Cystic Fibrosis
0.0(0)
Studied by 0 peopleCard Sorting
1/154
Earn XP
Description and Tags
Last updated 8:04 PM on 4/1/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
155 Terms
1
New cards
Cystic Fibrosis Progression
Initiation of treatment early in life is critical to prevent disease progression
2
New cards
Cystic Fibrosis: Organ-System Disease
* Multiple organ-system disease
* Pulmonary
* Digestive
* Reproductive organs
* and more are affected
* Pulmonary
* Digestive
* Reproductive organs
* and more are affected
3
New cards
Cystic Fibrosis
Mortality usually due to lung disease
4
New cards
CF Diagnosis
* Newborn screening/ Immunoreactive Trypsinogen (IRT)
* Meconium Ileus (MI)
* Sweat Chloride test
* Meconium Ileus (MI)
* Sweat Chloride test
5
New cards
CF Diagnosis: Newborn Screening/ Immunoreactive Trypsinogen (IRT)
* NOT diagnostic—only identifies infants at risk for CF
* High value necessitates genetic testing
* High value necessitates genetic testing
6
New cards
CF Diagnosis: Meconium Ileus (MI)
* \~ 20% of CF cases present with MI
* 80-90% of patients with MI have CF
* 80-90% of patients with MI have CF
7
New cards
CF Diagnosis: Sweat Chloride Test
* Sweat Chloride test is diagnostic gold standard
* 2nd confirmatory test required
* ≥ 60 mmol/L: CF diagnosis
* Borderline sweat chloride ranges vary between infants and older children/adults
* Patients with borderline values may still have CF
* 2nd confirmatory test required
* ≥ 60 mmol/L: CF diagnosis
* Borderline sweat chloride ranges vary between infants and older children/adults
* Patients with borderline values may still have CF
8
New cards
Cystic Fibrosis (CF) Genetics
* Autosomal recessive disease
* 1 mutation on each allele of cystic fibrosis transmembrane conductance regulator (CFTR) gene leads to CF
* Presentation on only 1 allele prevents full expression of CF
* 1 mutation on each allele of cystic fibrosis transmembrane conductance regulator (CFTR) gene leads to CF
* Presentation on only 1 allele prevents full expression of CF
9
New cards
Cystic Fibrosis (CF) Genetic Testing
* 2 mutations identified on genetic testing of CF patient
* Most common genetic mutation is F508del
* Most common genetic mutation is F508del
10
New cards
Cystic Fibrosis (CF) Severity
Disease severity depends on genetic mutation
11
New cards
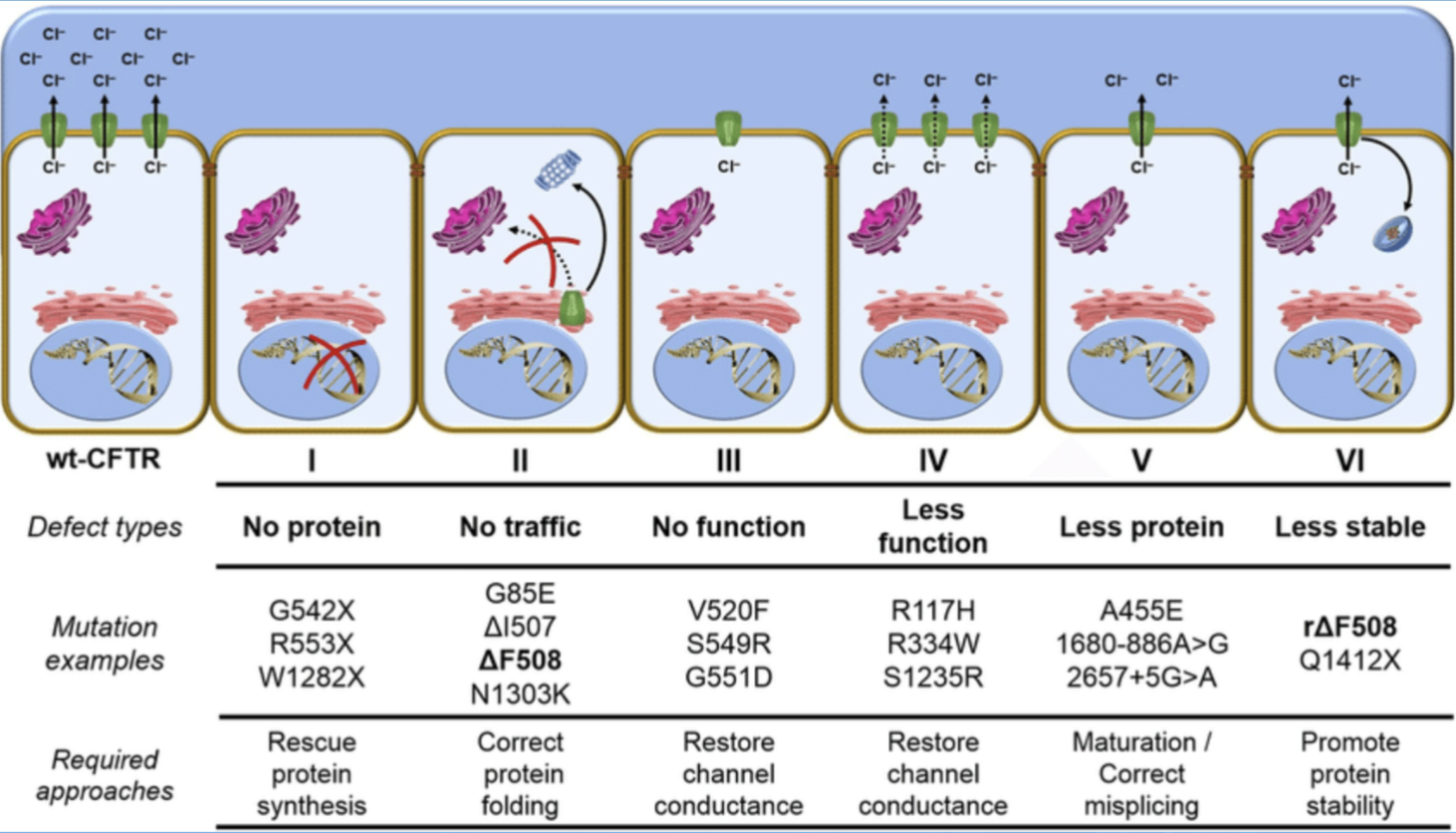
Cystic Fibrosis (CF) Mutation Classes
* Class 1 is the most severe form
* F508del is a class 2 mutation
* Class 4-6 usually pancreatic sufficient
* F508del is a class 2 mutation
* Class 4-6 usually pancreatic sufficient
12
New cards
