Psychopathology
1/37
Earn XP
Description and Tags
definitions of abnormality, phobias, depression, OCD
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
Deviation from social norms
away from the ways most people behave
norms are explicit (laws) or implicit (unwritten)
what is seen as abnormal varies over time and cultures
Evaluation of deviation from social norms
real life application in diagnosis of antisocial personality disorder
social norms change over time e.g. homosexuality was a crime
social norms are culturally relevant e.g hearing voices- this creates problems for once culture within another
can lead to human rights issues e.g. drapetomania (black slaves running away) was a diagnosis to maintain social control
Statistical infrequency
defines abnormality in how many times it is observed
common behaviour in sample= normal
e.g. 2% have IQ below 70 → rare
Evaluation of statistical infrequency
real life application- all assessments of patients with mental disorders involve some measurements of symptons compared with statistical norms.
some rare characteristics are desired e.g high IQ so measurement canot be used alone
having a label does not benefit everyone especially when they are fulfilled and happy. can negatively effect them and how others see them
Deviation from ideal mental health
DO NOT HAVE:
positive attitudes to self
personal autonomy
ability to adapt to environment
resistance to stress
accurate perceptions of reality
healthy self esteem
Evaluation from ideal mental health
comprehensive definition as has a broad range of criteria for mental health so covers most reasons someone would seek help
may be culturally relative to individualistic cultures- emphasis on personal achievement would be selfish in collectivist cultures
unrealistically high standards for mental health- few people would fulfil this criteria
Failure to function adequately
not coping with the demands of each day
severe personal distress and observer discomfort
unpredictable behaviour
e.g. not having a job or maintaing personal hygeine
Evaluation for failure to function adequately
attempts to include subjective experience of individual e.g. their personal distress so captures experiences of people who need help
hard to determine whether someone is struggling to function or just deviating from social norms e.g. extreme sports (treating them as failures would begin to limit freedoms)
deciding this means you have to judge whether a patient is distressed- a psychopath may not feel distressed but is abnormal, a student may feel distressed before exam but this is not abnormal
Types of depression
major depressive disorder- severe but often short term
persistent depressive disorder- long term or recurring
disruptive mood dysregulation disorder- childhood temper tantrums
premenstrual dysphoric disorder- disruption to mood prior/ during menstruation
Behavioural characteristics of depression
activity levels- fatigue or psychomotor agitation (restlessness)
disruption to sleep and eating- insomnia, hypersomnia, weight gain/ loss
agression and self harm
Emotional characteristics of depression
lowered mood- feel worthless and empty
extreme anger- at themselves or others
lowered self esteem- hating themselves
Cognitive characteristics of depression
poor concentration- performing tasks and decision making
attending to and dwelling on the negative- bias to unhappy events and negative aspects
absolutist thiking- ‘everything is bad’, ‘everything is good’
Ellis’ cognitive theory of depression- irrational thoughts
Activating event- negative events that trigger irrational beliefs (interfere with happiness)
Beliefs- “must always succeed” or a “major disaster has happened”
Consequences- emotional and behavioural
Evaluation for Ellis’ theory of depression
Practical application- Ellis’ thoery led to REBT which challengs irrational beliefs to reduce depressive symptons
Only partial explanation- only some cases of depression follow activating events (known as reactive depression) so theory only applies to some
Alternative explanations- depression is a biological condition caused by genes and neurotransmitters e.g drug therapies, SSRIs are effective in the treatment of depression showing neurotransmitters have a role
Cannot determine the origin of irrational thoughts- do negative thoughts cause depression or depression cause negative mindset. Possible neurotransmitters are the cause and negative thoughts are the symptons.
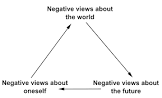
Becks’ cognitive theory of depression- cognitive vulnerability
Faulty information processing- only focus on negative aspects of situation and ignore the positives. small problems are blown out of proportion and we think in black and white.
