ANA 873 Obesity Baker & Leighow PP
1/150
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
151 Terms
Obesity
•Complex & multifactorial, chronic disease
•Develops from interaction between an individual’s genotype & the environment
•2nd leading cause of preventable death in the U.S. (112K /year)
~75% of U.S. adults are overweight or obese
•Class 3 obesity (BMI >40) Men= 5.5% Women= 9.9%
•In U.S. obese individuals have 10-50% greater risk for death, greatest risk is cardiovascular causes.
obesity definitions- KNOW 1,2,3
•BMI= weight (kg)/height(m)² OR
BMI = (weight lbs /height [in inches]²) x 703
•Overweight: BMI= 25-29 kg/m²
•Obesity: BMI= >30 kg/m²
•Class I : 30-34.9 kg/m²
•Class II: 35-39.9 kg/m²
•Class III: >40 kg/m²
•Use extreme obesity not morbid obesity
What is IBW used for
•Useful for calculating drug dosages
•Certain drugs if given per weight can lead to toxicity, renal damage or hemodynamic instability
LBW is 30% higher than IBW.
How to calculate IBW for men
height (cm)-100
How to calculate IBW for women
height (cm) - 105
How much does lean body mass increase in obese person
•Lean body mass increases by 30% in the obese individual d/t increased muscle development to carry extra body weight
LBW is 30% more than IBW
How to calculate LBW
IBW x 1.3
adipose tissue fxn
•Has major integrative physiological functions
•Secretes numerous protein hormones: leptin, adiponectin & resistin. (influence energy metabolism)
•Is considered an endocrine organ
•Synthesizes & secretes fatty acid substances called prostanoids (prostaglandin) which inhibits the breakdown of fat.
•Adipose cells secrete cholesterol and retinol (Vitamin A)
•Provides a reservoir of readily convertible & usable energy
•Maintains heat insulation
Liver fat metabolism & adipose tissue
•Degradation of fatty acids into usable units of energy
•Synthesis of triglycerides from carbohydrates & proteins
•Synthesis of other lipids from fatty acids (i.e.) cholesterol & phospholipids
•All cells contain some unsaturated fats synthesized by the liver
•Important in heat regulation & insulation
•Fat cells, which are modified fibroblasts enlarge & will fill with liquid triglycerides 95% capacity
•Liquid fat can be hydrolyzed &transported from the cells to be used for energy
body fat distribution
•Fat cell formation occurs rapidly in early childhood
•Overfeeding during this time accelerates fat storage & triggers hyperproliferation of fat cells
•During adolescence, the number of fat cells stabilizes and remains constant throughout adult life
•Children become obese through increase in fat cell numbers, whereas adults become obese through hypertrophy of existing fat cells. They shrink but do not decrease in number.
•Where the fat is distributed is a better indication of increased health risk.
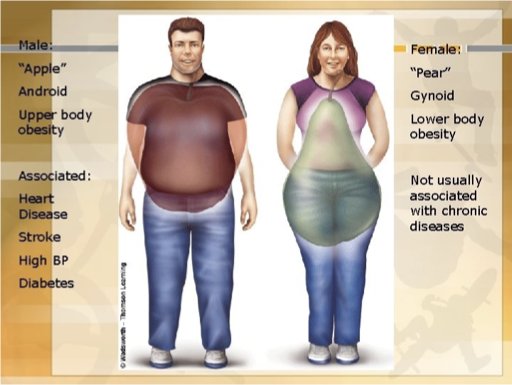
High risk of comorbidites in obese patients
Central, android or abdominal visceral (apple shape)
waist: hip ratio >0.85 in men & >0.92in women
is correlated with a higher risk of comorbidities in obese patients.