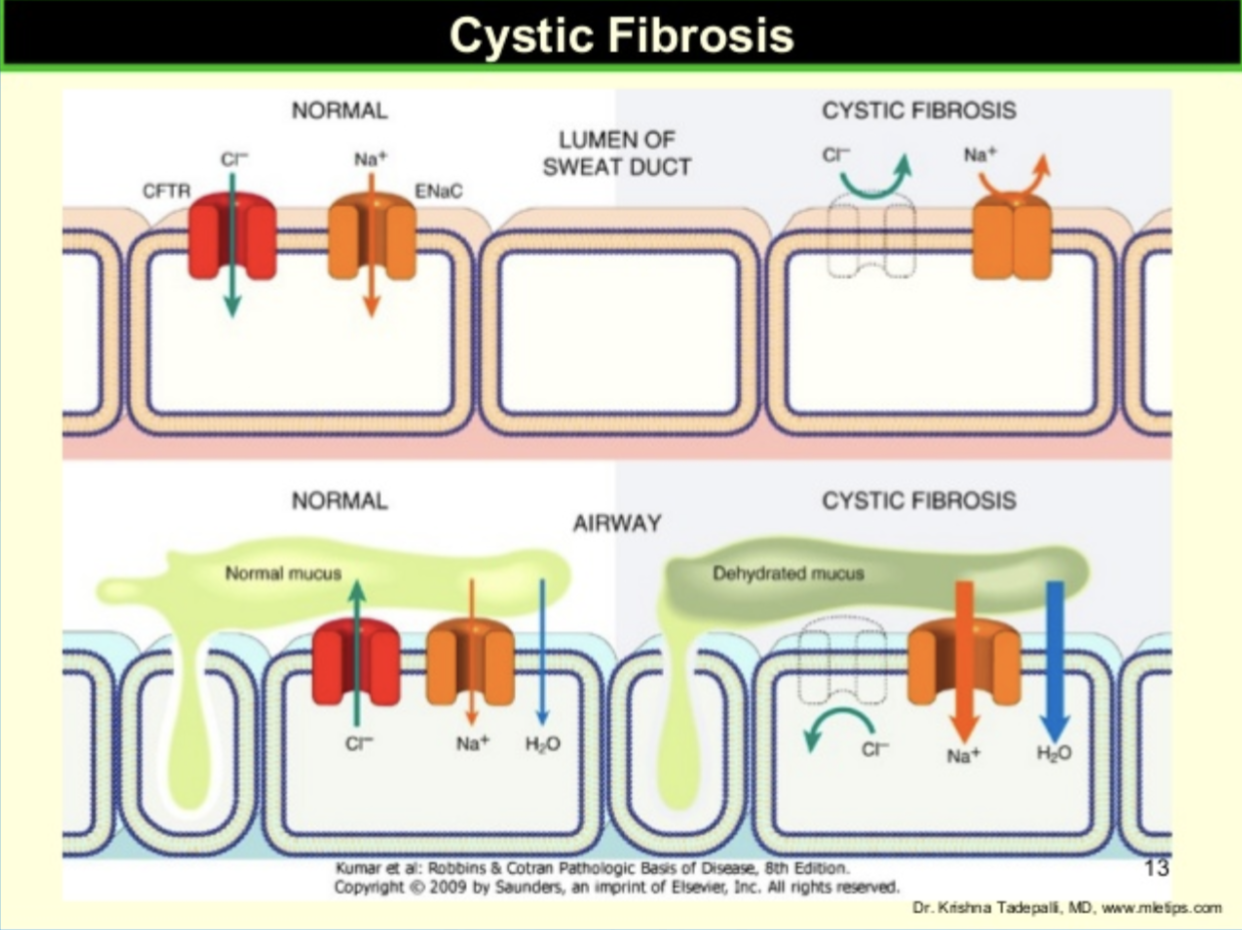
CF Pathophysiology
* Genetic mutations cause defect in the CFTR
* 2000 different genetic mutations identified
* CFTR normally regulates Na+ and Cl- transport across the cell membrane
* Defective CFTR → impaired chloride transport → dehydrated cell surface liquid → mucus plugging → organ dysfunction
* 2000 different genetic mutations identified
* CFTR normally regulates Na+ and Cl- transport across the cell membrane
* Defective CFTR → impaired chloride transport → dehydrated cell surface liquid → mucus plugging → organ dysfunction
13
New cards
Lung Disease
* Thickened mucus → decreased mucus clearance → bacterial overgrowth and colonization → plugging, increased cough, SOB → decreased O2 sats, lung scarring → eventual mortality
14
New cards
Lung Disease: Other Complications
* Pneumothorax
* Pleurisy
* Pleurisy
15
New cards
GI Disease: Bile Duct
Thick secretions in bile ducts → scarring → gallstones, decreased bicarbonate production, liver dysfunction
16
New cards
GI Disease: Pancreas
* Thick secretions in pancreas → plugged pancreatic ducts & scarring
* → decreased pancreatic enzyme secretion → poor digestion → poor nutrient absorption → decreased weight gain, malnutrition → worsened lung disease, osteoporosis
* → decreased or sporadic insulin secretion, impaired insulin sensitivity → hyperglycemia → microvascular complications (nephrotoxicity, neurotoxicity, retinopathy)
* → decreased pancreatic enzyme secretion → poor digestion → poor nutrient absorption → decreased weight gain, malnutrition → worsened lung disease, osteoporosis
* → decreased or sporadic insulin secretion, impaired insulin sensitivity → hyperglycemia → microvascular complications (nephrotoxicity, neurotoxicity, retinopathy)
17
New cards
Reproductive Disease: Males
* In utero blockage of vas deferens leads to male infertility in CF
* **Do not assume infertility**
* Sperm may still be produced and may be retrieved for In-Vitro Fertilization (IVF)
* Recommend genetic counseling
* **Do not assume infertility**
* Sperm may still be produced and may be retrieved for In-Vitro Fertilization (IVF)
* Recommend genetic counseling
18
New cards
Reproductive Disease: Females
* Females may be infertile due to thickened cervical mucus or malnutrition
* Medication counseling by the pharmacist
* Recommend genetic counseling
* Medication counseling by the pharmacist
* Recommend genetic counseling
19
New cards
Cystic Fibrosis (CF) Diet
* High-calorie, high-protein, unrestricted fat diet
* Balance
* Nutritional supplements
* Scandishakes
* Boost, Kids Essentials, Ensure, etc.
