Posterior Fossa- IAC
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
Common Indications IAC:
Asoustic neuroma
facial palsy/numbness
hemifacial spasm
IAC: Patient lies supine on the examination table with their head within the head coil.
The head is adjusted so that the interpupillary line is parallel to the table and the head is straight.
IAC: Longitudinal alignment light lies in the midline and the horizontal alignment light passes through
the nasion
Slice coverage for saggital IAC
R —> L entire brain
Sequences sag. IAC
T1: SE, FSE, incoherent GRE
FOV sag. IAC
220-240 × 100%
Sag IAC phase
A —>P
Matrix sag. & coronal IAC
256-320 × 75-100%
Slice/gap sagittal IAC
5/1, 4/1
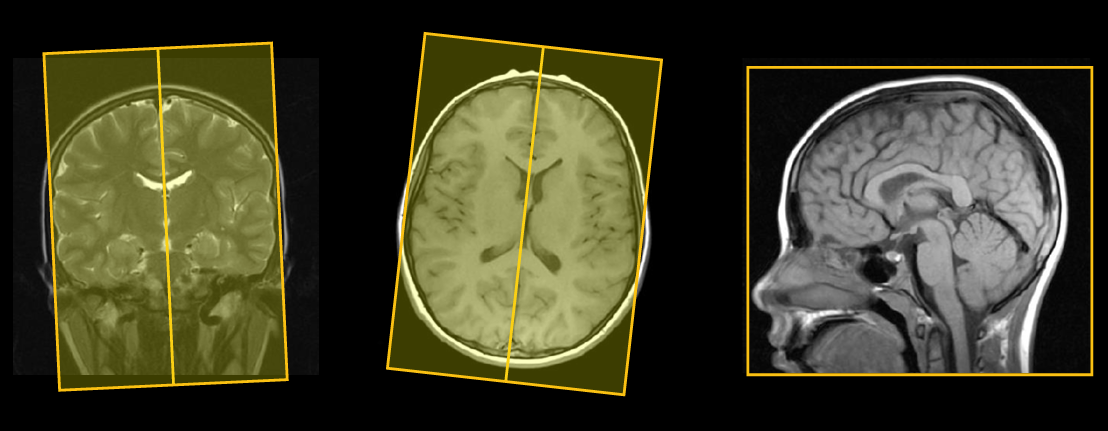
Slice angulation for sagittial IAC: coronal and axial
parallel to the midline
Axial coverage for IAC
S —> I from foramen magnum to superior border of petrous ridge
Axial IAC sequenes
T1: SE, FSE, 3D incoherent GRE*
T2: SE, FSE
Axial and coronal IAC FOV:
180-200 × 100%
Axial phase IAC:
R —> L
Axial matrix IAC:
256-512* x 75-100%*
Axial slice/gap IAC:
3/1, 0.5/0* (512×100% matrix)
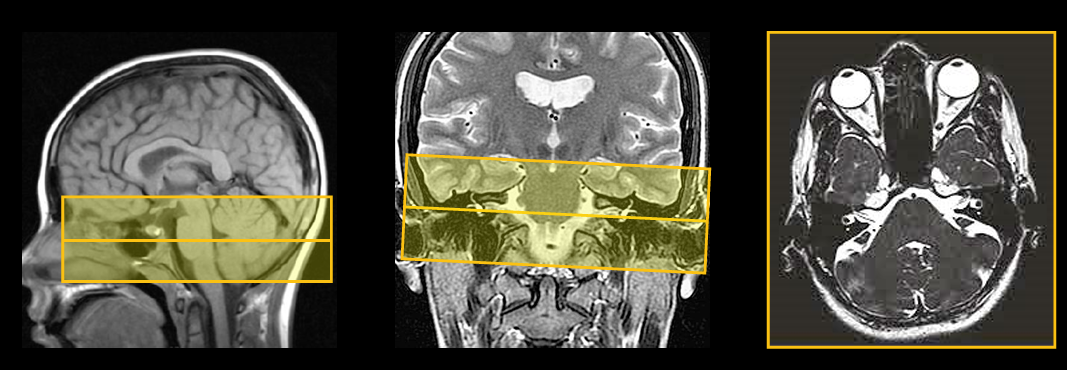
Slice angulation for axial IAC: Sagittal and coronal
Parallel to IAC/cochlear nerves
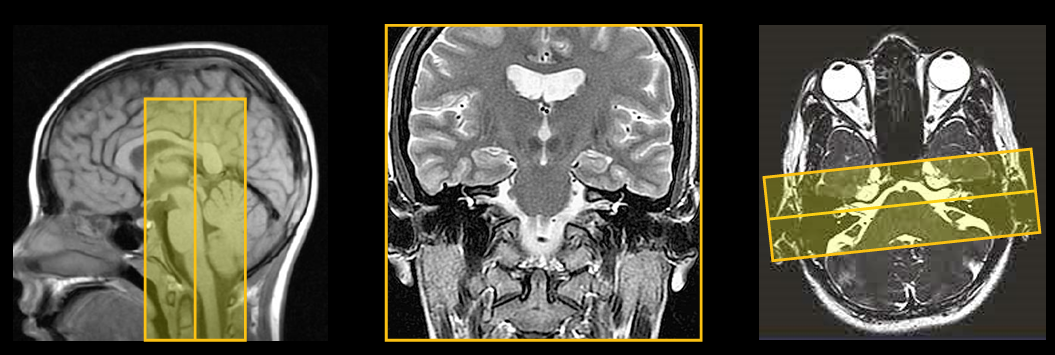
Coronal slice coverage for IAC
A —> P cerebellum to clivus
Coronal sequences IAC
