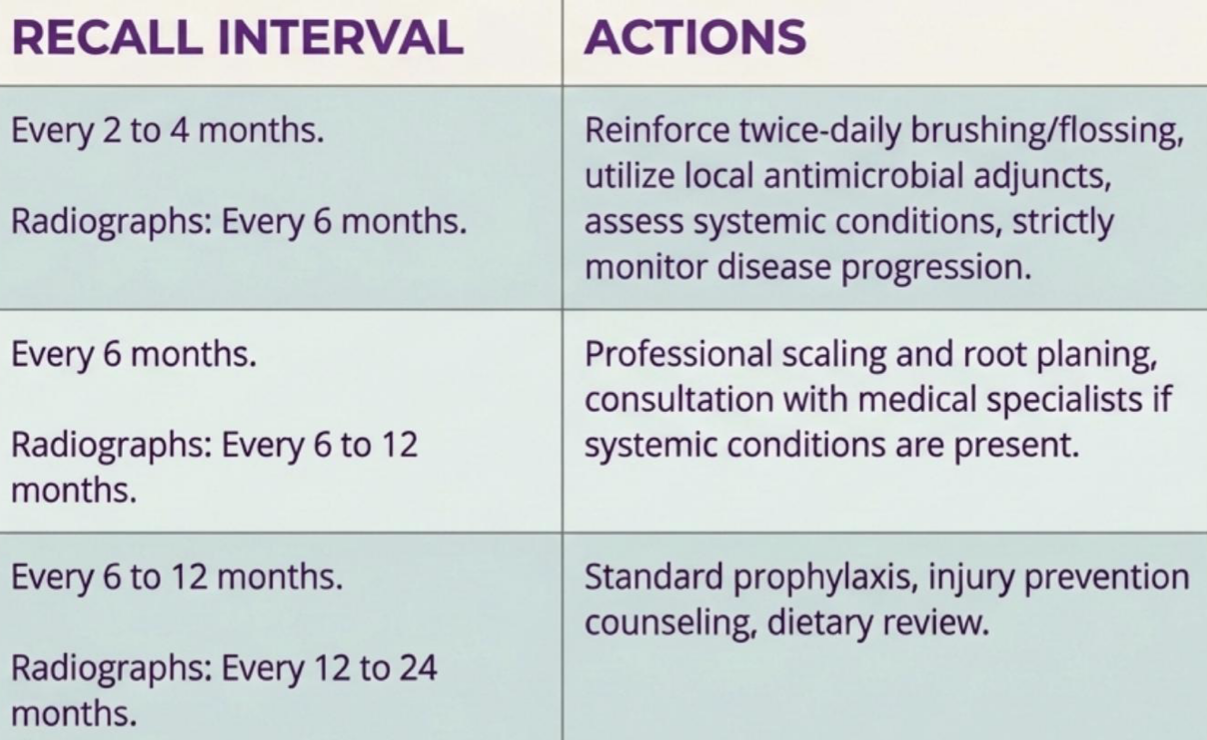
describe phases and dynamic clinical loop of perio
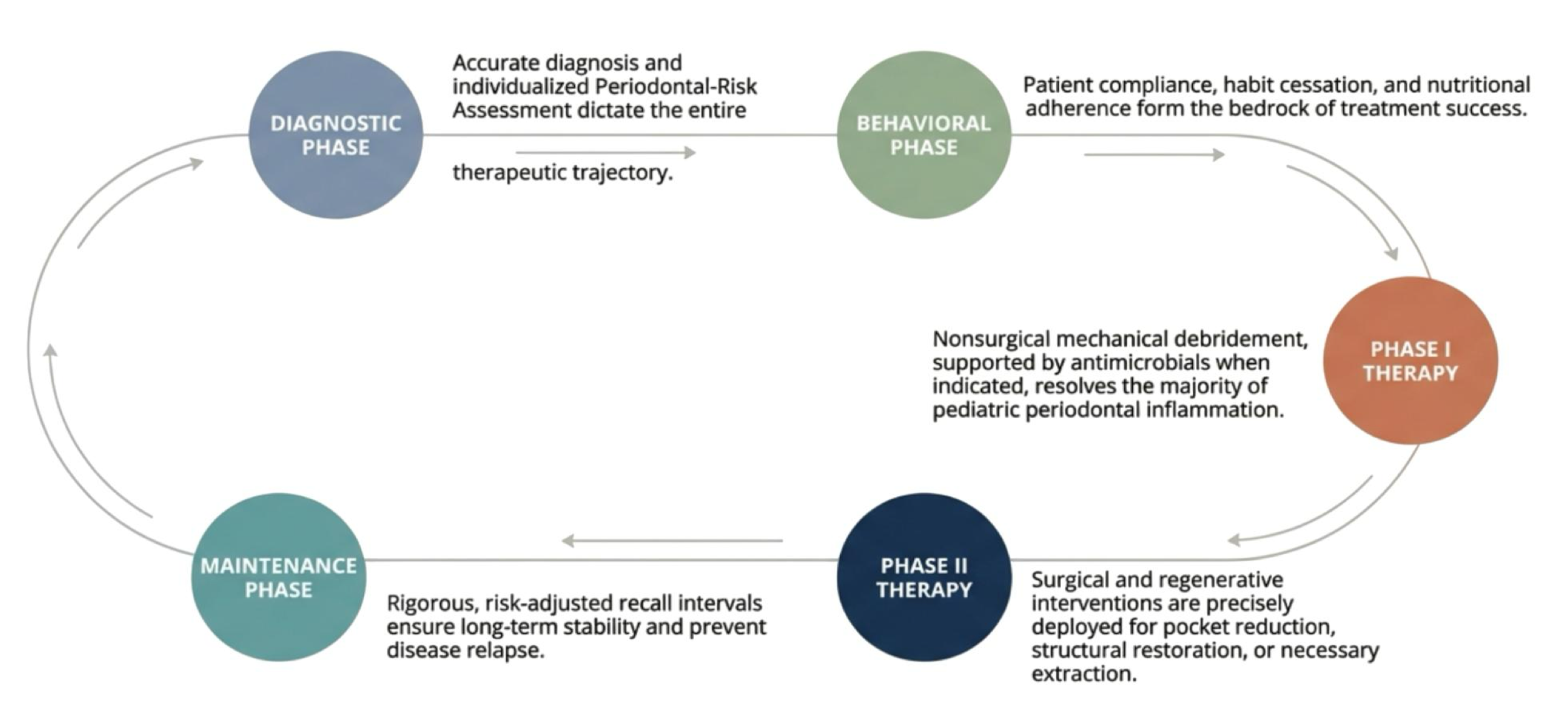
what three things are done is diagnostic phase for establishing baseline?
clinical probing, radiographic standards, risk assessment (PRA)
for peds when do you start comprehensive probing? when you would probe early?