* Good nutrition means better lung health, outcomes
* Goal BMI ≥ 50 percentile
* Hyperlipidemia is rare in CF
* Balance
* Nutritional supplements
* Scandishakes
* Boost, Kids Essentials, Ensure, etc.
* Good nutrition means better lung health, outcomes
* Goal BMI ≥ 50 percentile
* Hyperlipidemia is rare in CF
20
New cards
Cystic Fibrosis (CF) and Fat Soluble Vitamins
* Poor absorption of fat-soluble vitamins in CF
* AquADEK
* Contains A,D,E,K and other minerals
* Dosed Qday - BID
* Hydrophilic microsphere structure aids absorption
* 3 formulations: liquid, gelcap, and chewtab
* OTC; often not covered by insurance, cost \~$30/60 doses
* AquADEK
* Contains A,D,E,K and other minerals
* Dosed Qday - BID
* Hydrophilic microsphere structure aids absorption
* 3 formulations: liquid, gelcap, and chewtab
* OTC; often not covered by insurance, cost \~$30/60 doses
21
New cards
Vitamin Supplementation
* Additional supplementation of A, D, E, K may be necessary
* Vitamin K (Mephyton): 5 or 10mg PO Qday to BID
* Vitamin K (Mephyton): 5 or 10mg PO Qday to BID
22
New cards
Percentage of Bone Disease in Cystic Fibrosis (CF)
\~50-75% of CF patients
23
New cards
Cystic Fibrosis (CF): Risk Factors of Bone Disease
* Poor Calcium, Vit D & K absorption
* Glucocorticoid, PPI, H2 blocker therapy
* Low activity levels
* Chronic inflammation
* Glucocorticoid, PPI, H2 blocker therapy
* Low activity levels
* Chronic inflammation
24
New cards
Cystic Fibrosis (CF): Bone Disease Monitoring
Bone density scans and vitamin levels recommended for monitoring
25
New cards
Cystic Fibrosis (CF): Bone Disease Treatment
* Consider bisphosphonates if T/Z score ≤ -2.0
* IV better than oral?? No data, but worry about absorption
* Calcium, Vitamin D & K supplementation
* Exercise
* IV better than oral?? No data, but worry about absorption
* Calcium, Vitamin D & K supplementation
* Exercise
26
New cards
Pancreatic Enzyme Replacement Therapy (PERT) Administration
Administered with all meals and snacks
27
New cards
Pancreatic Enzyme Replacement Therapy (PERT) Capsules
* Capsules contain microtablets or microspheres
* Enteric-coated
* Role of H2 blockers & PPIs
* Enteric-coated
* Role of H2 blockers & PPIs
28
New cards
Pancreatic Enzyme Replacement Therapy (PERT) Dosing
* Dose usually based on units of lipase/kg
* \~1500 lipase units/kg/meal
* Usual max dosage = 2,500 units of lipase/kg/meal, 10,000 units of lipase/kg/day
* Colonic strictures associated with lipase >6000 units/kg/meal
* \~1500 lipase units/kg/meal
* Usual max dosage = 2,500 units of lipase/kg/meal, 10,000 units of lipase/kg/day
