Looks like no one added any tags here yet for you.
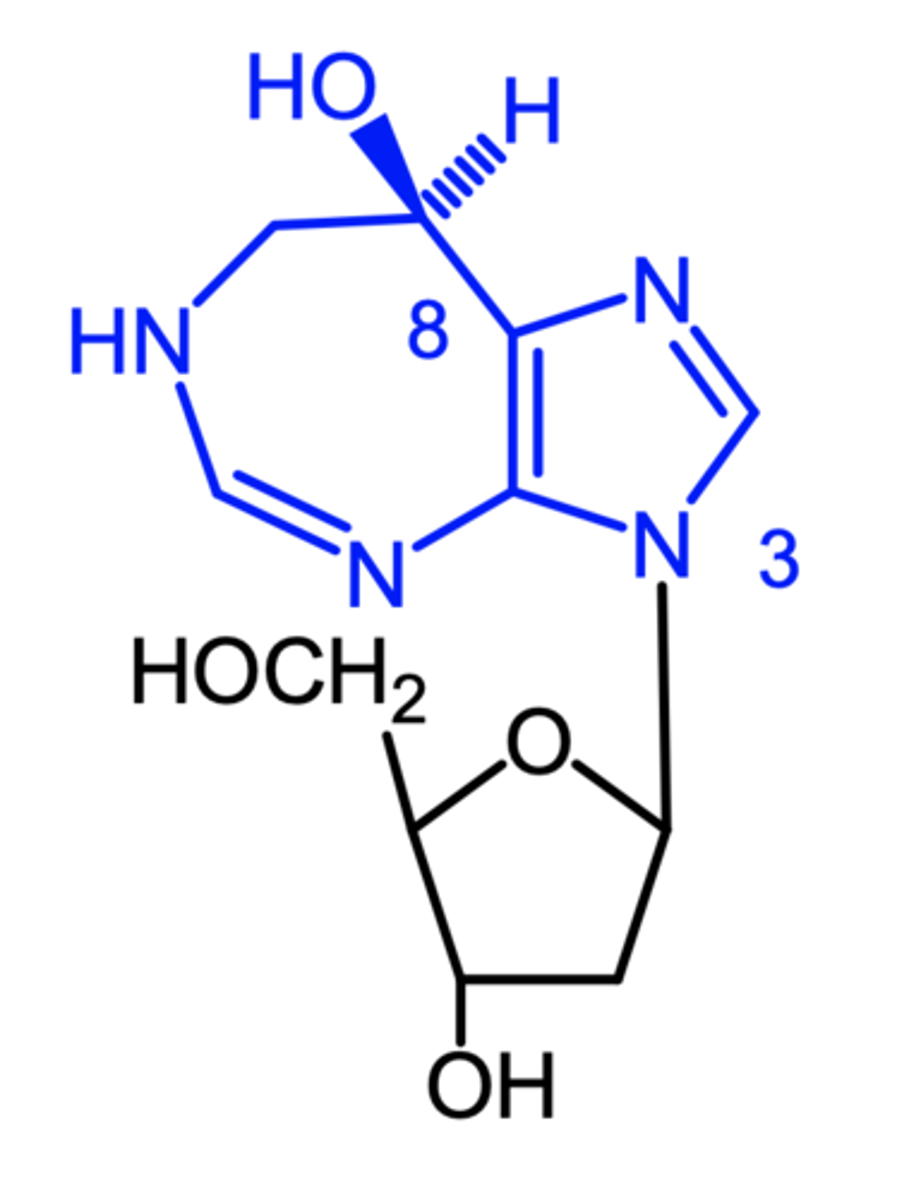
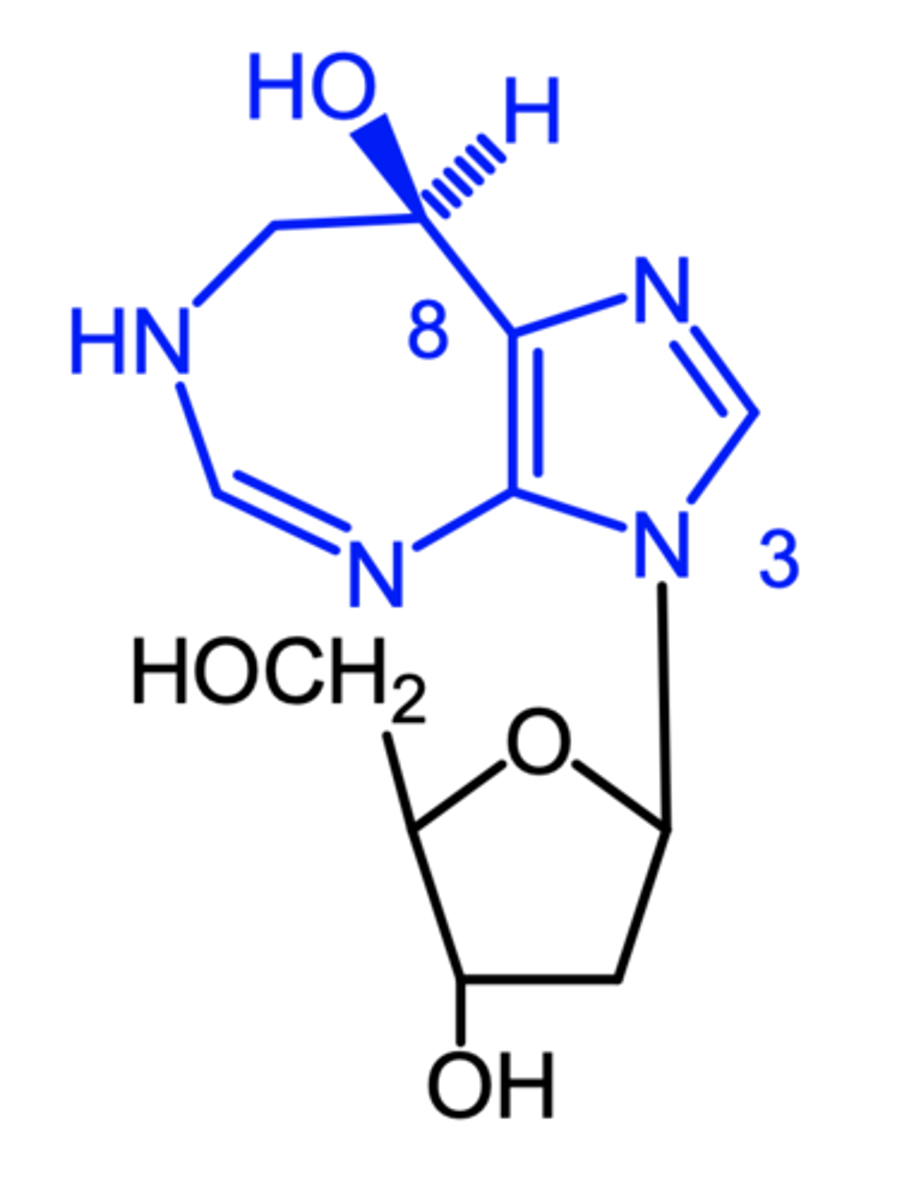
pentostatin
pentostatin
(misc antimetabolite)
ROA: IV
MOA: indirect inhibition of ribonucleotide reductase
- inhibits adenosine deaminase, which leads to high levels of deoxyadenosine = inhibitor of ribonucleotide reductase, leading to stopping DNA synthesis in tumor cell
indication: b-cell chronic lymphocytic leukemia
- similar efficacy to fludarabine, but lower toxicity
AE: myelosuppression, rash
pentostatin
which b-cell chronic lymphocytic leukemia agent has less toxicity?
a. pentostatin
b. fludarabine
microtubules, mitotic arrest, apoptosis
Mitosis Inhibitors:
inhibits mitosis (cell division) by disrupting ______ of the spindle apparatus, which pulls the cell apart + divides
by inhibiting this essential hyperdynamic change in structure, it results in _____ ______ and ______
b-tubulin, elongation, disassembly
MOA of taxanes:
bind to polymerized ____ promoting stable tubulin conformation, which then renders the microtubules resistant to depolymerization + prone to polymerization.
this promotes the ______ phase of the microtubule dynamic instability at the expense of the shortening phase + inhibits the _______ of the tubule into the mitotic spindle
