oxygenation
the process of providing cells with oxygen through the respiratory system and is accomplished by pulmonary ventilation, respiration, and perfusion
gas exchange
process by which oxygen is transported to cells and carbon dioxide is transported from cells
factors affecting respiratory function
-body position -environment/weather -air pollution -pollens/allergens -heart failure -COPD -pregnancy -medications -anxiety/fear -airway obstruction
lifestyle: -smoking -alcohol -nutrition -drugs -obesity -exersize -occupational hazards
nursing respiratory function assessment
-respiratory rate -breathing pattern and effort -chest symmetry -auscultation of lung sounds -pulse oximetry -vital signs -skin color (cyanosis)
cyanosis
occurs when a person has unoxygenated hemoglobin in the arterial blood in body
central cyanosis
cyanosis of the lips, mucus membranes, and tongue; occurs when arterial blood's oxygen saturation falls below 85%
cyanosis on light skinned individuals
dark bluish tint to skin and mucus membranes reflecting the blue tint of unoxygenated hemoglobin
cyanosis of dark skinned individuals
gray or whitish skin tone; gray/white tint around the mouth and conjunctiva
cyanosis on yellowish toned individuals
grayish/green skin tone
respiratory nursing assessment
inspection: -skin color -use of accessory muscles -pt. positioning -respiratory rate -quality of respirations
auscultation: -listening for normal breath sounds -note any adventitious/abnormal breath sounds
patient teaching to support respiratory function
-smoking cessation -hydration -nutrition -reduce allergen exposure -exercise -flu, pneumonia, and covid vaccinations -weight loss -coughing and deep breathing exercised to move secretions
deep breathing
technique used for maximizing ventilation by taking in a large volume of air to improve gas exchange
pursed lip breathing
form of controlled ventilation to consciously prolong the expiration phase of breathing to improve gas exchange
diaphragmatic breathing
used to promote diaphragm use for breathing (instead of upper chest) and to increase volume of air exchange; decreases respiratory effort and relieves rapid ineffective breathing with hypertension
incentive spirometry
technique used to encourage deep breathing using a calibrated device to teach a goal-directed volume of inspired air -used every hour awake; 10 times an hour -insert the mouthpiece between lips, inhale slowly and deeply until the ball reaches predetermined goal
indications for incentive spirometry
-post-operative -chronic respiratory disease -pneumonia
oxygen saturation
pulse oximetry; a noninvasive measure of pulse saturation and direct oxygenation through blood gases
-normal: 95%-100% -low readings can be found with elderly, dark skinned pts, and COPD pts
COPD oxygen saturation
