Maternal Complications in Pregnancy (Lecture 20a&b)
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
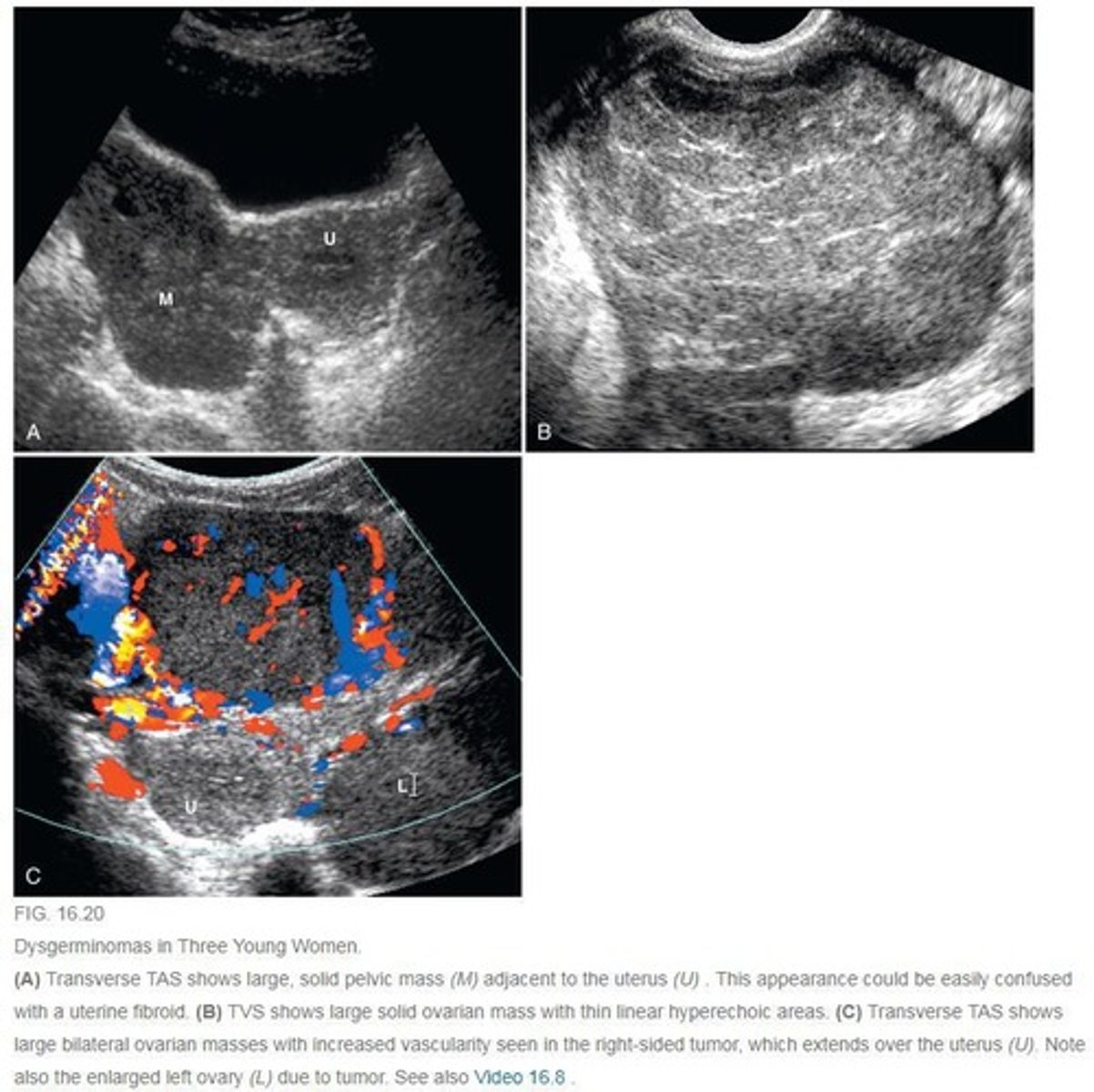
What neoplasms are m/c seen in pregnancy? (HINT: 3)
- Mature cystic teratoma (benign)
- Dysgerminomas (malignant)
- Serous cystadenoma
TRUE or FALSE: A corpus luteal cyst can be seen in early pregnancy.