this whole process disrupts the normal process of cell division
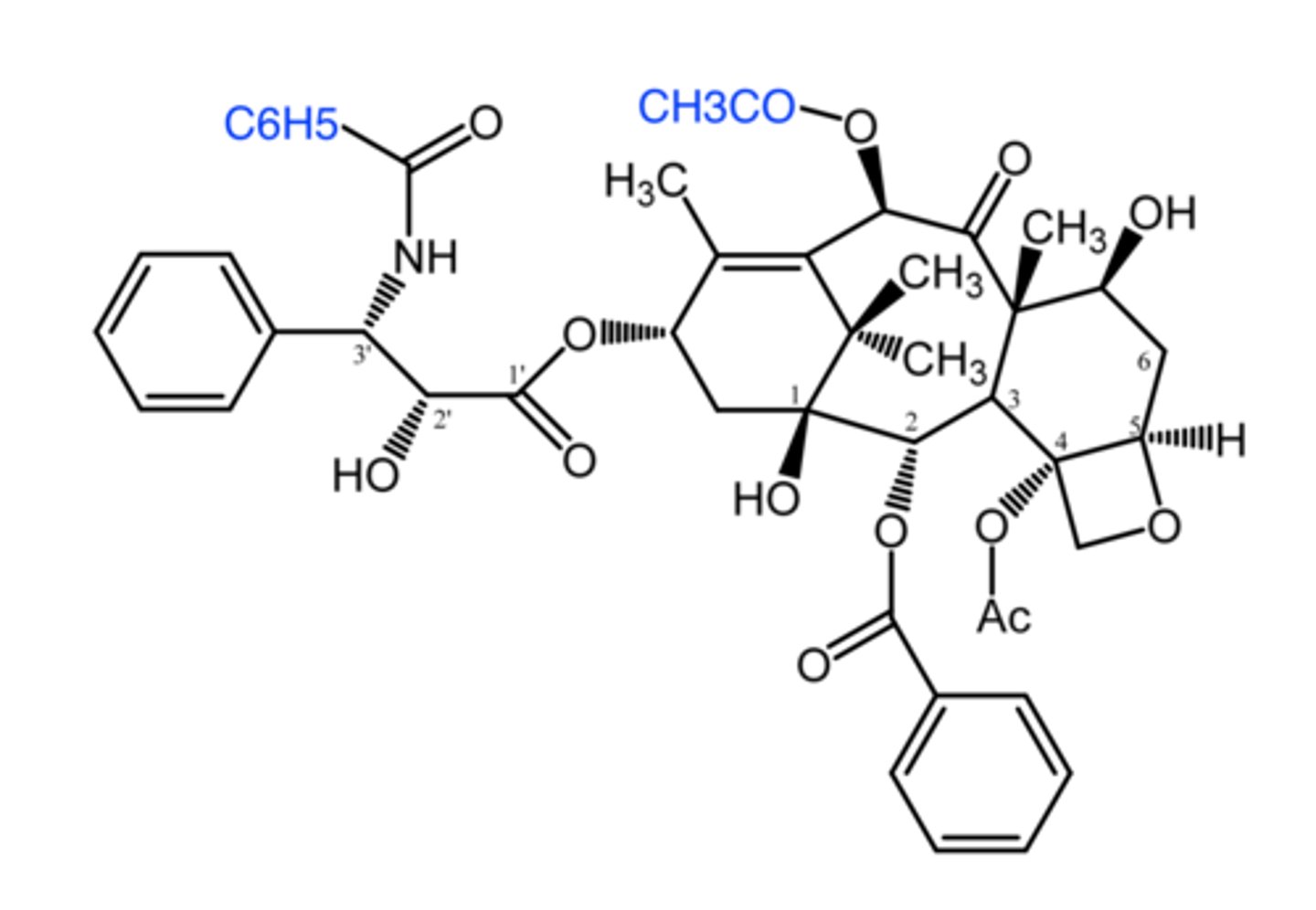
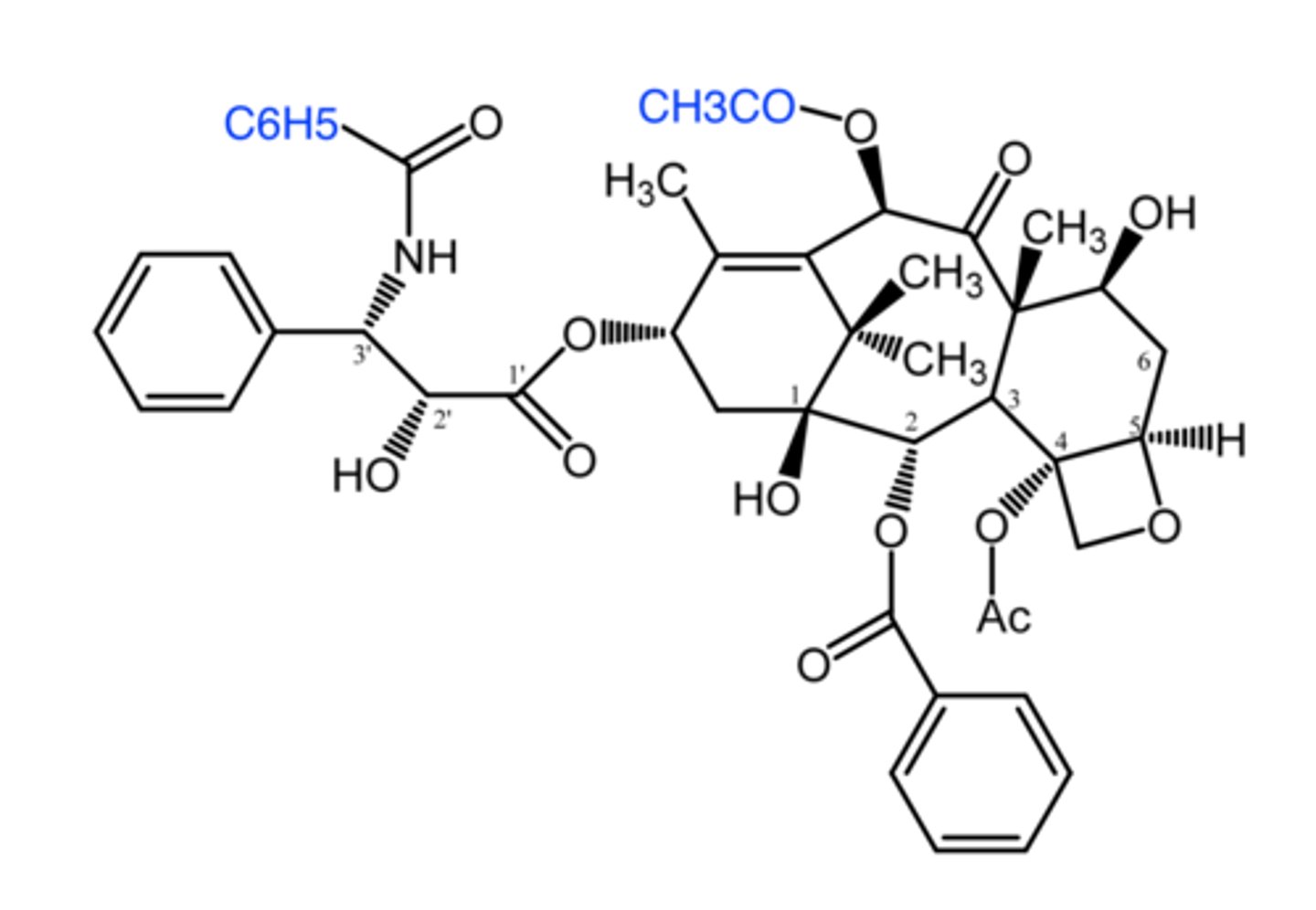
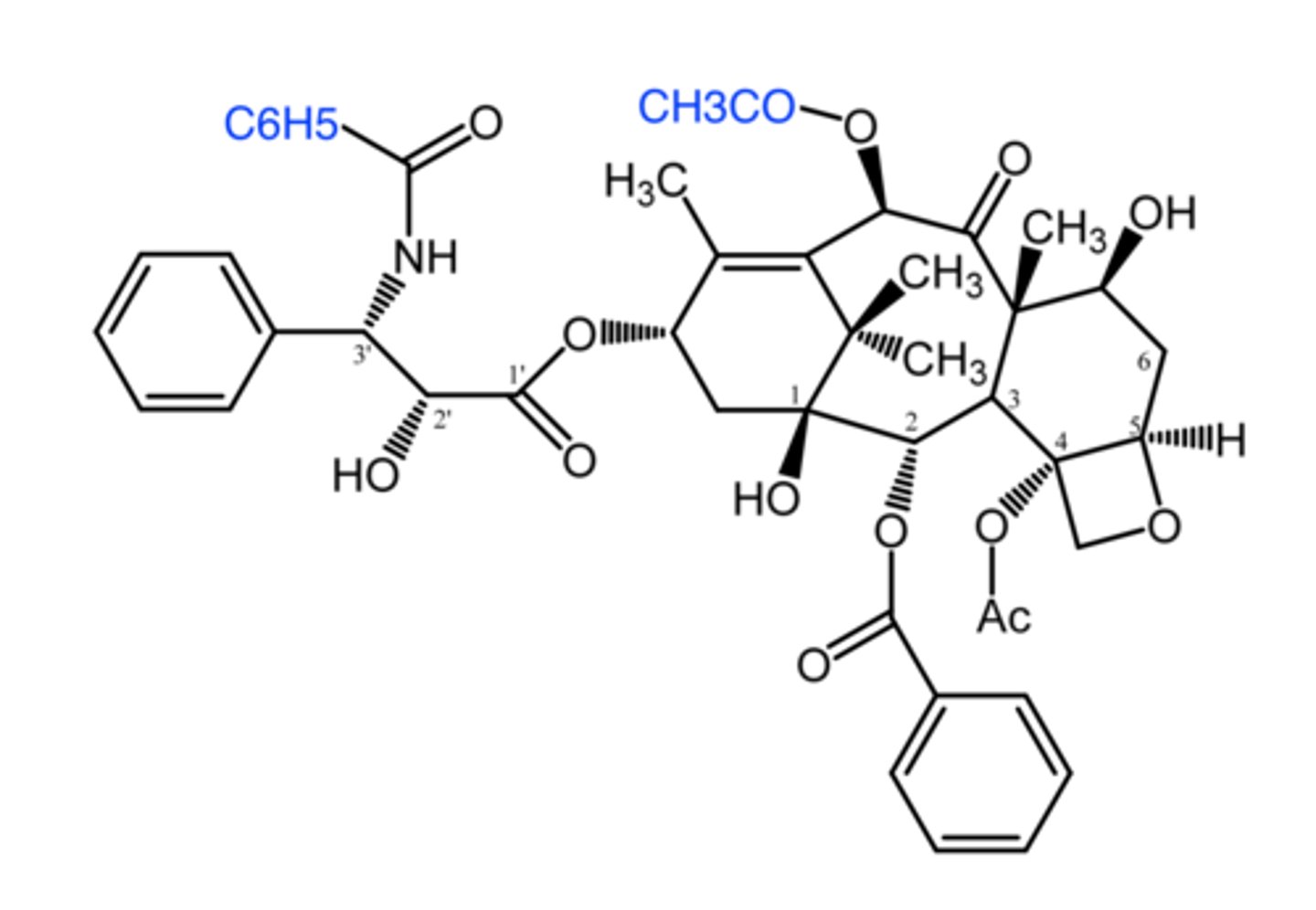
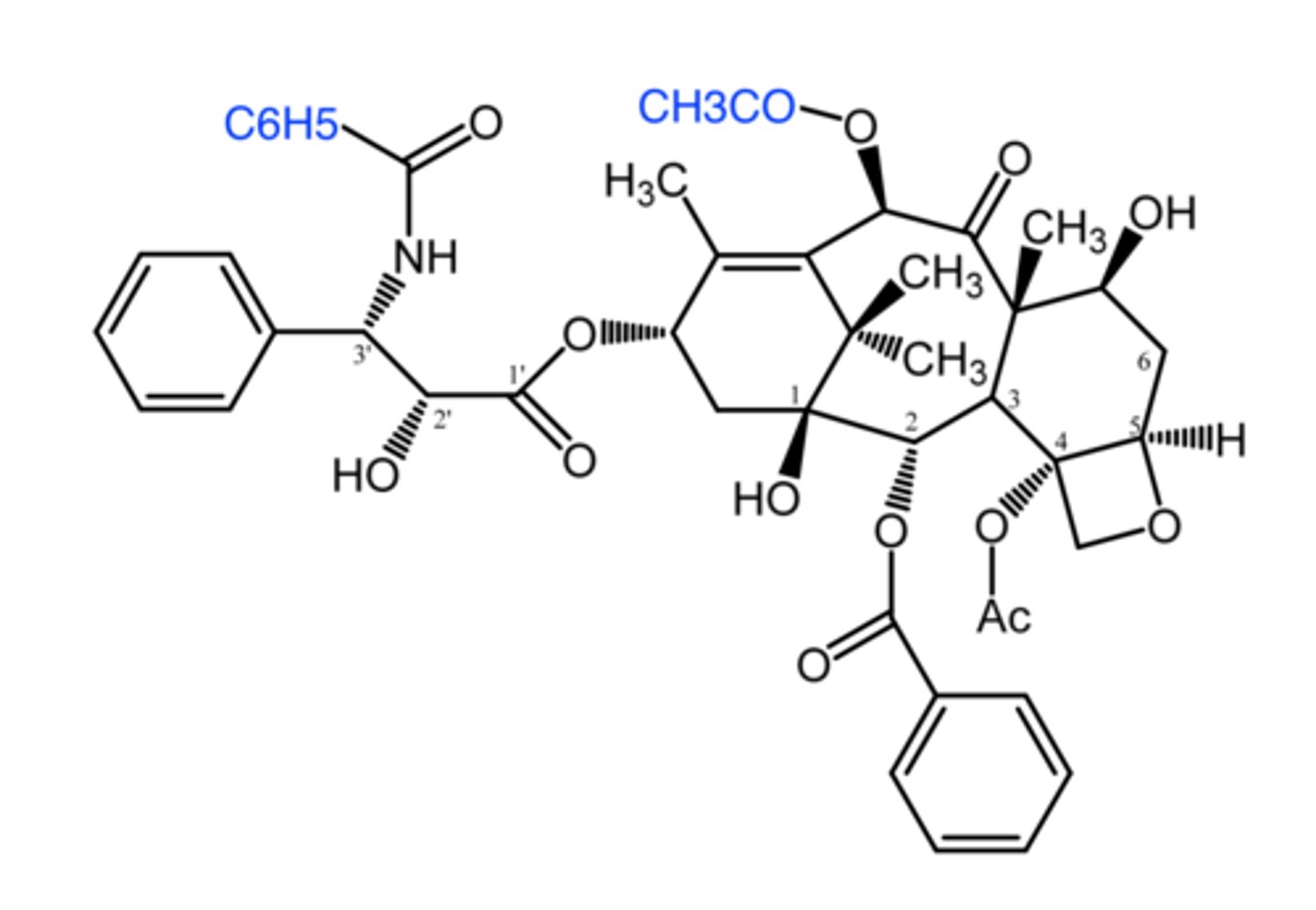
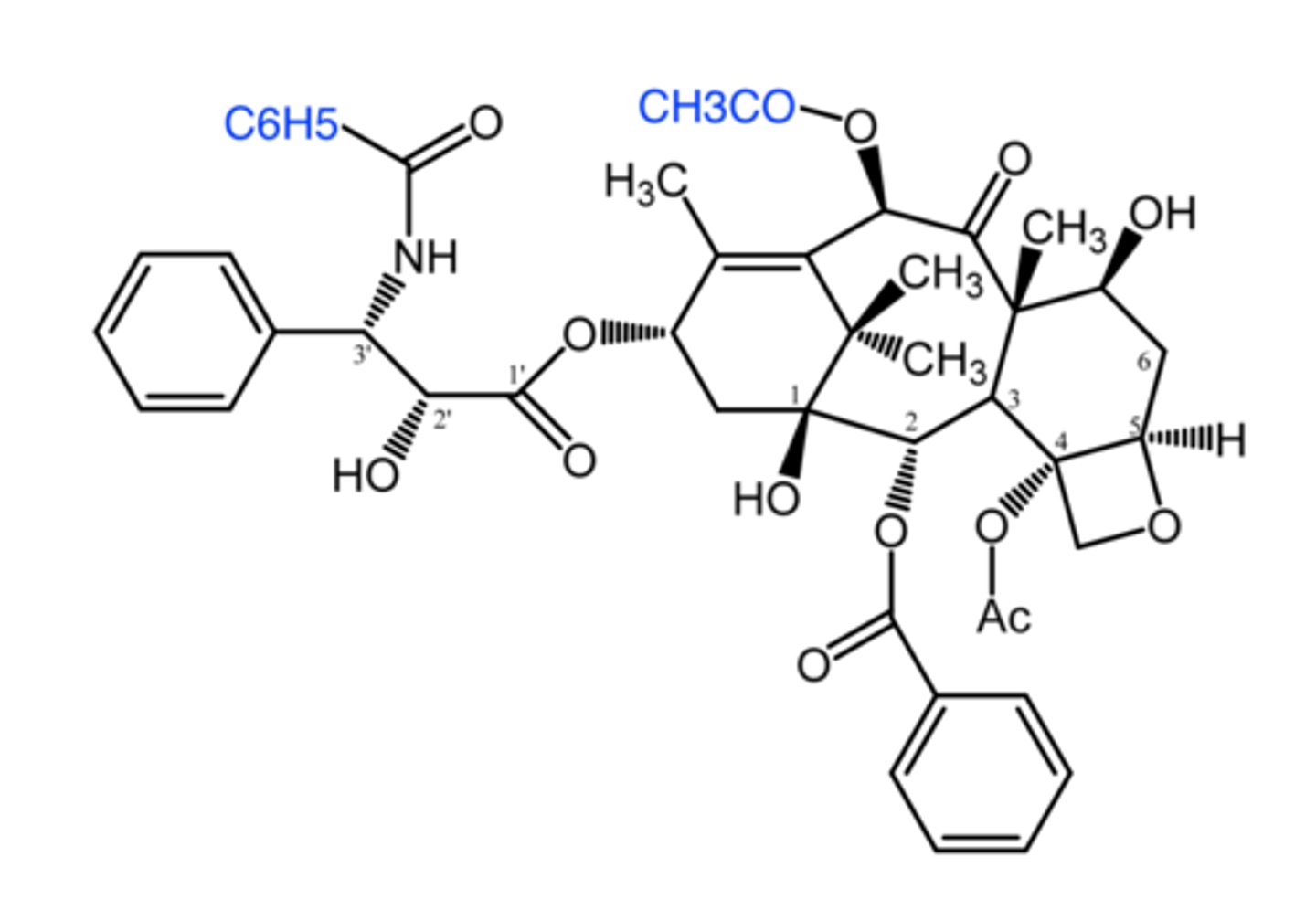
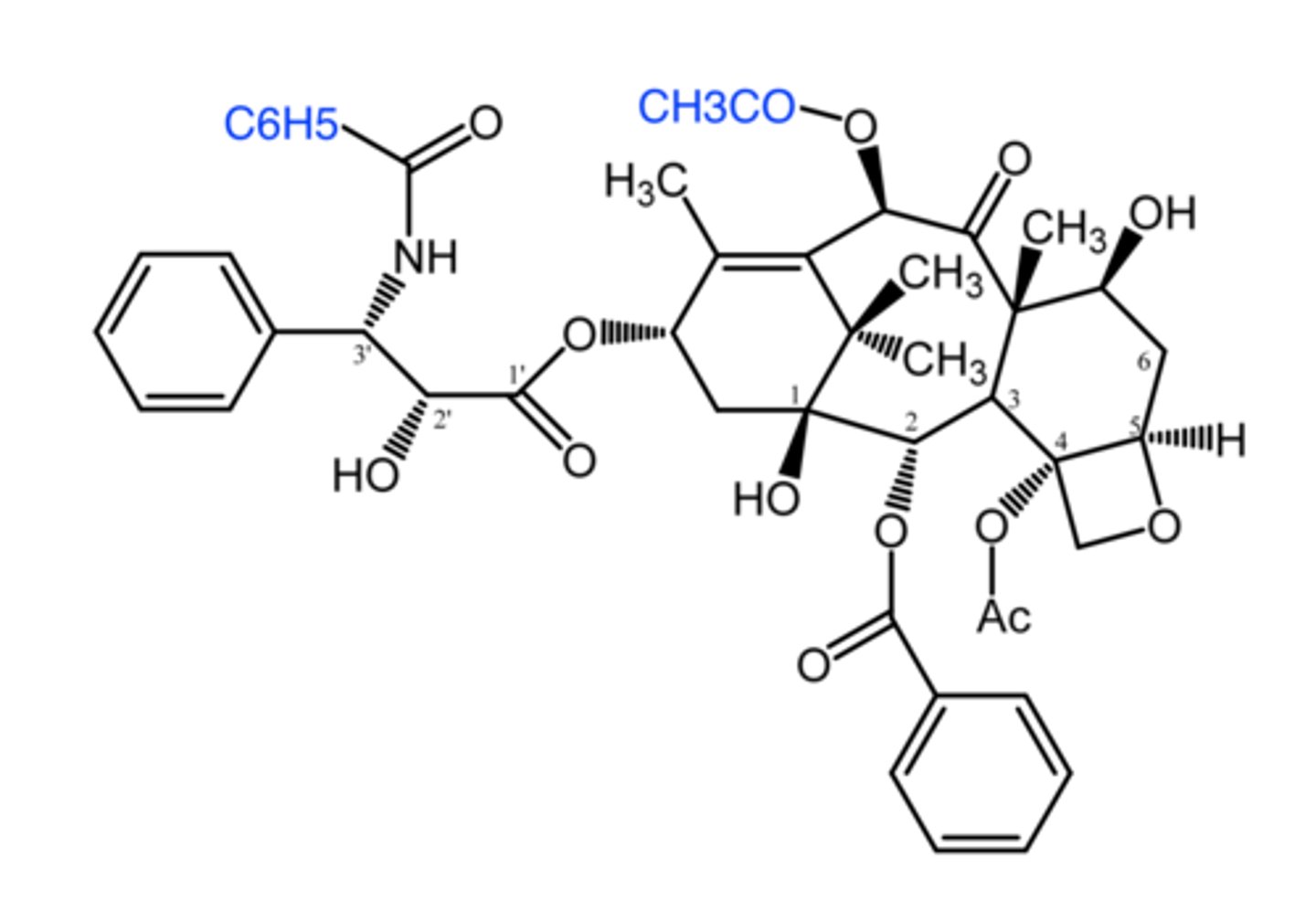
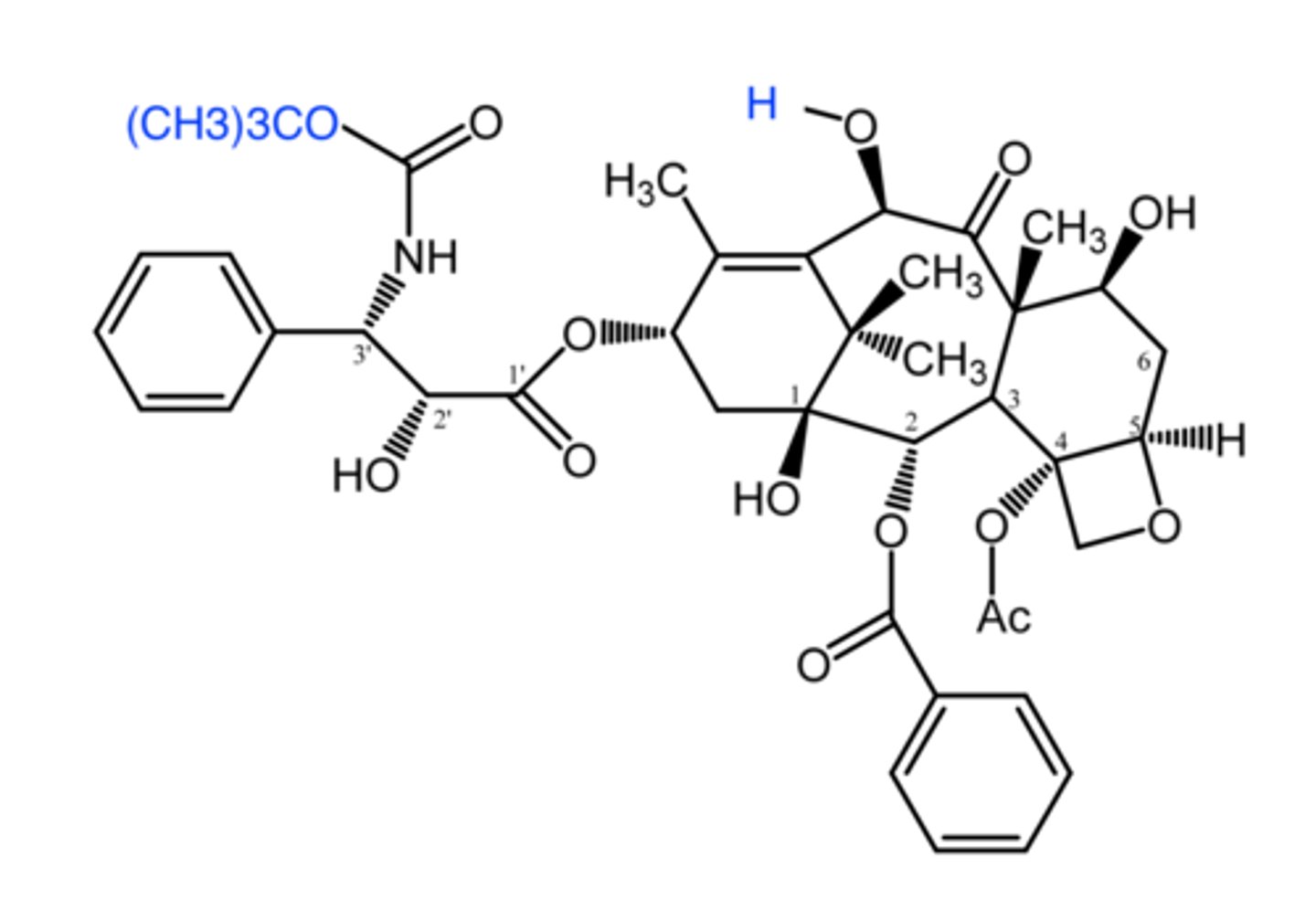
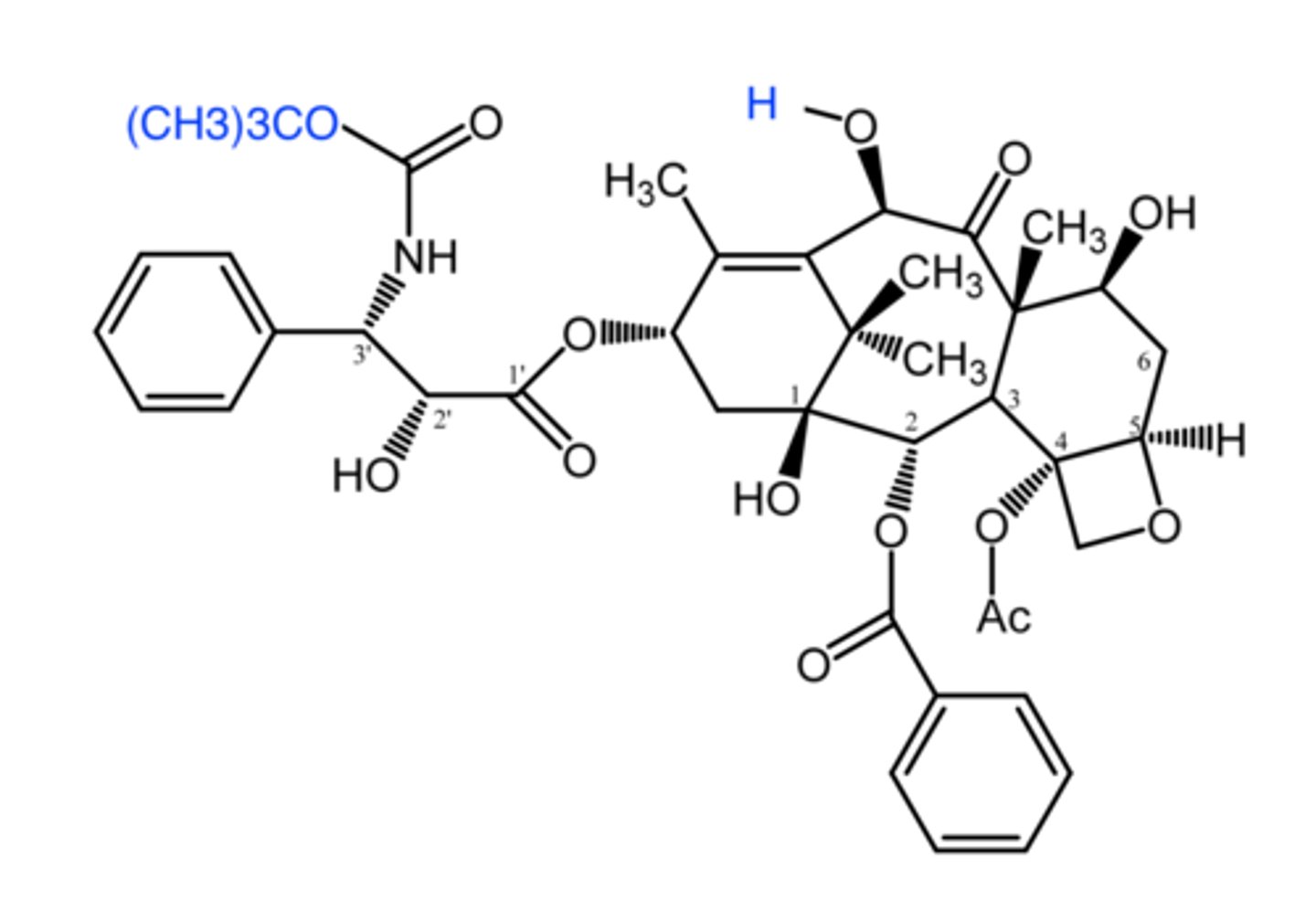
paclitaxel
paclitaxel
(taxane -- mitosis inhibitor)
natural product isolated from Pacific yew tree, Taxus brevifolia
ROA: IV
- poor solubility = use mixture of water + alcohol + cremophor EL
- albumin bound formulation (Abraxane) = no hypersensitivity, improved solubility (better tumor penetration)
MOA: binds polymerized b-tubulin promoting stable tubulin conformation which leads to resistant microtubules + promotes elongation phase + inhibits disassembly of tubule into mitotic spindle
- resistance: cellular efflux via Pgp
indication: 1st line for advanced ovarian + NSCLC in combo w cisplatin
- anthracycline resistant metastatic breast cancer
ADME: extensive distribution into tissues + long t1/2
DDIs: with drugs metabolized by CYP2C8
AE: myelosuppression, neutropenia, hypersensitivity rxn
- avoid hypersensitivity by pre-admin antihistamine + corticosteroid
- pregnancy risk category D
poor
taxanes have (poor/good) water solubility
hypersensitivity
