ROSH Surgery BOOST exam
1/107
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
Preferred method for breast mass workup
Core needle biopsy
When to suspect breast abscess vs mastitis
When symptoms of mastitis do not respond to therapy after 48 hours.
- PE: Fluctuant, tender mass.
Hidradenitis Supportiva
- Clusters of abscesses, epidermoid cysts, sebaceous cysts, pilonidal cysts
- Affects apocrine sweat glands
- Axilla, under breasts, inner thigh, groin, buttox
- Triggered by sweating, hormonal changes related to menstrual cycle, friction.
- Persistent lesions lead to sinus tracts
Fecal Impaction
- Etiology: lack of fiber, opioids, IBS, Diabetes, Hypothyroidism'
- Abdominal pain and distention
- Chronic constipation
- Fecal incontinence/overflow diarrhea
- Can lead to rectal necrosis and ulcers
- Treat with manual disimpaction, stool softening, osmotic laxatives, surgery
Subarachnoid Hemorrhage
- Sudden headache, loss of consciousness, meningismus, N/V
- CT scan, LP (Xanthochromia), CT Angiography
- Supportive (airway), BP control with Nicardipine or labetalol, aneurysm repair, Nimodipine (within4 days), Target fluid resuscitation to euvolemia.
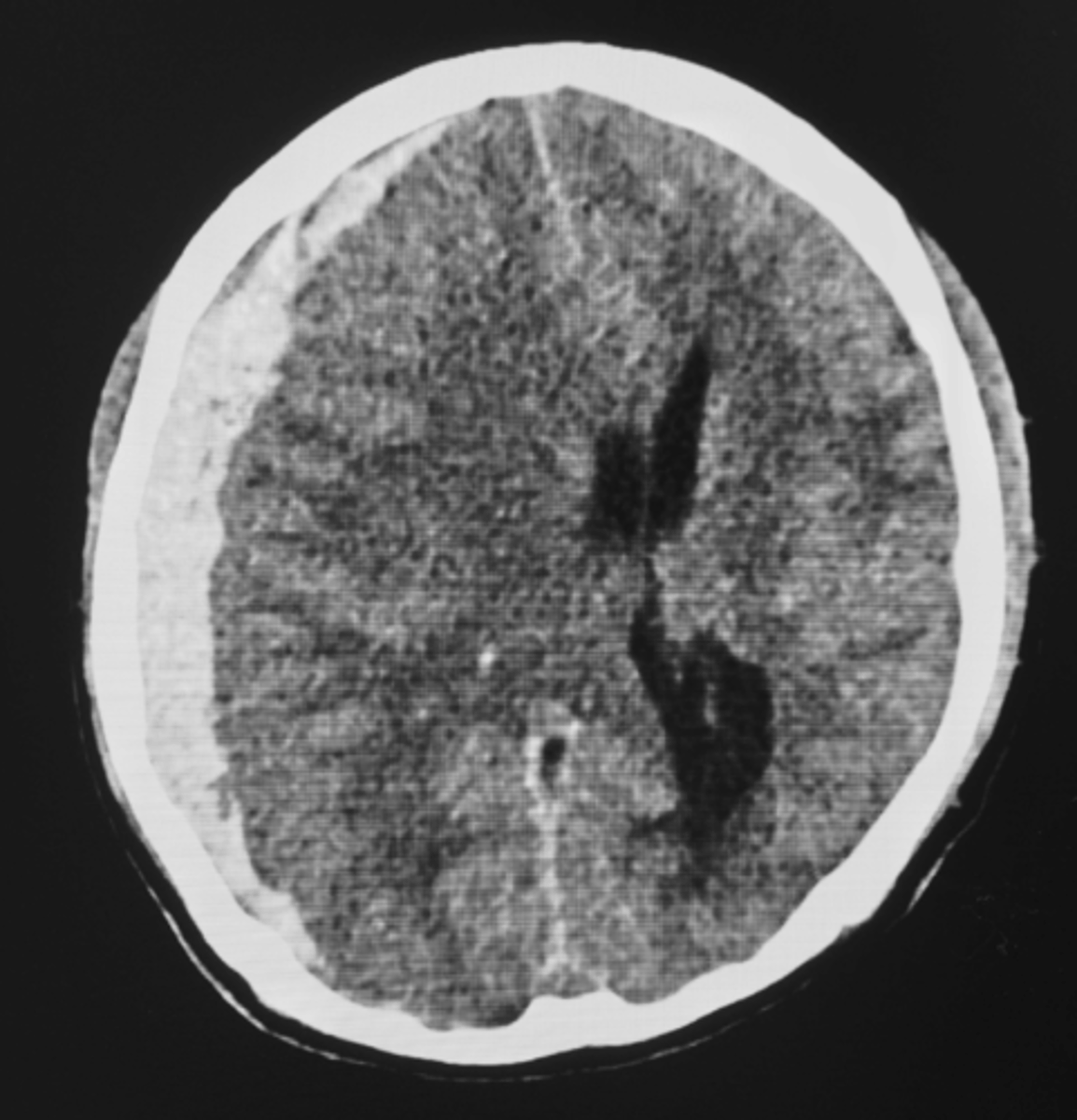
Subdermal Hematoma
- Between dura and arachnoid mater
- Tearing of bridging veins (alcohol use and older population)
- Acute or subacute neurological symptoms
- Neurosurgery consult, BP control, reverse anticoagulation
Post-Operative Voiding Dysfunction in Women General
- Defined in post-op period as retention >100 mL
Post-Operative Voiding Dysfunction in Women Detrusor Etiology
Failure to sense bladder:
- Anesthesia/narcotics
- Nerve injury: surgical or acute overdistension injury
- Missed cystotomy
Failure to contract:
- Anesthetic/narcotic
- Nerve injury
- Pre-existing voiding dysfunction
Post-Operative Voiding Dysfunction in Women Urethra/Pelvic Floor Etiology