What is associated with increased risk for ischemic heart disease, diabetes, hypertension, dyslipidemia & death
•Waist circumference > 102 cms (40 inches) in men & >88 cm (35inches) in females
What correlates with varicose vein development & joint disease
•Peripheral gynecoid, or gluteal femoral obesity (pear shape)
waist: hip ratio < 0.76
correlates with varicose veins & joint disease and a reduced incidence of non-insulin-dependent DM
Medical risk are decreased in what individuals?
individuals with gynecoid fat distribution compared to those with android fat distribution
What is the difference in morbidity between android & gynecoid fat patterns
RT metabolic characteristics of the adipose tissue & the adjacent tissues.
Gynecoid fat- KNOW 7
Peripheral/ Glut-Fem/ pear-shaped
lower body obesity
primarily found in women
less metabolically active (inactive)
fxn= energy store for pregnancy/ lactation
Waist hip ratio <0.76
less medical risk but A/W varicose veins and joint dx
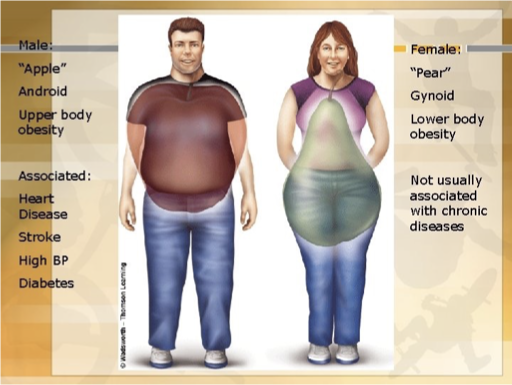
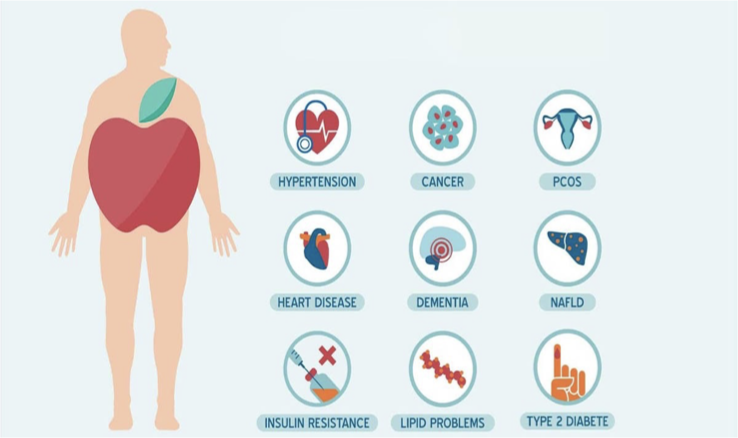
Android Fat- KNOW 8
Central/abdominal/ apple shaped
Upper body obesity
Increased visceral & retroperitoneal fat which compresses renal veins, lymph vessels, ureters and renal tissues
Increased pressure is linked to HTN
primarily found in men
waist hip >0.85 men; 0.92 women
metabolically active in free fatty acid release
↑ risk of CV dz, metabolic syndrome, HTN, DM, CVA
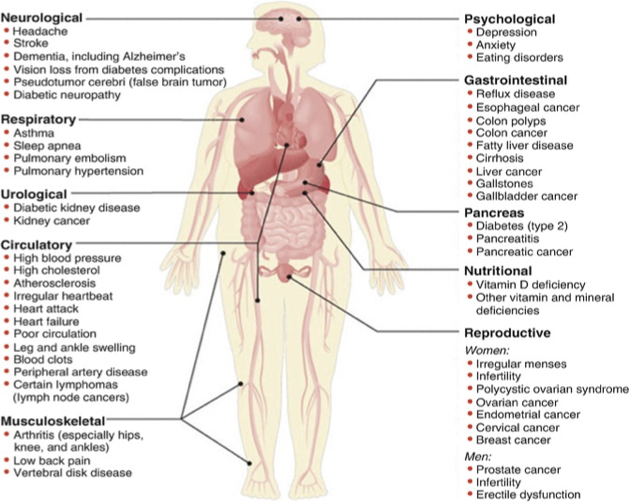
diseases related to obesity 8
HTN (most common)
CAD
HLD
DM
Coagulopathy
Cholelithais
DJD
OSA
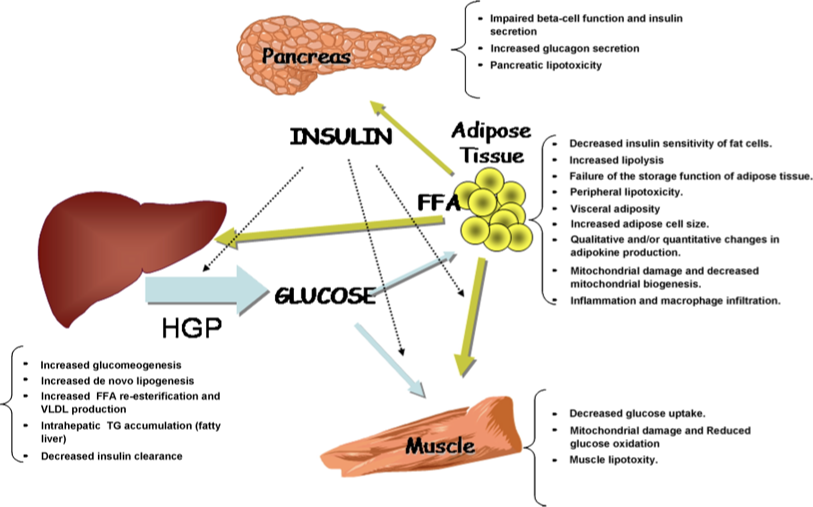
Liver & adipose tissue
•When increased free fatty acids (FFA) are released from adipose tissue, portal venous drainage delivers high concentrations of FFA to the liver
•This stimulates the liver to make VLDL & LDL
•Liver exposure to high levels of FFA increases gluconeogenesis & inhibits insulin uptake, which l/t non-insulin dependent diabetes
What is A/W cardiovascular & cerebrovascular disease
VDL, LDL, and hyperglycemia
slide 17
(not on leighow’s pp)
Causes of obesity
•Genetics ~40% of the variances in body mass
•Environmental factors that result in increased caloric intake & decreased physical activity
•Other factors include, socioeconomic factors, age, sex & race
•U.S “super-sizing” portions & easily available high-fat foods
•Physical activity is reduced d/t modernization (I-pads, computers, T.V.)
•Our lifestyles are more sedentary
Role of inflammation
•Several inflammatory mediators including, angiotensin, growth factor a, alpha? & interleukin 6 are elevated in morbidly obese patients
•Leads to insulin resistance
•When these patients lose weight, the inflammatory mediators and comorbidities associated with obesity are decreased.
Leukocytes and adipose tissue inflammation.
Macrophage and lymphocyte infiltration in adipose tissue may greatly contribute to obesity-related metabolic dysfunction and chronic inflammation.
Box 48.1 Conditions A/W obesity