in the paclitaxel formulation with water, alcohol, and cremophor, what negative side effect is associated with cremophor?
thymidine phosphorylase
what does paclitaxel upregulate that increases the efficacy of the combo treatment with capecitabine?
no hypersensitivity, better solubility
what are the 2 advantages of the albumin-bound formulation of paclitaxel?
D
what pregnancy risk category is paclitaxel and cabazitaxel?
2C8
paclitaxel has DDIs with drugs metabolized by which CYP enzyme?
docetaxel
docetaxel
(taxane -- mitosis inhibitor)
ROA: IV
- slightly better solubility due to C10-OH group
MOA: binds polymerized b-tubulin promoting stable tubulin conformation which leads to resistant microtubules + promotes elongation phase + inhibits disassembly of tubule into mitotic spindle
- resistance: efflux via Pgp
indication: NSCL, prostate, gastric, and head/neck cancer
ADME: extensive tissue bound, metabolized by CYP3A4
better
docetaxel has (better/worse) solubility than paclitaxel
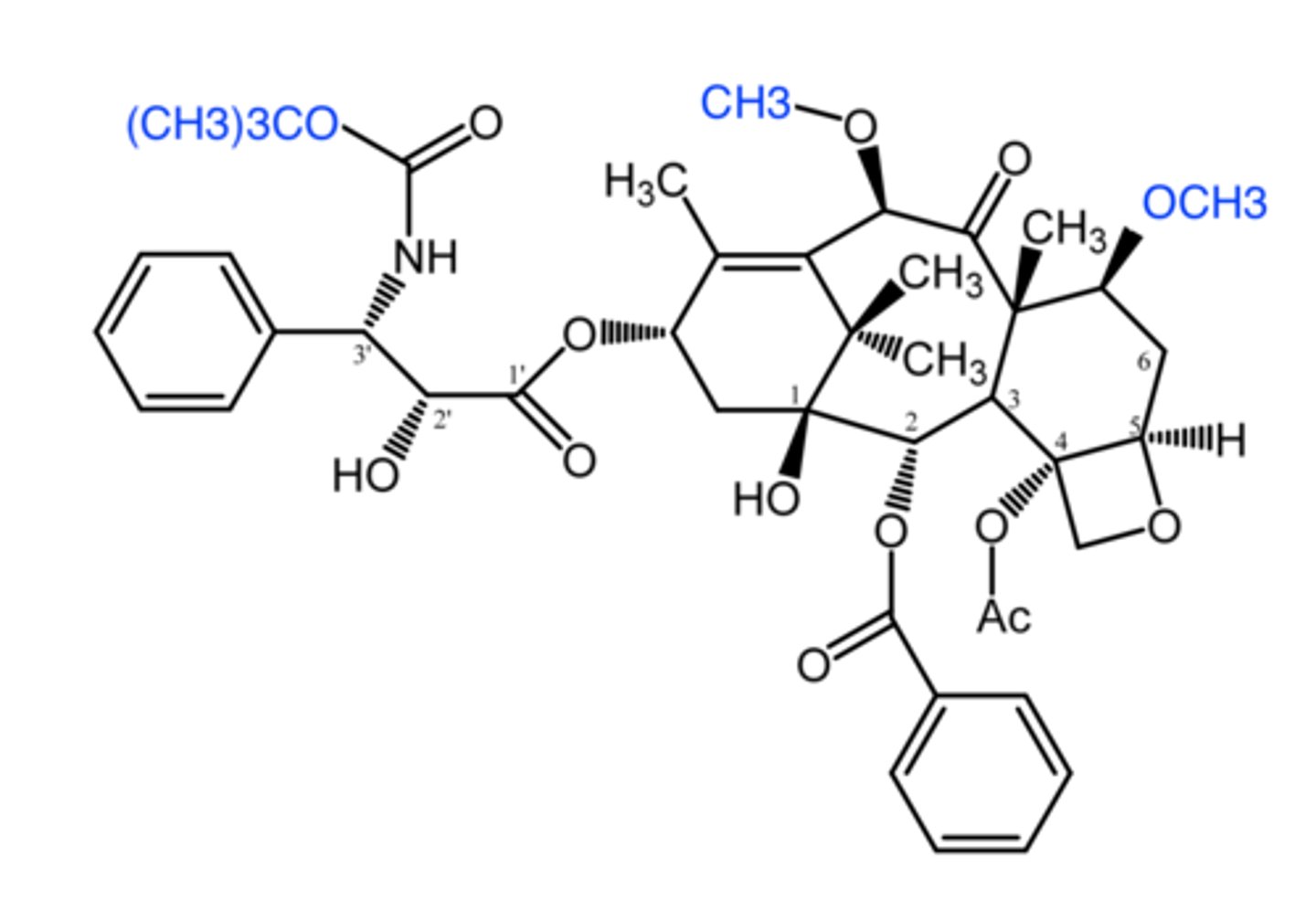
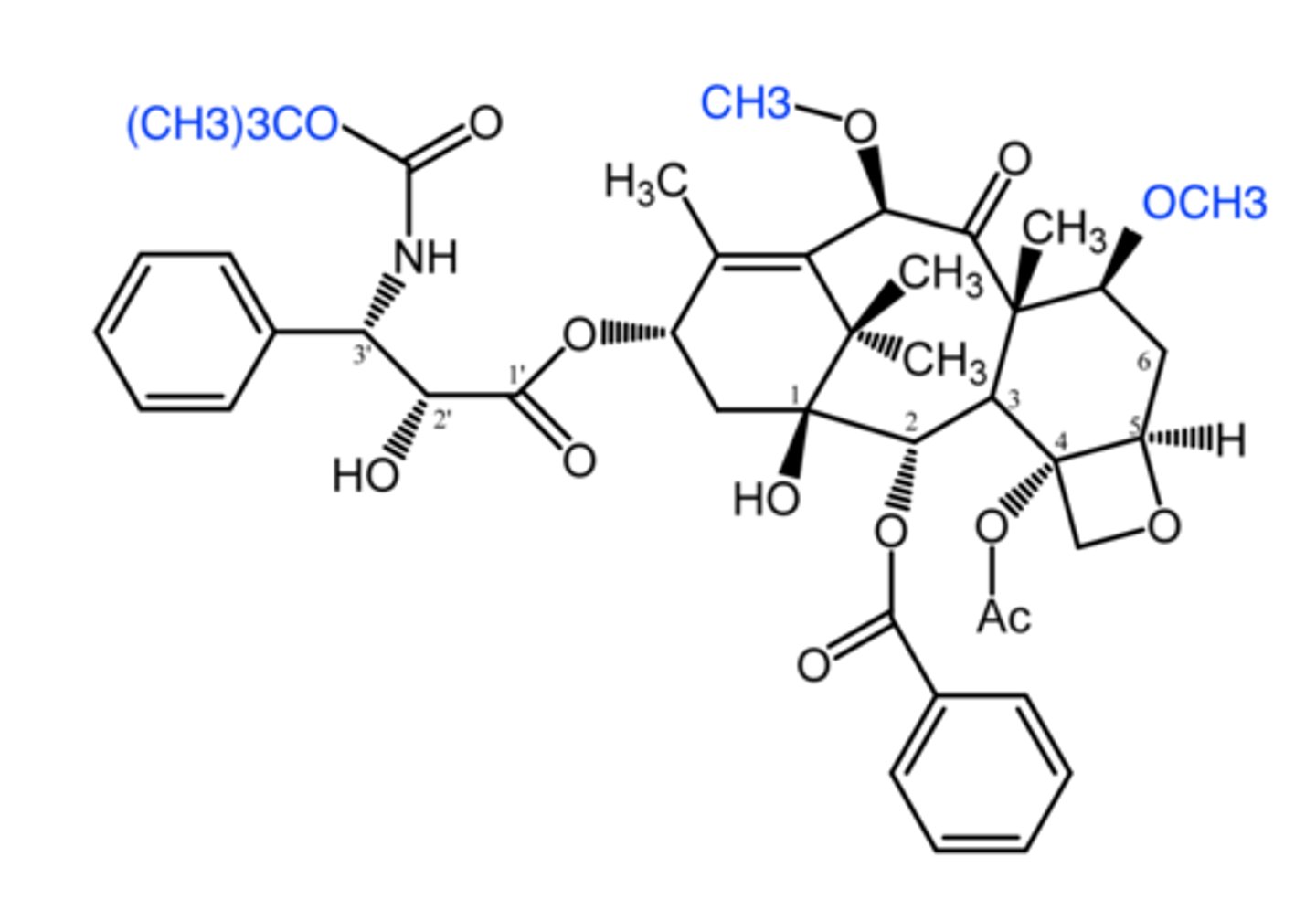
cabazitaxel
cabazitaxel
(taxane -- mitosis inhibitor)
ROA: IV
SAR: 7,10-dimethoxy analog of docetaxel = lower affinity for pgp = inc cellular retention + high BBB penetration