* Colonic strictures associated with lipase >6000 units/kg/meal
29
New cards
Pancreatic Enzyme Replacement Therapy (PERT) Brands
DO NOT SUBSTITUTE
* Cotazyme
* Zenpep
* Creon
* Pancreaz
* Pertzye
* Ultresa
* Viokace
* Cotazyme
* Zenpep
* Creon
* Pancreaz
* Pertzye
* Ultresa
* Viokace
30
New cards
Pancreatic Enzyme Replacement Therapy (PERT): Options for Tube Feed Patients
* New options may be coming out soon
* Jejunally-placed tube: Dissolve capsule contents in Sodium Bicarbonate
* Gastrically-placed tube: distribute contents in acidic juice such as nectar-thick (don’t crush)
* Jejunally-placed tube: Dissolve capsule contents in Sodium Bicarbonate
* Gastrically-placed tube: distribute contents in acidic juice such as nectar-thick (don’t crush)
31
New cards
Airway Clearance Techniques
* Percussion vest
* Manual chest percussion therapy (CPT)
* Positive Expiratory Pressure
* Flutter device
* Acapella
* Postural drainage
* Aerobic exercise
* Manual chest percussion therapy (CPT)
* Positive Expiratory Pressure
* Flutter device
* Acapella
* Postural drainage
* Aerobic exercise
32
New cards
Goals of Respiratory Treatments
* Clear mucus from lungs
* Reduce bacterial concentration in sputum
* Improve quality of life & survival
* Reduce bacterial concentration in sputum
* Improve quality of life & survival
33
New cards
Goals of Respiratory Treatments: Clear Mucus from Lungs
* Improve respiratory function
* Prevent further colonization
* Prevent further lung damage
* Prevent further colonization
* Prevent further lung damage
34
New cards
Goals of Respiratory Treatments: Reduce Bacterial Concentration in Sputum
* Reduce inflammation in the lungs
* Prevent exacerbations
* Prevent exacerbations
35
New cards
Correct Order of Respiratory Meds
1) Albuterol (MDI or neb)
2) Hypertonic saline (not used frequently)
3) Pulmozyme
* Vest simultaneously
4) Inhaled antibiotic
5) Steroid nebulizer or inhaler
2) Hypertonic saline (not used frequently)
3) Pulmozyme
* Vest simultaneously
4) Inhaled antibiotic
5) Steroid nebulizer or inhaler
36
New cards
Correct Order of Respiratory Meds Goals
Goal is open, clear airways for better drug distribution and absorption into lung tissue
37
New cards
Drugs for t-piece Nebulizer
As recommended by your physician
38
New cards
Drugs for Sidestream Nebulizer
* Pulmozyme® (dornase alpha)
* Albuterol (salbutamol)Albuterol (salbutamol
* Albuterol (salbutamol)Albuterol (salbutamol
39
New cards
Drugs for PARI LC PLUS® Breath-Enhanced Nebulizer
**Use with 25 psi compressor**
* TOBI®
* Colymycin (sterile colistimethate sodium, USP)
