Schizophrenia
1/131
Earn XP
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
132 Terms
Why is schizophrenia ranked among top 10 illnesses by W.H.O
30% of schizos attempt suicide
10% die
Where does word Schizophrenia come from
Skhizien= split (split from reality)
Phren= mind
Does schizo effect men + women differently?
Men diagnosed= teens- 20s
Women= 20s-30s
What are the suspected causes of schizo
Brain abnormalities + fam history
Why can diagnostic be hard
Shares symptoms with other mental illnesses
Definition of Classification (and in terms of schizo)
The act of distributing things into different categories of the same type
In context of Schizo, the ICD10 manual lists the symptoms of schizo e.g. auditory hallucinations
How is diagnosis formed?
Questionnaires, interviews of fam + friends, examine mental history
Some treatments that are avaliab le?
Medication, Psychotherapy, Peer + fam support groups
Definition of Schizophrenia
Schizo is a serious mental disorder characterised by severe disruptions in psychological functioning, which affects thoughts, perception, lang + emotion and causes a loss of contact with reality (psychotic symptoms)
Prevalence rate of schizo
1% chance in developing schizo (1 in 100)
Onset is between 15-45 yrs (usually about 5yrs early for men but as common in both genders)
definiton Positive symptoms of Schizo
(not good just additional)
those where there is an addition or an excess to normal cognitive functioning e.g. delusions or hallucinations
Definition Negative symptoms of Schizo
Something in “taken away”
Where there is a loss of normal functioning e.g. affective flattening
Examples of positive symptoms of Schizo (* on spec)
*Delusions
*Hallucinations
Disordered thinking
Examples of negative symptoms of Schizo (* on spec)
*Avolition
*Speech poverty
Affective flattening
Catatonia
Delusions definition
Fixed, untrue + irrational beliefs strongly held despite contradictory evidence, can be bizarre (I can fly- not going to happen), paranoid (watched by gov), grandiose (superpowers). Another class of delusions concerns the body (delusions of control), suffers believe that they or a part of their body is being controlled externally
Hallucinations definition
Unreal perceptions of the environment, usually auditory (voices), may be visual (people who don’t exist), olfactory (smell), tactile, gustatory (taste)
Disordered thinking definition
Inability to think logically. Thoughts often show derailment, which can manifest as convo shifting rapidly from one topic to another making it difficult to understand
Avolition definition
Sometimes called Apathy.
It is inability to take part in goal directed behaviours. Motivation is reduced and individual appears to be uninterested. First signs can be poor hygiene + grooming + then lack of persistence in work or education.
Speech poverty definition
Reduction in amount and qual of speech, sometimes accompanied by a delay in verbal responses. Speech becomes less clear (incoherent). May insert unrelated words midway through sentence
Affective flattening definition
Lack of emotional expression: facial expression, tone of voice + body lang is reduced
Catatonia definition
An extreme loss of motor function. Patients will hold rigid poses for hours which no rection to any environmental stimuli
What is the number of criteria you need to classify as schizo according to ICD
A min of 1 very clear symptom from their 1st rank symptoms or 2 symptoms from their 2nd rank symptoms should be clearly present from the most time during a 1 month period
What are the 1st rank symptoms for ICD (need 1)
Thought echo- thought insertion or withdrawal + thought broadcasting
Delusions of control- influence or passivity, clearly referred to body or limb movements or specific thoughts, actions or sensations, delusional perceptions
Hallucinatory voices giving a running commentary on the patient’s behaviour or discussing the patient among themselves, or other types of hallucinatory voices coming from some part of the body
Persistent delusions of other kinds that are culturally inappropriate and completely impossible, such as religious or political identity, or superhuman powers
2nd rank symptoms (need 2) for ICD
Persistent hallucinations in any modality, when accompanied either by fleeting or half formed delusions without clear affective content or by persistent over valued ideas, or when occurring everyday for weeks or months
Breaks or interpolations in the train of thought, resulting in incoherence or irrelevant speech, or neologisms
Catatonic behaviours such as posturing or waxy flexibility, negativism, mutism + stupor
Negative symptoms, such as marked apathy, paucity of speech, blunting or incongruity of emotional responses, usually resulting in social withdrawal and lowering of social performance; it must be clear that these are not due to depression or neuroleptic medication.
A significant + consistent change in overall qual of some aspects of personal behaviour, manifest as loss of interest, aimlessness, idleness, a self absorbed attitude + social withdrawal
ICD-10 Mnemonics
Destroy- Delusions of control
The- Thought echo
House- Hallucinatory voices
of
Parliament- persistent delusions
Outline how schizo is classified (4 makrs)
Schizophrenia is characterised by both positive + negative symptoms. “Positive” refers to symptoms where there is an addition to function such as hallucinations which are unreal perceptions of the environment e.g. hearing voices giving a running commentary on the person’s behaviour. “Negative” refers to symptoms where there is a lessening of function such as speech poverty whereby speech becomes less clear and the individual may insert unrelated words into their sentence.