MOA: binds polymerized b-tubulin promoting stable tubulin conformation which leads to resistant microtubules + promotes elongation phase + inhibits disassembly of tubule into mitotic spindle
indication: docetaxel resistant metastatic prostate cancer
AE: myelosuppression, neutropenia, hypersensitivity
- pregnancy risk D
cabazitaxel
which taxane has high BBB penetration:
a. paclitaxel
b. docetaxel
c. cabazitaxel
ixabepilone
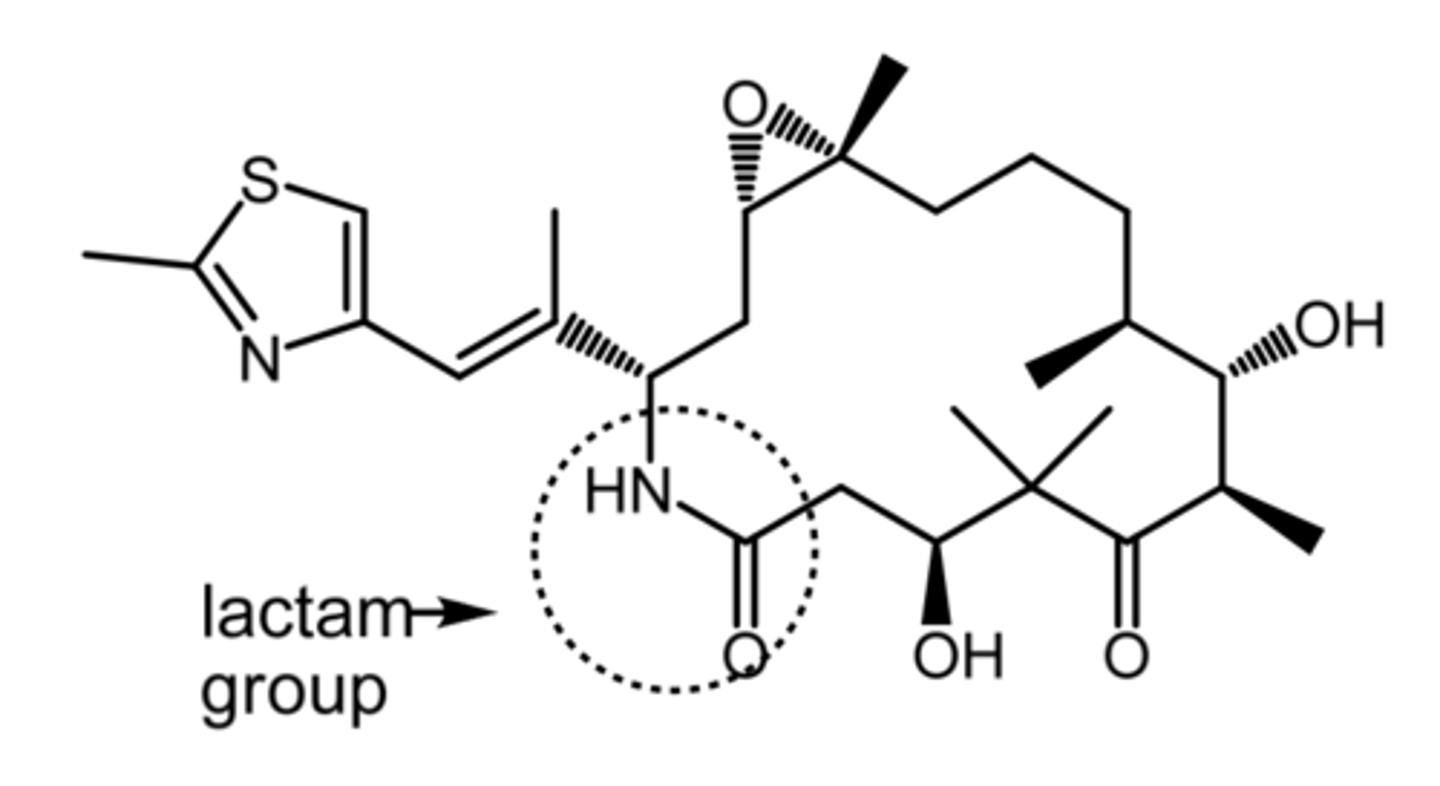
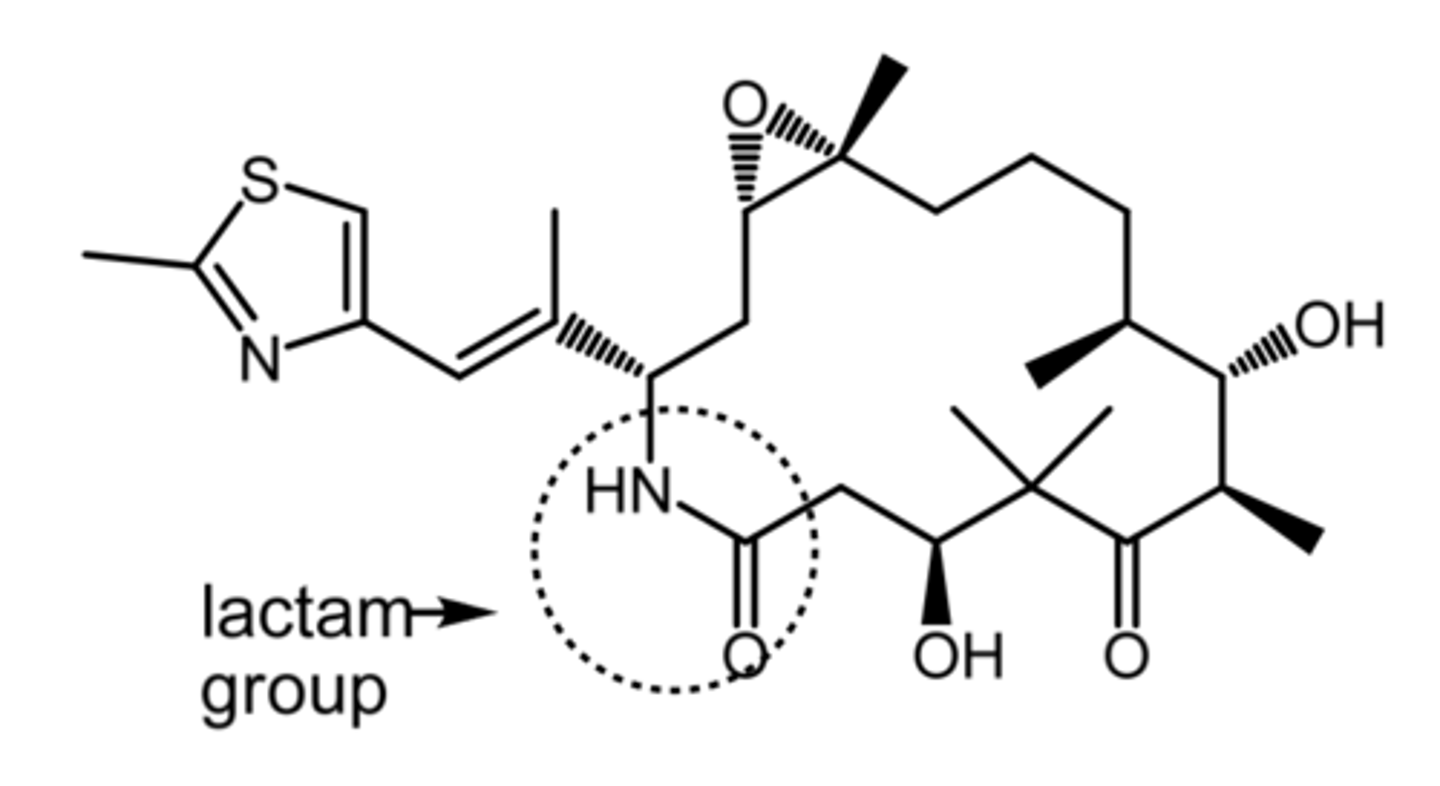
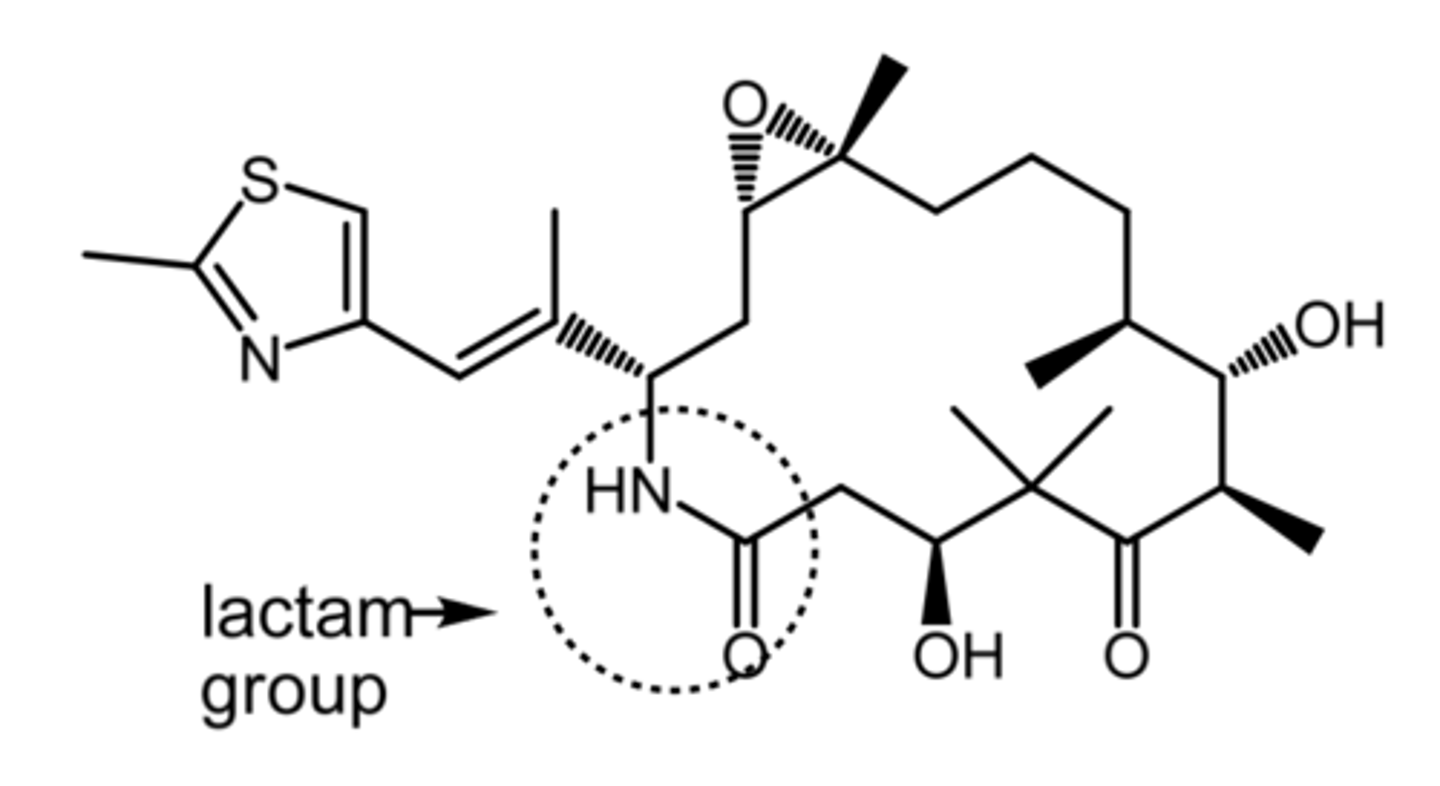
ixabepilone
(epothilone -- mitosis inhibitor)
SAR: semisynthetic epothilone B analog
- better water solubility + stability due to lactam group
- twice as potent as paclitaxel
MOA: promote cell death by inhibiting microtubule depolymerization
- low susceptibility to resistance
indication: in combo with capecitabine for anthracycline/taxane resistant advanced or metastatic breast cancer
AE: peripheral neuropathy, neutropenia
DDI: CYP3A4 substrates, inducers, and inhibitors
BBW: pts w impaired hepatic function (AST or ALT 2.5x higher than normal)
more
ixabepilone is (less/more) potent than paclitaxel
peripheral neuropathy, neutropenia
what are the 2 serious side effects associated with ixabepilone?
vincristine, vinblastine, vinorelbine
what are the 3 vinca alkaloids?
microtubule polymerization
vinca alkaloids stop cell division by inhibiting _______ _________.
