4. Neuropsychological Assessment Measures 2
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
59 Terms
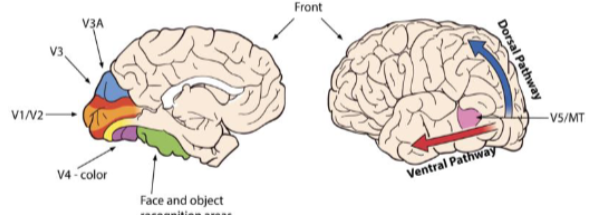
Visual system
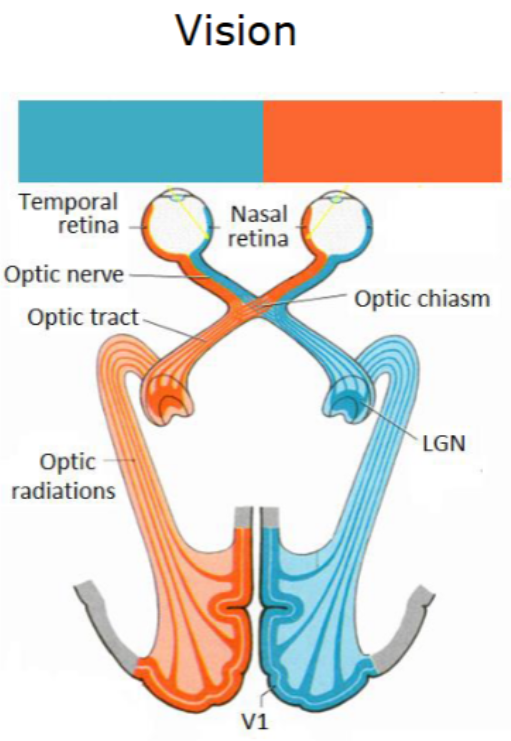
Optic radiations
Optic radiations - can split them into inferior and superior.
Images from superior visual field processed by inferior parts of the retina - adjacent representations.
That mapping retained for the rest of the visual system.
Inferior optic radiations - processing for superior visual field
IOR - come through part of temp lobe
SOR - come through part of parietal lobe
Both I and S are branches of middle cerebral artery and branches from posterior cerebral artery as they move to more posterior sections.
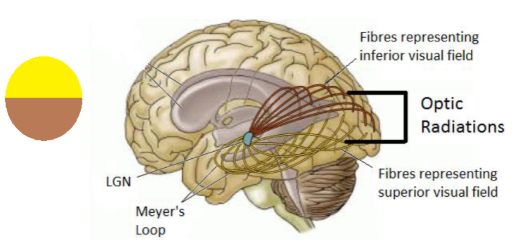
Inferior optic radiations
Processing for superior visual field
IOR - come through part of temp lobe
Branches of middle cerebral artery and branches from posterior cerebral artery as it moves to more posterior sections.
Superior optic radiations
Come through part of parietal lobe
Branches of middle cerebral artery and branches from posterior cerebral artery as it moves to more posterior sections.
Different types of stroke on optic radiations
Spreading out of optic radiations - only inferior and superior could be damaged, but then would see different pattern of visual impairment if the whole thing is damaged.
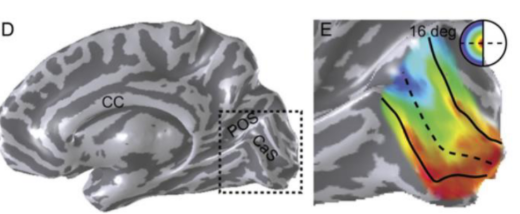
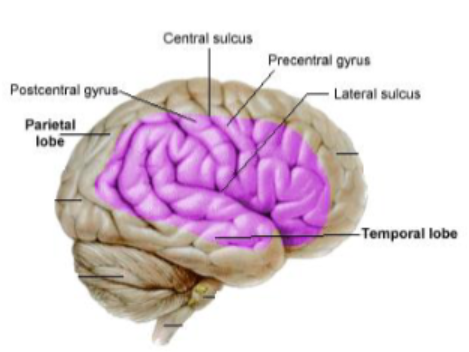
Parts of the primary visual cortex (PVC)
Central parts - POS, CaS
Processed on most posterior of PVC.