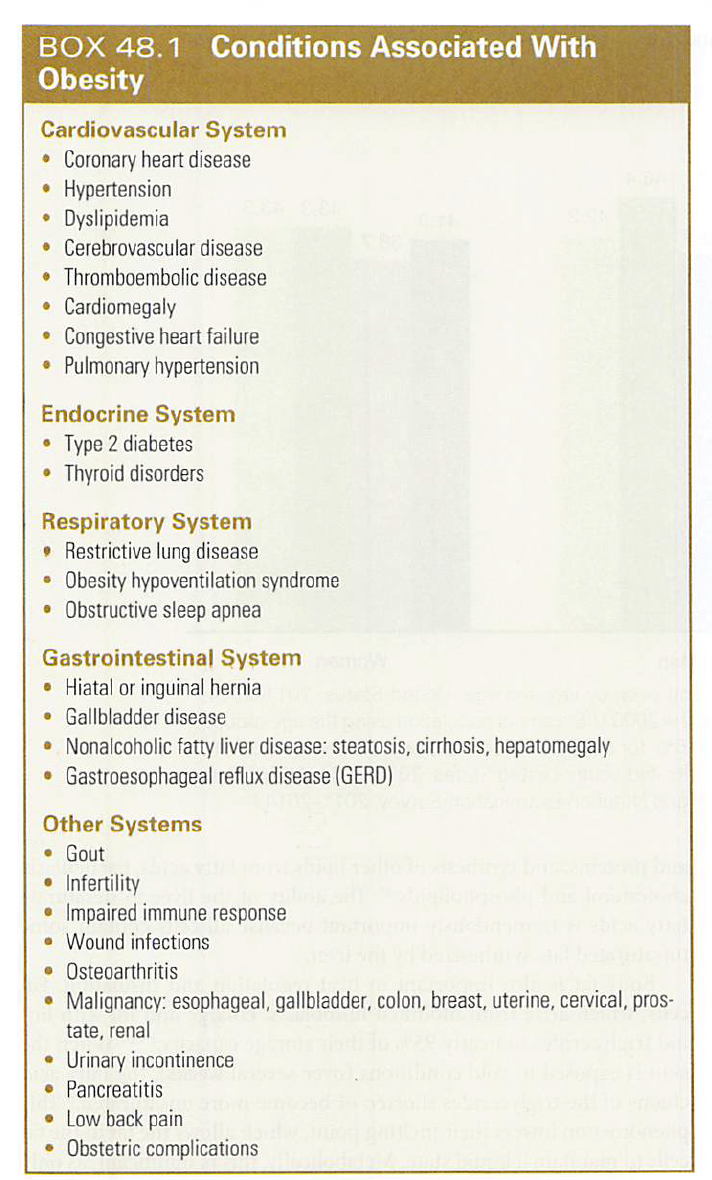
CV disease
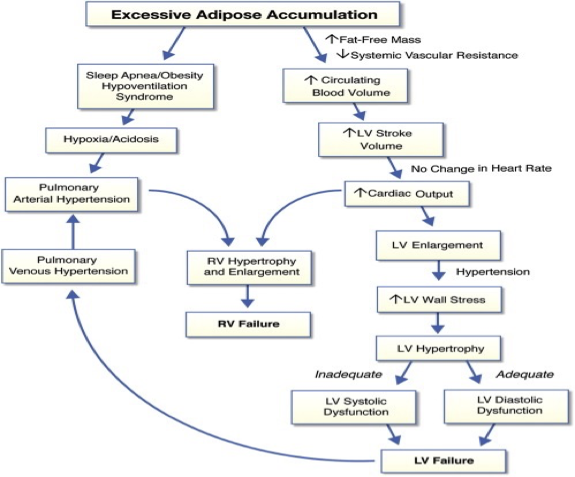
•Cardiac involvement is d/t the compensatory processes that occur to meet the increased metabolic demands
•CVD is the primary cause of the M&M in obese
•Manifests as ischemic heart disease, HTN & cardiac failure
organ is maintained by formation of extra blood vessels & increased circulatory, pulmonary, central & peripheral blood volume
•For every 13.5 (30 lbs.) gained, ~ 25 miles of neovascularization is generated to provide blood flow to the fat tissues
•Increased cardiac output of 0.1 L/min for each kg of fat
•Greater stress on the heart d/t expanded blood volume through expanded vascular system which is under pressure by adipose tissue
•Increased workload l/t increased CO, increased O2 consumption & increased CO2 production
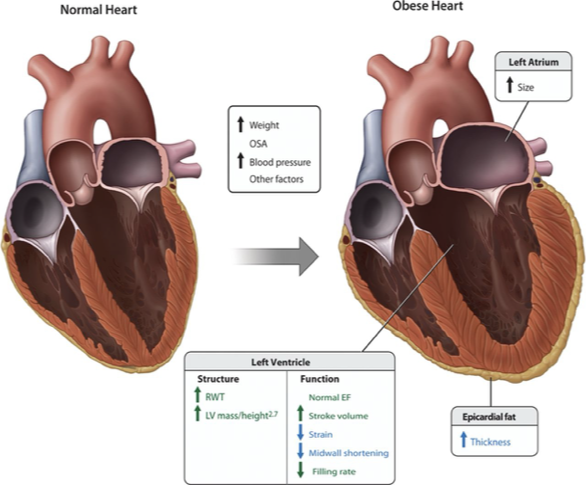
•Higher cardiac output leads to increased left-sided heart pressures and LVH
•HR unchanged= EXAM so increased CO RT increased SV
•Leads to cardiomegaly, atrial & biventricular dilation & hypertrophy which l/t HTN & CHF
•Reduced atrial filling is caused by decreased venous compliance
HTN
•SBP > 140 mmHg & DBP > 90 mmHg or both
Incidence of HTN in obese patients compared to lean patients
•HTN in obese patients is 2x that of lean patients
How much does BP increase per body weight
•BP increases 6.5 mmHg for every 10% increase in body weight
How do severely obese patients who are not hypertensive maintain BF
decreased SVR assists to maintain blood flow through the enlarged body habitus
HTN is due to 5
•increased blood viscosity
•altered catecholamines action
•hyperinsulinemia
•increased mineralocorticoids
•abnormal sodium reabsorption
Renal induced HTN caused by 5
•Visceral compression of the kidneys from fat deposits in & around the kidneys
•Impaired sodium excretion
•Activation of the renin-angiotensin-aldosterone system
•Increased SNS
•Hypercholesterolemia > 240 mg/dl l/t to atherosclerosis & CVAs
Arrythmias may occur due to 7
hypoxemia
hypercapnia
electrolyte disorder
OSA
ventricular hypertrophy
HTN
CAD
What is fequent A/W obestiy
•CAD is frequently associated with obesity, but it is an independent risk factor
CAD can occur ± 5
HTN
hypercholesterolemia
DM
HLD
sedentary lifestyle
Obese patients with CAD have 4
frequent angina
CHF
acute MI
sudden death
When is ischemic heart disease more common
•in obese patients with central fat distribution
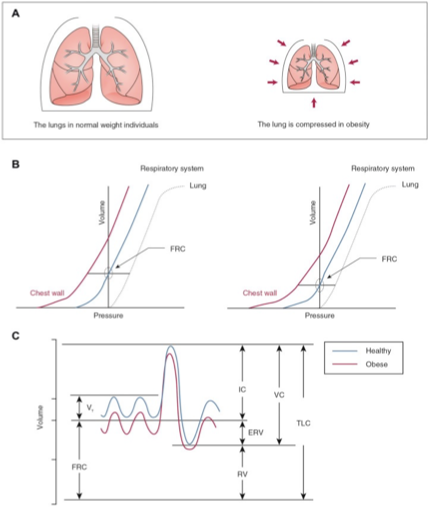
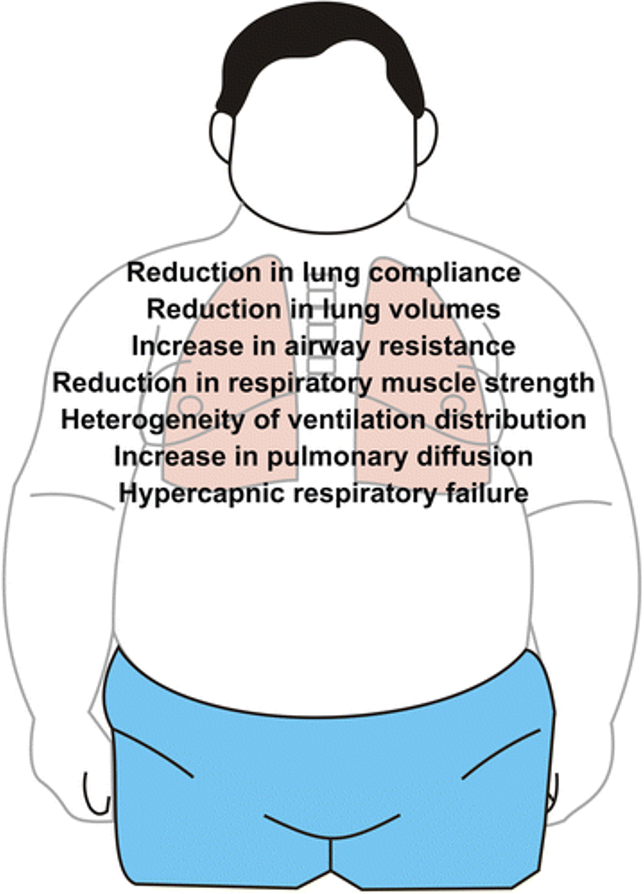
Resp system
•Compromise of the respiratory system results from the compression of fat on abdominal, diaphragmatic & thoracic structures
thoracic kyphosis/ lumbar lordosis impair rib movement and fixes thorax in the inspiratory position
l/t reduced chest wall compliance, parenchyma, lung and pulmonary system→Decreased TLC, VC & FRC
•Greater WOB
•Increases in CO2 production & retention with decreased ventilation L/T reduced respiratory muscle efficiency
•Lung inflation is inhibited—> decreased FRC< than CC
