Week 11 Pre-work
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
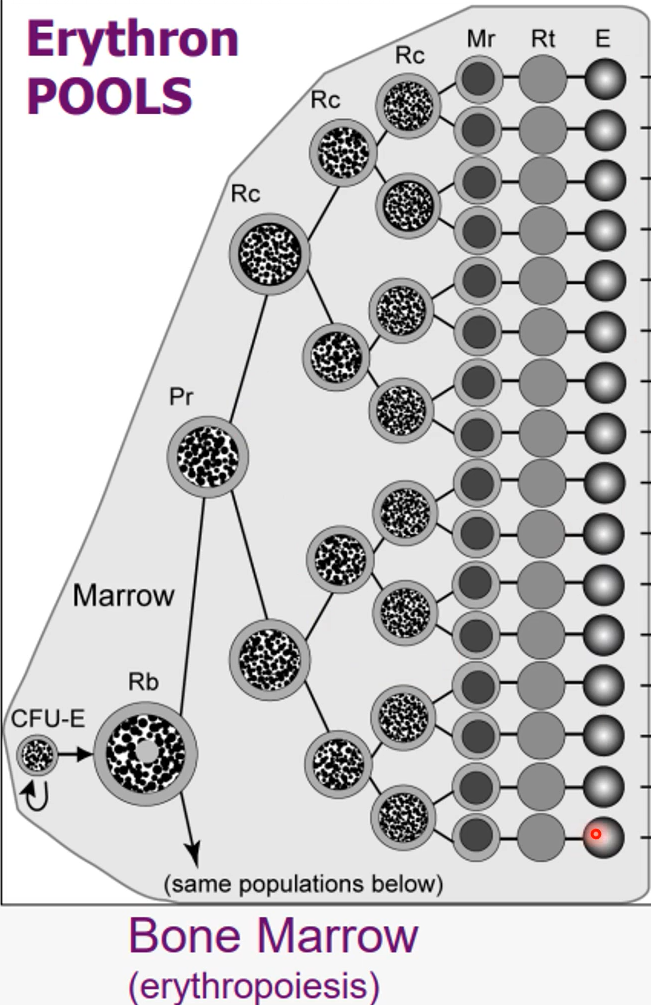
Bone marrow
become mature erythrocytes
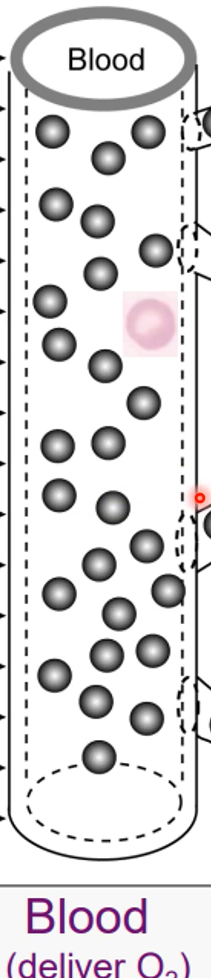
Blood
deliver oxygen to tissues
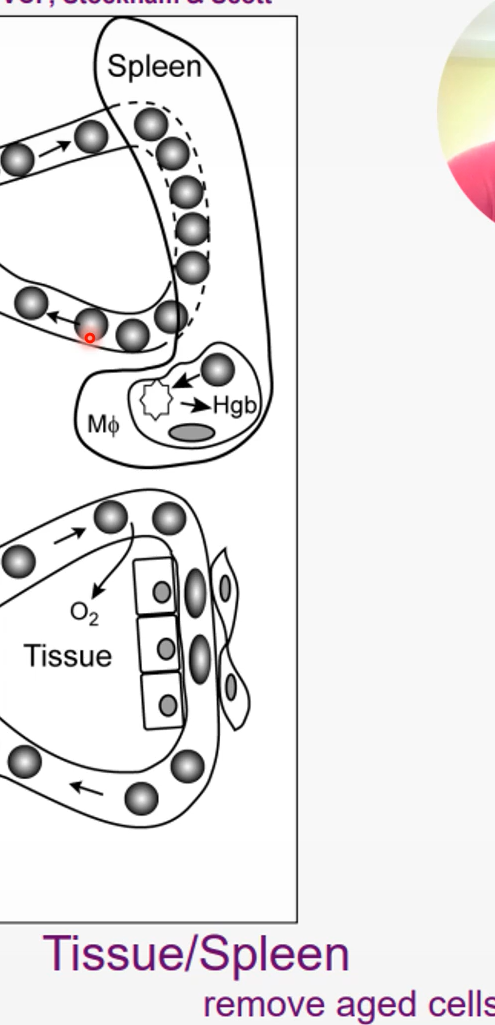
Spleen
reserve for RBCs
macrophages in the spleen destroy old RBCs
Iron kinetics in healthy animals
1) intestine absorption;
2) transported in plasma bound to transferrin; apotransferrin + Fe → transferrin
Fe binds…
ferritin in rubricyte then incorporated into hemoglobin
Iron is stored where?