* Albuterol
* Pulmozyme®
* Pulmicort® (budesonide)
* TOBI®
* Colymycin (sterile colistimethate sodium, USP)
* Albuterol
* Pulmozyme®
* Pulmicort® (budesonide)
40
New cards
Drugs for PARI LC STAR® Breath-Enhanced Nebulizer
**Use with 25 psi compressor**
* Colymycin
* AlbuterolAlbuterol
* Pulmozyme®
* Pulmicort®
* Colymycin
* AlbuterolAlbuterol
* Pulmozyme®
* Pulmicort®
41
New cards
Drugs for Altera® with eFlow® Technology Breath-Enhanced Nebulizer
Cayston®
42
New cards
E-Rapid®
* E-Rapid® nebulizer handset now available for use with Altera® compressor
* A substitute for the Pari-LC Plus® nebulizer that allows for rapid administration of meds
* A substitute for the Pari-LC Plus® nebulizer that allows for rapid administration of meds
43
New cards
Hypertonic Saline
* 7% NaCl via nebulizer (some pts use 3% or 10%)
* Increases hydration of airway surface liquid
* Increases hydration of airway surface liquid
44
New cards
Hypertonic Saline Dosing
Qday-BID
45
New cards
Hypertonic Saline ADE
* Can cause airway irritation and bronchospasm
* Use bronchodilator pre-treatment
* Use bronchodilator pre-treatment
46
New cards
Hypertonic Saline Studies
Studies show improved lung function and reduced frequency of exacerbations, to lesser extent than dornase alfa
47
New cards
Hypertonic Saline Indication
* Not FDA approved for CF, but used by >50% of pts
* CF Foundation recommends chronic therapy with hypertonic saline
* CF Foundation recommends chronic therapy with hypertonic saline
48
New cards
Pulmozyme (dornase alfa) MOA
Mucolytic; breaks up long white blood cell DNA strands, decreases mucus viscosity
49
New cards
Pulmozyme (dornase alfa) Dosing
* Nebulized liquid
* Dosed 2.5mg Qday – BID
* Dosed 2.5mg Qday – BID
50
New cards
Pulmozyme (dornase alfa) Studies
Studies show improved PFTs, decreased risk of infections requiring IV antibiotics
51
New cards
Pulmozyme (dornase alfa) ADE
* May cause:
* Increased cough
* Wheeze
* Hoarseness
* Skin rash
* Fever
* HA
* Malaise
* Increased cough
* Wheeze
* Hoarseness
* Skin rash
* Fever
* HA
* Malaise
52
New cards
Pulmozyme (dornase alfa) Indications
CF Foundation recommends using dornase alfa even in asymptomatic patients with mild lung disease
53
New cards
Anti-inflammatory/Other Therapies
* Ibuprofen
* Azithromycin
* Azithromycin
54
New cards
Anti-inflammatory/Other Therapies: Ibuprofen
* Traditional dosing 200-400mg q 4-6 hours
* High dose 20-30mg/kg/day, divided twice daily
* Requires PK monitoring of Ibuprofen levels
* Goal peak 50-100mcg/mL
* High dose 20-30mg/kg/day, divided twice daily
* Requires PK monitoring of Ibuprofen levels