•Premature airway closures increases dead space, and causes CO2 retention, V/Q mismatch, shunting & hypoxemia
•Extreme obesity A/W reduced FRC, ERV, TLC
•FRC declines as BMI increases
•Extreme obese patients will have major reductions in lung function even if asymptomatic
Rapid shallow breathing is from decreases in 4
VC
TLC
ERV
IC
are demonstrated by rapid shallow breathing
characteristics of restrictive lung disease
Decreased VC, TLC, ERV, and IC
•Eventual hypoventilation, hypercarbia and acidosis result from the depression of the CNS’s responsiveness to hypoxia
•Hypoxemia l/t polycythemia & increases rx of CAD CVA
Resp muscule dysfunction results from
•inefficiency d/t changes in chest wall compliance & lower lung volumes which can lead to respiratory failure
Obesity linked to what resp disease
•linked to asthma-like symptoms such as dyspnea, systemic inflammation and increased work of breathing
•Weight loss will result in improvement of these symptoms
Obstructive lung disease
characterized by reduction in airflow. so SOB—> in exhaling air
Air remains inside lung after full expiration
Ex COPD, asthma, Bronchiectasis
Restrictive lung disease
Reduction in lung volume (difficult taking in air in lungs)
RT stiffness inside the lung tissue or chest wall cavity
Ex. ILD, scoliosis, neuromuscular cause, marked obesity
32
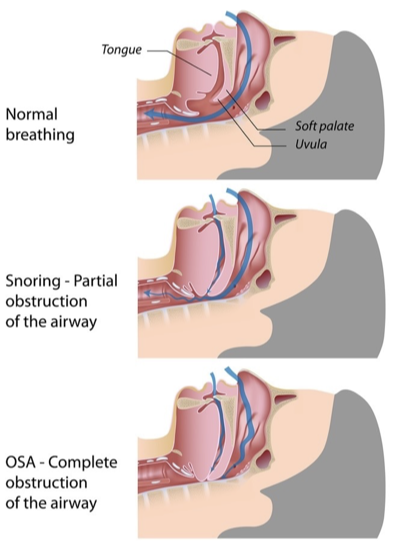
OSA
•Patients with OSA have a BMI > 30kg/m², abdominal fat distribution and neck girth >17 inches in men & 16 inches in women
•Characterized by excessive episodes of apnea (>10 seconds) and hypopnea caused by complete or partial airway obstruction
•OSA is present in 25% of surgical patients
•Apnea is considered obstructive if there is continued respiratory effort despite airflow cessation
•Hypopnea is a 50% reduction in airflow for 10 seconds that occurs 15 or more times per hour & is associated with snoring and low SaO2 readings
•Is diagnosed by10 episodes of apnea-hypopnea per hour of sleep plus daytime sleepiness
•Obese patients have more adipose tissue in the airway & relaxation of muscle tone during sleep leads to collapse of the upper airway
mild OSA as an AHI 5 and 15; moderate 15-30, and severe >30.
•More than 30 episodes per night results in hypoxia, systemic & pulmonary hypertension and arrhythmias
•OSA patients have higher incidences of comorbidities
Mallampati score
Class I: no limitation
Class II: Loss of pillars
Class 3: loss of pillars and fauces
Class 4: Hard palate only
STOP- BANG
STOP
Do you SNORE loudly
do feel TIRED, fatigued, sleepy during day
has anyone OBSERVED you stop breathing
do you have high blood PRESSURE
BANG
BMI >35
Age >50
Neck >40cm
Gender: Male
0-2=low risk
3-4 intermediate
>5 high risk
OSA outpt vs inaptient basis consdierations
•Sleep apnea status
•Anatomic & physiologic abnormalities
•Coexisting diseases
•What surgery is being performed
Type of anesthesia
•Need for post op opioids
•Patient’s age
•Postop observation
•Capabilities of outpt facility: difficult airway equipment, Xray avail, etc.