stored in marrow, spleen, and liver as hemosiderin, ferritin
Hypoferremia
low iron in serum or plasma
Hypoferritinemia
low ferritin in serum or plasma
Two important important conditions that lead to hypothermia
iron deficiency and inflammation
transferrin: negative acute phase protein
inflammatory cytokines cause liver to decrease production of transferrin
hypoferremia: persistent low-grade blood loss(intestine or skin)
loss of RBCs with iron rich hemoglobin →
stored iron used to produce more hemoglobin for RBCs →
eventually, depleted total body iron content →
decrease in stainable iron in marrow/spleen
Hypoferremia: persistent inflammatory disease
Cytokines(IL-6) promotes synthesis of hepcidin →
hepcidin internalizes iron in macrophages membranes →
iron stays in macrophages →
increase in stainable iron in marrow/spleen
Erythrocyte Analytes of the Complete Blood Count (CBC)
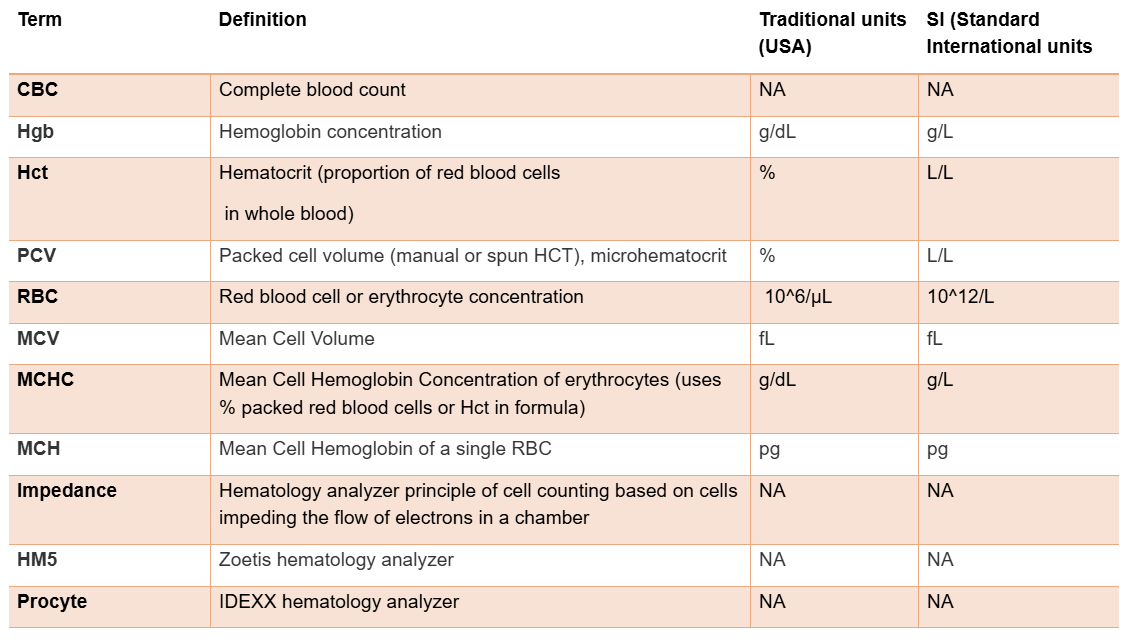
PVC, Hct, Hgb, and RBC all measure?