* Goal peak 50-100mcg/mL
55
New cards
Anti-inflammatory/Other Therapies: Azithromycin
* 250mg (
56
New cards
Cultures
* Sputum or throat
* Usually done quarterly
* Often multiple organisms on culture
* Usually done quarterly
* Often multiple organisms on culture
57
New cards
Cultures: Commonly Isolated Organisms
* MSSA (methicillin-sensitive staph aureus)
* MRSA
* __**Pseudomonas aeruginosa**__
* Stenotrophomonas maltophilia
* Achromobacter
* Burkholderia cepacia
* MRSA
* __**Pseudomonas aeruginosa**__
* Stenotrophomonas maltophilia
* Achromobacter
* Burkholderia cepacia
58
New cards
Cultures Complications
* Full eradication is rare; methods being studied
* Antibiotic resistance is common
* Antibiotic resistance is common
59
New cards
Inhaled Antipseudomonal Antibiotics
* Tobi (tobramycin) & Tobi Podhaler
* Cayston (aztreonam)
* Off-label:
* Colistimethate
* Ceftazidime
* Meropene
* Cayston (aztreonam)
* Off-label:
* Colistimethate
* Ceftazidime
* Meropene
60
New cards
Oral Antipseudomonal Antibiotics
* Ciprofloxacin
* Cipro suspension cannot be given per tube
* Cipro suspension cannot be given per tube
61
New cards
Oral Antipseudomonal Antibiotics: Ciprofloxacin Dosing
* Children: 40mg/kg/day PO divided q12 hours
* Lower bioavailability
* Lower bioavailability
62
New cards
Antipseudomonal Antibiotics: Counseling Points
* Benefit outweighs risk of joint/connective tissue toxicity
* Counsel to separate from dairy, enteral feeds, Ca, Fe, Zn
* Counsel to separate from dairy, enteral feeds, Ca, Fe, Zn
63
New cards
Inhaled Tobramycin
Generic tobramycin neb solution now available (do not sub without authorization from MD)
64
New cards
Inhaled Tobramycin Indication
Treatment of CF patients with pseudomonas
65
New cards
Inhaled Tobramycin MOA
* Aminoglycoside
* Inhibits protein synthesis
* Bactericidal
* Concentration-dependent
* Inhibits protein synthesis
* Bactericidal
* Concentration-dependent
66
New cards
Inhaled Tobramycin: Tobi Dosing
300mg (5mL ampule) BID via neb
67
New cards
Inhaled Tobramycin: Bethkis Dosing
300mg (4mL ampule) BID via neb
68
New cards
Inhaled Tobramycin: Tobi Podhaler Dosing
* 4 caps (2 inhalations per cap; 112mg total)
* Inhaled BID via device
* Inhaled BID via device
69
New cards
Inhaled Tobramycin Durations
* Usually 28 days on, 28 days off
* Some patients alternate with Cayston or Colistimethate
* Some patients alternate with Cayston or Colistimethate
70
New cards
Inhaled Tobramycin Counseling Points
Do not mix Tobi in nebulizer with any other meds
71
New cards
Inhaled Tobramycin ADE
* May cause
* Coughing
* Wheeze