day sx with OSA
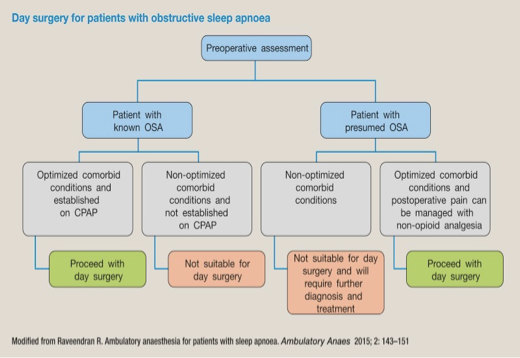
What are the 7 anesthetic concerns
Premedication
Potential difficult airway, difficult mask ventilation, and tracheal intubation
GERD
Opioid resp depression
Carry over sedative effects from longer acting IV and VA
Excessive sedation in MAC
post extubation airway obstruction
Premedication principles of management 2
avoid sedation premedication
consider A2 agonists (clonidine, Dex)
Potential difficult airway, difficult mask ventilation, and tracheal intubation principles of management
optimal positioning (Head Elevated Laryngoscopy Position) if patient obese
Adequate preoxygenate
consider CPAP preoxygenation
2 handed triple airway maneuvers
Anticipated difficult airway. personnel familiar with difficult airway algo
GERD principles of management
Consider PPI, antacids, RSI with cric pressure
Opioid resp depression principles of management
Minimize opioid use
Use short acting agents (remifent)
multimodal analgesia (NSAIDs, tylenol, tramadol, ketamine, gabapentin, pregabalin, dex, clonidine, dexamethasone, melatonin)
consider local and regional anesthesia
Carry over sedative effects from long acting IV and VA agents principles of management
Use prop, remifent for maintence of anesthesia
Use of insoluble potent anesthetic agents (desflurane)
use regional blocks as sole anesthetic technquies
Excessive sedation in MAC principles of management
use intraop capno for monitoring of ventilation
Post extubation airway obstruction principles of management
verify full reversal of NMB
only extubate when fully conscious and cooperative
non-supine posture for extubation and recovery
Resume use of Positive airway pressure device after surgery
Obesity hypoventilation(Pickwickian) syndrome (OHS) characteristics
OSA
•BMI > 30 kg/m²
•Chronic hypercapnia- partial pressure of PcO2> 45 mmHg
•Daytime hypersomnolence
•Arterial hypoxemia PO2 <70
•Cyanosis-induced polycythemia
•Respiratory acidosis
•PHTN —> R HF
Extreme OHS
•patients develop nocturnal episodes of central apnea without respiratory effort
•This reflects the progressive desensitization of the respiratory centers to nocturnal hypercarbia
90% of patients with OHS have OSA
•Alveolar hypoventilation is the main impairment of OHS= EXAM
•Decreased TV, inadequate inspiratory strength & inadequate diaphragm movement
OHS & CNS
decreases central respiratory drive
OHS & airway
potential difficult airway
OSA
OHS & CV
CAD
CHF
OHS & resp
restrictive chest physiology
PHTN
Hypoxemia/hypercapnia
OHS & other
difficult vascular access
difficult positioning
GI system changes with obesity
•High risk for regurgitation & aspiration
•Increased gastric volume & acidity
•Delayed gastric emptying, even if fasted will still have high gastric volume
•Increased incidence of hiatal hernia
•Prone to GERD & esophageal strictures
Give bicitra to
GI disease
•Increased incidence of GERD, gallstones & pancreatitis
•At risk for developing esophageal varices, liver failure & liver cancer
•Nonalcoholic fatty liver disease (NAFLD) includes
Steatosis
Fibrosis
Cirrhosis
Hepatomegaly
Abnormal liver enzymes
Non alcoholic fatty liver disease (NAFLD)