COPD pts are chronically hypoxic due to oxygen saturation being their drive to breathe, so a low O2 sat is maintained to maintain breathing
-healthy pt drive to breath is the build up of CO2
oxygen therapy
goal is to prevent or relieve hypoxia; oxygen is used as a drug where dose and concentration are continuously monitored
hypoxia
an inadequate amount of oxygen in the cells and tissues
early signs/symptoms of hypoxia
-tachypnea -tachycardia -restlessness, anxiety, confusion -pale skin -elevated blood pressure -use of accessory muscled, nasal flaring, adventitious lung sounds
late signs/symptoms of hypoxia
-stupor/dazed -cyanosis -bradypnea -bradycardia -hypotension -cardiac dysrhythmias
hypoxemia
insufficient oxygen in the arterial blood
dyspnea
difficulty breathing
nasal canula
simple comfortable device that delivers oxygen concentrations at: 24%-44% 2-6L/min
simple face mask
short term oxygen administration delivering oxygen concentrations at: 35%-60% 6-10L/min
venturi mask
delivers the most precise amount of oxygen @ 24%-55% 4-10L/min
-color coded valves
partial rebreather mask
works by allowing 2/3 of air to be exhaled to environment while 1/3 is exhaled to reservoir bag; delivers @ 70-90% 6-15L/min
nonrebreather mask
all air is exhaled into the environment and reservoir bag must be inflated at all times; delivers @ 60%-100% 6-15L/min
related oxygenation lab work
-sputum culture -peak flow -tuberculine testing -arterial blood gases
arterial blood gases (ABG)
blood from radial artery tested and used to measure the amounts of arterial gases (O2; CO2) in the arterial blood and blood pH
normal ABG testing results
-pH: 7.35-7.45 -PaO2: partial pressure of O2; 80-100 mm Hg -PaCO2: partial pressure of CO2; 35-45 mm Hg -SpO2: 95%-100% -FiO2: measures O2 delivery
abnormal ABG testing results
pH -less than 7.35 = acidosis -more than 7.45 = alkalosis
PaO2 -less than 80mm Hg = hypoxia
PaCO2: -either less than 35 or more than 45 = compromising respiratory issues -less than 35mm Hg = hyperventilation -more than 45mm Hg = hypoventilation; breathing depth and rate are insufficient
hand held device used to measure the highest flow during maximal expiration and indicated how rapidly and at what volume a patient can breath out -reading changes indicate changes in airway diameter -can prevent acute asthma attack -use the best (%) of 3 measured reading
chest physiotherapy
commonly prescribed to help clear excessive bronchial secretions from the airways -use cupped hand and clap on pt back in hollow sounding areas
elimination
the secretion and excretion of body wastes
urine specimen
collected urine samples used for laboratory tests to inspect urine
clean catch/midstream specimen
after perineum care, pt. catches urine sample mid-stream after urination begins -first voided amount is contaminated
sterile urine specimen
using asepsis, obtain a sterile specimen from a straight or indwelling catheter port