Negative self schema (developed in childhood and adolescence)- through loss abuse, criticism, meaning we interpret all information about ourselves negatively
Negative triad- negative thinking that occurs automatically
Evaluation for Beck’s theory of depression
Good supporting evidence, Grazioli and Terry
assessed 65 pregnant women for cognitive vulnerability before and after they gave birth
women high in cognitive vulnerability are more likely to suffer post natal depression
Practical application as Beck’s theory forms basis of CBT- components of negative triad can be identified, challenged and rested so translates into a successful therapy
Alternative explanations- depression is a biological condition caused by genes and neurotransmitters e.g drug therapies, SSRIs are effective in the treatment of depression showing neurotransmitters have a role
Cannot determine the origin of irrational thoughts- do negative thoughts cause depression or depression cause negative mindset. Possible neurotransmitters are the cause and negative thoughts are the symptons.
Beck’s cognitive therapy
identify automatic thoughts in the negative triad and challenge them
helps client test reality of negative beliefs- set homework to record events they enjoyed or when someone complimeted them→ in future sessions therapist has evidence against irrational thoughts
Ellis’ rational emotive behaviour therapy (REBT)
extends ABC- to Activating events, Beliefs, Consequences, Dispute, Effect
breaks link between negative life events and depression through vigorous arguments
empirical- actual evidence against beliefs
logical- whether negative thoughts follow logically from facts
Behavioural activation
Works with depressed individuals to decrease avoidance and isolation, more engagements in mood boosting activities e.g. walk, meal out
Evaluation for cognitive treatments of depression
Evidence supporting effectiveness
march et al. compared CBT to antidepressants as well as mixture of both on 327 depressed teenagers
36 weeks: 81% of CBT, 81% of antidepressants, 86% of CBT+antidepressants were significantly improved
Fairly brief (only 6-12 sessions)
First choice of treatment for health services
Long term benefits to stop symptons returning
Few side effects and stops mild depression developing
Lacks effectiveness for severe cases and clients with learning disabilites - Lewis+ Lewis argue CBT is as effective for severe depression
in severe cases clients cannot motivate themselves to engage with cognitive aspect or pay attention
talking therapy not suitable for those with learning difficulties- Taylor et al. argue it is effective for those with learning difficulties
Overemphasis on what is happening in mind which minimizes importance of cirumstances- patient suffering abuse needs to change environment not their thinking
Ethical concerns of being too therapist centred- can lead to an abuse of power, too much dependence or being forced into a way of thinking
Recent studies show long term outcomes are not as good as had been assumed
Ali et al: 42% relapses within 6 months, 53% in a year
may need to be repeated periodically
Behavioural characteristics of phobias
panic e.g. crying, screaming, running away
avoidance- making an effort to avoid stimuli (may interfere with life)
endurance- cope with phobic stimulus but have high levels
Emotional characteristics of phobias
anxierty- unplesant state of high arousal
fear- immediate response
(both excessive and unreasonable)
Cognitive characteristics of phobias
selective attention to the phobic stimulus- hard for person to look away and continue with their day
irrational beliefs in relation to stimulus
cognitive distortions- perception of stimulus is distorted
Behavioural approach to explaining phobias- 2 process model (MAWRER)
classical conditioning- phobia initially required through association
e.g before: white rat → no response
loud noise → fear
during: loud noise+white rat → fear
after: white rat → fear
operant conditioning- once a fear is established, the individual avoids the object/ situation which helps to reduce anxiety. they maintain phobia through negative reinforcement. avoiding behaviour → reward of no anxiety (so repeat avoidance)
Flooding
exposing people to phobic stimulus without a gradual build up
one session lasts 2-3 hurs
without the option of avoidance, client learns phobic stimulus is harmless- extinction
may achieve relaxation by being exhausted by fear response
Systematic desensitization
gradually reduce phobic anxiety though classical conditioning- new response learned by pairing phobic stimulus with relaxation counterconditioning
anxiety hierachy- put together by a client and the therapist, a list of situations related to phobia arranged in order from best to worst