Further out in visual field - move further forward in PVC.
PVC at the back but moves anteriorally across the surface.
As representations moves further across the PVC, there are less neurons processing it - more resources at central parts, which is why vision at the side is more fuzzy as it is processed by fewer neurons.
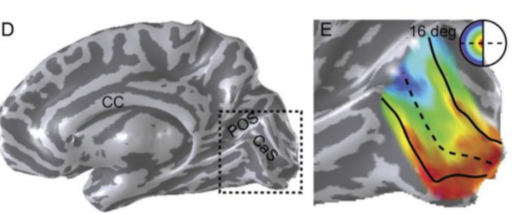
Lesion to the central PVC vs. further out regions
If a lesion took out the red activity, vision would be missing. As long as the red area is preserved, a lesion will have less impact on other coloured regions.
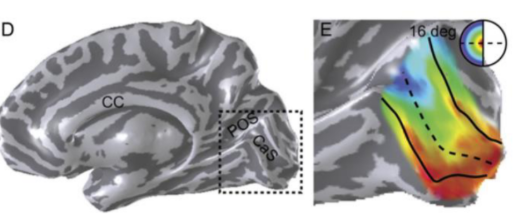
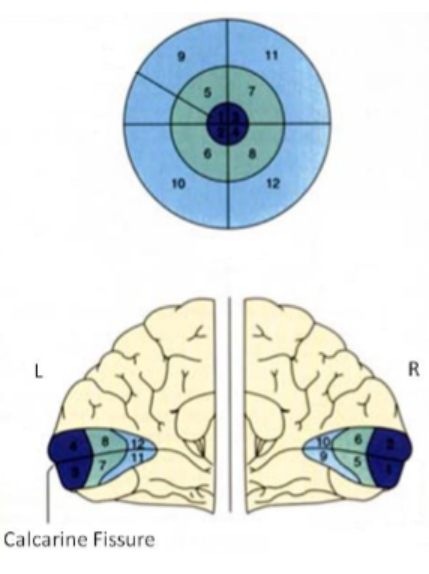
How are elements of the visual field represented?
Each hemifield is represented in the contralateral hemisphere.
Fovea at occipital pole and increasingly peripheral regions are represented towards middle of the brain.
Purpose of the Posterior Cerebral Artery (PCA)
Supplies blood to B1 and the PVC
Visual field
Everything that can be seen whilst fixating
Visual field defect
An area of blindness
Quadrantanopia
Loss of a quadrant of the visual field
Hemianopia
Loss of half of the visual field
Possible causes of hemianopia
Could be damage to entire of V1 in one hemisphere
Could be damage to other locations along that primary visual pathway
Could be superior and inferior radiations
Scotoma
A hole in the visual field, most likely following certain types of trauma
Are all people with visual impairments aware of their defect?
Not necessarily - some people may not be perceptually aware, and it might only be apparent through their behaviour (e.g., not seeing something that should be in their visual field).
Sorts of behavioural problems brought from visual impairments
Driving - prohibited
Reading
Seeing objects
Avoiding collisions
Using public transport
Negative impact on social + emotional functioning
What might the extent of reading difficulties caused by visual loss depend on?
Location and size
Left or right?
Typically worse for right
Foveal sparing or splitting?
Worse for sparing
Issues with measuring visual field defects
Measure is subjective
Reliant upon patient comprehension and cooperation
Conditionalities - remind them to fixate? Prompt for answer?
Sensation belongs to the patient so the examiner must rely on them
Individual criteria can only change - patient might decide to say they've seen it if they think they have - response criteria shifts, variability to data.
Suggestion can also modify a patient’s response, so be careful with instructions.