The ICD-10 states that 1 ‘first rank’ symptom must be present for the majority of a one month period in order for a diagnosis to be made. Along with Auditory hallucinations, thought echoes is classed as a first rank symptom. This refers to experiences whereby the individual feels that they are not in control of their thoughts + can include thought broadcasting (believe their thoughts can be heard by others)
At least 2 ‘second rank’ symptoms are required for a diagnosis according to ICD- 10. Catatonic behaviour, such as posturing and hallucinations in other sensory modes (e.g. visual) are classed as 2nd rank.
What is reliability in terms of schizophrenia
Consistency- do all specialists agree with the diagnosis
What is validity in terms of schizophrenia
Internal val- how good is a measuring tool/ specialist at diagnosing schizophrenia
Definition of Diagnosis
The recognition and identification of a disease or condition by its signs or symptoms
What is the dominant approach in explaining + treating mental illnesses
The biological approach
What does the biological approach assume about mental illnesses
They can be classified and diagnosed
There are 2 main systems widely used in psychiatry:
ICD (by W.H.O), DSM (by APA- American psychiatric association)
What is the main difference between the ICD-10 + DSM when classifying schizo
DSM only includes auditory hallucinations + bizarre delusions as 1st rank symptoms. ICD also includes thought echo as a 1st rank symptom. bv
What is another difference between the ICD-10 + DSM when classifying schizo
Definition differences, DSM uses bizarre to describe delusions whereas ICD give more detail e.g. culturally inappropriate
What problem may arise because of the difference in DSM + ICD classification?
Issue of diagnosis- someone might be diagnosed as schizophrenic using ICD but not DSM= people don’t get correct diagnosis + correct treatment= likely to get worse.
Who conducted + at what time the experiment ‘Being sane in insane places’
Rosenhan 1973
What can Rosenhan’s experiment be used as
AO1/3 for reliability or validity
Remember no double cred
What does Rosenhan’s experiment highlight?
The problems with validity + reliability of diagnosis of schizo
Rosenhan’s procedure
Sent 8 healthy individuals to try gain hospital admission
12 hospitals were used in 5 states
Some new, old, well-staffed + under staffed hospitals
The ‘pseudopatients’ faked auditory hallucinations, saying the could here voice saying “empty”, “hollow”, “Thud”
They stopped all symptoms after admission + acted normal + said they felt well + asked to be released
Rosenhan’s findings
All diagnosed as insane + Admitted
7/8 diagnosed with schizo + 1 with bipolar
It took p’s between 7+52 days to be released
No doctor or nurse ever identified them as normal
On release they were diagnosed as ‘in remission’ not as sane + healthy
Rosenhan’s conclusions
psychiatrics aren’t very reliably diagnosing schizo as different clinicians may arrive at different diagnoses for same patient /symptoms
They aren’t validly diagnosing schizo as they may not distinguish between real + pseudo patients.
AO1 for reliability
In this context refers to level of agreement on diagnosis by different psychiatrists across time + cultures; the stability of diagnosis over time given no change in symptoms.
An important measure of reliability is inter-rater reliability, the extent to which different Mental Heath professional agree on same diagnosis for patient.
A problem for reliability is there is 2 slightly different classification systems used (DSM+ICD). One difference is DSM has only auditory hallucinations + bizarre delusions as 1st rank symptom but ICD also includes though echoes. So for DSM thought echo doesn’t alone mean a diagnosis.
AO3 for Reliability
Cheniaux 2009- 2 psychiatrics independently diagnose 100 patients with both DSM + ICD. Inter-rater reliability= poor. 1 made 26 diagnosis with DSM, other 13. ICD one made 44 and other 13. This shows very low rates of inter-rater reliability in diagnosis.
Consequently diagnosis may be unreliable. This could lead to a person being diagnosed when the don’t have schizo (false positive)= negative label as schizo has stigma surrounding it, the person may lose personal relationships + could cause a self fulfilling prophecy whereby the person starts to feel paranoid + withdrawn. It could also lead to person with schizo not receiving diagnosis (false neg)= person doesn’t bet treatment + could worsen.
Overall AO1 for validity
In this context refers to the extent to which schizo is a unique syndrome with characteristic signs + symptoms. It can also refer to extent which psychiatrics are correctly identifying schizo. The Cheniaux research also highlights this- results suggest that schizo is being under/ over diagnosed, possibly because it is not being correctly identified in clinical practice.