T1: SE, FSE
T2: SE, FSE
coronal phase IAC
R —> L
Coronal IAC slice/gap
3/1
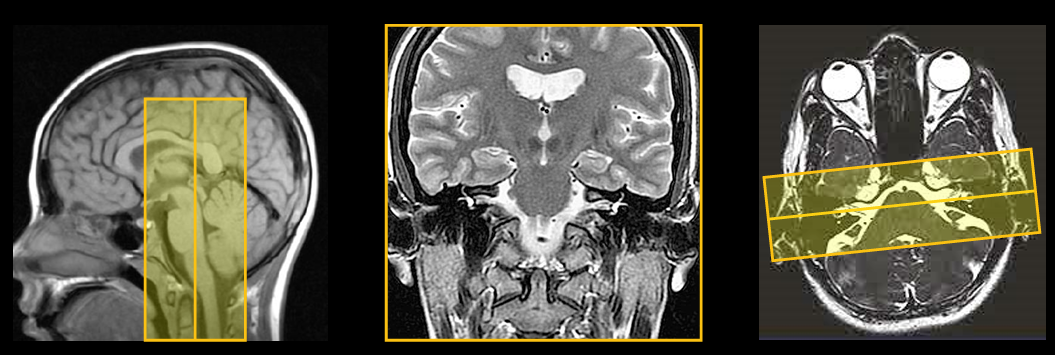
Slice angulation for coronal IAC: Sagittal and axial
Sagittal is perpendicular to the ACPC line. Axial is parallel to the CN VIII nerves
Technical issues for IAC:
IAMs are very small structures and this examination is usually carried out to exclude a small acoustic neuroma situated within the canal.
Therefore, it is important to achieve the highest spatial resolution possible in keeping with good SNR.
To optimize spatial resolution even further, the FOV is reduced compared with standard brain imaging.
As a result of all these measures, the NEX/NSA may have to be increased to maintain SNR.
IAC is mostly T2 sequences. T1-weighted sequences yield low inherent contrast
Artifact for IAC:
Flow motion from the venous sinuses is often troublesome in the posterior fossa.
GMN minimizes this artifact but it not only increases the signal in vessels but also the minimum TE available and is therefore reserved for T2-weighted sequences.
Spatial presaturation pulses placed Superior and Inferior to the FOV are also beneficial.
Contrast usage for IAC:
As T1-weighted sequences yield low inherent contrast between the petrous ridge and the IAM and acoustic neuromas demonstrate good enchantment, contrast is usually necessary.