•Most common liver condition in the world
•Frequently found in patients with central obesity or diabetes
•Insulin resistance and obesity are associated with increased lipid influx into the liver and increased triglyceride accumulation
•Clinically, NAFLD is asymptomatic
•Increased risk of cardiovascular disease and diabetes
Gallstones
•Higher concentrations of cholesterol in the bile
•Increased ratio of bile salts to lecithin (fatty substance) causes gallstones
•Jaundice if the bile duct is obstructed
•Laparoscopic cholecystectomy
Endocrine and metabolic diseases
•Obesity is rarely the result of primary endocrine dysfunction
•Thyroid, adrenocortical and pituitary function should be investigated in obese patients
•In women, menstrual problems (oligomenorrhea, amenorrhea, menorrhagia) & hirsutism may be a sign of hypothalamic-pituitary abnormalities
•In men, decreased libido or impotence may be a sign of hypogonadism with low levels of follicle stimulating hormone and testosterone
•80% of individuals with type 2 diabetes are obese
Metabolic syndrome
Central (android) fat is strongly linked to metabolic syndrome
•Metabolic syndrome consists of an array of conditions including glucose intolerance &/or type 2 diabetes, HTN, dyslipidemia, and cardiovascular disease
•Are at increased risk of developing CAD, stroke, PVD, DM2
•Pts have proinflammatory and prothrombotic conditions
Metabolic syndrome diagnostic criteria
Need to have 3/5
central obesity (increased waist circumference >102cm (40”) males; >88cm (35”) females
TG >150
HDL <40 males; <50 females
HTN >130/85 or use of antiHTN meds
fasting BG >100 or meds for hyperglycemia
Orthopedic and joint disease
OA from continued mechanical stress on weight-bearing joints
•Ankles, hips, knees and L-spine= most affected
•Because of limited physical activity, patients may have reduced bone density, may lead to stress fractures
•Bones need to become heavier to support increased weight
Obestiy effects on bone
increases skeletal loading
cushioning affect of fat during falls
increased leptin & estrogen from fat tissue
Less physical activity
poor diet or low nutrient density
Co morbidies (DM)
degenerative joint disease
inflammation
lower vitamin D status
low bone mass relative to weight
poor balance
greater force during falls
Every lb of body weight
adds 5 pounds of force on your knee joints
pediatric obestiy
•~31% of Americans between ages 2-19 are considered overweight or obese
•Obese adolescents have a 70-80% chance of being obese adults
•Childhood obesity has increased risk of premature death and disability in adulthood
•Obese children are 3-5x more likely to suffer a heart attack or stroke before age 65
•Pediatric obesity is more common than diabetes, HIV, cystic fibrosis and all childhood cancers combined
•Prevalence of metabolic syndrome is high due to abdominal obesity, insulin resistance, high triglycerides, HTN, proinflammatory and prothrombic states
maternal obestiy
•Maternal obesity, not diabetes, is the most important link to the nation’s increase in mean birth weights
•Prepregnancy obesity significantly increases the risk for C-Section(40%)