TRUE: CL cyst may be seen in early pregnancy but should resolve in about 3 months
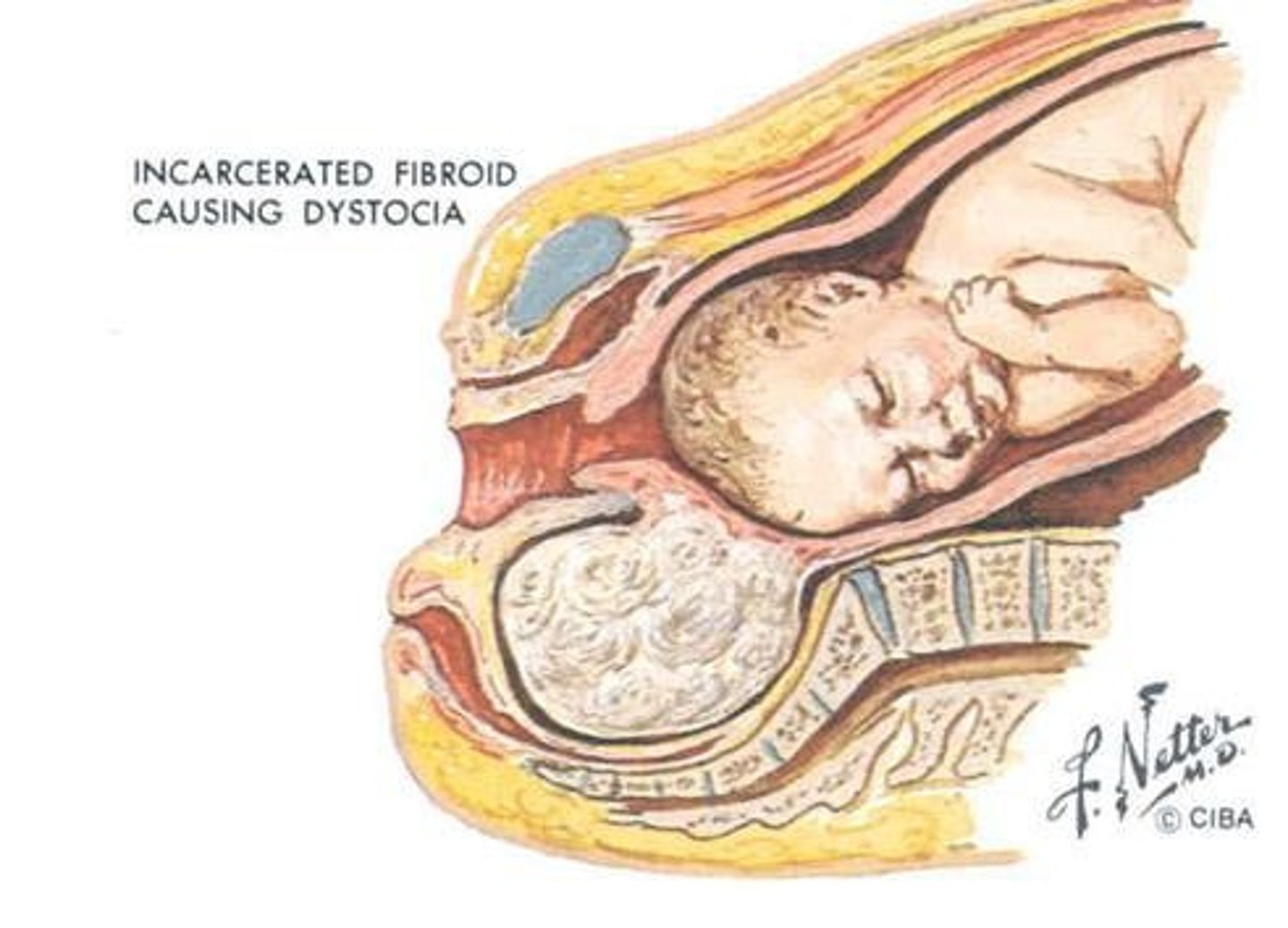
What are the complications of fibroids in pregnancy?