* Sore throat
* Hoarseness
* Coughing
* Wheeze
* Sore throat
* Hoarseness
72
New cards
Cayston (aztreonam lysine) Dosing
Dose is 75mg inhaled TID via Altera nebulizer
73
New cards
Cayston (aztreonam lysine) Duration
Usually 28 days on, 28 days off
74
New cards
Cayston (aztreonam lysine) MOA
* Binds to PBP-3 on gram(-) aerobes
* Inhibits cell wall synthesis
* Bactericidal
* Inhibits cell wall synthesis
* Bactericidal
75
New cards
Cayston (aztreonam lysine) ADE
* Cough
* Bronchospasm
* Hoarseness
* Bronchospasm
* Hoarseness
76
New cards
Cayston (aztreonam lysine): Pre-Treatment
Always pre-treat with albuterol or other beta-agonist
77
New cards
Colistin (colistimethate) Dosing
* Dosing is 150mg (diluted in 2 mL of sterile water) inhaled BID via nebulizer
* Use injectable colistin in the nebulizer (off label)
* Use injectable colistin in the nebulizer (off label)
78
New cards
Colistin (colistimethate) Duration
* Usually a 28-day course
* May alternate with tobramycin or aztreonam inhalation for 28d on, 28d off
* May alternate with tobramycin or aztreonam inhalation for 28d on, 28d off
79
New cards
Colistin (colistimethate) MOA
* Cationic detergent
* Damages bacterial cytoplasmic membrane causing leaking of intracellular substances and cell death
* Damages bacterial cytoplasmic membrane causing leaking of intracellular substances and cell death
80
New cards
Colistin (colistimethate) Pre-Treatment
Pre-treat with bronchodilator
81
New cards
IV Antipseudomonal Antibiotics
* Penicillins
* Cephalosporins
* Carbapenems
* Tobramycin
* Ciprofloxacin
* Aztreonam
* Cephalosporins
* Carbapenems
* Tobramycin
* Ciprofloxacin
* Aztreonam
82
New cards
IV Antipseudomonal Antibiotics: Penicillins
Piperacillin-Tazobactam (Zosyn)
83
New cards
IV Antipseudomonal Antibiotics: Cephalosporins
* Ceftazidime (Fortaz)
* Cefepime
* Cefepime
84
New cards
IV Antipseudomonal Antibiotics: Carbapenems
* Meropenem (Merem
* 1st choice among carbapenems
* Doripenem (Doribax) or Imipenem-cilastatin (Primaxin)
* Resistance may develop more quickly to Primaxin
* 1st choice among carbapenems
* Doripenem (Doribax) or Imipenem-cilastatin (Primaxin)
* Resistance may develop more quickly to Primaxin
85
New cards
IV Antipseudomonal Antibiotics: Ciprofloxacin Dosing
10mg/kg Q8H IV required for CF children due to increased clearance
86
New cards
IV Tobramycin Dosing
* Traditional vs. extended interval dosing (EID)
* EID is preferred at the Sacred Heart CF Clinic (q24h dosing)
* EID is preferred at the Sacred Heart CF Clinic (q24h dosing)
87
New cards
Why is extended interval dosing (EID) preferred?