after eruption of first permanent molars and incisors
before if if clinical/radiographic findings indicate disease → bop in primary teeth indicates high susceptibility
generalized gingivitis is ≥(?)% affected
30
which radiographic type is standard for diagnostic phase
bitewing
which radiograph rules out root resorption for anterior mobility?
periapical
for primary dentition normal height from CEJ to crest is?
1 ± 0.5 mm
bone loss for peds is
>2mm
a pseudopocket >3mm may be present around partially and newly erupted teeth
true
why would radiographs be essential for definitive perio diagnosis?
severe bone loss can exist beneath deceptively healthy-looking gingival tissue
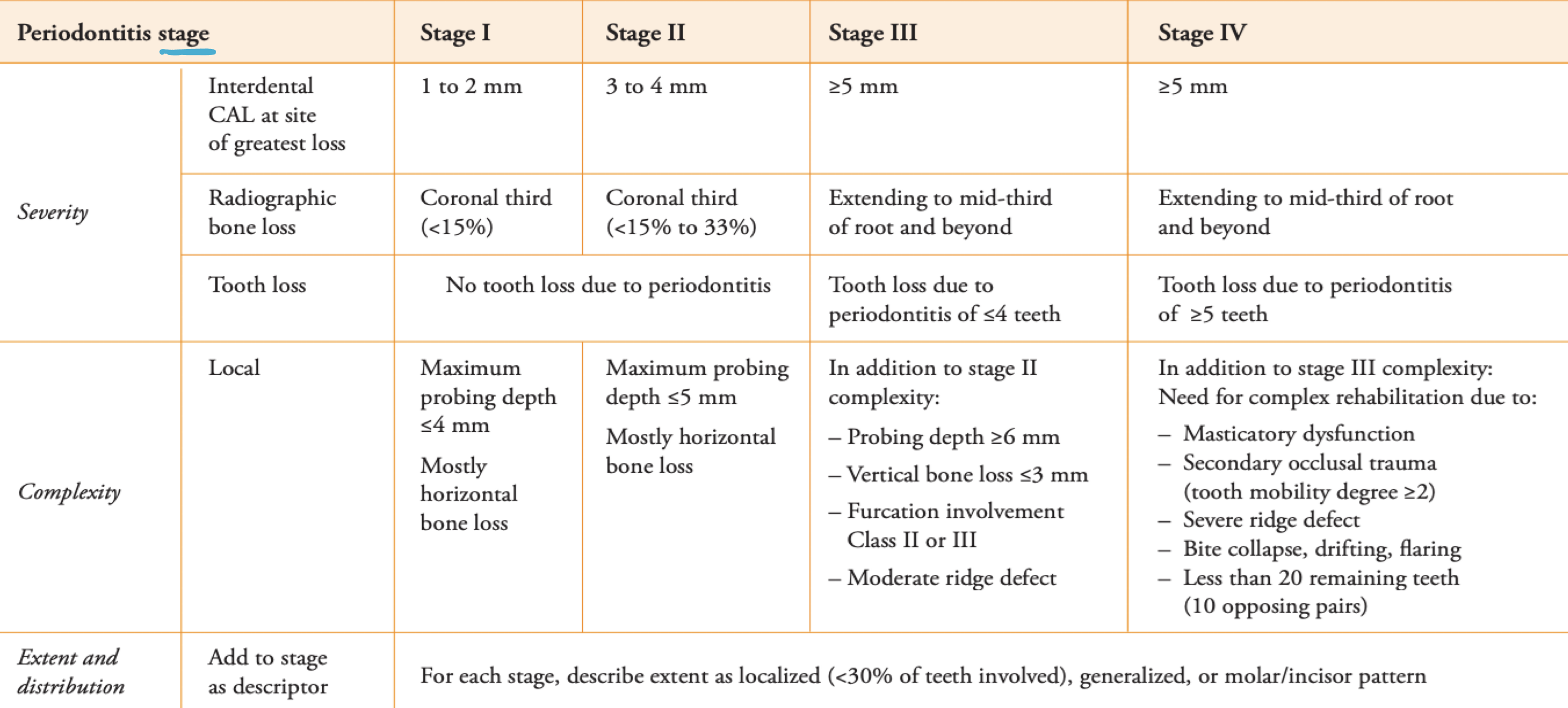
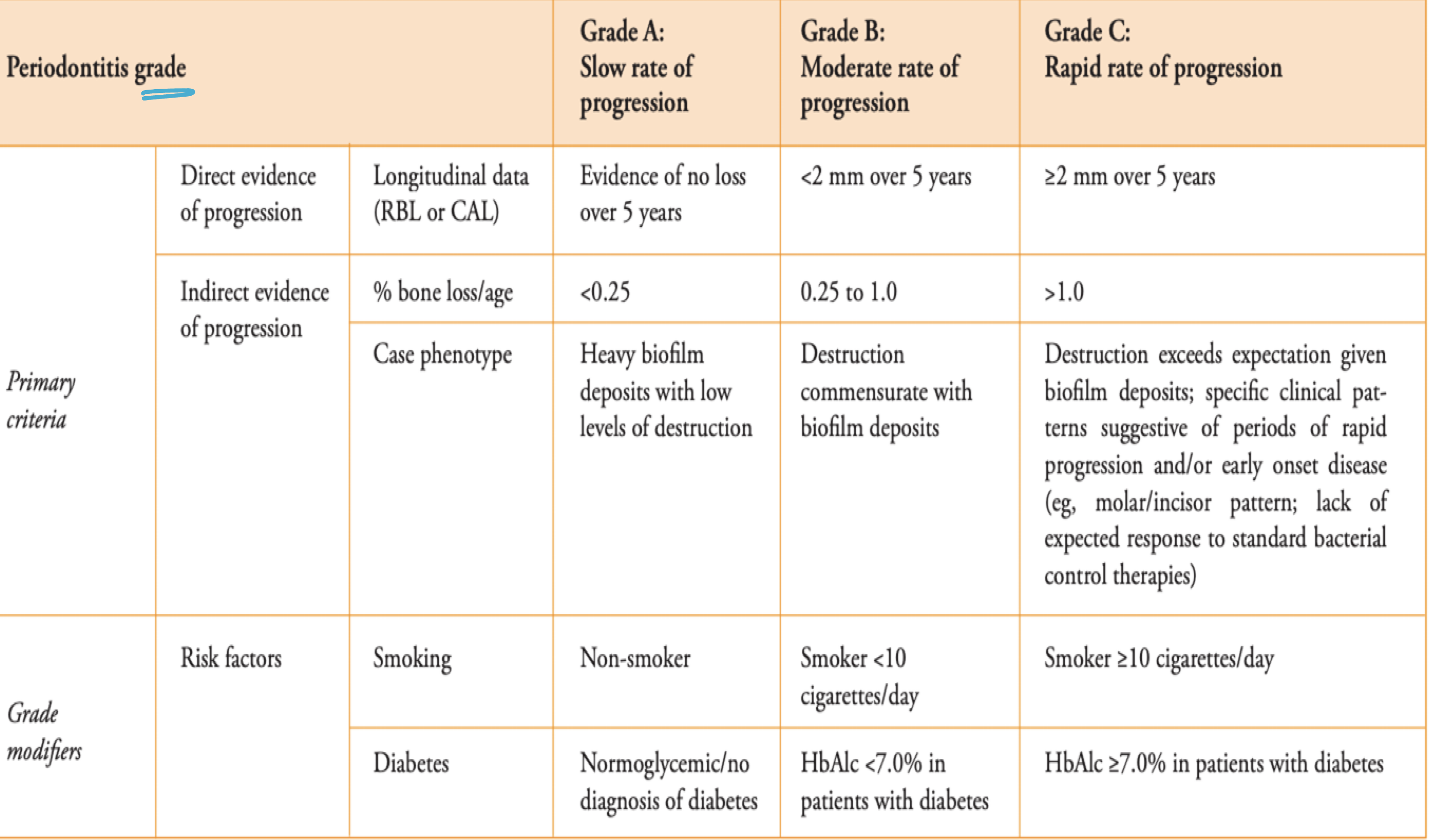
