Transfusion Medicine & Antibody Titration
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
Immunohematology
The study of immunologic responses to blood components
Blood Banking
Procedures involved in collecting, storing, and processing blood. The distribution of RBC and blood components
Transfusion Medicine
Medical practices and clinical uses associated with procurement (acquiring), processing, and distribution of blood components to patient
Benefits & Reasons for Transfusion
Restore/maintain hemoglobin. Done by transfusion of RBC w/o plasma from packed RBC
Restore/maintain blood volume. Whole blood transfusion is limited to situations involving massive trauma
Replace coagulation factors to maintain hemostasis. Components include platelet and cryoprecipitate
Restore/maintain leukocytes. Granulocytopenic (reduced granulocytes) patients with infections that do not respond to antibiotic
Component
Products prepared from whole blood by mechanical methods such as centrifugation
Blood Derivative/Fractions
Products separated by more complex automated processes
Packed Red Blood Cells
If the container is entered (opened), the RBC are usable within 24 hours.
Packed RBC replaced whole blood transfusion practice. Even in the case of severe blood loss, combined RBC and plasma substitutes are used
Blood are irradiated to prevent proliferate of T-lymphocytes that cause GVHD
Used to restore oxygen-carrying capacity
Have the same expiration date if kept sterile while being prepared as the original donor unit
Graft-Versus-Host Disease
The donor T-lymphocytes detect recipient’s body as foreign and attack the tissues
Fresh Frozen Plasma
Replace heat-labile coagulation factors
Not used to replace blood volume or proteins because it can transmit disease. Safer methods including albumin, salt solution (prepared by chemical fractionation of pooled plasma), synthetic colloids (saline/electrolytes).
Good for treating immune deficiencies
NOT a source of all coagulation factor
Factor VIII
Clotting proteins in blood that play intristic pathway of coagulation cascade
Traditionally produce from fresh frozen plasma. Transition to using monoclonal antibody technology to reduce risk of transmitting diseases
Cryoprecipitate
Extracted from fresh frozen plasma
Used as replacement for fibrinogen in cases of liver failure, massive transfusion, or deficiencies in fibrinogen
Plateletpheresis
High yield collection of platelets from whole blood (all components except platelets are returned to donor)
Random donor platelets: four to six random donors (compatible ABO type) units are pooled into a single bag for transfusion. Expire 4 hours after pooling
Platelet concentrates must be monitored for bacterial contamination, are useful in case of massive blood loos & replacement. It can stimulate production of HLA antibodies
Donor Guideline
17 years old (16 by state law)
Weight > 110 pounds
Not have donated whole blood in the last 8 weeks or double red cells in the last 16 weeks
Medical screening
Measure temperature, pulse, BP, hematocrit
1 unit of blood (450mL) is collected
Additional 30mL in extra tubes for testing (HIV, HBV, HCV, HTLV, Syphilis, T-Cell Lymphotropic virus, West Nile virus, T-cruzi)
Anticoagulants & Preservatives
Contain citrate to bind calcium
Contain dextrose to provide energy source for RBC
Phosphate buffer to increase ATP production (RBC viability)
Adenine to prolong shelf life up to 35 days
Store at 1C to 6C. Some type of alarm go off if the temperature deviates.