relaxation- taught how to relax as deeply as possible
cannot be afriad and relaxed at same time as one emotion prevents other reciprocal inhibition
e.g. breathing excercises, mental imagery of relaxing situations, meditation, medication
exposure- client exposed to phobic stimulus while in a relaxed state. they work through the anxiety hierachy. the treatent is successful when client can stay in situations high on hierachy. (they could use virtual reality to expose patients to save money and avoid dangerous situation- lacks realism)
Evaluation for flooding
Highly cost effective- clinically effective but also not expensive as can be done in one session unlike systematic desensitization
Not suitable for those with poor physical health or learning difficulties
Highly traumatic experience
high refusal rate- patient to not start treament
high altrition rate- patients do not follow through to the end
find it significantly stressful (as long as clients give informed consent this is not unethical)
Not suitable fo social phobias or agoraphobia as do not address faulty thinking so these may be treated more effectively using CBT which challenges irrational thoughts
Can lead to sympton substitution- do not tackle underlying causes so phobia may only be removed and occur worse at a late data (research is mixed)
Evaluation for systematic desensitization
Preferred as more pleasant
Effective for treating specific phobias
researchers follow up 42 people who had arachnophobia 🕷 and then did systematic desensitization
after both 3 months and 33 months, the systematic desensitization group were less fearful than the control group who had only been taught relaxation
long lasting effects for simple phobias
Suitable for diverse range of patients
those with poor physical health cannot do flooding as anxiety could lead to heart attack
those with learning disabilites find flooding too traumatic and confusing so systematic desensitization is more appropriate
Not suitable fo social phobias or agoraphobia as do not address faulty thinking so these may be treated more effectively using CBT which challenges irrational thoughts
Can lead to sympton substitution- do not tackle underlying causes so phobia may only be removed and occur worse at a late data (research is mixed)
Evaluation for 2 process model
understanding how behaviours are maintained has implications for therapies as it shows patients need to be exposed to their fear stimulus otherwise negative reinforcement happens
systematic desensitization is a behavioural treatment based on this which effectively treats specific phobias
sometimes people develop a phobia without having a traumatic experience- may happen through social learning theory: parent is role model who reacts fearfully and avoides it which leads to children imitating. child may be reinforced for this avoidance as it reduces their anxiety and their parents
does not account for evolutionary factors. stimuli may have been source of danger in past.
biological preparedness- innate preparedness to acquire certain fears
Joslin- wild monkeys had fear of snakes and lab monkeys did not suggesting fear is learned and not evolutionary
evidence that some avoidance behaviour is maintained by positive feelings of safety rather than anxiety reduction e.g people with agoraphobia WILL leave the house if they are with a trusted person or on a particular road
Behavioural characteristics of OCD
compulsions
repetitive- sufferers of OCD are compelled to repeat a behaviour e.g. counting
reduce anxiety- an attempt to manage anxiety produced by obsessions e.g. hand washing to conquer fear of germs
avoidance- attempt to reduce anxiety by keeping away from situations that trigger it which can lead to people avoiding ordinary situations and can interfere with living a normal life
Emotional characteristics of OCD
Anxiety and distress- obsessive thoughts are unpleasant and frightening, anxiety can be overwhelming
Accompanying depression- low mood and lack of enjoyment in activities. compulsive behaviour only brings temporary relief.
Guilt and disgust- negative emotions such as irrational guilt (over minor moral issues) or disgust (external or internal)
Cognitive characteritics of OCD
Obsessive thoughts- recur over and over again and are very unpleasant e.g. impulses to hurt someone
Cognitive strategies to deal with obessions- religious person may pray or meditate constantly which appears abnormal and distracts them from everyday life
Insight into excessive anxiety- people suffering from OCD are aware it is not rational but still suffer catastrophic thoughts about worst case scenarios. Also tend to be hypervigilant.