- Dystocia: difficult birth from fibroid compressing lower uterine segment
- Cystic degeneration of fibroid: could cause pain (inc estrogen from preg = inc size of fibroid)
What are teratogens? Name the 4 m/c and their effect on the mother/fetus
Substance causing fetal development issues or birth defects
- Smoking: maternal hypertension, IUGR fetus from dec. placental circulation
- Alcohol: premature birth, fetal alcohol syndrome, hydrocephalus, microcephaly, irreversible CNS damage
- X-rays: dec. development of fetus
- Drugs (DES, thalidomide): cancer later in life for fetus, birth defects (renal agenesis, club foot)
What does "TORCH" stand for?
Group of infections
T - Toxoplasmosis
O - other (syphylis, COVID-19, chickenpox, parovirus, Zika,)
R - rubella
C - cytomegalovirus (CMV): subset of herpes
H - herpes
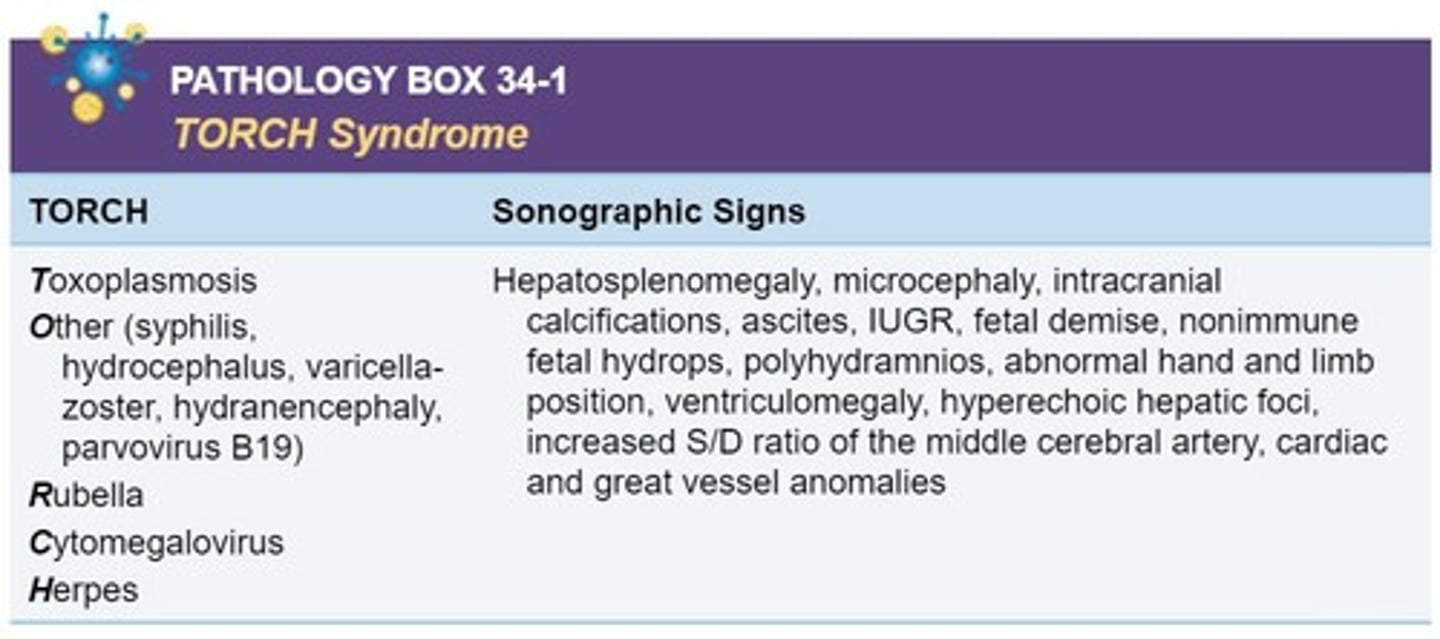
What is toxoplasmosis? What are the outcomes of the infection in the first vs. third trimester? What is their CP/SF?
- Parasitic infection linked to cat feces and undercooked pork/lamb
- 1st trim: less likely to be transmitted (less vasc connections to mother) but more severe effects if it does (organogensis has not occur/is occuring)
- 3rd trim: more likely to transmit but less severe outcomes
- CP/SF: CNS anomalies (hydrocphalus, microcephaly), ascites, intracranial calcifications hepatosplenomegaly
TRUE or FALSE: Varicella-zoster is only exposed to the fetus if the mother is infected in the first trimester.