Autologous Transfusion
Blood collected from patient for re-transfusion at later time into the same individual
Intraoperative autologous transfusion (reinfuses own blood during operation)
Directed Transfusion
Blood transfusion from family or friends
Antigen
A marker that the immune system can detect as self or foreign and initiate appropriate actions
Alloantibodies
Antibodies that was not present at first but form specifically against antigens from another individual
Usually form after exposure through blood transfusion, pregnancy, organ transplant
Example: Rh neg person develops anti-D after exposure to Rh pos
Blood Type Inheritance
Blood Type | Possible Genotype |
|---|---|
A | AA or AO |
B | BB or BO |
AB | AB |
O | OO |
If both parents are type OO, the kid can only be O
If both parents are type AB, the kid cannot be O
Phenotype of genotype AO is A
Phenotype of genotype BO is B
Phenotype
What is seen by tests made directly on the RBC
Genotype
Total genetic makeup, impossible to determine the complete genotype in the laboratory. It requires additional studies especially family studies
Isoantibodies
Naturally occurring ABO antibodies in the blood group system
Type IgM
Immune Antobodies
Antibodies that develop after the immune system is exposed to a foreign antigen
Form after transfusion, pregnancy, transplantation
Type IgG
Avidity
Strength of reaction with corresponding RBC antigens
Hemolysis
Destruction of RBC by the antibody. Rupture of cell membrane and release of hemoglobin
Result is a clear, cherry-red solution with no cloudiness because no cells are present
Complement
Naturally present in the body, complex substance with 18 plasma protein components that aid in hemolysis
Almost all antisera contains complement
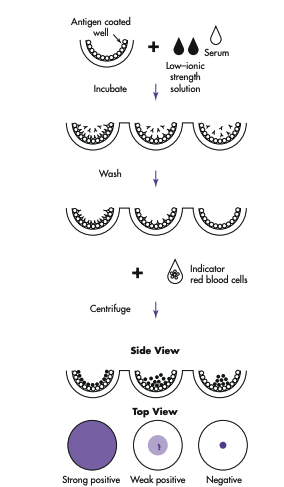
Solid-Phase RBC Adherence Methods
Step 1: Antigen is stuck to the well.
Step 2: Patient antibody is added. It will wash away if not matched, binds to antigen if compatible.
Step 3: Add indicator RBCs. It will bind to the antibody (if present) already on the well.
If antibodies were present → indicator RBCs stick to the well → forms a layer of cells all over the bottom.
If no antibodies were present → indicator RBCs do not stick → they form a tight button at the bottom when the plate is tilted.
Direct Antiglobulin Test (Front) vs Indirect Antiglobulin (Back)
Front type: use known antibody with undetermined RBC
Back type: use known RBC with unknown antibodies
Landsteiner’s Rule
Corresponding antigens & antibodies cannot normally coexist in the same person RBC
Ex: a person with A antigens cannot have antibody-A
Compatibility Testing
Detect unexpected antibodies in the patient’s serum
ABO compatibility
Detect errors in labelling, recording, or identifying patients or donors
Crossmatching
Donor’s RBC with the patient’s serum to detect any antibody in the patient’s serum
Hemolytic Disease of Fetus Newborn (HDFN)
The fetus has the antigen which the mother is negative.
The D-antigen is the most severe/immunogenic (likeliness of stimulating immune response)
The mother formed antibody IgG type that can cross the placenta into the fetus.
The hemoglobin breakdown accumulates bilirubin. The infant can’t produce enzyme to convert bilirubin just yet and this causes severe neurologic problems
Greatest exposure of the mother to the baby’s RBCs with D antigens is during labor and delivery. That’s why it does not occur in the first pregnancy
ABO HDFN occurs when the mother is of type O and the baby is NOT type O
RhIG/RhoGAM
Injected in intramuscularly within 72 hours of delivery in mothers
The anti-d (Rh immune globulin) in the injection bind to fetal antigen-D to prevent the mother from developing anti-D
Antibody Titration
Method to measure titrate (concentration) of maternal antibodies against fetal blood cell antigens. Monitor HDFN using serial twofold dilution
Serial dilute of maternal serum and test against red cells containing the antigen
Record the highest titrate (highest dilution factor that have agglutination)
A fourfold change in titer is
considered significant
Periodically test to measure the trend of titer. Or if ti
Stable titer → low risk to fetus
Rising titer → increased antibody production
Significant rise → possible fetal hemolysis
Critical titer: titer is 16 or 32, considered at risk for HDFN
Maternal Immunizing Event
Exposure of mother to foreign RBC antigens that triggers antibody production
Amniocentesis: medical procedures in prenatal diagnosis of genetic conditions
Miscarriage
Abortion
Chorionic villus sampling: sampling of placental tissue
Cordocentesis: fetal blood sampling
Blunt trauma to the abdomen
Rupture of an ectopic pregnancy: fetal tissue & blood enter maternal circulation
3 Classification of HDFN
ABO
Rh
Other
Prenatal Serologic Tests
ABO/D type & antibody screen
Antibody identification
Determine clinical significance based on patient history/previously affected infant
Human Leukocyte Antigens (HLA)
Found on WBC and most tissues
HLA antibodies produced when exposed to foreign HLA through
Blood transfusion
Organ/tissue transplant
Pregnancy