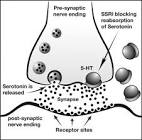
Biological treatment for OCD
SSRIs- selective seretonin reuptake inhibitors
improve mood and reduce anxiety experienced by patients with OCD
e.g. Prozac
when seretonin is released from the presynaptic cell into the synapse, it travels to the receptor sites on the post synaptic cell.
seretonin which is not absorbed into the post synaptic cell is reabsorbed into the pre-synaptic cell.
SSRIs increase the level of seretonin available in the synapse by preventing it from being reabsorbed
increased level of seretonin improves communication betyween cells.
may be combined with anti-anxiety drugs or CBT
tricyclics- similar but with more severe side effects
SNRIs- increase seretonin and noradrenaline
Genetic explanation to OCD
OCD is inherited by receiving specific genes from parents that influence onset of OCD
candidate genes- create vulnerabiity for OCD (such as genes involved in transport of seretonin)
polygenic- several genes are involved (Taylor- 230 genes are involved. e.g. COMT= increases dopamime, SERT= decreases seretonin
one group of genes may cause OCD in one person but different group in another.
different genetic variations may lead to different types of OCD
more likely to have it if relatives have it
Lewis- OCD is genetic vulnerability so have to have genes and environmental trigger to actually develop it.
37% had parents with OCD
21% had siblings with OCD
Nestadt- studied 80 patients with OCD and 343 of their relatives, and compared them with 73 people without OCD and 300 of their relatives.
patients with first degree relative with OCD are 5x more likely to develop OCD than having no relative with it
Diathesis stress model (genes+trigger=OCD)
Neural explanation for OCD
orbital frontal cortex sends worry signals to thalamus
usually supressed by caudate nucleus after a behaviour has been performed.
if the caudate nucleus is damaged then the thalumus is alerted which confirms “worry” to orbital frontal cortex creating a worry circuit ♻
Low levels of seretonin means there is an abnormal transmission of mood relevant information so the person has low mood and other mental processes are affected.
Evaluation for neural explanation for OCD
evidence to support neural mechanisms- antidepressant drugs can relieve OCD symptons by increasing seretonin demonstrating that seretonin is involved
cannot assume neural mechanisms cause OCD
evidence that some neural systems do not work properly in patients with OCD but does not mean abnormalities cause OCD
could just be a sympton but hard to know as would not have studied brains before OCD developed
seretonin link with OCD may be due to comorbidity as patients also have depression. they cannot tell if the seretonin system is disrupted due to just OCD.
Evaluation for genetic explanation for OCD
good supporting evidence- NESTADT et al reviewed twin studieds: 68% of MZ twins shared OCD and 31% of DZ twins highlighting the genetic influence.
genetic explanation minimises environmental risk factors- twin studies never show 100% concordance meanng OCD cannot just be due to genes
Cromer- over ½ of OCD patients had traumatic event in their life
therefore more effective to focus on environmental causes as can actually change these.
not useful as so many potential genes are involved so cannot predict OCD.
Evaluation for SSRIs
Soomra et al- reviewed research examining effectiveness of SSRIs
significantly more effective than placebos in treatment of OCD across 17 different studies
symptons declined significantly for 70% of people taking SSRIs
only researched short term effectiveness not long term effects
SSRIs- lead to nauseau, constipation, weight loss, insomnia, headaches
Tricyclics-lead to constipation, dizziness, weight gain, heart rhythmn problems
this means people stop taking them
Simpson- 45% of patients relapsed within 12 weeks of completing medication course
only 12% when completing CBT
therefore only a short term solution- will return
Drug treatments were criticised for treating symptons not the cause
Koren et al. suggested psychological treatments such as CBT may be more effective long term to providing lasting treatment and care
take 3-4 months to start working