RBC mass
decreased RBC mass= anemia
Hematocrit
Proportion of RBCs per blood volume
Hemoglobin
reflects oxygen carrying capacity of blood
Hgb x 3 = Hct
MCHC(mean cell hemoglobin concentration) =
Hgb x 100 / Hct
Platelet or thrombocyte:
Cellular fragment of a megakaryocyte that participates in the first hemostasis step
Fibrin:
Is the active form of factor I; it is a sticky, threadlike protein that “glues” together the cells and clotting factors in a blood clot
Thrombopoietin:
A liver protein that is the primary regulator of megakaryocyte development and platelet production
endothelial cells have a dynamic interaction with?
Platelets
they regulate the activation of platelets in both intact and injured vessel walls
An intact endothelium prevents?
the adhesion of platelets through the release of nitric oxide and prostacyclin
Following a vessel injury, activated endothelial cells will release what molecules?
vWF, Tissue plasminogen activator(tPA), and endothelin-1 and express a variety of surface receptors that increase platelet cell adhesion
Activated endothelial cells favor…
the formation of thrombin, which stimulate blood clotting
Platelets will release a variety of molecules…
Serotonin and thromboxane A2 and platelet plug formation(Prothrombotic molecules ADP and thromboxane A2)
After activation platelets bind to
exposed factors in the injury site, vWF and collagen
vWF(GP1B) receptors
receptors on platelets that bind to the vWF which have bound to the exposed collagen molecules and platelets are activated
Alpha granules(in platelets)
release additional vWF and platelet derived growth factor for clotting
Dense granules(in platelets)
release ADP(binds to P2y12) and thromboxane(binds to TP) which bind to other platelets
Fibrinogen
linking molecule which adheres to other platelets and makes platelet aggregation
The enzymes in the 3 pathways are which by which cofactors?
Ca, phospholipids, and Factor V
Fibrinolysis
process that involves the activation of proteolytic enzymes which aims to degrade the fibrin clot
Process of fibrinolysis
endothelial cells release tissue plasminogen activator(tPA) →
tPA activates plasminogen →
plasmin degrades fibrin, and the clot dissolves
factor Xa
activates thrombin to recruit more platelets
Thrombocytopenia refers to a
platelet concentration below the lower reference interval, in this case 150,000
most common cause of bleeding
Inaccurate platelet count due to cell size
large platelets; miscounted as RBCs or excluded
Pseudothrombocytopenia
Due to platelet clumps/clots
large platelets(cats) and cavaliers and norfolk terriers
Platelet graphs
Ski slope is healthy
bumpy when clumping
upward trend: large platelets
Adequate platelets
About 1 platelet per 30 RBCs, 8-10/hpf in a healthy dog or cat
Pathogenesis of thrombocytopenia
1) decreased production
2) decreased survival(increased survival and consumption)
3) abnormal distribution(sequestration)
4) Idiopathic or multifactorial(decreased production and survival)
Tests for intrinsic and common pathway
Activated clotting time(ACT), Partial thromboplastin time(PTT)
Tests for extrinsic and common pathway
prothrombin time(OSPT,PT)
Activated clotting time(ACT) test
screening test, tests most of the coagulation pathway
activates the intrinsic and the common pathway
normal dogs <90s, cats <165s
For ACT severe thrombocytopenia <10,000/ul can cause?
mild prolongation of ACT
APTT test
evaluates intrinsic and common pathways
more sensitive than ACT
ran using plasma rather than whole blood
Process of APTT test
reagent and calcium → added to plasma
Goal of the three pathways
Thrombin(II) → fibrinogen(I) → fibrin
PT/OSPT test
similar to PTT
Key points for PTT/PT
if the citrate tube is underfilled → excess anticoagulant and artificial prolongation of PT/PTT
FDPs are
any of the many protein fragments that can be produced when either fibrinogen or fibrin is cleaved by plasmin
D-dimers are
a specific sub-set of FDPs
can only be formed by the breakdown of cross-linked fibrin and not fibrinogen
FDPs/D-dimers are a marker for
thrombotic disease
Increased concentrations are not 100% specific for thrombotic disease but…
the higher the concentration the more likely its due to thrombosis
Disseminated intravascular coagulation(DIC)
accelerated clotting within blood vessels →
increased consumption of platelets and clotting factors →
uncontrollable bleeding
D-dimer general concentrations
500-1000 are seen with trauma, post-sx, liver disease
1000-2000 and above are strongly specific for thromboembolism