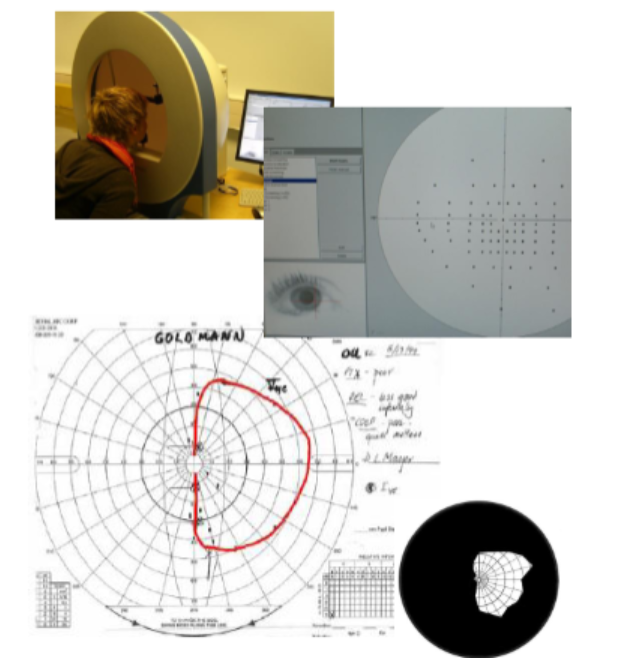
Perimetry
Examination which yields a description of the affected and preserved portions of the visual field.
Perimetry process and methods
Patient look at nose.
Then researcher puts hands out to sides and wiggles them until patient can see them.
Test all parts of visual field.
Method 1:
Confrontation
Method 2:
Perimeter
Perimetry limitations
Not good at distinguishing the boundary between seeing and blind.
Patient may be influenced by sounds instead of sight.
Preferable to use formal parametric method (image)
Present spots of light.
Use a clicker to indicate if they can see it.
Important to test eye separately
Issue with large number of available parametric tools
If the department you're working in has one of those tools, that's the one you're going to use - the one that's most readily available, the cheapest thing.
Nice Guideline (NG236; 2023) for stroke rehabilitation in adults, relating to vision

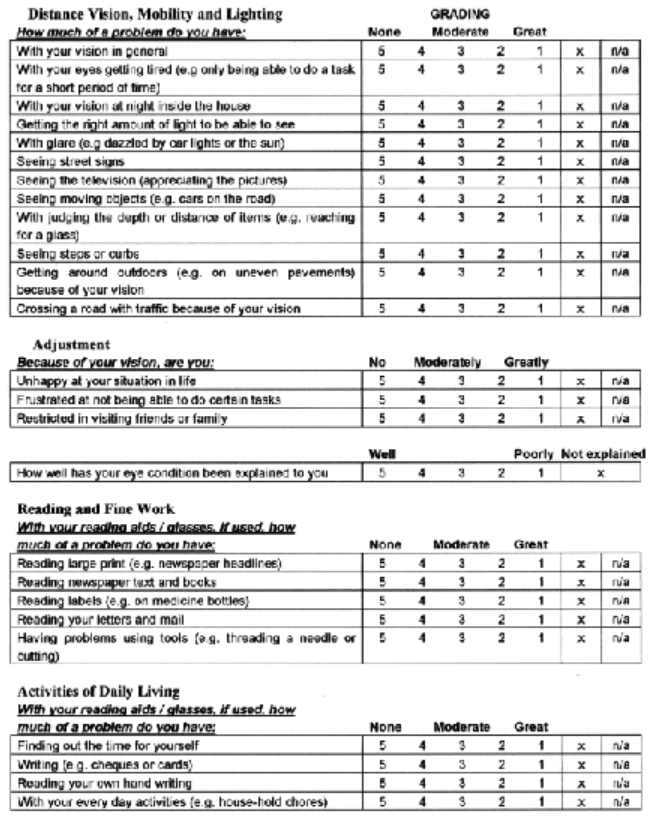
National Eye Institute Visual Functioning Questionnaire – 25 (VFQ-25) (Mangione et al., 2001)
Measure of vision-related quality of life.
Available in self-administered and interviewer-administered formats.
25 items:
General health
Difficulty with activities
Responses to vision problems
Means we're not just relying on perimetry.
Low Vision Quality-of-Life Questionnaire (LVQOL) (Wolffsohn & Cochrane, 2000)
High order perception
Motion
Colour
Shapes
Faces
Objects
Test for achromatopsia?
Farnsworth Munsell 100 Hue Test - people given coloured dots and have to put them into a sequence.