This may be because of :
People with Schizo often also struggle with PTSD or depression. Co-morbitity
Sub validity AO1- Co-morbidity
The phenomenon that 2 or more conditions occur together within same patient at same time. This can cause problems with diagnosis, as there may be confusion over which disorder is being diagnosed. People with Schizo often also struggle with PTSD or depression. Co-morbidity is a problem for the validity of diagnosis as it could be questioned as to whether schizo actually a sperate + distinct disorder.
AO3 for co-morbidity (sub section of validity)
Evidence for this issue- Buckley 2009- concluded after review around ½ patients with schizo also have depression (50%), PTSD (29%), OCD (23%). shows a problem with validity; perhaps professional aren’t very good at telling the difference, perhaps severe depression looks like schizo or vise versa.
AO1 for symptom overlap
Symptoms of Schizo can also appear in other disorders e.g. bi-polar. Schizo and bipolar both include positive symptoms such as delusions + neg such as avolation. This calls into qu the validity of classification and diagnosis of schizo
AO3 for symptom overlap
Ellason and Ross provide support for this being an issue and point out that people with Dissociative identity disorder have more schizo symptoms than people being diagnosed as Schizo. Makes it very hard for psychiatrist to be certain which disorder the patient has
Cultural bias AO1
Schizo does occur across all cultures it is consistently seen diagnosed more frequently in African Americans and African- Carribean pops living in Britain. Giving rates of schizo are no higher there than anywhere else, there is no biological or genetic vulnerability for these groups of people (so must be cultural)
Cultural bias AO3
Support from Harrison 1988. He argued 1 explanation could be Western clinicians misinterpret cultural dig fences in behaviour and expression as symptoms of schizo. E.G. hallucinations such as hearing voices may be more accepted in African cultures- belief of communication with ancestors and so people are more likely to talk about it. To psychiatrist may seen bizarre or irrationals. Doctors may not be measuring schizo but instead cultural differences which impacts validity.
Gender Bias AO1
Some disagreement between psychologist over gender prevalence rate of schizo. The accepted belief is that make and female are equally vulnerable, some argue that clinicians (who as manly men) have misapplied diagnostics criteria to women. More recent studies show there may be up ton50% more female suffers
Gender Bias AO3
One explanation is female patients tend to function better than men, being more likely to work and have good fam relationships( Cotton). This high functioning may explain why some women haven’t been diagnosed with schizo where men with similar symptoms might have been: their better interpersonal functioning may bias practitioners. Not diagnosing women who show same symptoms as men = diagnosis is not reliable + means that they aren’t diagnosing schizo in a valid way
Final evaluation point for longer answer on reliability and validity of diagnosing and classification of schizophrenia
despite number of problem for reliability and validity since their introduction manuals have been improved and diagnostic practice has improved e.g. categories and definitions are more detailed and operstionsied and psychiatric use standardised interviews when assessing patients. Also ICD and DSM have been brought more in line with each other. Osorio (2019) report inter rater realisability of 97% and test re-test of 92% when DSM was used to assess 180 patients. Such improvements have led to may people receiving reliability and valid diagnosis and timely, effective treatment. More people it’s schizo can now recover to normal level of functioning
What are the 2 biological explanations of schizo
The genetic explanation
Neural correlates
What is the idea of the Genetic explanation if schizo (start of Ao1)
Idea that schizo is passed down to children by their parents via DNA or genetic mutations
There is a strong positive correlation between genetic similarity of family members and likelihood of dev of schizo
Main piece of research for genetic explanation
Gottesman’s family study
What did Gottesman find
The more genetically similar you are to a schizophrenic the greater the chance if you developing schizophrenia
Both parents have schizophrenia-46% of dev
1 parent- concordance rate of 16%
1 sibling- 8%
These concordance rates should be compared against 1% of someone selected at random suffering from schizo
What did later research suggest schizo is? And a study in this?
Aetiologically heterogeneous- it can be caused by number of different gene combos.