•Both 1st & 2nd stages of labor are longer in obese women
•Increased risk for developing gestational diabetes, HTN, hydramnios, preeclampsia, preterm labor, postpartum hemorrhage & infection
•Risk of miscarriage in first 6 weeks is doubled
•Large for age infants (>4000 g/ 8.8 lbs.) have greater incidence of adolescent metabolic syndrome
•Difficult epidural & I.V. placement
maternal obesity during pregnancy 9
insulin resistance/ DM
induced labor/ C-section
coagulopathies/ DVT
difficulties in anestheic administration
pre-e/ HTN
fetal and neonatal complications
LT AE on mother and baby health
PP complications
Resp complications
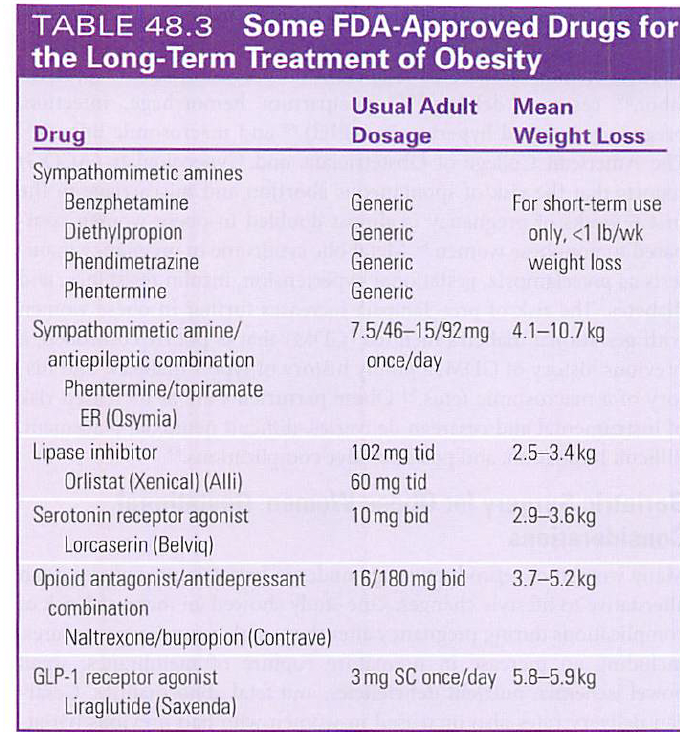
FDA approved drugs for LT tx of obesity
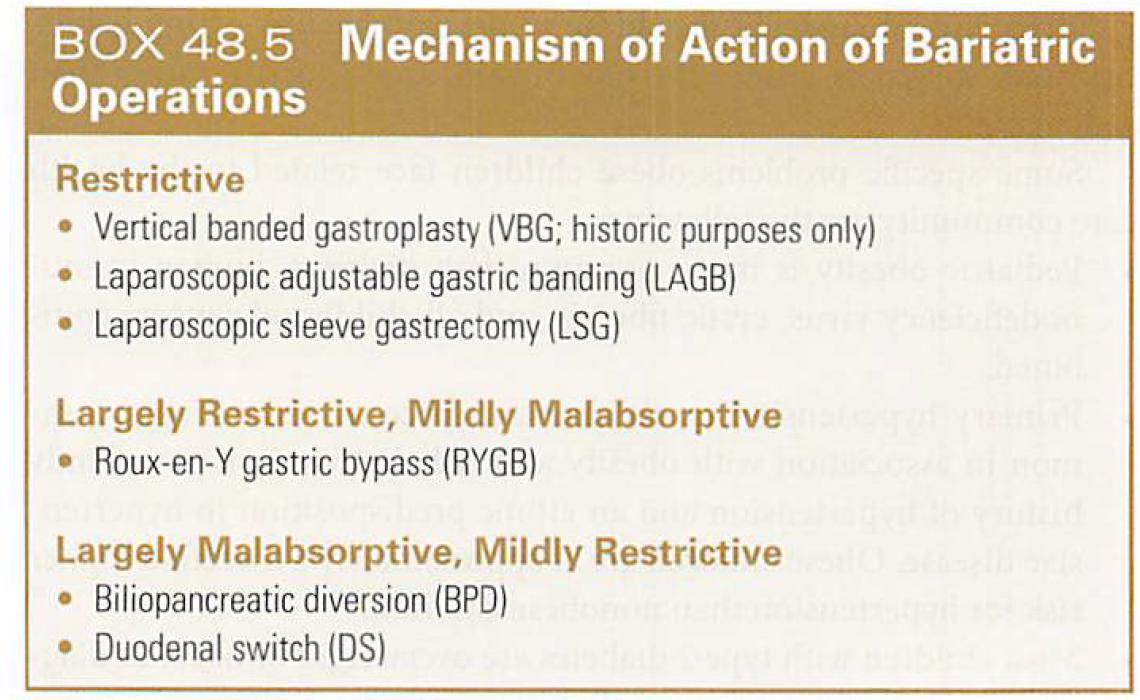
surgerical tx
•Roux-en-Y gastric bypass- largely restrictive/mildly malabsorptive
•Laparoscopic sleeve gastrectomy- restrictive
•Post op N&V common due to suture line & pressure on stomach. Manage aggressively!
f•If pt has GERD, do RSI, cricoid pressure, H2 blocker, proton-pump inhibitors
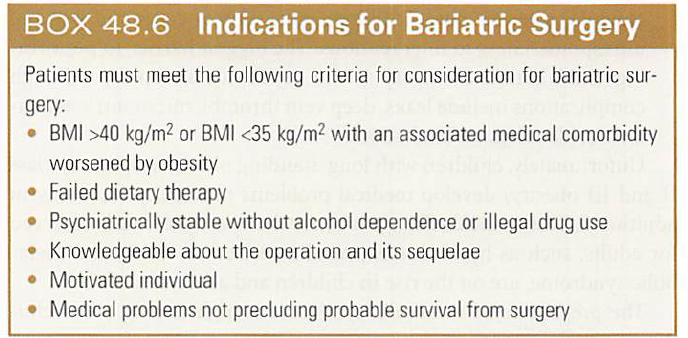
Indications for bariatric surgery
Obesity related diseases requiring surgery
which is the best weight loss surgery
gastric sleeve vs gastric bypass vs lap band

complications following surgery
•Rhabdomyolysis is more common in morbidly obese following laparoscopic procedures
•Careful positioning & padding of pressure points
•Adequate hydration
•Use of mannitol to stimulate diuresis
•Unexplained increase in creatinine phosphokinase (CPK)
•Complaints of buttock, hip or shoulder pain
•Myoglobinuric acute renal failure with CPK> 500 u/L
Pharm considerations with pharmcokinetics/dynamics
•Consider VOD for the loading dose
•Consider clearance for maintenance dose
•Give water soluble drugs according to IBW
•Give lipid soluble drugs according to TBW
•Volume of the central compartment where drugs are first distributed= unchanged
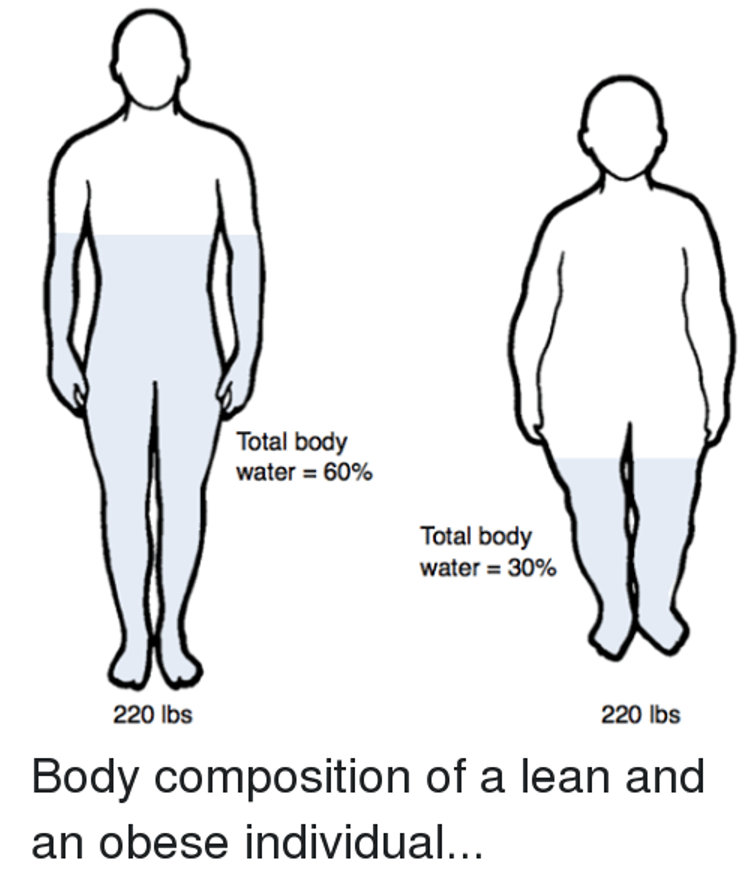
•Absolute body water content is decreased
•Lean body mass & adipose tissue are increased
Pharm considerations
Avoid post op resp depression
use short acting narcotics and adjuncts (tyleol, toradol, gapapentin)
des and sevo are good choice RT low BG coeff
N20 is safe and you use less VA
2nd gas effect N2O with induction and emergence will accelerate uptake and elimination of the VA
N2O has analgesic properties
Make sure to pretreat with antiemtics
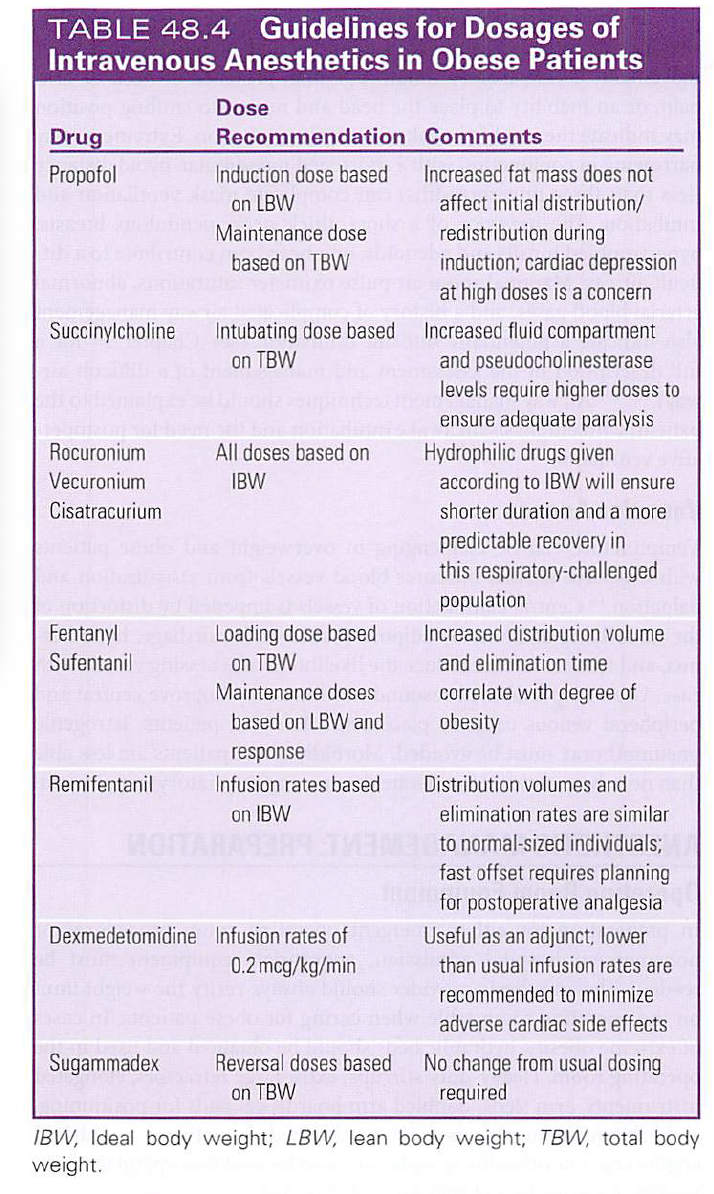
DRUG | DOSE | COMMENT |
Propofol | Induction dose based on IBW. Maintenance dose based on TBW | Increased fat mass doesn’t affect initial distribution/redistribution during induction. Cardiac depression at higher doses |
Succinylcholine | Intubating dose based on TBW | Increased volume of distribution & increased pseudocholinesterase levels require higher doses |
Rocuronium Vecuronium Cisatricurium | Doses based on IBW | Hydrophilic drugs, IBW doses ensure shorter duration & more predictable recovery |
Fentanyl Sufentanil | Loading dose - TBW Maintenance - IBW | Increased vol of distributionà increased loading dose |