24 hour urine specimen
after discarding the first voiding of the day, collect urine output for 24 hours and refridgerate
urinalysis
diagnostic test used to analyze the physical, chemical, and microscopic components of a pt's urine and the presence of disease or substance use
urine culture and sensitivity
urine culture tested to detect and identify the bacteria/germ causing infection and which drug can be used to treat it
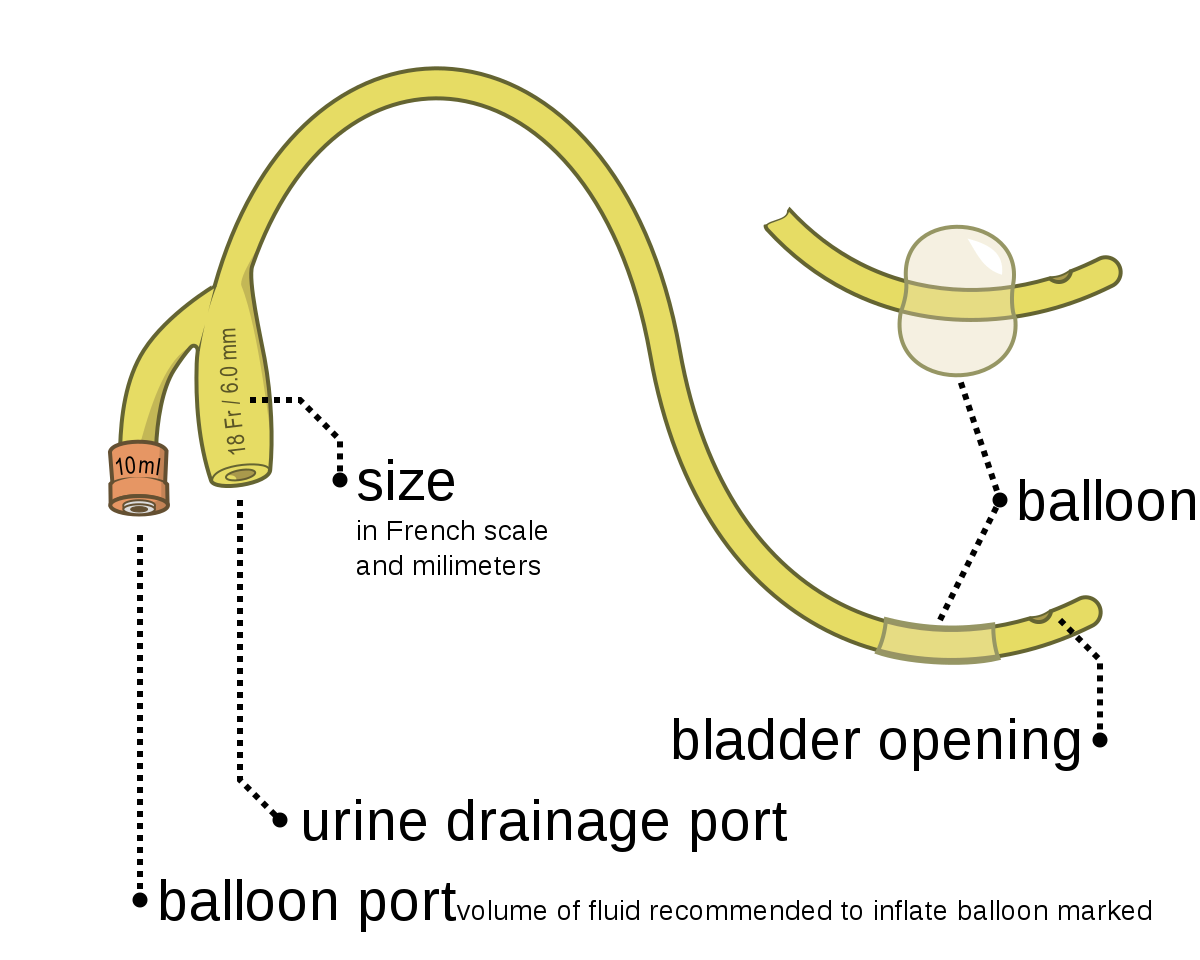
catheter
a flexible tube placed into the bladder (internal) or placed over the genitalia (external) to allow urine to drain
indwelling foley catheter
catheter placed into the urethra to the bladder for a specified amount of time to measure accurate output, unmanageable urinary retention, and incontinence
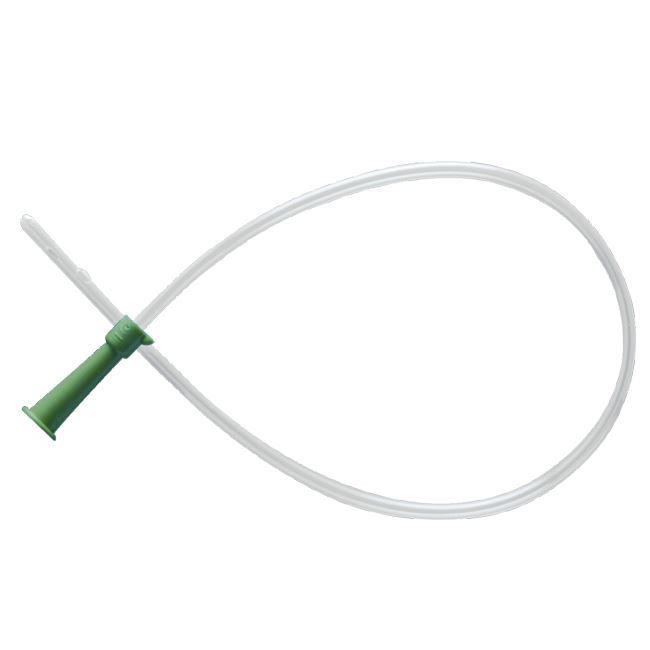
straight catheter
intermittent; used as needed to empty the bladder then removed and discarded when emptying is complete ur
urinary tract infection
infection of the urinary system caused by the introduction of bacteria to the tract
signs and symptoms of UTI
-urinalysis findings of RBCs, WBCs, bacteria, protein, and nitrites in urine sample -dysuria -increased frequency increased urgency cloudy urine -foul smelling urine -fever -confusion
nursing assessment of UTI
-typical voiding pattern -frequency -volume -color, odor, clarity -pain -distention
nursing education for UTIs
-female anatomy -hygiene -lifestyle (sexual intercourse)
CAUTI
catheter associated urinary tract infection
risk factors for CAUTI
-indwelling foley catheters -increased time of foley use -opening and placement of drainage system -changing and insertion of catheters
signs and symptoms of CAUTI
-increased frequency -increased urgency -nocturia -pain -hematuria -cloudy -foul smelling -fever -confusing -tachycardia -hypotension
prevention of CAUTI
-aseptic technique -prevent drainage system backflow perineum care
bladder retraining
retraining the bladder to increase the bladder's ability to hold urine and train a pt's ability to suppress urination incontinence
phenazopyridine
pyridium; used to treat manifestations/symptoms of UTI; doesn't treat infection but relieves bladder discomfort -changes urine orange
antibiotics
antimicrobial medications used to kill or inhibit bacterial growth
sulfamethoxazole and thrimethoprim
antibiotics used to treat UTI -take with water and avoid sun exposure
bowel retraining
training your bowels and body to return to or start a normal defecation pattern -used for pts who have the inability to control bowel movements, incomplete bowel emptying, or chronic constipation
bowel retraining assessment
-normal bowel function -nutrition and hydration -lifestyle -timing of bowel movements -consistency -use of enemas or laxitives (bulk builders)
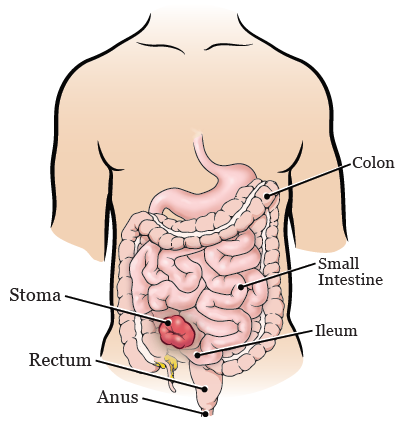
bowels