Large scale review by Ripke on over 37,000 schizo patients found 108 separate genetic variations associated with an increased risk of schizo. Therefore it is not beloved there is a single schizo gene but serval genes involved which increase and individuals vulnerability e.g. COMT gene
Who researched into COMT gene risk of schizo and what did they find
NIMH
Linked COMT gene on chromosome 22 to a near double risk of schizo. When the COMT gene is abnormally expressed it depletes the frontal lobe of dopamine and has been linked to problems rehearsing the perception of reality
Evaluation + for genetic /Biological explanation of schizo
Twin studies support genetic basis to Schizo. Gottesman reviews over 40 twin studies and found concordance rate for monozygotic twins to be 48% but only 17% for dizygotic twins. Hilker found mono 33% and 7% for dizygotic. This is strong evidence for genetic factors as concordance rates for mono are much higher that dizygotic
(Goes after negs for twins) evidence from adoption studies. Tienari compared 155 children who were given up for adoption by a schizophrenic mother to control group- 155 adopted children who didn’t have schizo parent. Children in Schizo group were 10x more likely to dev schizo. This suggest genetics have a greater influence on dev of schizo than the environment
Evaluation - for the genetic explanation is f Schizo
Problem with genetic explanation, twins presumably share a very similar environment, more so for identical twins as people respond to them the same way. The higher concordance rate in mono may be due to similar environment/ experiences rather than shared DNA
Concordance rate for mono isn’t 100% so psychological influences must be considered. Morkved et al found 67% of schizo patients reported at least 1 childhood trauma compared to 38% in a matched group with non psychotic health problems. Suggest genetic isn’t full explanation
However later analysis of Tienaris’ data found that majority of children that dev schizo came from adopted home named ‘abnormal’. Suggest schizo may be result of genetic predisposition but that it will not develop unless triggered by environment
Overall an interaction isn’t approach to explaining schizo may be more appropriate. This is one which argues schizo is result of combo of biological predisposition (diathesis) e.g. genes, brain abnormalities etc plus environmental triggers (stress) e.g. fam dysfunction, faulty cognitions, recreational drugs
Overall AO1 for neural correlates
The idea that a particular brain area (structure of function) is correlated with schizo. Researchers use non invasive scanning techniques e.g. fMRIs which give a pic of brain in action through use of magnetic fields and radio waves. In this way the functioning of brains of schizophrenics can be compared to none suffers to identify areas linked to schizo. This is best achieved by giving task to ps associated with types of functioning known to be abnormal in schizophrenics e.g. social cognitions through processing and working memory tasks
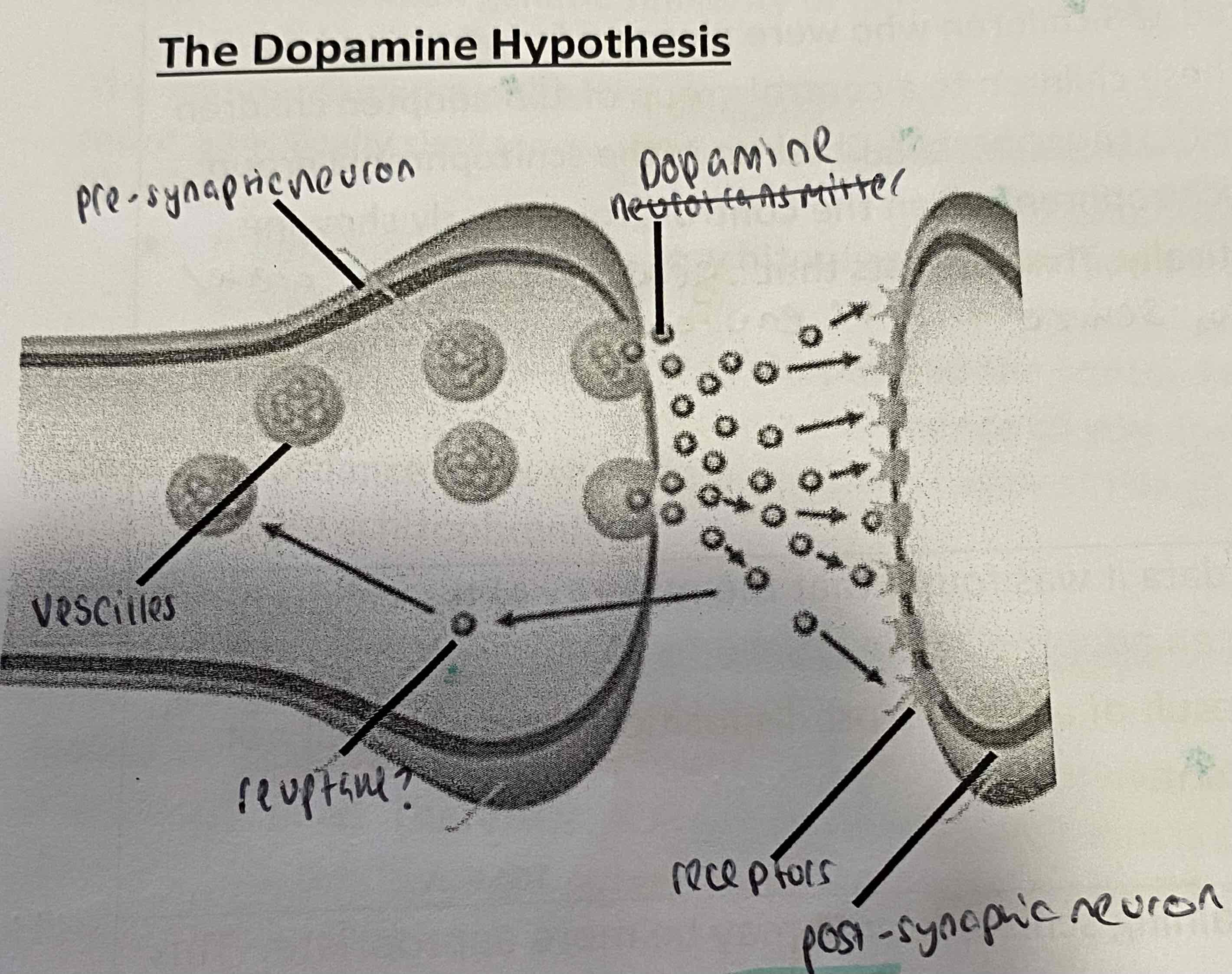
The dopamine hypothesis labels synapse diagram
2 key words in neural correlates explanation
Hyper- more active
Hypo- less
AO1 overall for the dopamine hypothesis (section of neural correlates)
The neurotransmitter dopamine appears to work differently in the brain of schizo patients. Dopamine is important in the functioning of serval brain systems and therefore may cause a wide variety of schizo symptoms
How many dopamine hypothesis are there?
3
AO1 for 1st dopamine hypothesis (hyper)