severity and extent of disease
staging
Assesses the future risk of periodontitis progression and anticipated treatment outcomes
grading
perio stage and grade
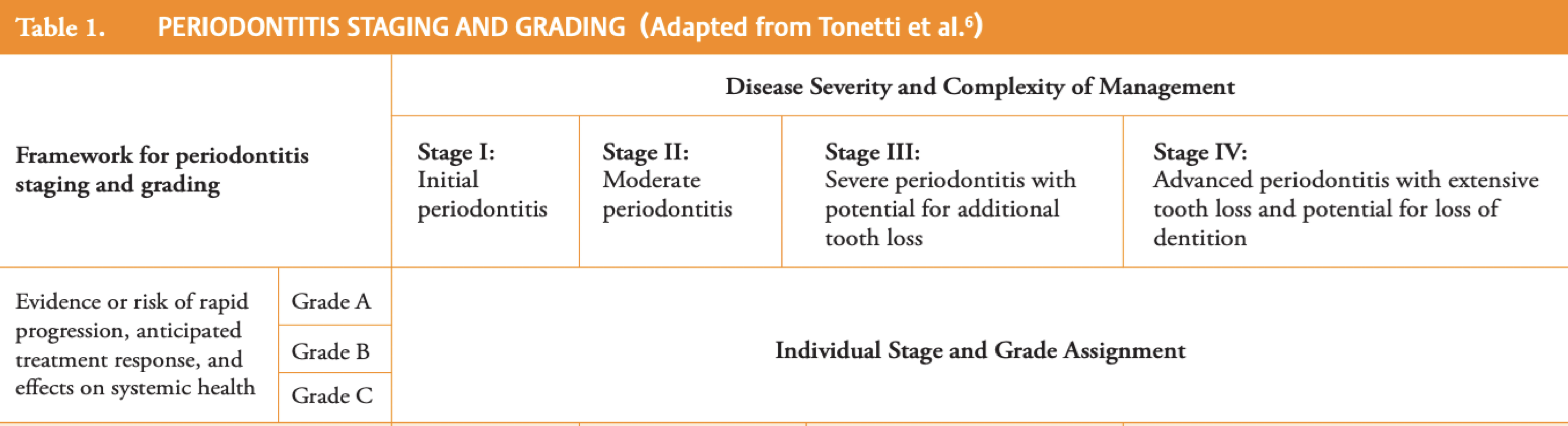
staging
grading
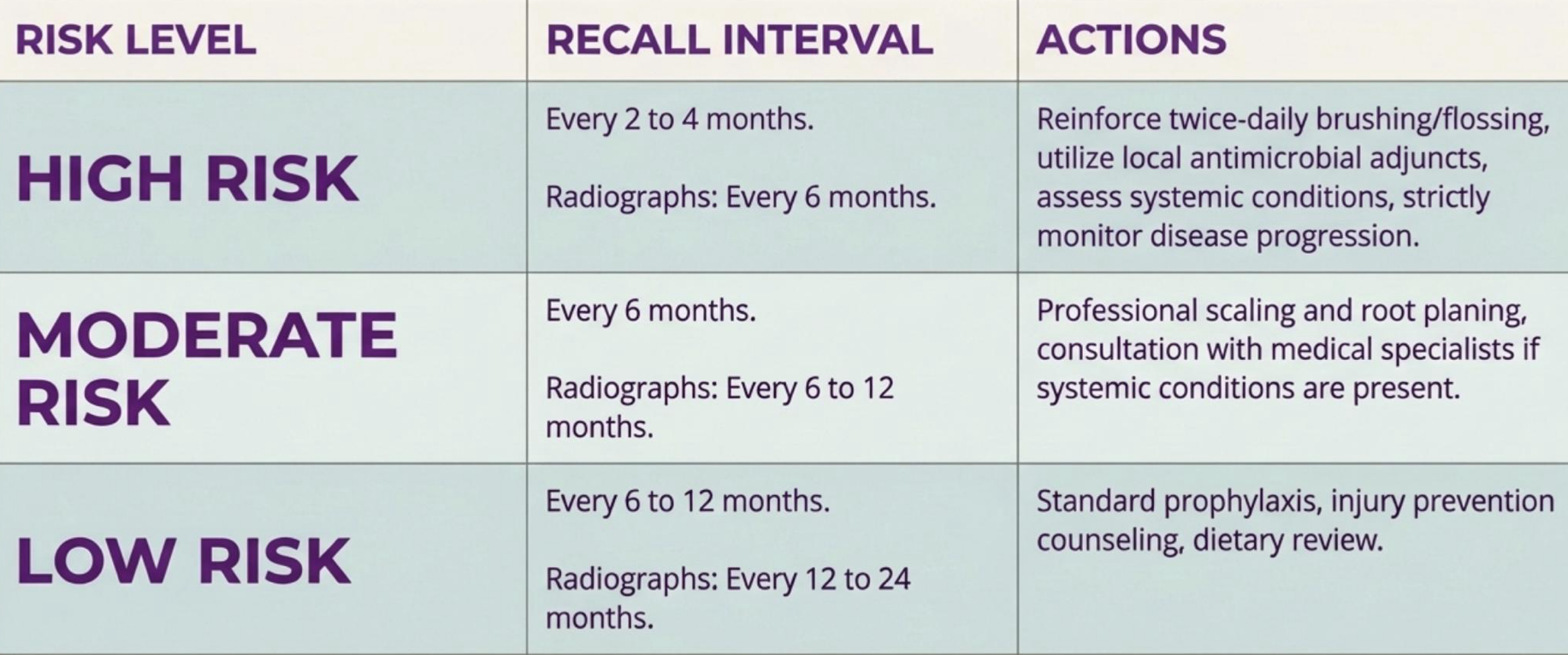
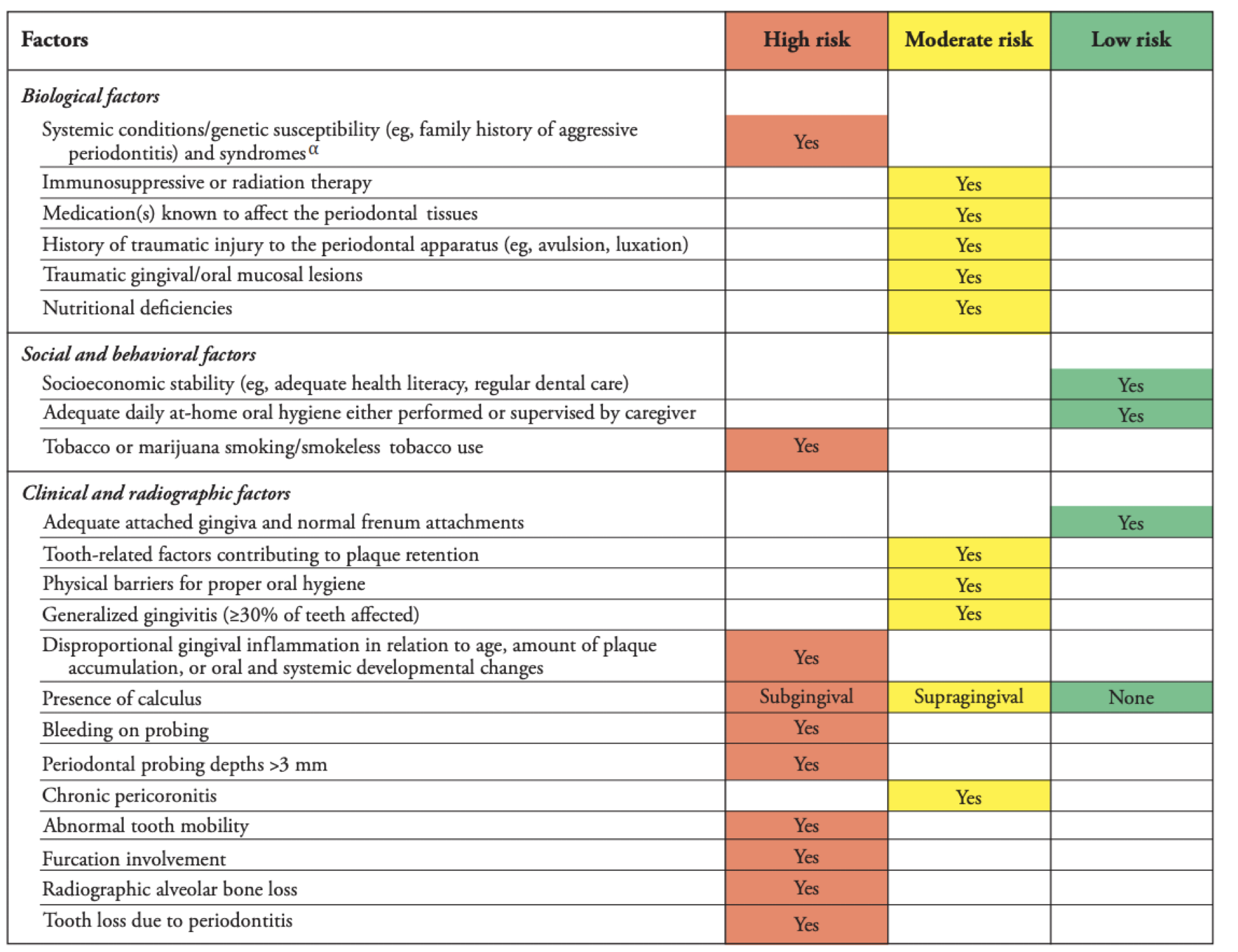
perio risk assessment <13 y/o
perio risk assessment ≥13 y/o