FALSE: Varicella-zoster can be exposed to the fetus at ANY TIME during the pregnancy
What are the effects if varicella-zoster (chicken pox) is exposed to the fetus in the 1st vs 3rd trimester?
1st trimester: inc. risk of spontaneous abortion
3rd trimester: neonate has chickenpox at birth
What the SF for varicella-zoster?
- Microcephaly
- Echogenic foci in liver
What is syphilis? What are the effects with early, late, and neonate exposure?
Congenital infection linked to STI
- Early: spontaneous abortion
- Late: still births and neonatal mortality
- Neonate: hepatosplenomegaly, hyperbilirubinemia, hemolysis, generalized lymphadenopathy
Name 2 complications associated with parvovirus B19. Name 2 sonographic features. When do these complications usually occur?
Complications:
- Fetal demise
- Fetal anemia (measure PSV of MCA)
- Neurologic anomalies
- Nonimmune hydrops
(most complications occur w/i 12 wks of infection)
SF:
- pleural/pericardial effusion
- ascites
- dilated heart
How is zika virus transmitted? What is the severity of symptoms for the mother and fetus?
- Transmitted by mosquito bites
- Mother: mild and manageable symptoms
- Passed onto fetus =
microcephaly, nervous system abnormalities
What are the pregnancy risks associated with COVID-19? (HINT: 3)
- Preterm birth
- Pregnancy loss
- Possibly IUGR
What are symptoms of rubella in the mother and fetus?
Mother = Fine pink rash
Fetus = IGUR, cardiovascular abn, microcephaly, microphthalmos, hepatosplenomegaly, osteopathy
What is cytomegalovirus (CMV)? How is it transmitted in mother and fetus? What are the SF?
- Herpes virus transmitted thru blood, body fluids (STI)
- Infections reach fetus thru cx/placenta or fetal contact w/ birth canal during vaginal delivery
- M/c congenital cause of infection
SF: CNS anomalies, ascites, splenomegaly, IUGR, hydrocephaly, polyhydramnios
What is the m/c congenital cause of infection?
CMV (cytomegalovirus)
What are the complications of herpes infection in the first half of pregnancy? What is CP/SF for fetuses w/ this infection? What is the outcome for fetuses?