* Provides higher peak:MIC ratio
* Maximizes concentration-dependent post-antibiotic effect
* 2.5-fold higher sputum Cmax vs TID dosing
* Lengthens drug-free interval
* Theoretically decreasing risk of nephro- & ototoxicity
* Increased resistance?
* Improved quality of life?
* Maximizes concentration-dependent post-antibiotic effect
* 2.5-fold higher sputum Cmax vs TID dosing
* Lengthens drug-free interval
* Theoretically decreasing risk of nephro- & ototoxicity
* Increased resistance?
* Improved quality of life?
88
New cards
IV Tobramycin PK Monitoring: Initial Starting Dose
Initial starting dose \~10mg/kg q24h
89
New cards
IV Tobramycin PK Monitoring: Volume & Clearance
Vd & clearance rates are higher in CF
90
New cards
IV Tobramycin PK Monitoring: Tobramycin Levels After 1st or 2nd Dose
**Difficult to obtain consistent levels; much adjustment** **required**
* 2 & 6 hours post-dose for patients
* 2 & 6 hours post-dose for patients
91
New cards
Oral Antibiotics for MRSA
* High-dose Septra
* Clindamycin
* Minocycline, doxycycline (CI
* Clindamycin
* Minocycline, doxycycline (CI
92
New cards
Oral Antibiotics for MRSA: High-dose Septra Dosing
* 20mg/kg divided BID for children
* Septra DS: 2 tabs BID for adults
* Septra DS: 2 tabs BID for adults
93
New cards
IV Antibiotics for MRSA
* Vancomycin, linezolid
* Daptomycin not appropriate (poor lung penetration)
* Daptomycin not appropriate (poor lung penetration)
94
New cards
Stenotrophomonas Maltophilia
* Bactrim is drug of choice (DOC)
* Levofloxacin, minocycline are alternatives
* Often resistant to aminoglycosides & carbapenems
* Levofloxacin, minocycline are alternatives
* Often resistant to aminoglycosides & carbapenems
95
New cards
Burkholderia Cepacia
* Bactrim is drug of choice
* Levofloxacin, minocycline are alternatives
* May be resistant to aminoglycosides, piperacillin, ceftazidime
* Levofloxacin, minocycline are alternatives
* May be resistant to aminoglycosides, piperacillin, ceftazidime
96
New cards
Ursodiol Indication
Treats & prevents CF liver disease
97
New cards
Ursodiol Dosing
* Children: 20-30mg/kg/day, divided BID
* Adults: 600mg BID
* Adults: 600mg BID
98
New cards
Ursodiol Counseling Points
Give with food
99
New cards
Ursodiol ADE
* Constipation
* N/V
* Diarrhea
* Backache
* Dizziness
* Rash
* Cough
* Pharyngitis/bronchitis
* N/V
* Diarrhea
* Backache
* Dizziness
* Rash
* Cough
* Pharyngitis/bronchitis
100
New cards
Ursodiol MOA
Decreased biliary cholesterol concentration → breakdown of gallstones → increases bile flow → protects liver by decreasing toxicity of bile acid