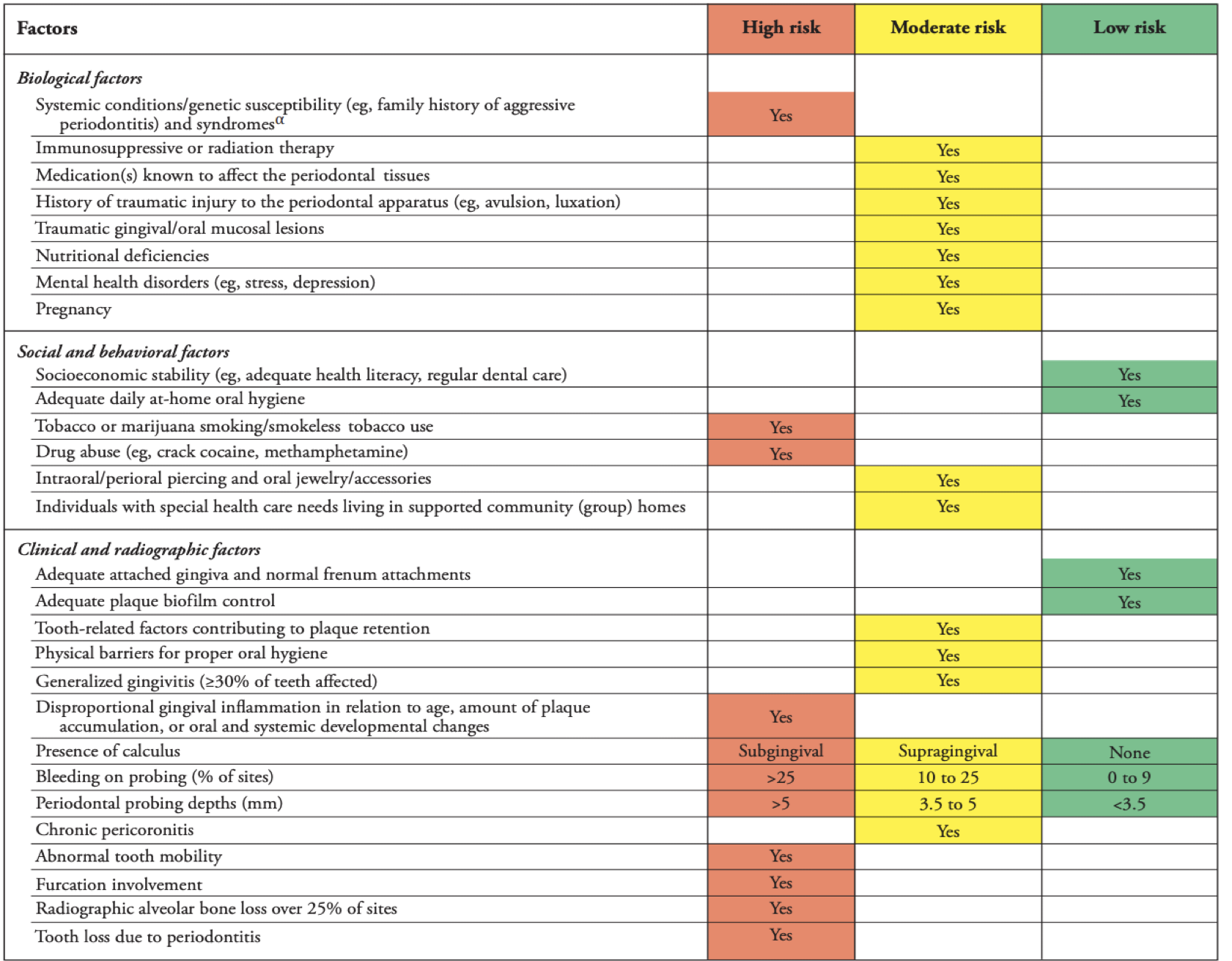
HIGH RISK INDICATED BY:
Periodontal probing depths > 5 mm
Bleeding on probing > 25% of sites
≥13 y/o
HIGH RISK INDICATED BY:
Periodontal probing depths > 3 mm
Bleeding on probing (any amount)
<13 y/o
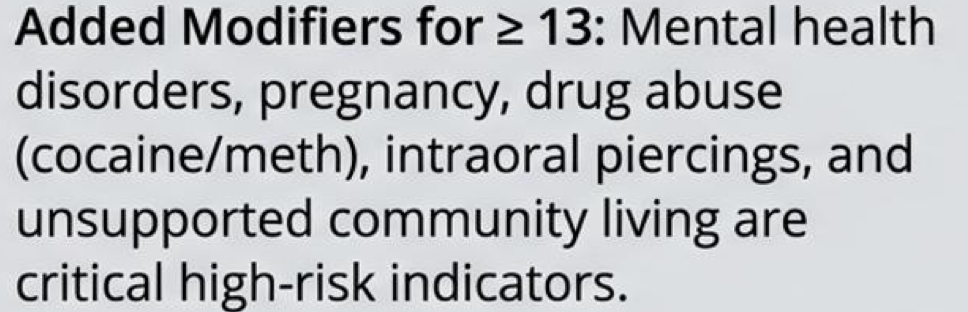
what are some age modifiers for high risk perio
GOAL: Debridement, scaling, and root planing to remove subgingival plaque, calculus and contaminated cementum
Hand instruments – smoother root surfaces
Ultrasonic scalers – less soft-tissue trauma, faster but avoid for patients unable to expectorate or at risk of aspiration
(systematic reviews show similar results)
phase I: mechanical plaque and local factor control
what are some restorative factors to consider?