Schizo is result of hyperdopaminergia in the mesolimbic pathway and s responsible for positive symptoms such as hallucinations. Hyperdopaminergia in regions in the sub cortex (central brain area), e.g. an excess of dopamine in Broca’s area (responsible for speech production) may lead to speech poverty + auditory hallucinations
AO1 for 2nd dopamine hypothesis (oversensitive)
Brains of schizos may be oversensitive to dopamine, as they contain an abnormally high nu. of D2 receptors. Means more dopamine can bind to the receptors which results in increased dopamine transmission. Dopamine neurons also play a key role in the transmission of messages relating to attention. Too many attention messages will result in an inability to focus, which could lead to disordered thinking or delusions (paying attention to irrelevant stimuli)
Ao1 for 3rd dopamine hypothesis (hypo)
Hypodopaminergia in mesocortical pathway (pre frontal cortex) causes neg symptoms e.g. affective flattening. This area controls thinking + decision making and so could also leas to avolition
Summary of 3 dopamine hypothesis
Too much dopamine produced + released
Normal levels of dopamine produced but over stimulation by dopamine receptors at post-synaptic neuron
Too little dopamine produced
AO3 + for neural correlates + dopamine hypothesis
Iverson conducted postmortems and consistently found unusually high levels of dopamine in schizo patients, especially in limbic system. This suggests schizo may be caused by the increased dopamine
Research from PET and MRI scans- Kessler et al compared brain activity in schizos and non schizos, they found schizos had significantly elevated dopamine receptor levels in basal forebrain, supports view they more be more sensitive to dopamine.
These studies provide strong evidence as they are based on empirical, scientific methods. As they have consistent findings it is clear that schizo symptoms are caused by elevated dopamine levels and dopamine hypothesis is a reliable explanation.
Implications from the success of antipsychotic meds also supports hypothesis. Antipsych meds have been 60-75% effective in reducing pos symptoms. Believed to work as they block dopamine activity in the brain, therefore reducing dopamine transmission. Because a reduction in dopamine reduces schizo symptoms it could be assumed that high levels of chemical may be responsible for causing the symptoms, therefore supporting the dopamine hypothesis.
AO3 - for neural correlates + dopamine hypothesis
However, a major issue is that although it is clear that increased dopamine transmissions is linked to schizo symptoms, the dopamine hypo doesn’t explain what has caused the increased levels of dopamine. Not full explanation.
Most of supporting evidence is retrospective/correlational in nature. As a result it is difficult to establish causes+ effect. We don’t know whether the change in dopamine activity in schizos occurs before or after onset. It could be that increased dopamine levels leads t o dev. of schizo or illness causes increased dopamine levels.
AO1 for neural correlates of negative symptoms
One neg symptom, avolition involves the loss of motivation. Motivation involves some complex thinking and decision making processes, and these functions are carried out in the pre frontal cortex. Hypodopaminergia in the prefrontal cortex means fewer messages are sent in this area leading to an inability to take part in goal directed behaviour: avolition. Negative symptoms are associated with several areas in the prefrontal cortex including the orbito-frontal cortex.
