HES 350 Test 3
1/106
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
107 Terms
Heart, blood vessels, and red blood cells
What are the three main parts of the cardiovascular system
Systemic circulation
Blood flow from the heart out toward the body
Pulmonary circulation
Transports blood to the lungs
Heart - arteries - capillaries - veins - heart
What is the order that the blood flows through the body
Atria
Upper chamber
Thinner wall
Receives blood from the venous circulation
Ventricles
Lower chamber
Thick muscular wall
Receives flow from the atrium
Main pump
Right side
What side of the heart provides bloods to the lungs
Left side
what side of the heart is supplying blood to the rest of the body
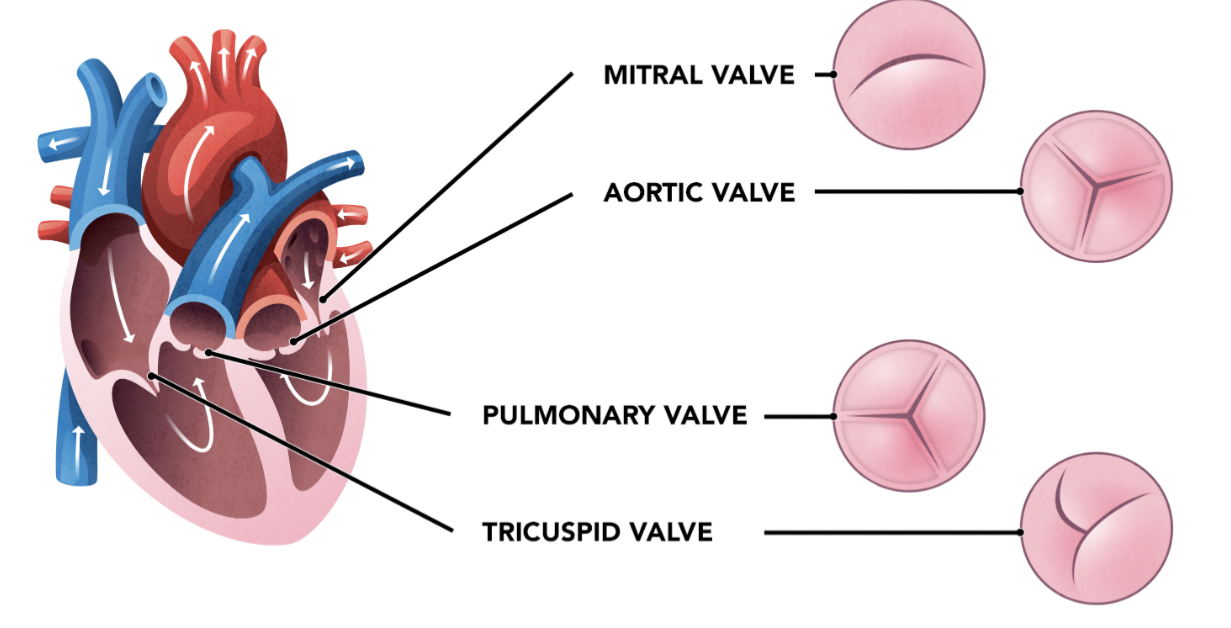
Valves
Chambers are separated by
Made up of these four
Tricuspid
Pulmonary semilunar
Mitral
Aortic Semilunar
Blood vessels
Superior and inferior vena cava fill the right atrium
Pulmonary trunk splits into the pulmonary arteries
Pulmonary veins bring blood to the left atrium
Blood leaves the left ventricle via the aorta
Veins
Have a lot less elastic properties in comparison to other blood vessels
Low pressure flow after the capillaries. Low pressure means valves are required to prevent backflow
Arteries
Role is to deliver high pressure flow from the heart to the tissue
Capillaries
Main role is estrange
has there different forms:
continuous - very tight (brain)
fenestrated - allows larger volumes to move across aveioliar level (kidneys)
Sinusoid - very leaky (found in liver)
Cardiac myocyte
Unlike the skeletal muscle cells which require a motor neuron, the cardiac myocytes form a network that can conduct electricity.