Apperceptive agnosia
The inability to recognise objects despite having intact sensory capabilities.

Associative agnosia
The inability to recognise or assign meaning to objects despite having intact sensory perception.

Edmans et al. - agnosia
76% of elderly stroke survivors suffer from agnosia.
~74% are never diagnosed.
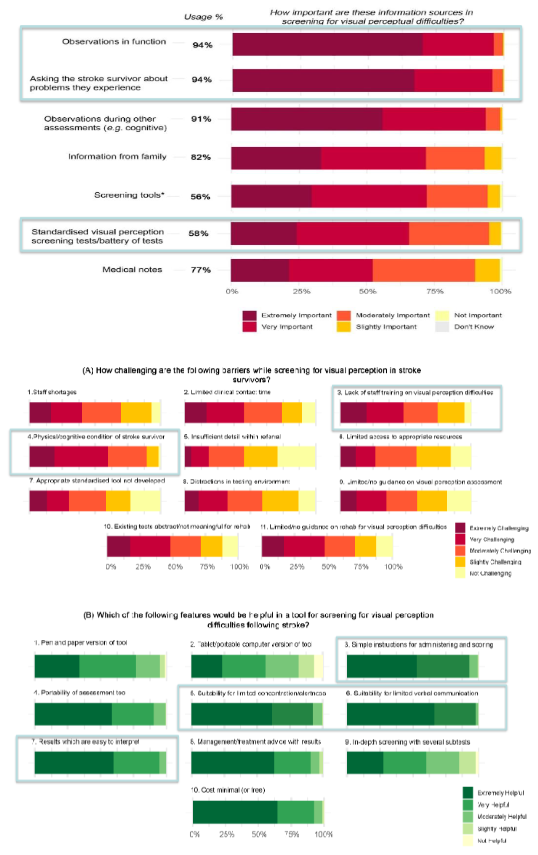
Vancleef et al. (2020), Colwell et al. (2021) - diagnosis of perceptual issues
Multimethod:
Semi-structured interviews (N=25)
UK-wide survey (N=214)
Participants:
UK-based orthoptists and occupational therapists involved in the assessment of visual perceptual problems after stroke
Poor understanding of visual perception
52% of sensory vision problems incorrectly categorised as visual perceptual problems.
91% consider visual neglect as a visual perceptual problem.
94% of clinicians rely on subjective methods.
Visual Object and Space Perception Battery (VOSP) (Warrington & James, 1991)
Initial screening task (shape detection)
8 tests designed to assess specific aspects of object or space perception.
Tasks involve other cognitive skills minimally.
Standardisation data available for each test.
But, age-related differences in performance (Bonello et al., 1997) - people under 70 perform better, not appropriate for older adult populations
Do need to have the specific test materials.
Neglect
The inability to attend to or respond to stimuli in a part (variable) of the visual field.
Neglect can occur in various modalities
The most extensive investigations typically concern visuospatial neglect.
Neglect is not a disorder of low-level perception.
Many patients with neglect also have non-spatial deficits in attention (e.g., sustained attention) - might need to think of quick assessments.
Visuospatial neglect - Heilman et al., 1994
An abnormality in the ability to orient attention towards, or respond to, the contralesional side of space which is not attributable to a primary sensory or motor deficit.
Rees et al., 2000 - neglect
Objects in neglected field still activate V1
Riddoch & Humphreys, 1983 - neglect
Stimuli presented to neglected side can often be detected if attention directed there first.
Kaplan et al., 1991 - neglect
Degree of clutter in visual environment related to extent of neglect.
The border between neglected space and non-neglected space is not absolute – there is a variable gradient.
Halligan & Marshall, 1992 - heterogeneity of behavioural impairments
Some patients may demonstrate impairments in line bisection but not cancellation and vice-versa.
Neglect as a syndrome rather than an indiv cond.