IV
what is the ROA for all vinca alkaloids?
vincristine
which is cleared slower and has a longer t1/2:
a. vincristine
b. vinblastine
c. vinorelbine
vesicants
all vinca alkaloids are severe _____ that can induce necrosis, cellulitis, and/or thrombophlebitis
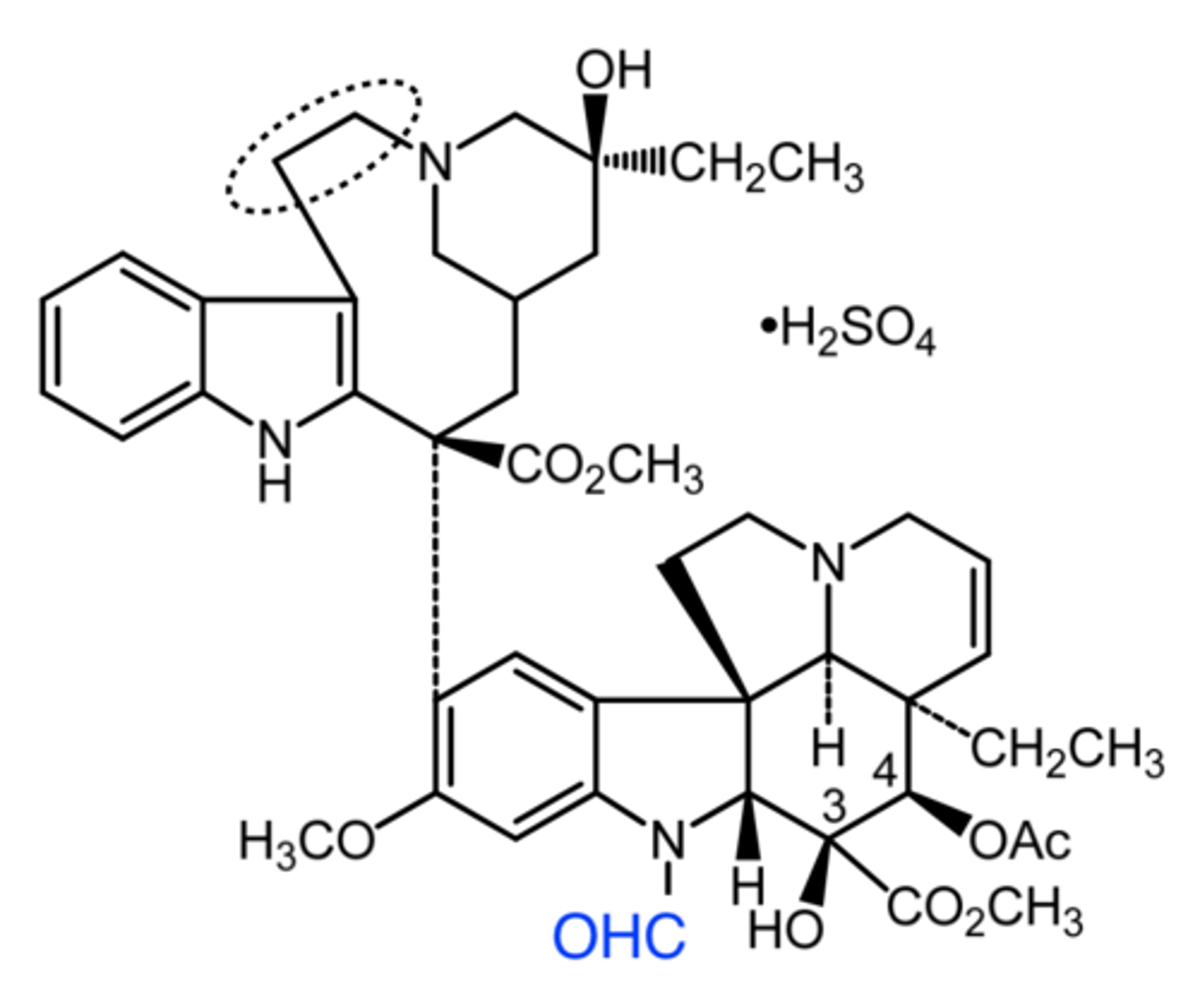
vincristine
vincristine
(vinca alkaloid -- mitosis inhibitor)
ROA: IV
MOA: inhibit microtubule polymerization
indication: advanced leukemia, Hodgkin's and non-Hodgkin's lymphoma, neuroblastoma
AE: severe vesicant
- inc toxicity risk in hepatic dysfunction
notes:
- longer t1/2 due to slower clearance
- over half of the children in US w cancer who receive chemo have been given this
vincristine
which drug have over half of the children in the US w cancer who receive chemo been given?
vinblastine
vinblastine
(vinca alkaloid -- mitosis inhibitor)
ROA: IV
MOA: inhibit microtubule polymerization
indication: Hodgkin's lymphoma, lymphocytic leukemia, testicular cancer, Kaposi sarcoma
AE: severe vesicant
- inc toxicity risk in hepatic dysfunction
vinorelbine
vinorelbine
(vinca alkaloid -- mitosis inhibitor)
ROA: IV
- has oral bioavailability, but only IV is available
MOA: inhibit microtubule polymerization
indication: NSCLC
AE: severe vesicant
- inc toxicity risk in hepatic dysfunction
- dose limiting granulocytopenia
intracellular domain
which part of the receptor tyrosine kinase (RTK) is able to phosphorylate selected substrates:
a. extracellular domain
b. transmembrane domain
c. intracellular domain
RTKs
EGFR/HER1, VEFGR, HER2, PDGFR are all examples of:
a. RTKs
b. NRTKs
NRTKs
Bcr-abl and Src are examples of:
a. RTKs
b. NRTKs
bcr-abl
which one is the philadelphia chromosome:
a. Bcr-Abl
b. Src
active, inactive
type 1 TK inhibitors bind the ____ conformation of the kinase
type 2 TK inhibitors binds the ____ conformation of the kinase
inhibit several kinases (AKA multikinase inhibitors)
what functional feature is common to promiscuous TK inhibitors?
bcr-abl, jak2, btk inhibitors
what are the 3 subclasses of NRTKIs?
imatinib, nilotinib, dasatinib
what are the 3 brc-abl inhibitors?
aberrant Ph chromosome
what is the viewed as the single cause of more than 90% of adult CML? (3)
imatinib
imatinib
(bcr-abl inhibitor --- NRTK)
ROA: oral
MOA: type 2 bcr-abl kinase inhibitor
- various resistance mechanisms
indication: 1Ph+ CML, Ph+ Acute Lymphoblastic Leukemia, GI stromal tumors, myelodysplastic/myeloproliferative diseases
ADME: high oral bioavailability and protein binding, t1/2 = 18 hr
AE: neutropenia, thrombocytopenia, anemia, rash
notes:
- greatest initial effect in the initial (chronic) phase of CML and significantly less effective later one
initial
imatinib has its greatest effect in the (initial/later) phase of CML
nilotinib
(bcr-abl inhibitor -- NTRKI)
ROA: oral, BID
MOA: type 2 bcr-abl kinase inhibitor
indication: Ph+ CML in chronic phase
ADME: low F (30%), t1/2 = 17 hr, mainly biliary elimination
AE: life threatening QT interval prolongation that can progress to torsades de pointes + sudden death
- inc risk w CYP3A4 inhibitors
- myelosuppression
nilotinib
which is associated with QTc prolongation + Torsades de pointes:
a. imatinib
b. nilotinib
c. dasatinib
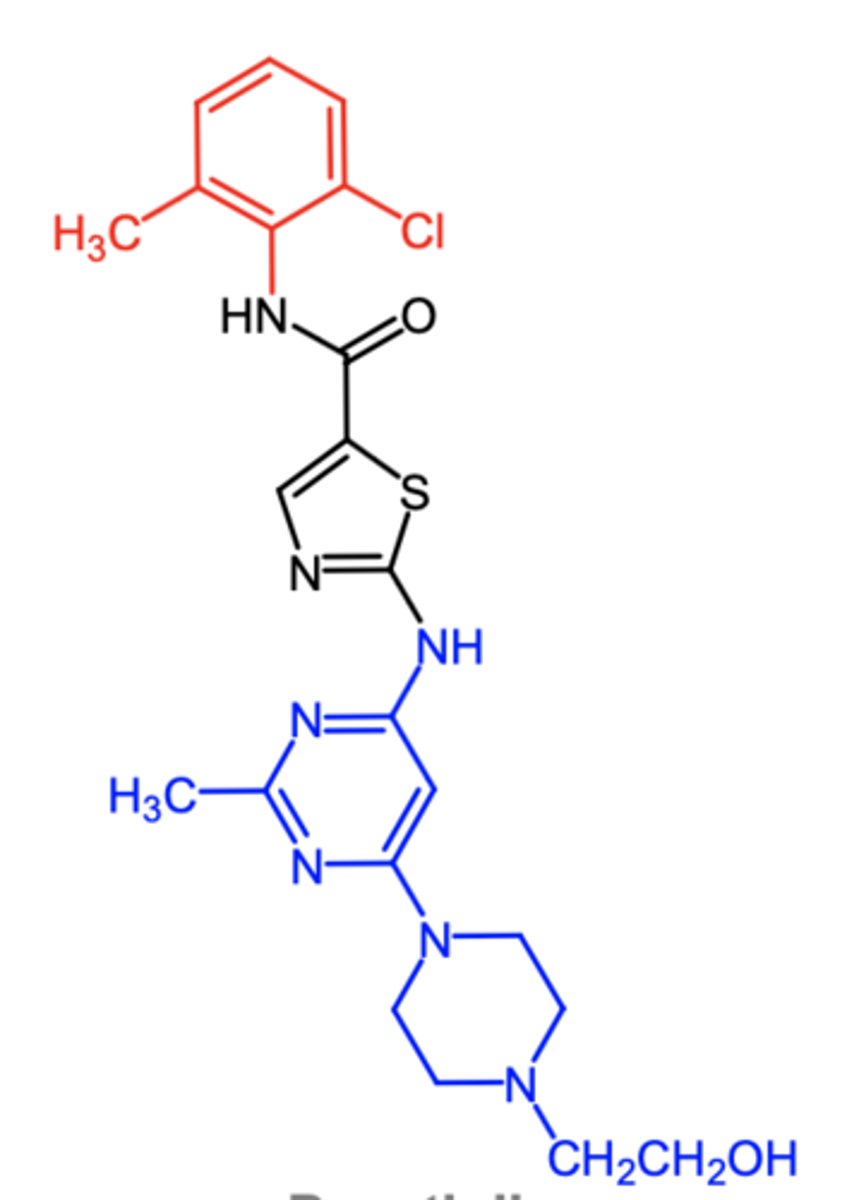
dasatinib
(bcr-abl inhibitor -- NRTKI)
ROA: oral
MOA: mixed type 1 and 2 bcr-abl kinase inhibitor that also has significant affinity for cellular Src kinases
indication: Ph+ CML, Ph+ ALL
ADME: low F due to poor absorption + fast first pass
- 3A4 mediated metabolism
- highly protein bound
oral
what is the ROA of brc-abl inhibitors?
dasatinib
which is associated with type 1 and 2 bcr-abl inhibition PLUS some Src kinase:
a. imatinib
b. nilotinib
c. dasatinib
cytokine, kinase, phosphate
Janus Kinase (JAK2) inhibitor:
family of intracellular, NRTK that transduce ________-mediated signals via the JAK-STAT pathway
they possess 2 phosphate-transferring domains: one exhibits ____ activity and the other removes _____.