Intercalated discs make it possible to have electrical conductivity
Majority of cells in the heart are myocytes, however there is a larger system of conduction
Intercalated discs:
Desmosomes - connect myocytes structurally
Gap Junctions - connect myocytes electrically
SA Node
Autorhythmic cells - self depolarizing
normal rhythm (pacemaker)
Highest rate of inherent depolarization (sinus rhythm)
Impulses spreads from SA node through atria by internode paths - atrial contractile cells and AV node
AV node
In atrioventricular septum
Connective tissue in septum prevents impulses spreading to ventricles without passing through AV node
Atrial cardiomyocytes
Pause in depolarization at AV node allows ….. to complete contraction before blood flows into ventricles
Atrioventricular bundle
(bundle of His)
Proceeds through inter ventricular septum before dividing into 2 atrioventricular bundle branches (L/R)
Purkinkie fibers
spread impulse to ventricle contractile cells - need notes
Conduction system of the heart
The SA node and the remainder of the conduction system are at rest
The SA node initiates the action potential, which sweeps across the atria
After reaching the AV node, there is a delay approximately NOTES
membrane potential and ion movements - diagram and NOTES
Calcium
Influx through the channels accounts for prolonged plateau phase and long absolute refractory
Combine with troponin in tropomyosin complex
20% of it its required for contraction supplied by influx of it during plateau phase
Remaining amount is released from SR
Echocardiogram
Method for measuring electrical activity in the heart by the placement of electrodes on the skin
P wave
atria depolarization
Patrica contraction 25 sec after start of P wave
Atria depolarization masked by QRS complex
QRS Complex
Depolarization of ventricles
larger due to muscle size
ventricles contract as QRS reaches R wave peak
T wave
Repolarization of ventricles
Segments
Regions between 2 waves
intervals include segment and wave
Cardiac contraction
Contraction of atria to ventricular relaxation
Diastole
Relaxation; filling
Systole
Contraction; ejection
Atrial Systole
Superior/inferior vena cava + coronary sinus - R atrium
Pulmonary veins = left atrium
AV (tricuspid and mitral) valves open - blood flows into ventricles
80% ventricular filling during diastole; 20% with atrial contraction
Ventricular systole
End diastolic volume (preload) = 130 mL
Phase 1 Increased pressure - tricuspid and mitral valves close; not enough pressure top open semilunar valves = isovolumic contraction
Phase 2 (ventricular ejection phase) - increased pressure opens semilunar valves - push blood into pulmonary trunk and aorta
End systomic NOTES
Ventricular Diastole
Phase 1 (isovolumic ventricular relaxation phase): Pressure in ventricle decreases below pulmonary trunk and aorta - semilunar valves close
Phase 2 (ventricular diastole): Pressure in ventricle drops below atria - tricuspid/mitral valves open - blood flows atria to ventricles
MAP
Mean arterial pressure
Average pressure in a person’s arteries across a cardiac cycle
= CO x TPR
= (Hr x SV) x TPR
Cardiac output
CO
A measurement of the amount of blood pumped by each ventricle in one minute (L/min)
Average resting CO is 4-8 L/min
Affects heart ate and the stroke volume
Total peripheral resistance
TPR
Heart Rate
HR
Regulated by both are of the autonomic nervous system
cardioaccelerator and cardio inhibitory center in medulla oblongata
Stroke volume
SV
slightly more complicated
preload, contractility, and after load
higher pressure to lower pressure
Blood flow from
Perfusion
The movement of blood through a tissue
In tissues, it ensures adequate delivery of oxygen and nutrient to support cell metabolism
Arteries are medium size
Capillaries are the smallest
Veins are the largest
Factors affecting heart rate
autonomic innervation
hormones
fitness levels
age
Factors affecting stroke volume
Heart size
fitness levels
gender
contractility
duration of contraction
preload (EDV)
afterload
SV = EDV - ESV
Preload
How full is the heart prior to contraction
similar to end diastolic volume.
As it increases, we have increased stretch on the heart
The greater the stretch the more powerful the contraction is , which in turn increases SV and contractility
Contractility
The force of the contraction of the heart muscle. This is the main determinant of ESV and therefore, impact SV
Positive inotropic effect
Factors that increase contracility
Negative inotropic effect
Factors that decrease contractility
Afterload
To the tension that the ventricles mist develop to pump blood effectively against the resistance in the vascular system
Total Peripheral Resistance
The resistance of the vasculature to blood flow. Determined by a few key vascular features
compliance
blood volume
blood viscosity
blood vessel length
blood vessel diameter
Compliance
The ability of any compartment to expand to accommodate increased content
Blood volume
hypovolemia, hypervolemia
Blood viscosity
The thickness of fluids that affects their ability to flow
Blood vessel length
does not typically change in adults, but increases as we grow
Blood vessel diameter
can be altered by vasoconstriction (narrowing) or vasodilation (widening)
Blood flow
Poiseuille’s law
viscosity doesn’t really change, length doesn’t really change
The radius of a blood vessel is the major determinant of blood flow
Skeletal muscle Venous Pump