- First half of preg: inc. in spontaneous abortions and stillbirths
- Associated w/ microcephaly, hydranencephaly, intracranial calcifications, microphthalmia, hepatosplenomegaly
- Need a c-section at time of delivery, w/ majority of infants born prematurely
TRUE or FALSE: The presence of rubella in the maternal genital tract at time of delivery indicates the need for a c-section.
FALSE: The presence of HERPES in the maternal genital tract at time of delivery indicates the need for a c-section.
A patient comes is scanned and the sonographer sees brain and liver calcifications. What is a plausible differential diagnosis for this patient?
TORCH infections
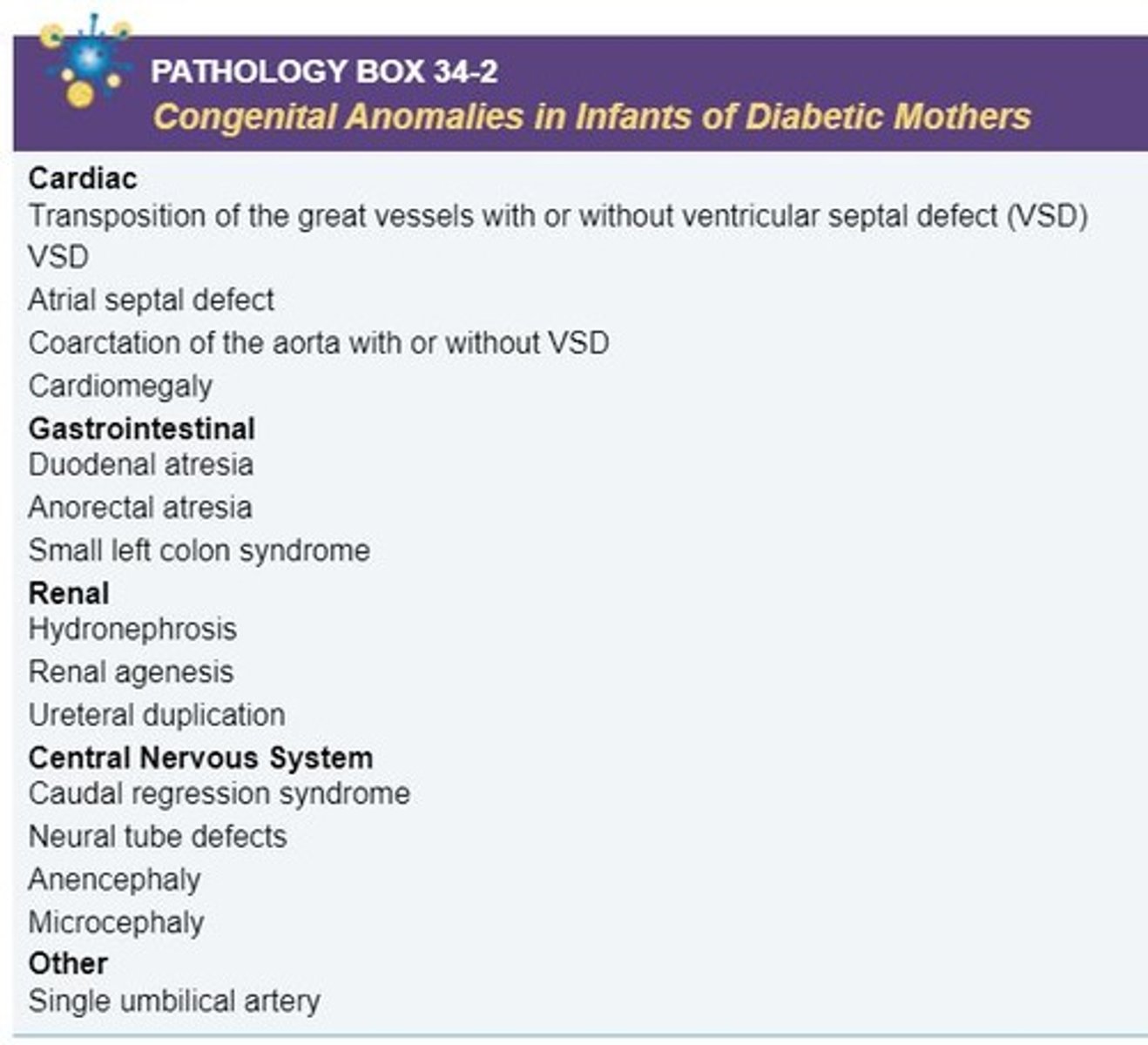
Why do fetuses have increased risk of anomalies and spontaneous abortion when a mother has diabetes?
High blood sugar levels result in disruption of embryonic organogensis
What is the difference between type 1 and 2 diabetes?
Type 1: insulin-dependent (previously juvenile-onset)
Type 2: noninsulin dependent (adult onset)
What is the White's classification of diabetes? What are the fetal complications associated with each type?
Types:
A - gestational diabetes
B - Diabetic before pregnancy (diet controlled)
C - Diet controlled, now needs insulin (may revert back after preg or continue to use insulin)
D - Type 1 diabetes
E - Type 1 diabetes + hypertension + vascular disease
Complications:
- Type A,B,C = macrosomic fetuses
- Type C,D,E = IUGR fetuses
Name 3 congenital anomalies that can occur with maternal diabetes.
- 2VC
- Anencephaly
- Club foot
- Skin thickening
- Enlarged eye orbits
Name 2 obstetric complications of diabetes.
- Polyhydramnios
- Preeclampsia
- Placentomegaly/placentomalacia
- Spontaneous abortion
TRUE or FALSE: Type 1 diabetes is associated with placentomalacia.
TRUE:
Type 1 = placentomalacia
Type 2 = placentomegaly
What are the 3 diabetic emergencies?
- Hypoglycemia
- Ketoacidosis
- Coma
What is supine hypotensive syndrome? What is the CP? What is the tx? What complication may occur?