Heilman & Valenstein (1985) - heterogeneity of brain regions
Heterogeneity of brain regions implicated, and the extent of lesions varies extensively
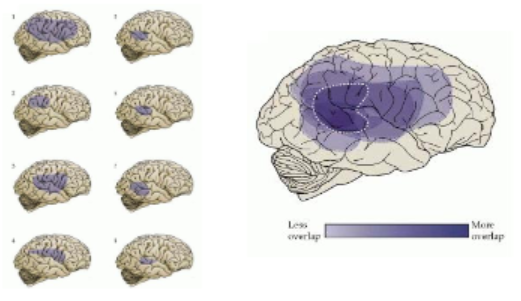
He et al., 2007 - neglect
Functional connectivity measured using fMRI revealed that disconnection of white matter tracts connecting frontal and parietal cortices was associated with more severe neglect.
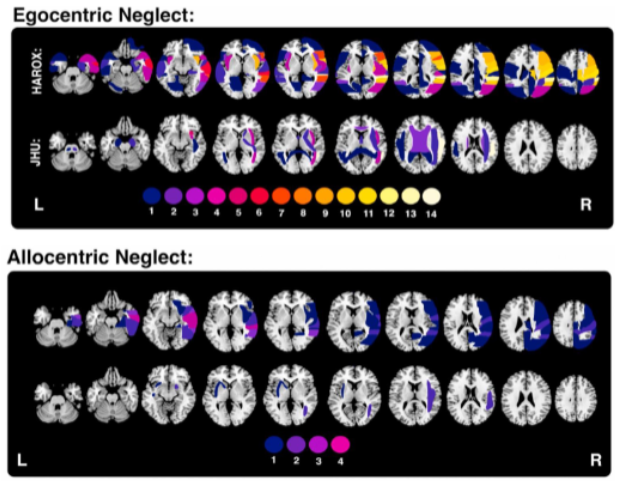
Moore et al. (2023) - egocentric vs. allocentric neglect
Cutting, 1978; Karatas et al., 2023 - anosognosia
Anosognosia in up to 81% of patients and is associated with neglect severity.
Ott et al., 2023 - delirium and neglect
Higher rates of delirium (acute decline in cog function) in right hemisphere stroke patients with neglect compared to those without neglect.
Tests of neglect

Bowen et al., 1999 - neglect assessment
There is no gold standard for neglect assessment
Williams et al. (2021) - neglect assessment
Identified 292 tools
Possible for two indivs to be diag with neglect with no overlapping symptoms.
The number of neglect assessment tools and the heterogeneity of patients makes it difficult for health care professionals to select the most appropriate tool.
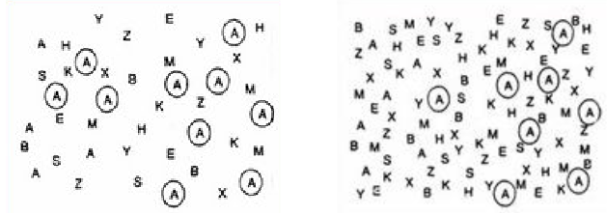
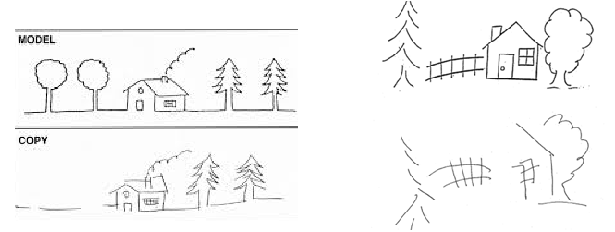
Behavioral Inattention Test (BIT) (Wilson, Cockburn, & Halligan, 1987) - subtests
Conventional (BITC)
Line crossing, letter cancellation, star cancellation, figure and shape copying, line bisection, representational drawing.
Behavioural (BITB)
Picture scanning, phone dialling, menu reading, article reading, telling and setting the time, coin sorting, address and sentence copying, map navigation, and card sorting.
Can tell if they fail to identify something due to their spatial location.
Behavioral Inattention Test (BIT) (Wilson, Cockburn, & Halligan, 1987) - overview
Maximum score for the BIT is 227 (BITC: 146; BITB: 81).