For blood to flow from the veins to the atria, the pressure in veins must exceed the atria
pressure in the atria during diastole is incredibly low, often almost zero
Physiological pumps increase venous pressure supporting venous return
muscles relaxed valves closed
muscles contracted valve above muscle opens
Cellular Respiration
Energy production in the cell
Respiration
Process of gas exchange at the lungs
carbon dioxide
Drives respiration because it monitors this gas
oxygen
oxygen and carbon dioxide
Gases are small molecules that follow the same rules of diffusion
both have a concentration gradient, they are not exchanged with one another
COnductiong Zone
Not involved in gas exchange
all about getting air flow down into the respiratory zone
typically larger structures
Nasal and oral cavity, nostril, pharynx, larynx, trachea, born his, lungs, and diaphragm
The structures in conduction zone
Right lung
Has three lobes
The bronchi is much more vertical
Respiratory zone
Gas exchange
Pleural membrane
Serous membrane surrounding lungs (visceral and parietal pleura)
produce fluid to lubricate surfaces and reduce friction between layers
Maintain position of lungs against thoracic wall
pleurisy
Pleural effusion
Visceral pleura
Sit against the organ
Parietal pleura
Sits against the chest wall
Pleurisy
Inflammation of pleura
becomes rough, causing friction and pain
excessive fluid produced that relieves pain - exerts pressure on lungs; hinders breathing
Pleural effusion
Fluid acclimates in pleural cavity
Trachea
notes
Nasal cavity, trachea, bronchi
conductive zone
Epithelial Type: Pseudostratified, ciliated columnar epithelium, goblet cells
Key Features: Cilia beat mucus upward toward pharynx
Function: Traps and removes debris and pathogens
Larger bronchioles
Conductive zone
Epithelial Type: Simple ciliated columnar or cuboidal epithelium
Key Features: Fewer goblet cells; some club cells appear
Function: continue air cleaning; secrete surfactant - like fluid
Terminal bronchioles
Conductive zone
Epithelial Type: Simple cuboidal epithelium with club cells, no goblet cells
Key Features: Smooth muscle present; no alveoli
Function: Control airflow, protect airway lining
Respiratory bronchioles
Respiratory zone
Epithelial Type: Simple cuboidal epithelium, transitions to simple squamous
Key Features: Some club cells; few alveoli budding off walls
Function: Beginning of gas exchange
Alveolar ducts and alveoli
Respiratory zone
Epithelial Type: Simple squamous epithelium
Key Features: Two main cell types
Type 1: Pneumocytes: abundant, thin, flattened for diffusion
Type 2 pneumocytes: Cuboidal, secrete surfactant
Function: Gas exchange across thin barrier; surfactant reduces surface tension
Red blood cells
Important for both oxygen and carbon dioxide for transport
plasma is majority of it includes water, proteins, electrolytes, a dissolved gases
also made up of erythrocytes
Pulmonary ventilation
Act of breathing or the movement of air in and out of the lungs like blood flow, air also flows down a pressure gradient
Inhalation
Air must flow in
Exhalation
Air flows back out
Pressure difference
Lungs alter their volume from inhalation and exhalation, creating … which helps encourage flow
Boyles Law
The pressure of a gas is inversely proportional to its volume; If volume increases, pressure decreases
P1V1=P2V2
compliance
Capacity for stretch to facilitate airflow
Airway Resistance
Resistance to flow
Compliance and airway resistance
Two things that affect the air moving through the body.
Atmospheric Pressure
Patm
Force exerted by the atmosphere 1 atm or 760 mmHG
Intra-alveolar pressure
Palv
changes across the breathing cycle
Intra-pleural pressure
Pip
Also changes across the breath cycle however, is always negative
negative pressure helps with suction
Elastic
What are lungs are made up of
Recoil away from the thoracic cavity. Surface tension in alveoli also plays a role in this recoil
inspiration and expiration
Pulmonary ventilation has two major phases
A complete respiratory cycle
quiet breathing vs forced breathing
Inspiration
active
Diaphragm and intercostal muscles contract
Increases the volume of the thoracic cavity which decreases intra-alveolar pressure
This creates a pressure gradient and air flows in
Pressure is decreasing
Forced Breathing notes
Accessory muscles (scalenes, sternocleidomastoid) and normally respiratory muscles contract more forcefully.
Expiration
passive
Lungs are elastic and this causes the lungs to recoil as the diaphragm and external intercostal muscles relax
This muscle relaxation and elastic recoil increases intra-alveolar pressure above atmospheric pressure
This creates a pressure gradient and air flow out
Forced breathing
Forced breathing
Abdominal muscles (obliques) recrutiez to push the diaphragm up further. Internal intercostal muscles contract to pull ribs down further decreasing thoracic volume
Tidal volume
Air that normally enters and exits during quiet breathing
Expiratory/inspiratory reserve
The volume beyond tidal volume that can be expired and inspired during forced breathing
Residual volume
Air left in the lungs upon maximal exhale
Total lung capacity
Sum of all lung volumes or volume a person can hold in their lungs after forceful inhalaition
Vital capacity
Volume a person can move in or out of their lungs (TV +IRV+ERV)
Inspiratory capacity
Maximum amount of air that can be inhaled (TV+IRV)