AO1 for neural correlates of positive symptoms
Positive symptoms such as auditory hallucinations also have neural correlates. The auditory cortex which is in the temporal lobe is the region responsible for the sensation of sound. Wernicke’s area (also temporal lobe), near auditory cortex, is responsible for the processing of speech so that is can be understood as language. Abnormal activity levels in these areas are thought to cause people to hear voices that aren’t really there, auditory hallucinations. Hugdahl also found significantly reduced grey matter density in schizos in an areas of the cerebral cortex that includes Broca’s area, Wernicke’s area + other lang processing structures.
AO3 + of neural correlates of positive and negative symptoms
Wilbe et al supports neural correlates for negative symptoms. They looked at grey and white matter in the prefrontal cortex in a group of male schizophrenics and matched 'normal' controls using MRI (matched for age, ethnicity, etc). They found no differences in grey matter between the 2 groups. They did find significant reductions in white matter in the right prefrontal cortex in the schizophrenia group which correlated with negative symptoms. This supports the idea that white matter in the (right) prefrontal cortex is a neural correlate for the negative symptoms of schizophrenia.
Support for neural correlates for positive symptoms comes from Allen et al. They scanned the brains of patients experiencing auditory hallucinations and compared them to a control group whilst they completed a task to identify whether pre-recorded speech was theirs or others. Lower activation in the auditory cortex and Wernicke's area was found in the hallucination group, who also made more errors than the control group. This supports the idea that the auditory cortex and Wernicke's area are neural correlates for auditory hallucinations.
AO3 - neural correlate positive + neg symptoms
(cause + effect issue)- Supporting research is useful in identifying brain systems that don’t work normally but I doesn’t tell use if the unusual activity in the brain causes the symptom. There are other explanations for the correlates e.g. neg symptoms such as avolition may cause less info to pass through the ventral striatum causing the reduced activity. Therefore, although neural correlates exist, they tell us relatively little about the causes of schizo.
Despite evidence to suggest existence of neural correlates, there is evidence of environmental factors (e.g. family functioning during childhood) can also play a role in dev of schizo. Suggests that schizo may be result of combo of biological and psychological approaches, implying that an interactionalist approach may be more suitable in explaining schizo
Overall AO1 sentence for family dysfunction explanations
These explanations all suggest the root cause of schizo lies in childhood and adulthood experiences of living in a dysfunctional family
How many family dysfunction explanations are there and names?
3
Schizophrenogenic mother
Double bind technique
Expressed emotions
AO1 schizophrenogenic mother (use for dev of schizo qu or psychological explanations qu)
Frieda Fromm-Reichman proposed a psychodynamic explanation for schizo based on accounts from her patients about their childhoods. Many patients spoke of particular type of parent who Freida described as is cold, rejecting, controlling and tends to create a family climate characterised by tension and secrecy (schizo mother). This leads to distrust that later devs into paranoid delusions + ultimately schizo.
What to look out for in application qu on schizophrenic family life
Fathers in the families witch schizophrenogenic mother are often passive + uninvolved. They don’t chnallage the mother’s neg behaviour or compensate for it. This creates a skewed family: one parent controlling + one with little input.
AO1 double bind theory
Bateson argued that family climate is very important in the dev of schizo. He emphasised the role of the regular communication style within the family. Double bind refers to contradictory messages children receive from the parent, usually on different communicative levels. E.g. if a mother (or another fam member) tells her son that she loves him, yet at the same time turns her head away in disgust, the child receives 2 conflicting messages about their relationship. In a double bind situation the developing child regularly find themselves in a trapped situation where they fear doing the wrong thing + feel unable to comment on the unfairness of the situation. When they get it wrong the child is punished with withdrawal of love.
This leaves the child with an understanding of the world as confusing and dangerous and this reflected in symptoms like disorganised thinking + paranoid delusions. It also prevents the dev of a coherent sense of reality and so could also explain the dev of psychotic symptoms.
AO1 expressed emotions (not as strong an explanation for why schizo appears in first place but good for explaining relapses)
This theory suggest that critcism and hostility lead to schizo and relapse in patients. Expressed emotion is the level of emotion (mainly neg) expressed towards the schizo patient includes:
verbal critcism of patient
Hostility towards them (anger, rejection..)
Emotional over involvement in their life, including needless self sacrifice
High levels of expressed emotion cause stress in patient which is main reason for relapse in schizo patients. Expressed emotion may explain onset of schizo in people with a biological predisposition.
AO3 + for psychological explanations of schizo
Evidence shows that difficult family relationships are associated with increased risk of Schizo. Read et al reviewed studies of schizo, found link between physical + sexual abuse in childhood + later dev of schizo, 69% women in-patients had a history of abuse, 59% for men. Schizo is also most common mental disorder for victims of sexual abuse. This lends support for the family dysfunction explanation as it shows schizo may be influenced by neg family climate + dysfunction.