small and large intestines responsible for physical and chemical digestion and absorption
small intestines
absorb nutrients and water from food
large intestine
compacting and removing waste products of food
factor affecting bowel function
-anatomy/length of intestines (increased length = increased risk for constipation) -activity/exercise -body positioning (on toilet) -ignoring impulse to defecate (increased time tim bowel = increased dryness) -lifestyle -pregnancy -medications (opioids decrease bowel function) -surgery -fecal diversion
bowel diversion
surgical procedure done to allow stool to safely leave the body when the large intestine is removed or needs to heal
ostomy
temporary or permenant opening (stoma) surgically created in the abdomen wall to allow fecal matter to pass; in either the small or large intestine
stoma
an artificial opening made into an organ from the surface of the body
ileostomy
ends in the ileum (last part of the small intestine) and produces fully liquid stool
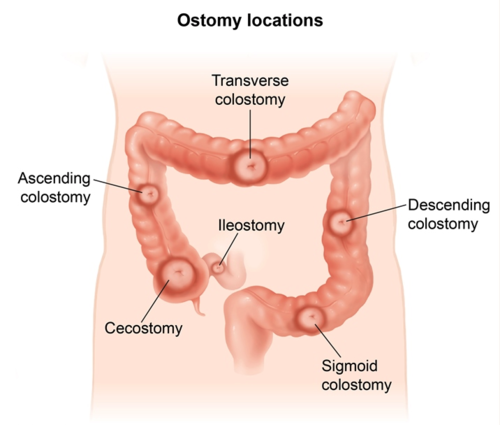
colostomy
ostomy ending in the colon/large intestine -ascending = liquid stool -transverse = soft stool -descending = solid stool -sigmoid = solid stool
stoma assessmenT
-stoma should be pink/red, moist and shiny -surrounding skin should be intact and healthys
stoma care
-assess stoma when changing bag (less than 1/2-1/3 full) -use mild soap and water to cleanse area -measure stoma using template -irrigate when necessary -pt. acceptance -odor control -skin care -body dysmorphia
constipation
infrequent, sometimes painful passage of hard, dry stool causes: -frequency of laxitaves -age -inadequate hydration -inadequate fiber intake -immobiloty -pregnancy -opioid use
can cause bradypnea or hypotension
hemorroids
blood vessels in the rectal wall that are engorged and dilated due to difficult defecation, pregnancy, or heart failure; can be itchy, painful, and bloody
fissures
tearing at the lining of the anus due to hard or large stools
syncope due to vasovagal response
straining while defecating decreases blood volume that returns to the heart and output; pressure receptors detect the increase of pressure and trigger the heart to slow down and blood pressure drops, causing fainting
assessment and prevention of constipation
-normal bowel function -encourage physical activity -encourage toilet use at same time daily -assess complications -increase fiber and fluid intake -monitor bloating -monitor cramping -avoid straining while defecating
risk factors for the elderly (bowel function)
-increased risk for dehydration -general muscle weakness -decrease peristalsis -relaxation of sphincters -ignored sense of defecation and dehydration -medications
nutrition for bowel function
-daily fiber intake of 25g-30g -daily fluid intake of 2,000mL-3,000mL
pain assessment
-subjective -use of standardized scales depending on pt.