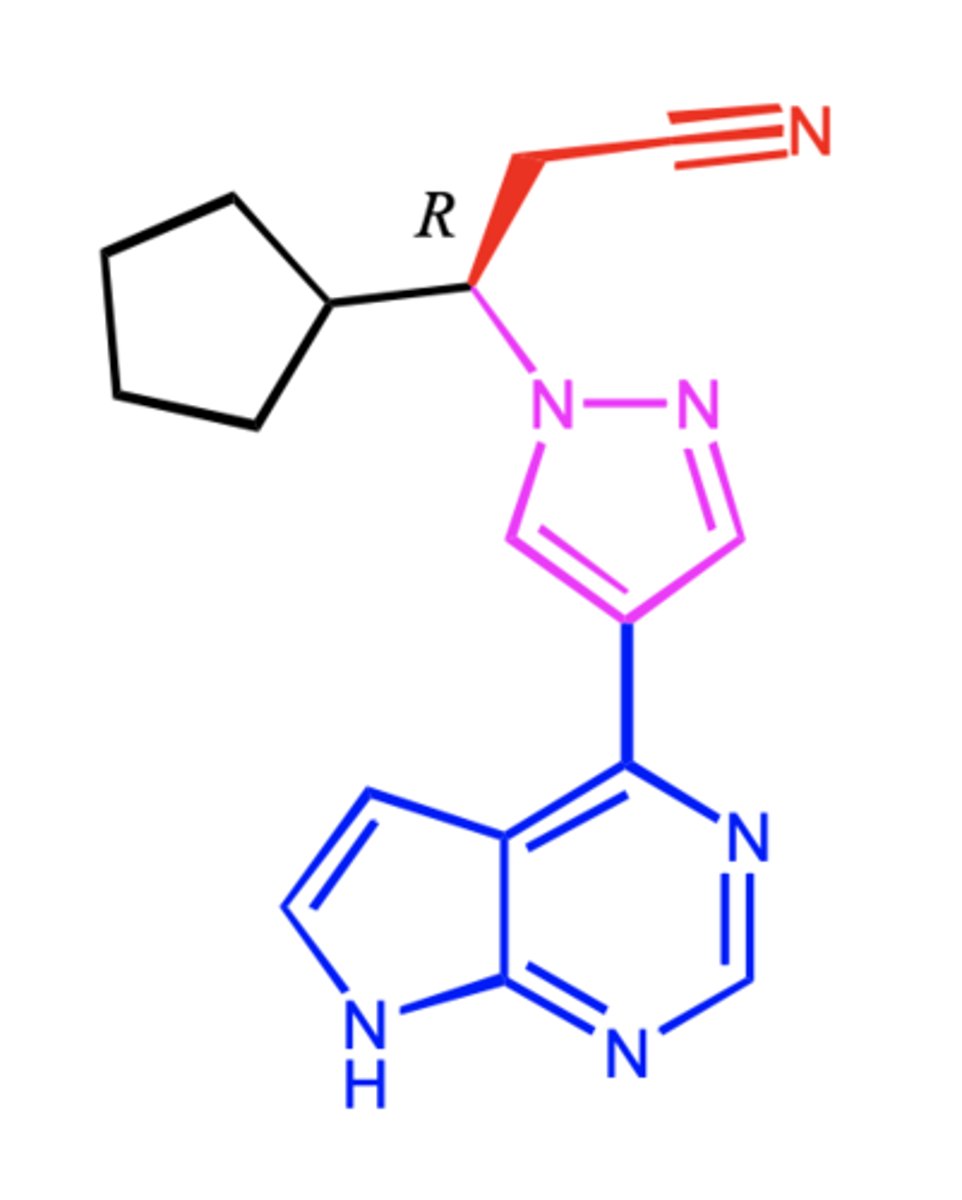
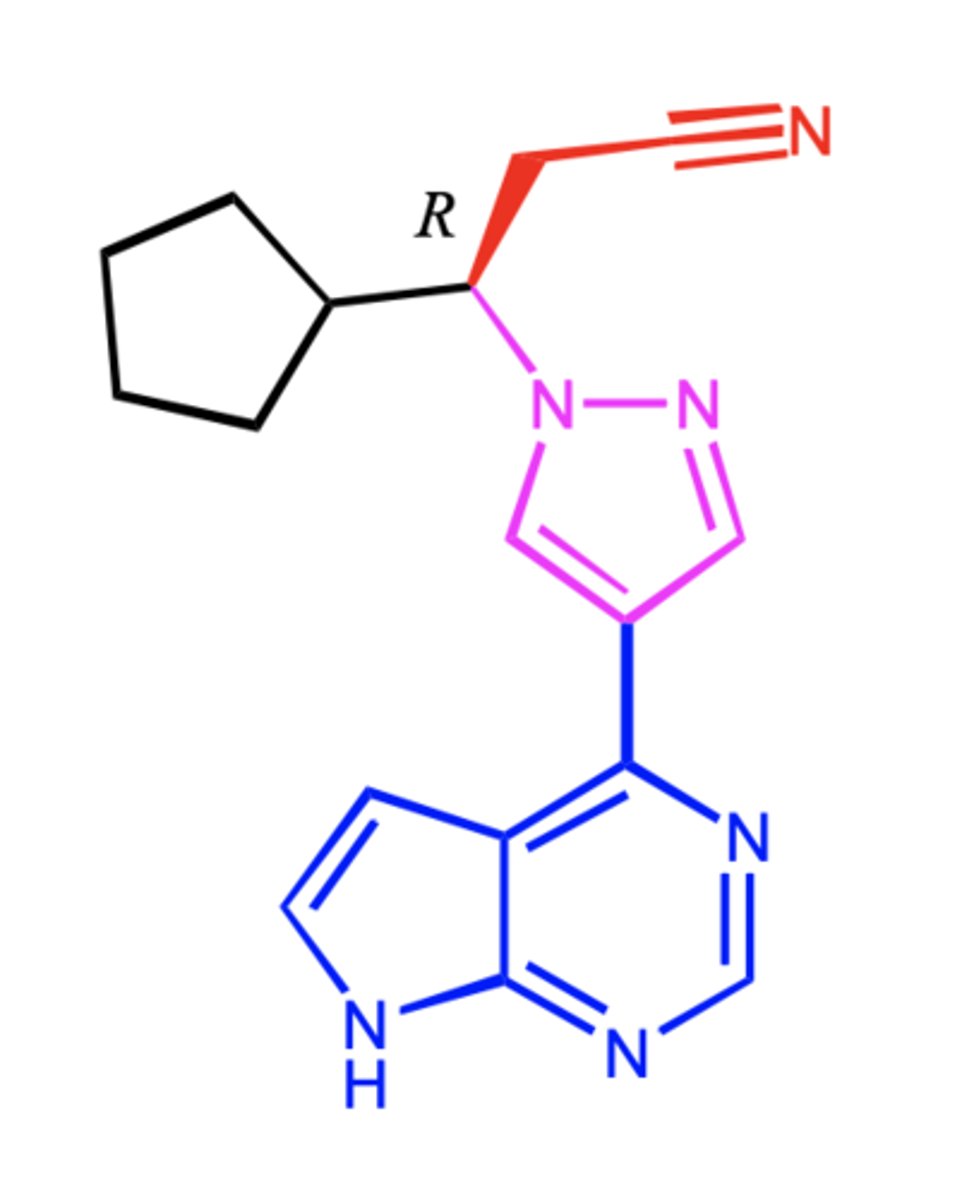
ruxolitinib (Jakafi)
ruxolitinib (Jakafi)
(jak2 inhibitor -- NRTKI)
ROA: oral
MOA: inhibits JAK1 and JAK2
indication: intermediate to high risk myelofibrosis
- polycythemia vera
AE: hematologic toxicity, infections, skin cancer
B cell maturation, lymphocytic leukemias
Bruton's Tyrosine Kinase (BTK) inhibitors
a cytoplasmic NRTK
plays an important role in __ ______ __________
BTK is constitutively phosphorylated by the oncogenic BCR-ABL1 fusion prodrug
BTK inhibition leads to dec malignant B cell proliferation and survival
defective expression of BTK is noted in ____
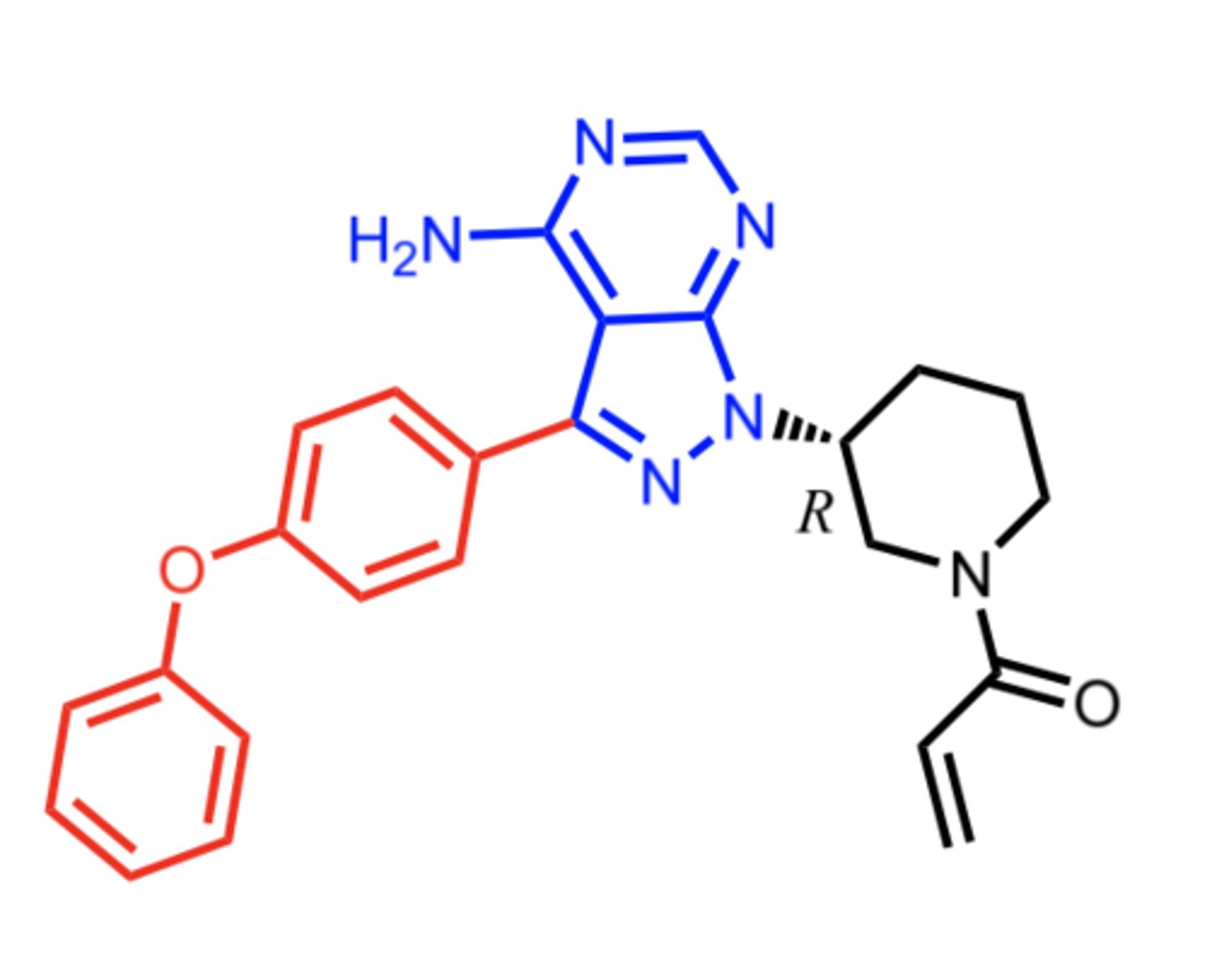
ibrutinib
(BTK inhibitor -- NRTKI)
ROA: oral
MOA: irreversible inhibitor of BTK
indication: CLL
AE: hematological effects (hemorrhage, neutropenia, thrombocytopenia, anemia), secondary malignancies (skin cancer)
hematological effects, skin cancer
what are the 2 most common side effects seen with JAK inhibitors (ruxolitinib) and BTK inhibitors (ibrutinib)?
EGFR, HER2