Restore open, cavitated lesions causing food impaction
Smooth or replace defective restorations with overhangs
Ensure preformed crowns are well-adapted, contoured, and crimped
what are some orthodontic and enamel factors?
Suspend orthodontic treatment if the patient cannot maintain proper oral hygiene
Use desensitizing toothpastes, fluoride varnishes, and sealants for enamel defects (amelogenesis imperfecta) to reduce sensitivity and improve brushing compliance
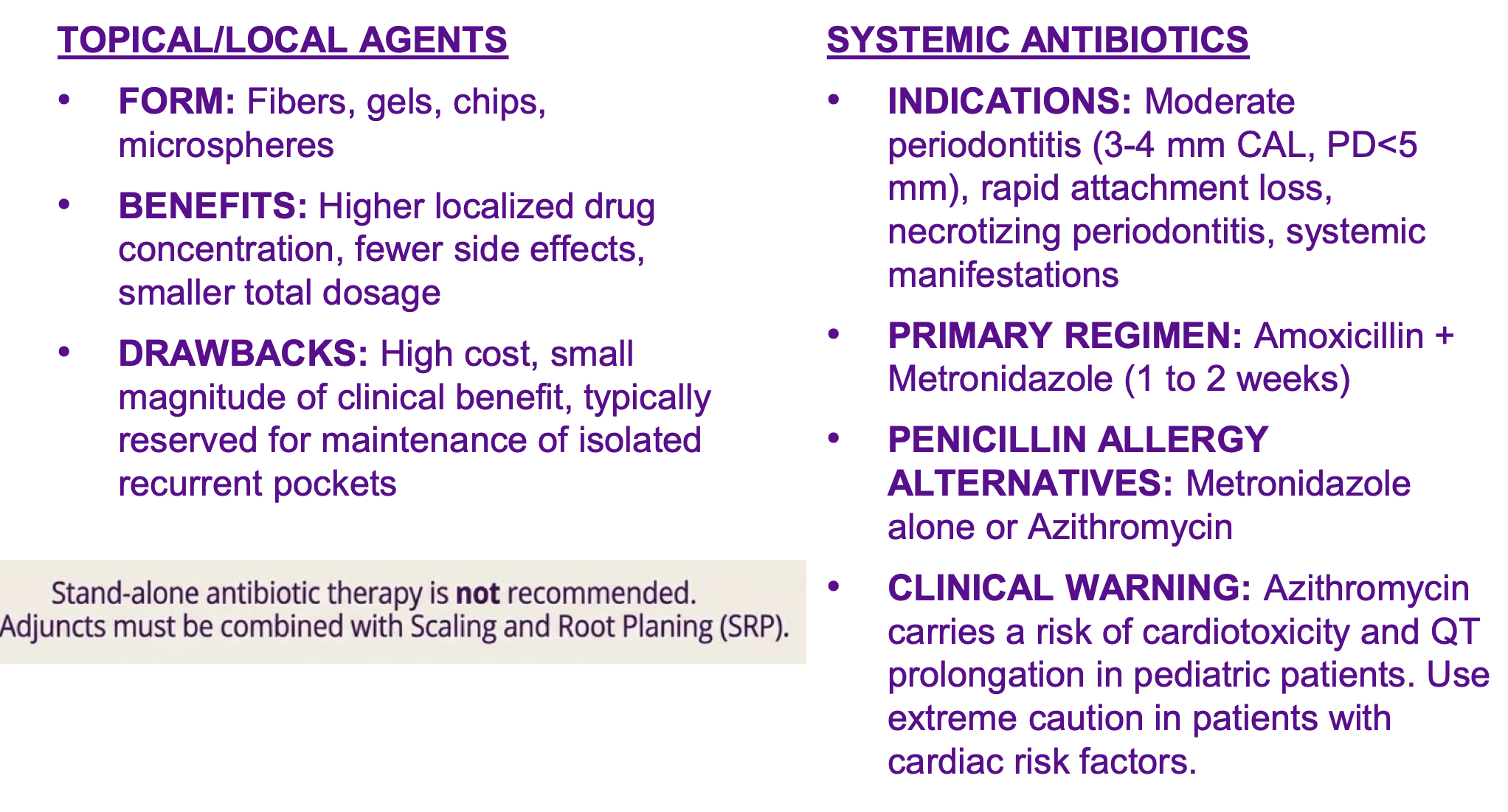
14 y/o pt w aggressive perio characterized by rapid attachment loss and pocket depths of 5mm. do you prescribe antibiotics? if using adjunctively what is the gold standard?