expected findings: -behavioral changes -facial expression -changes in vitals signs (for acute pain)
acute pain
pain lasting less than 6 months and is sudden and unusual -fight or flight response -direct cause resolved with healing
chronic pain
pain lasting more than 6 months that is ongoing or recurs
nociceptive pain
pain arising from damage to or inflammation of tissue -Triggers pain receptors called nociceptors and causes throbbing, aching, and localized pain -Responds to opioids and non-opioid medications
somatic (nociceptive) pain
localized pain originating in bone, skin, and soft tissue
visceral (nociceptive) pain
pain in internal organs as a result of stretching, distention, or inflammation -ex. period pain
neuropathic pain
pain arising from diseased or damaged nervous system pr spinal nerves; feels like tingling, electric, pins and needles -responds to adjuvant medications
verbal indicators of pain
-moaning -complaining -crying -screaming
nonverbal indicators of pain
-facial expressions -body movements -elevated blood pressure, respiration rate, and pulse
numeric pain scale
pain ratings from 1-10 1-3 = mild pain 4-6 = moderate pain 7-10 = severe pain
wong baker faces scale
used for pts who don't speak english and infants/children; series of faces ranging from 0 = no hurt to 10 = hurts worst
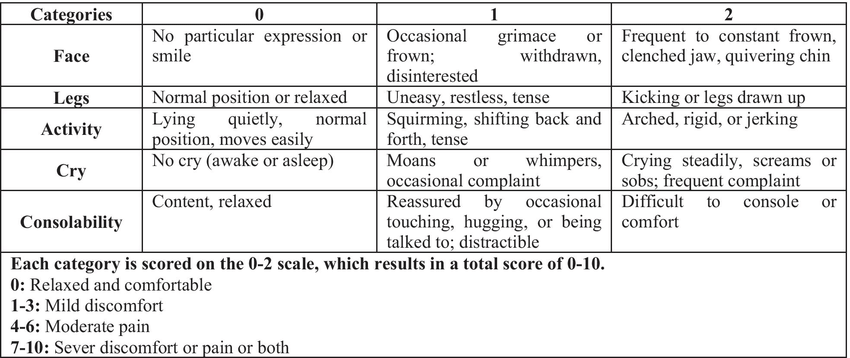
FLACC scale
scale used for nonverbal pts and infants; assesses face, legs, activity, cry, and consolability 0 = relaxed/comfortable 1-3 = mild discomfort 4-6 = moderate pain 7-10 = severe discomfort/pain
NIPS infant pain score
assessed 6 behavioral reactions to painful stimuli; 0-7
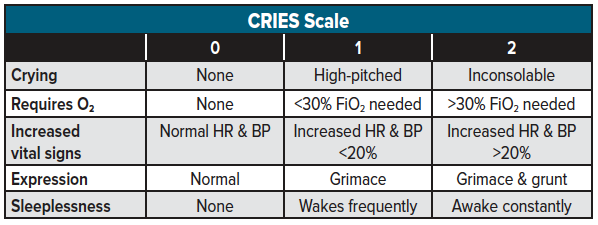
CRIES observer pain scale
assesses Crying, Requires oxygenation, Increased vitals, Expression, and Sleeplessness; 0-10
pharmacologic intervention
analgesic; pain relievers
nonopioids
treats mild to moderate pain (1-3) -acetimenophem -NSAID
opiods
appropriate for treating moderate tot severe pain (4-6) for post-op and cancer pain -morphine sulfate -dilauded -fentanyl (100x stronger than morphine) -codine
opioid adverse effects
-sedation -respiratory depression -orthostatic hypotention -urinary retention -nausea/vomiting -constipation -pruritus = itching
perioperative
begins with decision to have surgery until transfer to OR
intraperative
begins in OR intil transfer to PACU
post operative
lasts from PACU to follow up heath care provider visit
pre-operative nursing interventions
-establish theraputic relationship -listen to verbalized concerns -demonstrate empathy/caring -ensure tests are explained to pt. -collect appropriate specimen -report results -report any abnormalities
informed consent
signed consent given by the patient to the surgeon to perform the surgical proceedure -obtained by surgeon but a nurse but be physically present to witness signature of documents