____ overexpression is correlated with dec life expectancy in solid tumors + found in almost all epithelial derived cancers
____ overexpression is a classic failure of treatment resistant breast, ovarian, lung, and gastric cancers
- called "antiapoptotic shield" = immortal
erlotinib, gefitinib
what are the 2 examples of EGFR/HER inhibitors (RTKIS)?
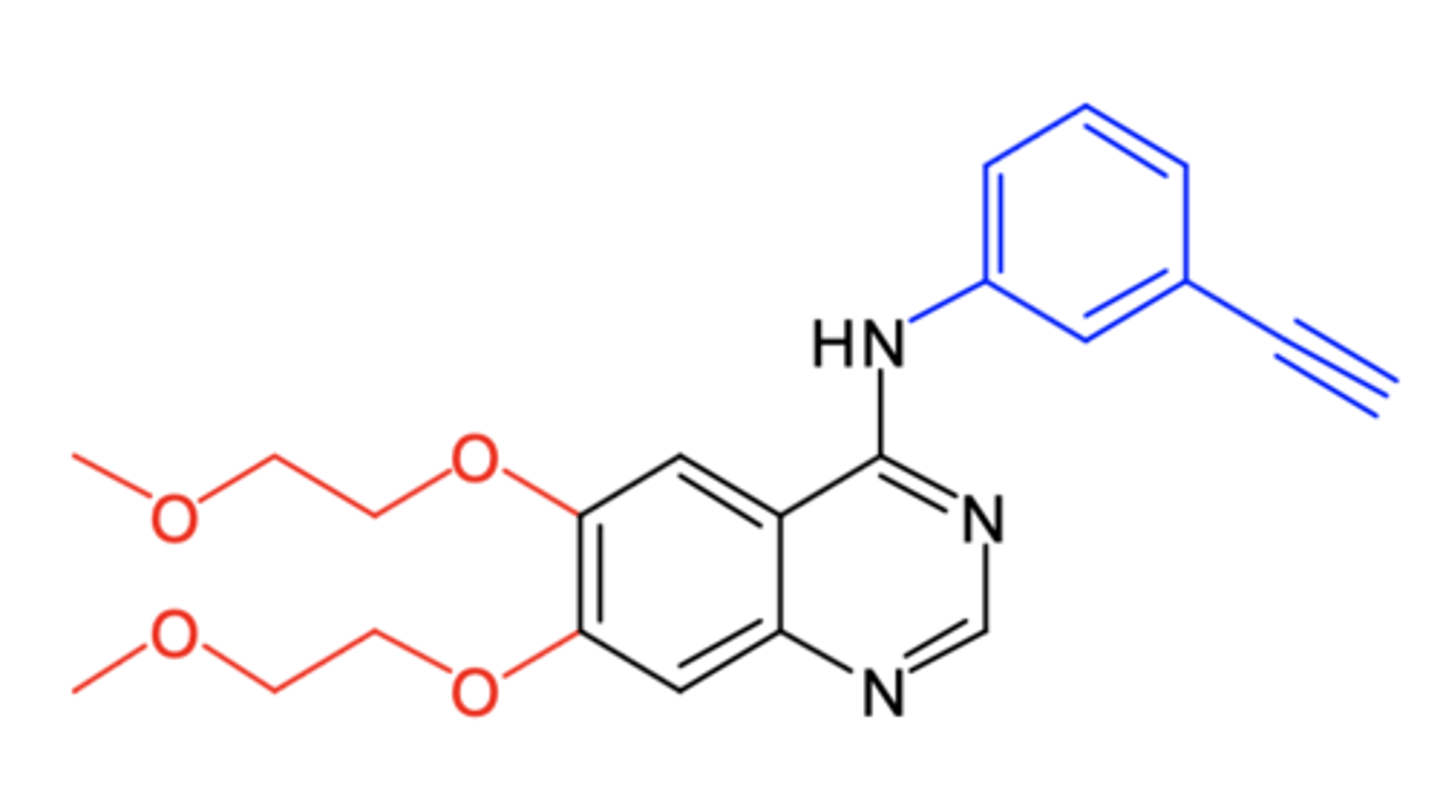
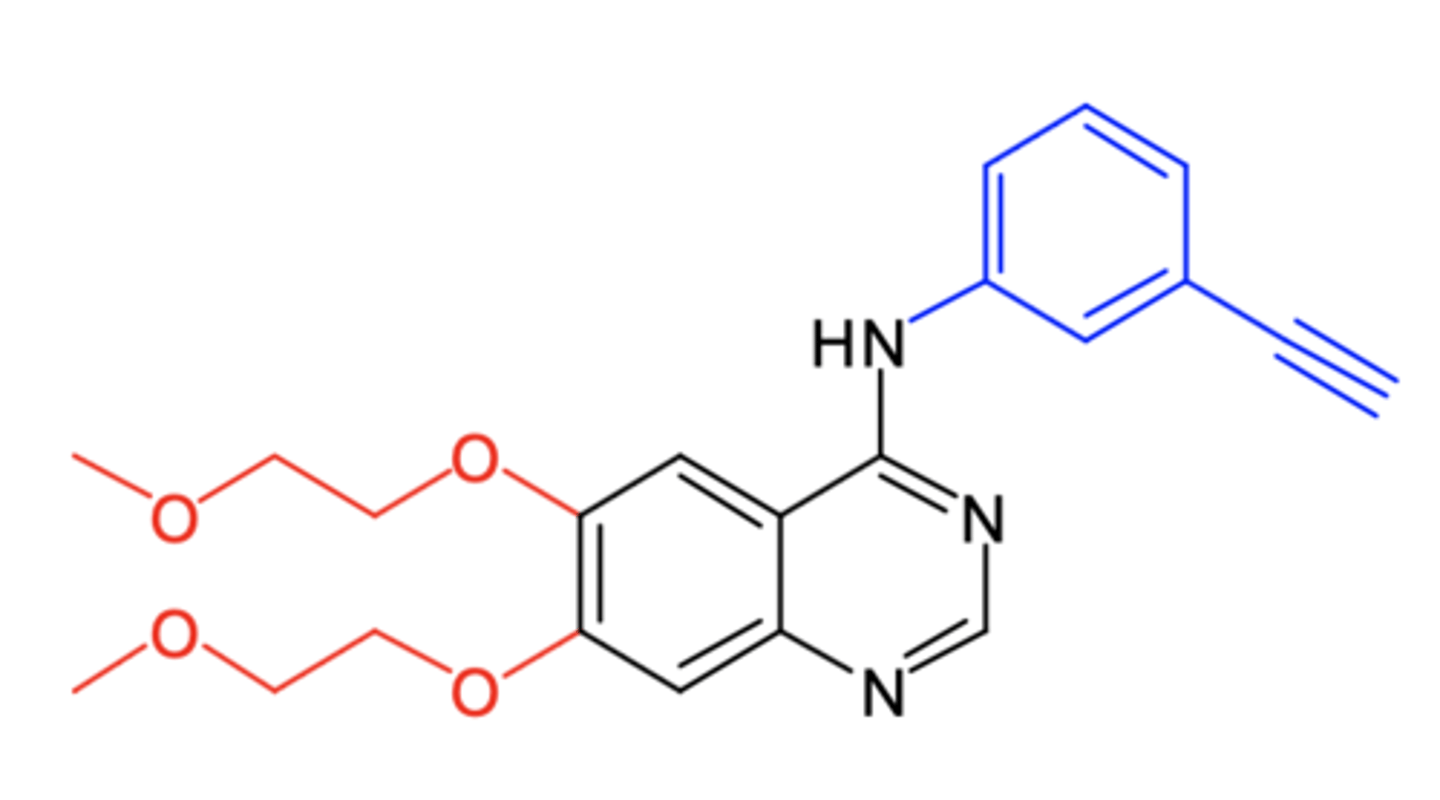
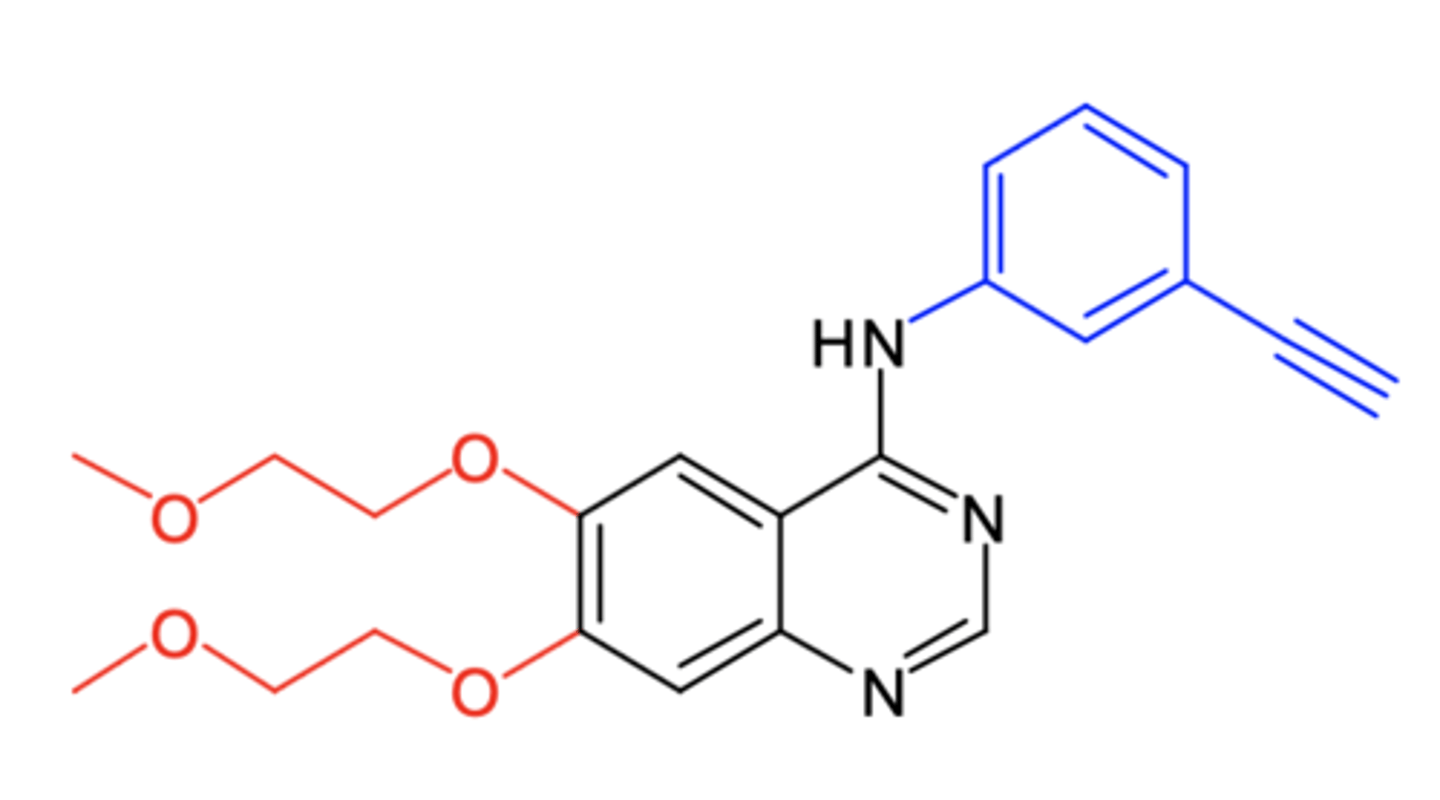
erlotinib
erlotinib
(EGFR inhibitor -- RTKI)
ROA: oral, QD
MOA: EGFR/HER1 inhibitor
indication: NSCLC, metastatic pancreatic cancer
ADME: biliary excretion, 60% absorption
AE: fatigue, rash, diarrhea, anorexia
- potentially fatal hepatotoxicity may be induced by this drug due to the formation of electrophilic quinoneimone
fatal hepatotoxicity
what is the consequence of erlotinib forming an electrophilic quinonemine?
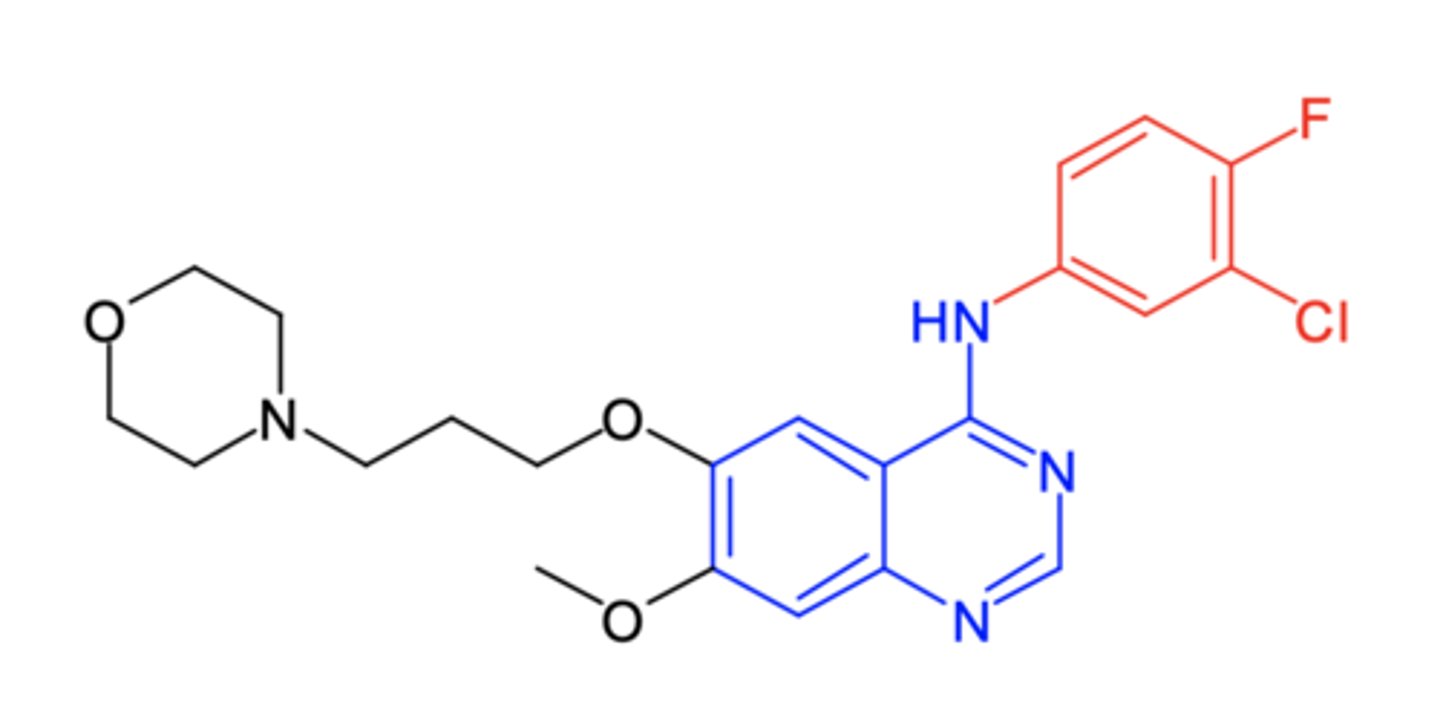
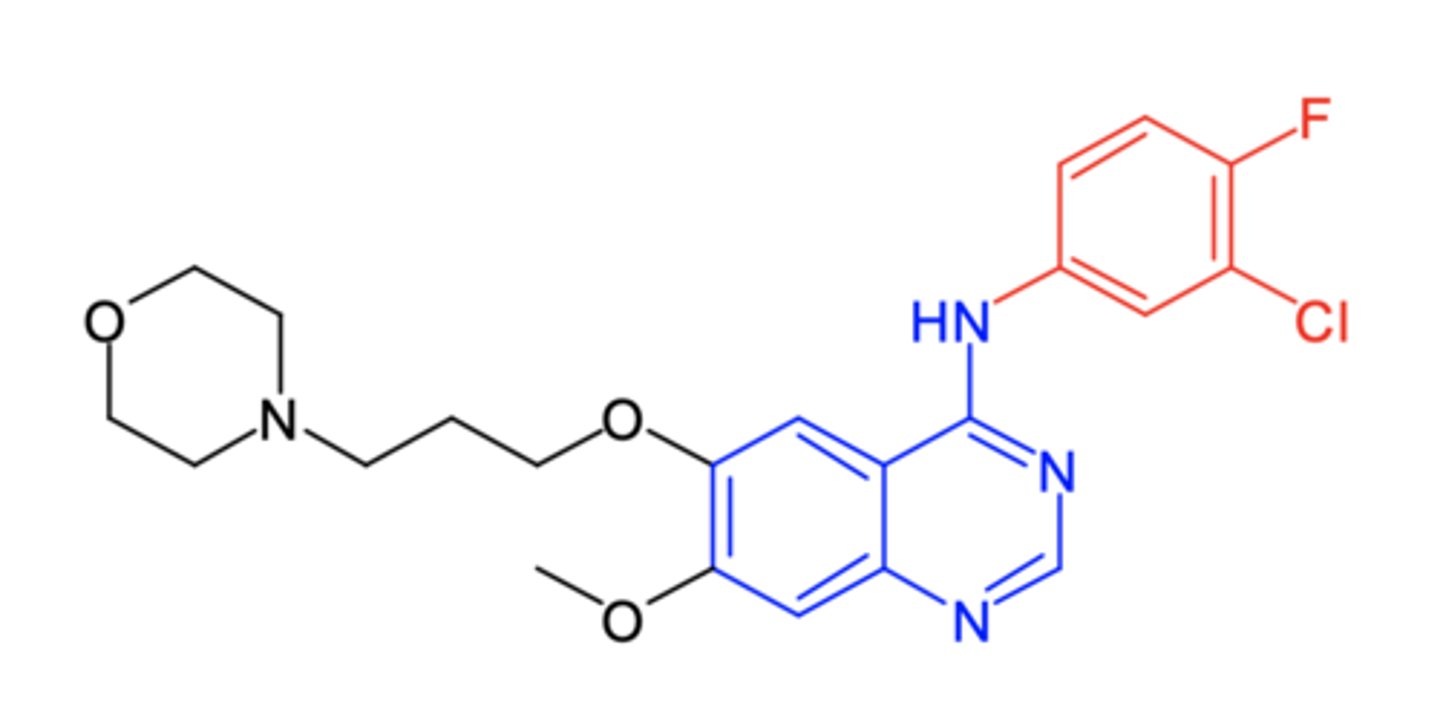
gefitinib
gefitinib
(EGFR inhibitor -- RTKI)
ROA: oral
MOA: EGFR inhibitor
- first one launched
indication: 1st line for metastatic NSCLC w EGFR mutations detected by FDA approved test
ADME: 59% F, 6-49hr t1/2, hepatic excretion, 90% ppb
AE: rash (due to EGFR kinase specificity), diarrhea
NSCLC
what are both EGFR inhibitors indicated to treat?