ab but also srp! no stand alone ab
antimicrobial adjuncts
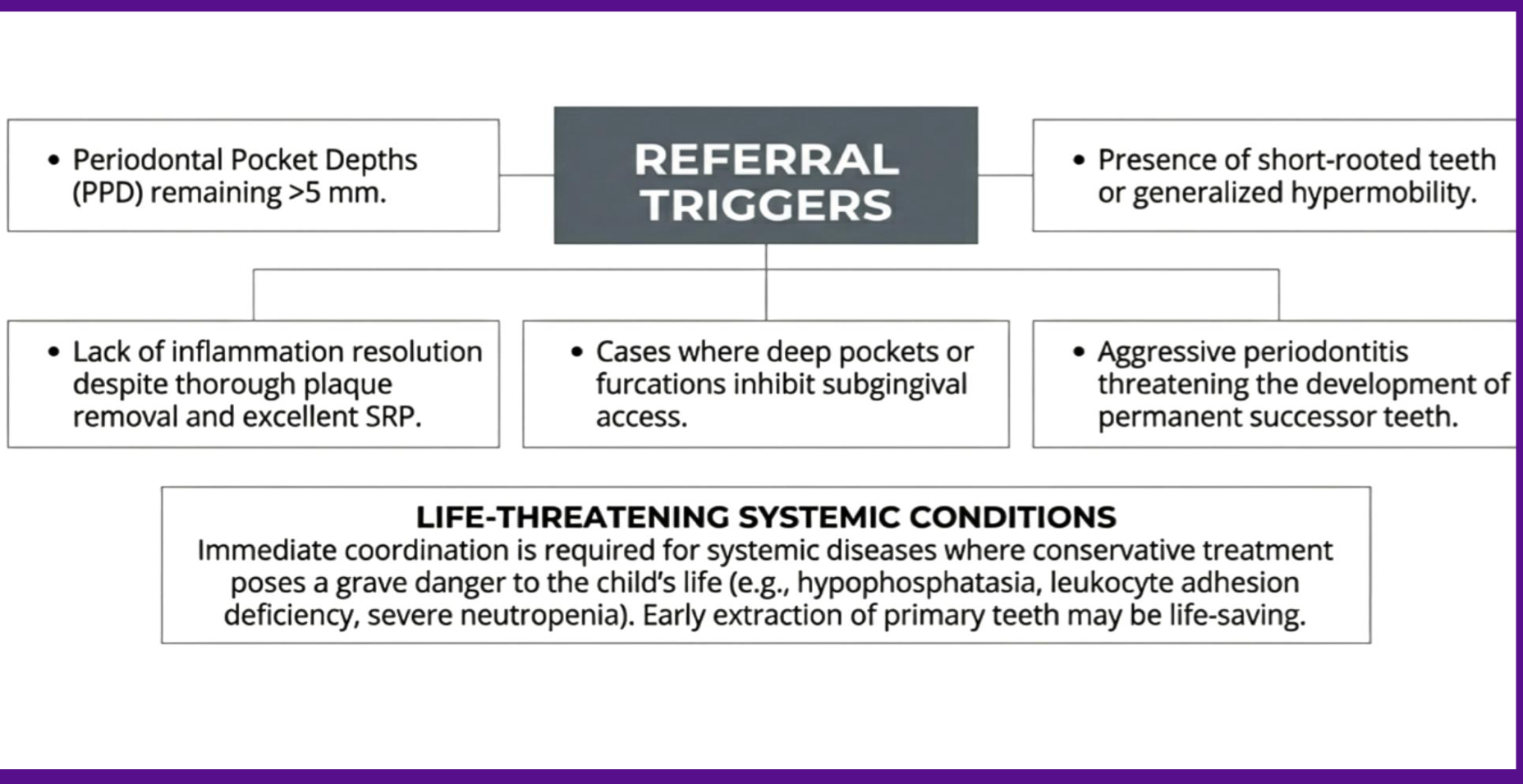
when do you refer?
what are some surgical interventions (phase II)?

can you place implants on a 15 y/o? why or why not?
no, not until all bone growth complete 18 for gurls 21 for boys, otherwise infraocclusion and twisting of implant w growth
diagnostic standard for implant placement
chronological age is insufficient, skeletal maturation must be assessed via cephalometric analysis or hand-wrist radiographs
what would be the best management for periodontally compromised teeth if implants/regen are not viable?
extraction
which phase
maintenance
long term success relies entirely on quality of supportive perio therapy to prevent disease relapse