Evidence to support Bateson’s double bind. Blotchky et al. observed 15 fams with child enrolled in short-term residential treatment program. Found mothers communicated a large proportion of messages, in which verbal content was rated as being conflicting with non verbal expression, to the symptom bearing child (71%) than to other family members + father= didn’t send more conflicting messages to symptom than non symptom family members.
Mothers also contributed the most conflicting messages than any other fam member- supports Fromm- Reichmann’s schizophrenogenic mother.
Evidence from studies into expressed emotion offer support for family dysfunction explanations. Kavanagh reviewed 26 studies of expressed emotion, finding that the mean relapse rate of schizos who returned to live with high expressed emotion families was 48% vs 21% with low. This supports idea family dysfunction leads to schizo symptoms.
AO3 - of psychological explanations for schizo
Info about childhood experience was gathered after dev of schizo. Schizo effects memory recall + includes inaccurate perceptions of reality, therefore it is difficult to establish what experiences from their childhood were real. this creates serious problem for validity of the family dysfunction explanation.
Problem for Blotchky’s research- cause + effect. Possible that mothers contradictory communication style has led to dev of schizo or as mum only uses double-bind with schizo child + not their siblings it is equally possible that the mother’s comms style is result of child having abnormal behaviours. This reduces support for Bateson’s explanation
Most schizo patients have not suffered childhood abuse + come from supportive, stable fams, so must be other factors such as biology e.g. Biological explanation argues that schizo is result of genetics. Idea that schizo is passed down via DNA or a genetic mutation.
This is supported by Gottesman’s family study. He found the more genetically similar you are to a schizo suffer the greater your chances of development. Both parents (46%), 1 parent (16%), one sibling (8%) compared to usually concordance rate of 1%
Therefore as there is evidence for both bio + psych factors a better explanation for dev of schizo would be diathesis stress model which proposes that schizo is a result of a combo of bio predisposition (diathesis) e.g. brain abnormalities, genes, etc plus environmental triggers e.g. family dysfunction, faulty cognitions, recreational drugs
What are the 2 cognitive explanations of schizo
Dysfunctional thought processing
Attention deficit theory
AO1- cognitive explanations- dysfunctional thought processing
Cognitive deficits are a key feature of schizo. Faulty cognitions might be responsible for a lot of the negative symptoms of schizo and some pos symptoms too. Faulty cognitions include poor attention and memory, difficulties with lant + disordered thinking. 2 other important examples for explaining schizo are metarepresentation + central control.
Metarepresentation definition
The cognitive ability to reflect on our thoughts. Dysfunction in metarepresentation may disrupt our ability to recognise our own actions and thoughts as being carried out by ourselves, possibly leading to hallucinations/ delusions which are symptoms of schizo
Central control definition
The cognitive ability to supress automatic responses while performing deliberate actions instead. Dysfunctions in central control may lead to the inability to supress automatic thoughts + speech. This may lead to disordered thinking and speech poverty which are symptoms of schizo
what is the difference in Metarepresentation + central control in normals and schizos
We all have them, when it is dysfunctional that can lead to symptoms of schizo
AO1- cognitive explanations- Attention deficit theory
(have to pick don’t write all of it in long marker)
Frith argues schizo is result of faulty attention system. Preconscious thought contains huge amount of info from our senses that would normally be filtered out. If this filtering process doesn’t happen, there will be a sensory overload in conscious thought. Thoughts that would usually be filtered out as irrelevant instead are noticed as more significant. Frith says this accounts for the positive symptoms of schizo, hallucinations, delusions + disordered thinking.
Not filtering out irrelevant stimulus could lead to paranoid delusions. Activity in the brain regions responsible for attention (e.g. in the prefrontal cortex and anterior cingulate gyrus) has found to be reduced in schizophrenics.
Hemsley- schizophrenia involves a breakdown in the relationship between memory and perception. People with schizo have a disconnect between their schemata and what they actually see and hear. When they encounter new situations, their schemata are not activated. Schizos experience sensory overload because they don’t know which aspects to ignore and not. It means they struggle to predict what happens next. Their poor integration of memory and perception leads to disordered thinking and behaviour that may manifest as avolition.
Definition of preconscious thought
thoughts that occurs without awareness
AO3 + for cognitive explanations
Stirling- compared 30 schizo patients with 18 non- schizo p’s (control) on cognitive task- Stroop test. Schizos took twice as long as control to supress impulse to read the word and read ink colour instead. Supports Frith’s theory of attention deficits suggests schizo may be less able to filter out irrelevant info. It may also be explained through dysfunction in central control- the schizos found it much harder to supress the automatic response of reading the world.