VEGFR2
which VEGF receptor is more important + is involved with the mediation of angiogenic effects:
a. VEGFR1
b. VEGFR2
blood vessels
inhibition of VEGFR-2 blocks the formation of new _____ _______ around tumors thereby blocks oxygen and essential nutrients from reaching the tumor
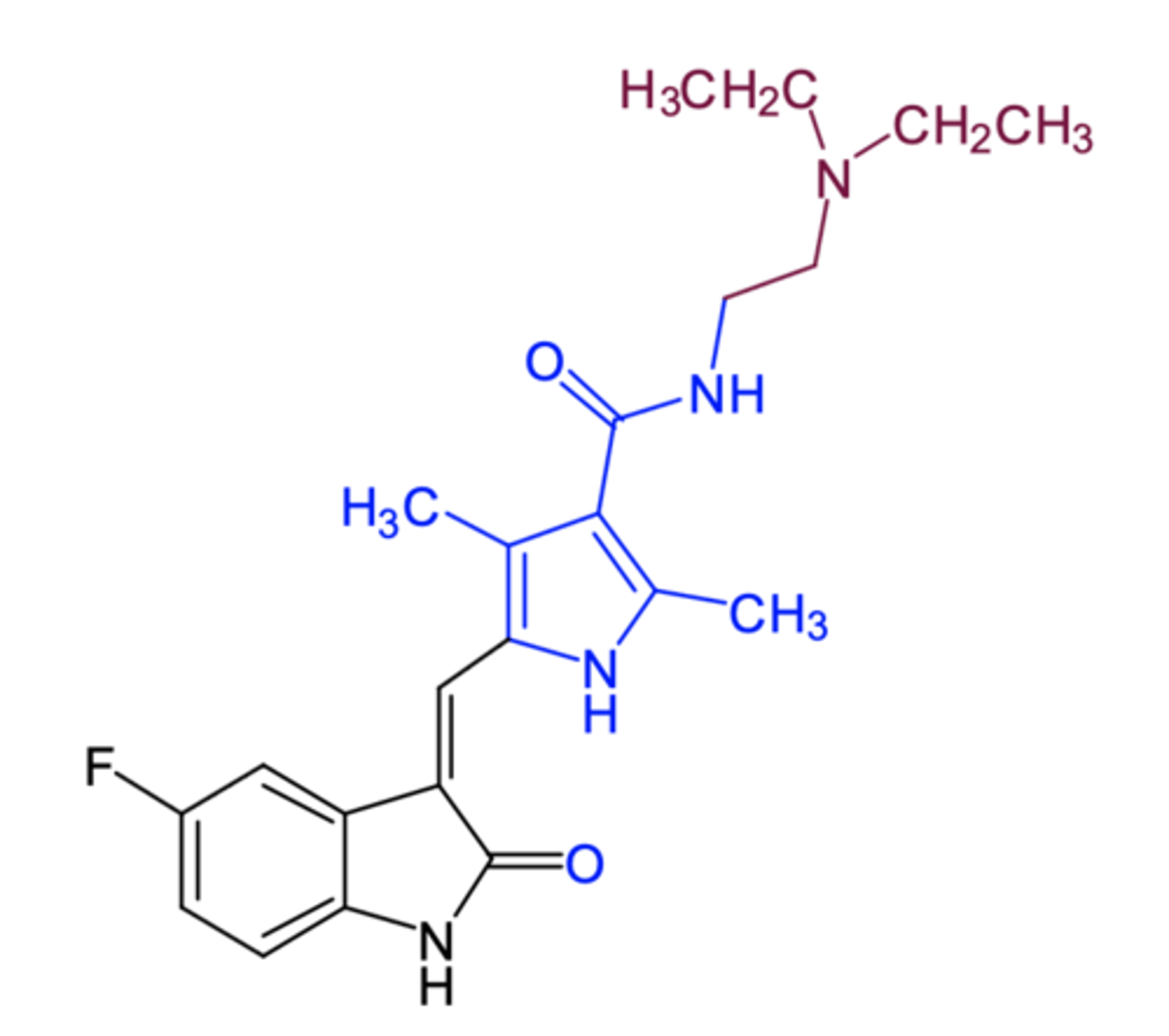
sunitinib
(VEGFR2 inhibitor -- RTKI)
ROA: oral, QD
MOA: inhibits multiple receptor kinases including VEGFR2 (both active + inactive forms)
- also inhibits PDGFRa/b, KTI, FLT3, CSF-1R, RET in vitro
indication:
- GI stromal tumor after disease progression or imatinib intolerance
- advanced renal cell carcinoma
- progressive pancreatic neuroendocrine tumors
ADME; Pgp substrate, t1/2 = 40-60 hr, biliary elimination
AE: many targets = more side effects
- hand-foot syndrome, stomatitis, and other dermatologic toxicities
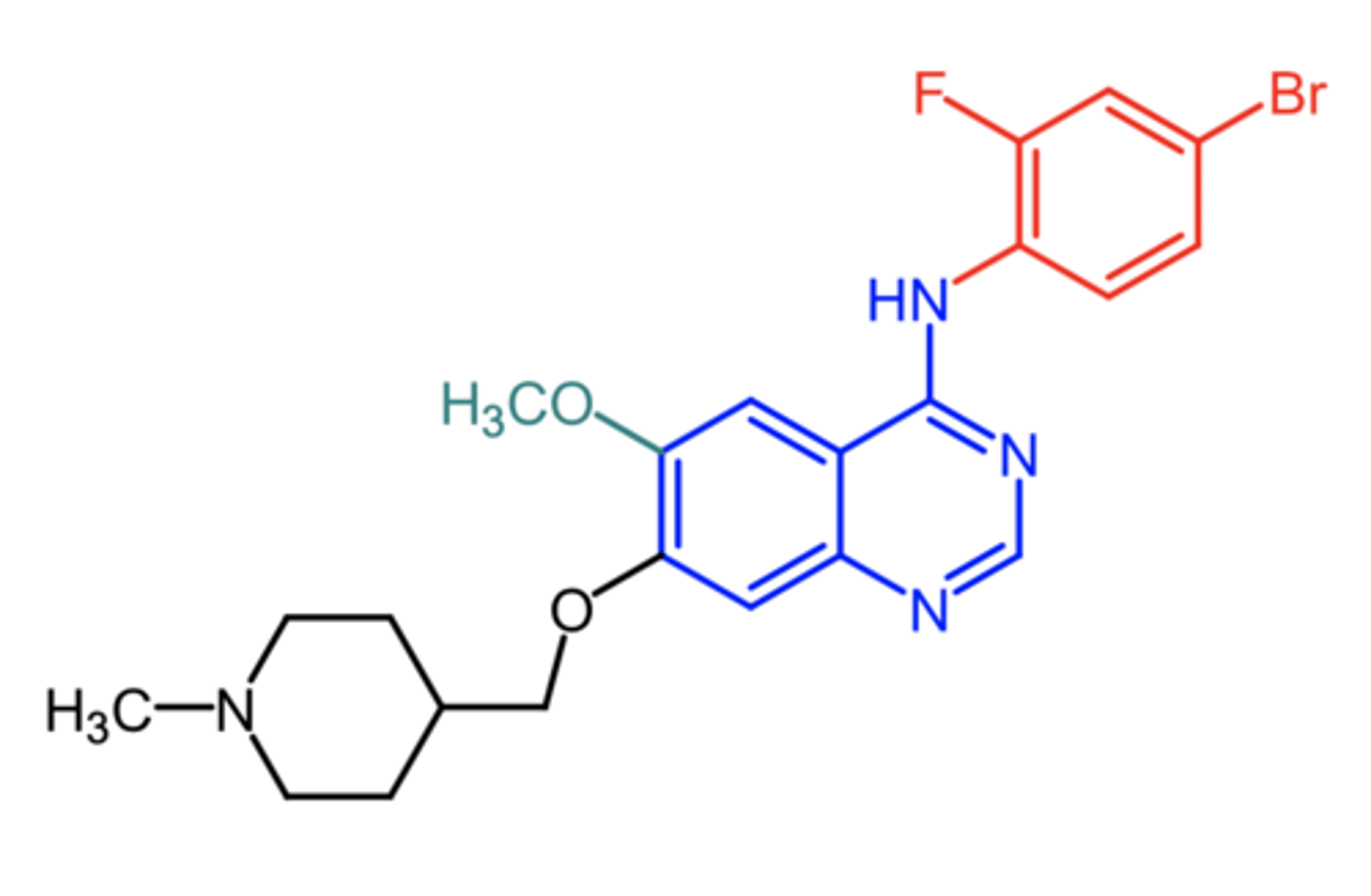
vandetanib
(VEGFR inhibitor -- RTKI)
ROA: oral, QD
MOA: inhibits VEGFR, EGFR, PTK6, and members of Src family of tyrosine kinases
indication: medullary thyroid cancer in patients with unresectable or metastatic disease
AE: diarrhea, rash, nausea, HTN, QTc prolongation, etc
rash
what is a common side effect with VEFGR inhibitors?
sunitinib, vandetanib, axitinib
what are the 3 VEFGR inhibitors?
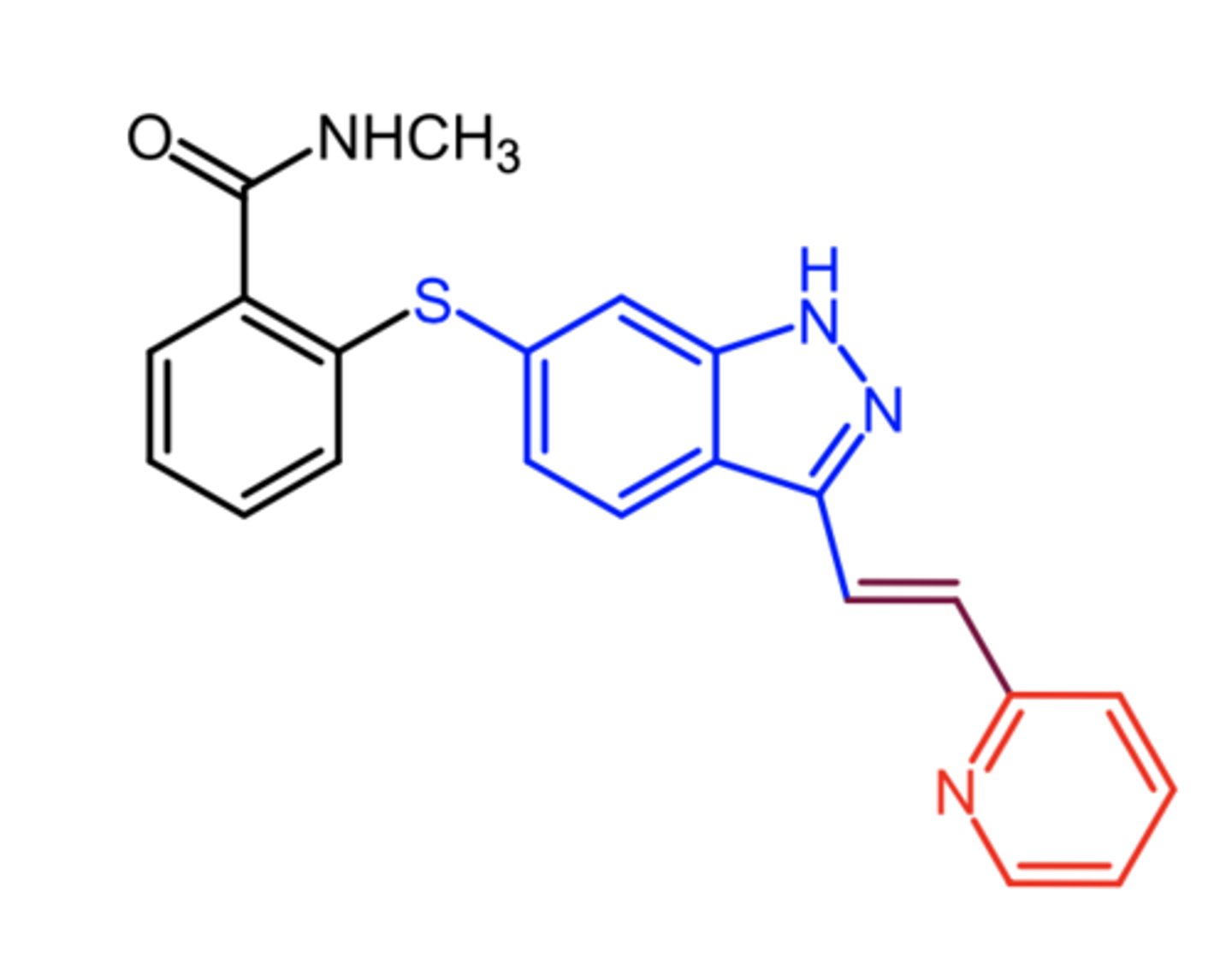
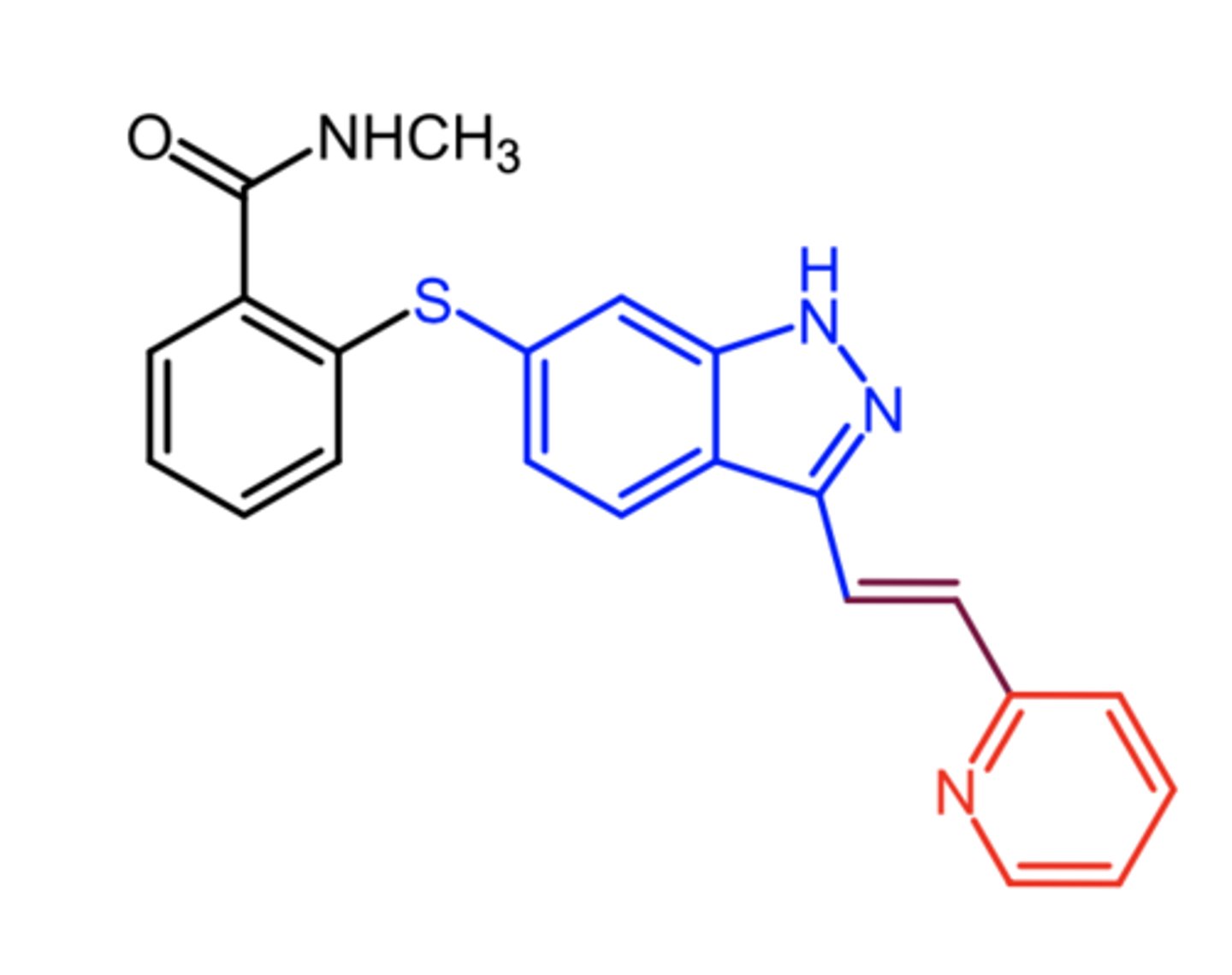
axitinib
axitinib
(VEFGR inhibitor -- RTKI)
ROA: oral, BID
MOA: inhibits VEGFR1/2/3
indication: advanced RCC after failure of one prior systemic therapy
ADME: good F, high ppb, very high Vd
- strong CYP3A4/5 inhibitor
AE: diarrhea, HTN, fatigue, dec appetite, nausea