Remifentanil | Infusion rate - IBW | Fast off- plan for postop analgesia |
Dexmedetomidine | Infusion rate – 0.2 mcg/kg/min | Use lower than usual rate to minimize cardiac s/e |
Sugammadex | Reverse -TBW | Regular dose/ # of twitches |
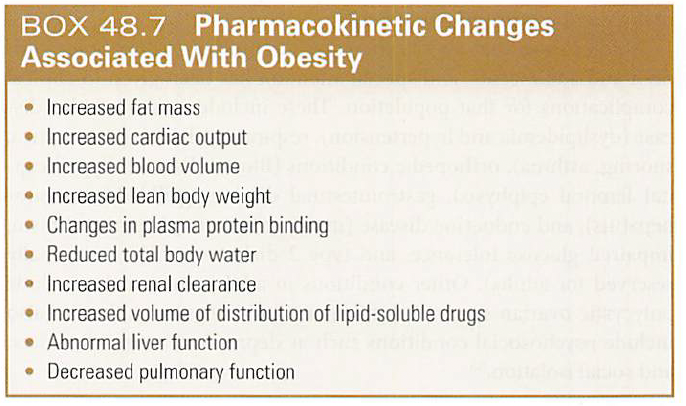
Pharmacokinetic changes INCREASED 8
•fat mass
•cardiac output
•blood volume
•lean body weight
alpha-1-acid glycoprotein (AAG)
•free fatty acids
•lipophilicity of the drug
•Renal clearance d/t increased renal blood flow
Pharmacokinetic changes DECREASED 3
TBW
Liver function
Pulmonary function
Pharmacokinetic changes
Increased distribution of a drug prolongs elimination ½ life (benzos)
•Hyperlipidemia & ↑ AAG-1 reduces free drug concentration
•No significant changes in absorption & bioavailability
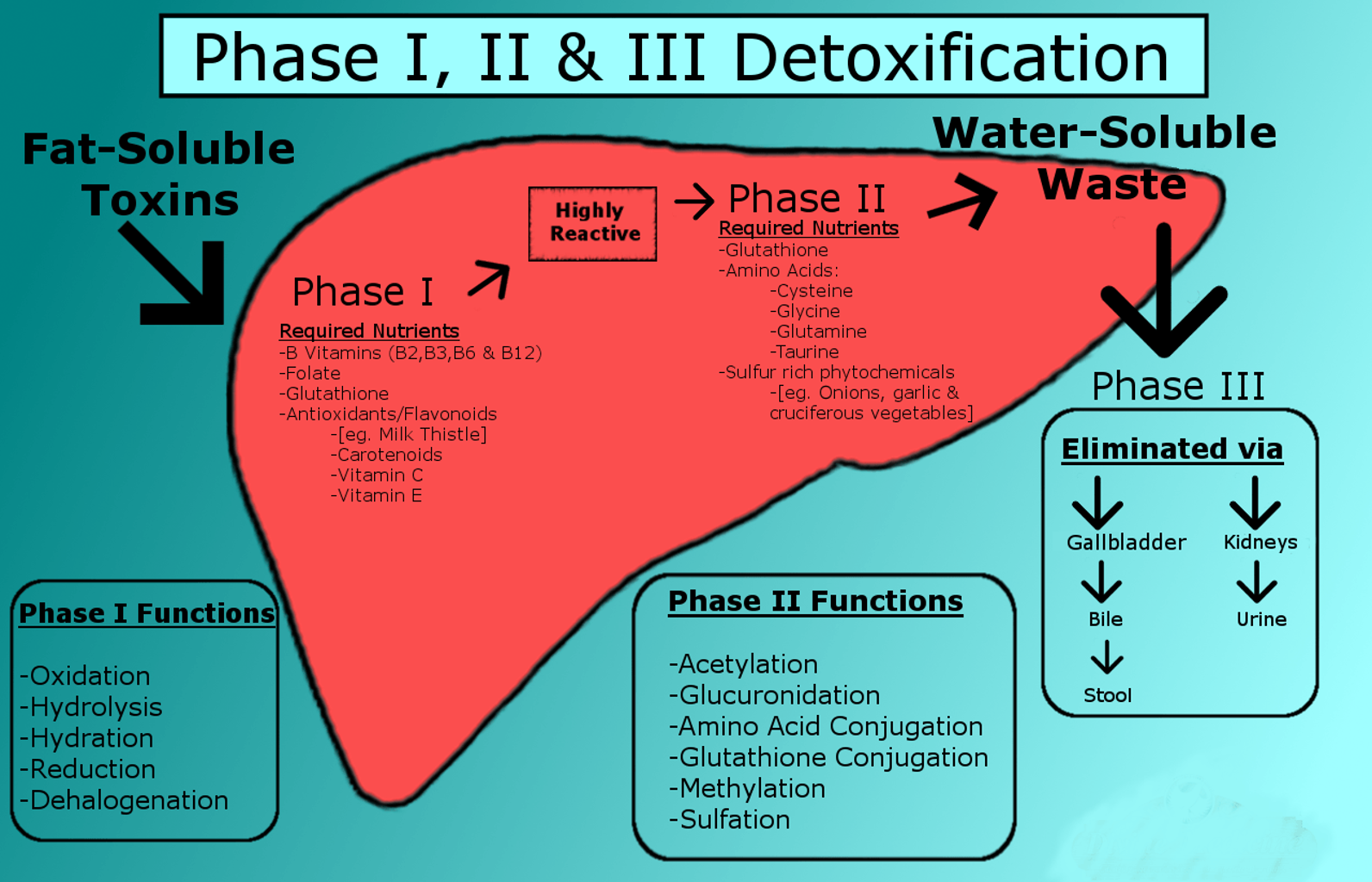
•Drug clearance is not affected by the liver
•Drugs that undergo phase I metabolism (oxidation, reduction hydrolysis) are not affected by obesity
•Drugs that undergo phase II reactions (glucuronidation, sulfation) are enhanced
•Renal clearance is increased d/t increased RBF & GFR
Preanesthetic management
•Discuss anticipated events: multiple I.V. sticks (use US), awake intubation, central line, arterial line, difficult spinal or epidural
•Discuss postop pain plan (if failed spinal or epidural)
•Medications: OTC meds for weight loss? Diet pills can cause ↑ QT-Interval
•Continue usual medications up to surgery, except diabetic meds/insulin
•Prophylaxis against aspiration (Bicitra)
•Prophylaxis against DVT’s (Heparin SQ, check with surgeon)
•Antibiotics given prior to incision, prone to wound infection
•CPAP? OSA?
Lab tests
•CBC, BMP
•Chemistry: K+, Na+
•Blood sugar, what is their A1C? Well managed?
•BUN & creatinine
•Liver enzymes usually elevated
•Coagulation studies if pt. is on anticoagulants
cardiac assessment
•Prior MI? Angina? Added heart sounds?
•Heart failure(hepatomegaly, peripheral edema, elevated jugular venous pressure)
•HTN
•Peripheral vascular disease
•Exercise tolerance: Can you walk up a flight of stairs?
•Continue all cardiac meds up to morning of surgery, except ACE-Is
•12 lead ECG: rate, rhythm, ventricular hypertrophy, axis deviation, QT interval, low voltage reading may underestimate ventricular hypertrophy
•Axis deviation & atrial tachycardia are common
•Sudden cardiac death with morbid obese & refractory dysrhythmias
•ECHO will show LVEDP’s, valvular disease & wall motion abnormalities
•If TR present, think pulmonary HTN
•Cardiomegaly, pulmonary congestion, elevated diaphragm and tortuous aorta can be seen with chest X-ray
•Portable X-rays may not be sufficient to visualize structures on morbidly obese
resp eval
•OSA
•Orthopnea
•Wheezing
•Sputum, recent URI?
•Smoking
•Airway management: beard, edentulous?
•Room air pulse ox reading
airway eval
•Atlantoaxial joint & cervical spine movement d/t cervical fat pads
•Thyromental distance, mouth opening, Mallampati class
•History of difficult airway?
•Mouth has extra tissue, how wide can they open, missing or decayed teeth
•Short thick neck
•Submental fat pad (double chin)
•BMI per se is not a factor in potential difficult airway