Cut off scores: 196/227; 129/146; 67/81
Available in English and Chinese
Behavioral Inattention Test (BIT) (Wilson, Cockburn, & Halligan, 1987) - considerations when conducting assessment
Position of materials, make sure they're centralised
Instructions and cues - no bias
How to end the task
Behavioral Inattention Test (BIT) (Wilson, Cockburn, & Halligan, 1987) - advantages
Excellent test-retest reliability of BITB (r = 0.97) and BITC (r = 0.89), and inter-rater reliability of both (r = 0.99) (Halligan et al., 1991)
Convergent validity: excellent correlation with the Barthel Index (r = 0.64) (Cassidy et al., 1999)
Manual easy to read and administer
Simulates daily life activities
Behavioral Inattention Test (BIT) (Wilson, Cockburn, & Halligan, 1987) - disadvantages
Materials are extremely dated - e.g., using pictures of ‘70s-’80s bedrooms
Not suitable for people with communication impairments
Costs
Assessment of peripersonal, egocentric neglect only - not testing for an allocentric form of neglect
Karnath et al., 2011 - neglectt
Research suggests that neglect improves within the first few months
Andres et al., 2019 - neglect
Neglect may not improve within the first few months - could be lack of sensitivity of tests and practice effects, or coming up with compensatory strategies over time, so patients are doing better on simplistic tasks.
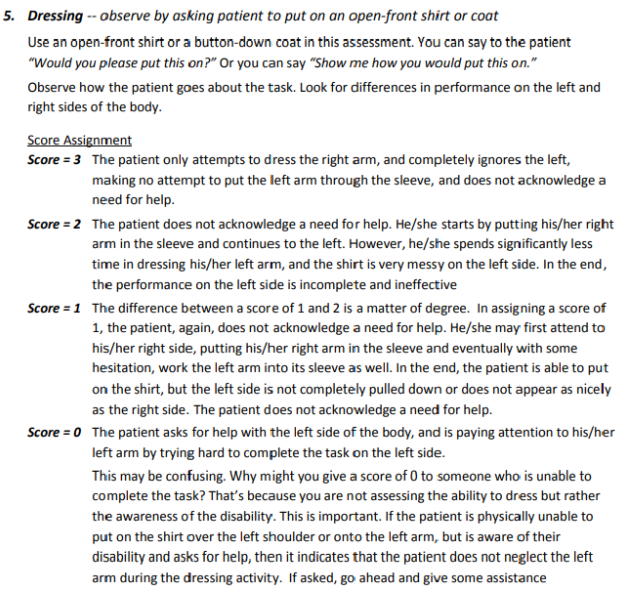
Catherine Bergego Scale (CBS) (Bergego et al., 1995)
Indicate severity of neglect on 10 different activities

Catherine Bergego Scale (CBS) (Bergego et al., 1995) - advantages
Adequate to excellent correlations between items (r = 0.48 – 0.73) (Azouvi et al., 2003)
Excellent inter-rater reliability (Bergego et al., 1995)
Adequate to excellent correlations between CBS and other conventional assessments for neglect (r = 0.49 – 0.77) (Azouvi et al., 2002)
No formal training
Can be assessed in hospitals/community settings + equipment generally household items
Representative of daily life (or designed to be)
Catherine Bergego Scale (CBS) (Bergego et al., 1995) - disadvantages
Not suitable for people with movement impairments - but scoring can be adjusted to take out items, but will have to consider if that's the neglect or another reason - brings subjectivity back in
General principles (e.g., suggestions for scoring) will be different - what does ineffective and incomplete describe?
Kessler Foundation Neglect Assessment Process (KF-NAP) (Chen et al., 2012)
Additional instructions for administering the Catherine Bergego Scale (CBS) more reliably.
General principles (e.g., no lateralised cue; suggestions for scoring)
Delivery of CBS in more standardised way
Kessler Foundation Neglect Assessment Process (KF-NAP) (Chen et al., 2012) - evaluation
Measuring what they can do in the moment, but improves examiner variability to an extent/
Possible that very explicit tasks differently affect performance relative to patient initiating the actions themselves - not spontaneous every day behaviour.
Explicitness will make patients feel like they're being assessed and alter performance - might be better with naturalistic observations.
Important to observe patients regularly - more likely to pick up on behavioural variation + noting spontaneous behaviour.