Frith et al conducted PET scans to identify brain systems involved in some cognitive processing processes underlying symptoms associated with schizo. They gave tasks to elicit cognitive processing whilst scanning the brains of schizo patients. They found that schizo patients defects in willed actions (where they want to do something and cant and say it is because an alien is controlling them) and defects of self-monitoring (being aware you are talking out load or in head) were associated with abnormal activity in left hippocampus + frontal lobe= suggest link between cognitive abnormalities described by Hemsley and dev of schizo.
Such research can be considered robust and scientific as the researchers use empirical measures of brain processes
AO3 - for cognitive explanations
Cognitive explanations predict that individuals with schizo would have extreme difficulty completing tasks that require focused attention. McKenna found schizos where more sensitive than control group when judging in photographs of painful electric shocks being administered were genuine or whether they involved an actor. This suggests the attention deficit theory may be too simplistic in its explanation and other explanations that account for this must be considered.
🙂 Mondal et al found this was possibly due to schizos having bias towards negative emptions; they are more successful at reading negative emotions rather than all emotions. This limits the challenge of McKenna’s research poses to the cognitive explanation of schizo
Furthermore it is difficult to establish cause + effect. It is possible that abnormalities in cognitive areas of the brain cause schizo, however, it is equally possible that the illness itself causes the difficulties with cognitive processing e.g. cognitive deficits may be a symptom of the disorder rather than the cause.
Important to consider alternative biological explanations as the psychiatric community regard schizo as a biological disorder. Many studies show high dopamine transmission in the mesocortical pathways create pos symptoms such as hallucinations e.g. Wong found 2x as many dopamine receptor in brains of schizos than controls. Research has also suggested that childhood trauma may be contributing factor. Therefore a more plausible explanation may be diathesis- stress model which suggest a biological predisposition to schizo which is then paired which an environmental or psychological triggers
What are the 2 types of biological therapies
Antipsychotic drugs
Electroconvulsive Therapy (ECT)
AO1 overall for antipsychotic drugs
Most common treatment for schizo. They can be taken as tablets, syrups, injections (given to people at risk of failing to take meds).
Divided into 2 categories: Typical (traditional)- used from the 1950s and atypical (2nd generation)- used from the 1970s
AO1 for typical antipsychotics
The basic mechanism of antipsychotic drugs is to reduce the effects of the neurotransmitter dopamine. According to the dopamine hypothesis schizo symptoms are caused by abnormally high numbers of D2 receptors which increases dopamine transmissions (hyperdopaminergia) in the subcortex, e.g. an excess in Broca’s area may lead to speech poverty and the experience of auditory hallucinations.
Typical drugs such as Chlorpromazine, are dopamine antagonist, which means that they bind to dopamine receptors on the post synaptic neuron, but don’t stimulate them, thus blocking dopamine transmission. This reduces positive symptoms such as auditory hallucinations. Typical antipsychotics bind to dopamine receptors for longer than atypical= longer lasting effect.
Chlorpromazine also effects histamine receptors to produce a sedative effect. This helps reduce anxiety as the patient feels calm.
AO1- Atypical antipsychotics
Clozapine = atypical because it binds to serotonin as well as dopamine receptors. Used to treat positive symptoms and have been found to reduce some neg too. They bind to dopamine receptors on the post synaptic neuron (in particular, D2 receptors) without stimulating them, allowing a more ‘normal’ level of dopamine transmission. More temporary as bind and then dissociate quickly, thought to be responsible for lower level of side effects.
Clozapine is also a serotonin antagonist; blocks serotonin receptors without stimulating them, reducing transmission. Clozapine also includes the release of glutamate. These actions are thought to improve depression, anxiety + neg cognitive symptoms associated with schizo.
Comparison of Typical + Atypical - what neurotransmitters are effected
Typical | Atypical |
Reduction in dopamine transmitters | Reduction in dopamine + serotonin transmitters |
Comparison of Typical + Atypical - Length of effect + why
Typical | Atypical |
Longer lasting effect- binds to dopamine receptor for longer | Shorter lasting effect- bind temporarily then quickly dissociate |
Comparison of Typical + Atypical -Summary of side effects
Typical | Atypical |
Sedative effect- reduce anxiety- feel calmer More side effect but less threatening | Less side effects- more serious + some can be fatal e.g. agranulocytosis |
AO3 + drug therapies
Davis et al= meta-analysis over 100 studies that compared antipsychotics with placebos. Drugs= found more effective. More than 70% of suffers treated with antipsych drug improved within 6 weeks + less than 25% improved with placebo. Suggest antipsych have beneficial medical effect reducing schizo symptoms. Enable patients to live a more normal life.