- Low blood pressure from pressure of pregnancy pushing on vena cava and stopping blood flow to the heart, usually occurs from lying flat for extended time
- CP: restlessness, feeling ill, faint, nausea
- Tx: Turn pt and have them breathe deeply
- Complication: marginal placental abruption
What is essential hypertension?
High blood pressure before or after pregnancy
What is pregnancy-induced hypertension (PIH)
Hypertension occurring during pregnancy and disappears after parturition (giving birth)
What is chronic hypertension? What 2 conditions does this increase the risk for? What are the SF?
- High blood pressure before pregnancy or 20 weeks gestation
- Inc. risk of preeclampsia and placental abruption
SF:
- premature aging of placenta (calcifications)
- thin placenta
- placental infarcts
- IUGR
What is preeclampsia (toxemia)? What is the pt population? When does it usually occur?
- Preeclampsia is characterized by 3 things: hypertension, proteinuria, and edema of hands, feet, and/or face
- Pt population: older multipara women or young pts w/ 1st preg
- Often seen in 3rd trim
What are SF for preeclampsia?
- IUGR
- Oligohydramnios
- Placental infarcts
- Placental abruption
- Dec. placental volume
- Inc placental maturation
- Fetal demise
- Increased S/D ratio in umb. artery
What is the theory for the pathophysiology of preeclampsia?
- Spiral arterioles fail to convert to low resistance vessels + vasoconstriction = hypertension
- Dec renal flow = proteinuria
- Inc. capillary permeability, allowing fluid in interstitial spaces = edema
What is eclampsia?
- Preeclampsia + seizures (life threatening)
- Fetus will be delivered at this point b/c the condition is so life threatening
TRUE or FALSE: Once a patient has preeclampsia, the fetus is delivered.
FALSE: Once a patient has ECLAMPSIA, the fetus is delivered b/c the condition is so life threatening.
What is HELLP syndrome? When does it usually occur? What is the CP?
- A severe variant of preeclampsia (Hemolysis
Elevated Liver enzymes
Low Platelets)
- Usually occurs in 3rd trim
- CP: thrombocytopenia, abn liver function, nausea, vision problems, hypertension, proteinuria, excessive weight gain, generalized edema
What are the SF for HELLP syndrome?
- IUGR
- Dec fetal tone and movement
- Abn Doppler of UA (inc resistance = placental insufficiency)
What anomaly is associated with HELLP syndrome?
DIC - disseminated intravascular coagulopathy
What is DIC?
Disseminated intravascular coagulopathy
- fibrinogen (clotting factor) deficiency that results in clots occurring in the bloodstream and running out of clotting factors happening at the same time. This causes the patient to bleed and clot at the same time
What pregnancy complications are associated with DIC? (HINT: 3)
- Abruption
- Fetal demise
- Amniotic fluid embolism
What is urinary retention syndrome (mechanical renal obstruction, nephrotic syndrome, pyelocaliectasis)?
- Growing uterus w/ pregnancy causes pressure on ureters
- May lead to hydronephrosis (m/c right side)
What is an amniotic fluid embolism? When does it usually occur?
- Rare condition where amniotic fluid enters maternal bloodstream, causing an anaphylactoid rxn resulting in DIC (due to high phospholipids in amniotic fluid)
- M/c occurs during labour
What is pseudocyesis? What is the CP? Who is at risk for this condition (HINT: 3)
False pregnancy
- Somatic disorder where pt presents w/ outward signs of preg but not actually pregnant
- CP: enlarged abdo, amenorrhea, apparent fetal movements, hormonal changes
At risk population: lower socioeconomic status, limited access to healthcare, feel stress to conceive
What is lupus? Who is the pt population? Name 2 complications.
- Multisystem autoimmune disease attacking skin, joints, kidneys, nervous system, and mucous membranes
- Pt population: women in childbearing age
Complications:
- preeclampsia
- premature delivery
- maternal autoantibodies cause clots within placenta
- fetal loss
TRUE or FALSE: The best fetal outcome for pts with lupus are with planned pregnancies during remission.
TRUE
What is deep vein thrombosis? Why do pregnant pts have an increased risk to develop this condition (HINT: 3)? What complication may arise from a DVT?
- Blood clot in a deep vein, often in legs
- Inc risk in preg pts due to: venous stasis, pressure on pelvic vessels, hypercoaguability
- Complication: pulmonary embolism