Mechanical Obstruction
- Incontinence procedures
- Pelvic organ prolapse
- Urethral perforation/foreign body
- Constipation/pelvic mass
Functional Obstruction
- Failure to relax the pelvic floor
Esophageal Spasm
Dx: Esophageal manometry
Tx
1- CCB
1- TCA
2- Isosorbide-Sildenafil
2- Botulinum Toxin
Burn Infection Prophylaxis
- If NO MRSA: Ceftazidime plus Tobramycin
- If MRSA: Pip-Tazo plus Vanco
Acute Pancreatitis
PE: flank ecchymosis (turner sign), umbilical ecchymosis (Cullen sign)
Labs: Elevated lipase is most sensitive
- Causes: gallstones > alcohol, hypertriglyceridemia, drugs
- Complications: necrotizing pancreatitis, pancreatic pseudocyst
Primary Adrenal Insufficiency
- Adrenal gland: decreased cortisol/aldosterone = low glucose and high potassium
-> MC Cause is autoimmune destruction
- Clinical signs: Hypotension, shock, vomiting, diarrhea, abdominal pain, hypernatremia, hypoglycemia, hyperkalemia
- Dx: serum cortisol at 8 am, then cosyntropin stimulation test
- Tx: Hydrocortisone, supportive
Testing for primary vs secondary adrenal insufficiency
If a patient presents with signs or symptoms of adrenal insufficiency, the first step in evaluation is a basic metabolic panel and a serum cortisol level measured at 8 AM. If the cortisol level is low with a normal to high potassium level and low to normal sodium level, the next step is to perform a cosyntropin stimulation test. In this test, the basal ACTH level is measured before administering intravenous ACTH. Cortisol is measured again 30–60 minutes after administration. If the cortisol level is low and ACTH level is high,
Esophageal Varices Tx
Acutely
- Hemodynamic resuscitation
- Octeotride
- Banding, sclerotherapy
- Prophylactic antibiotics
Chronic
- Beta-Blockers
- Endoscopic Variceal ligation
- Definitive Treatment is Liver transplantation
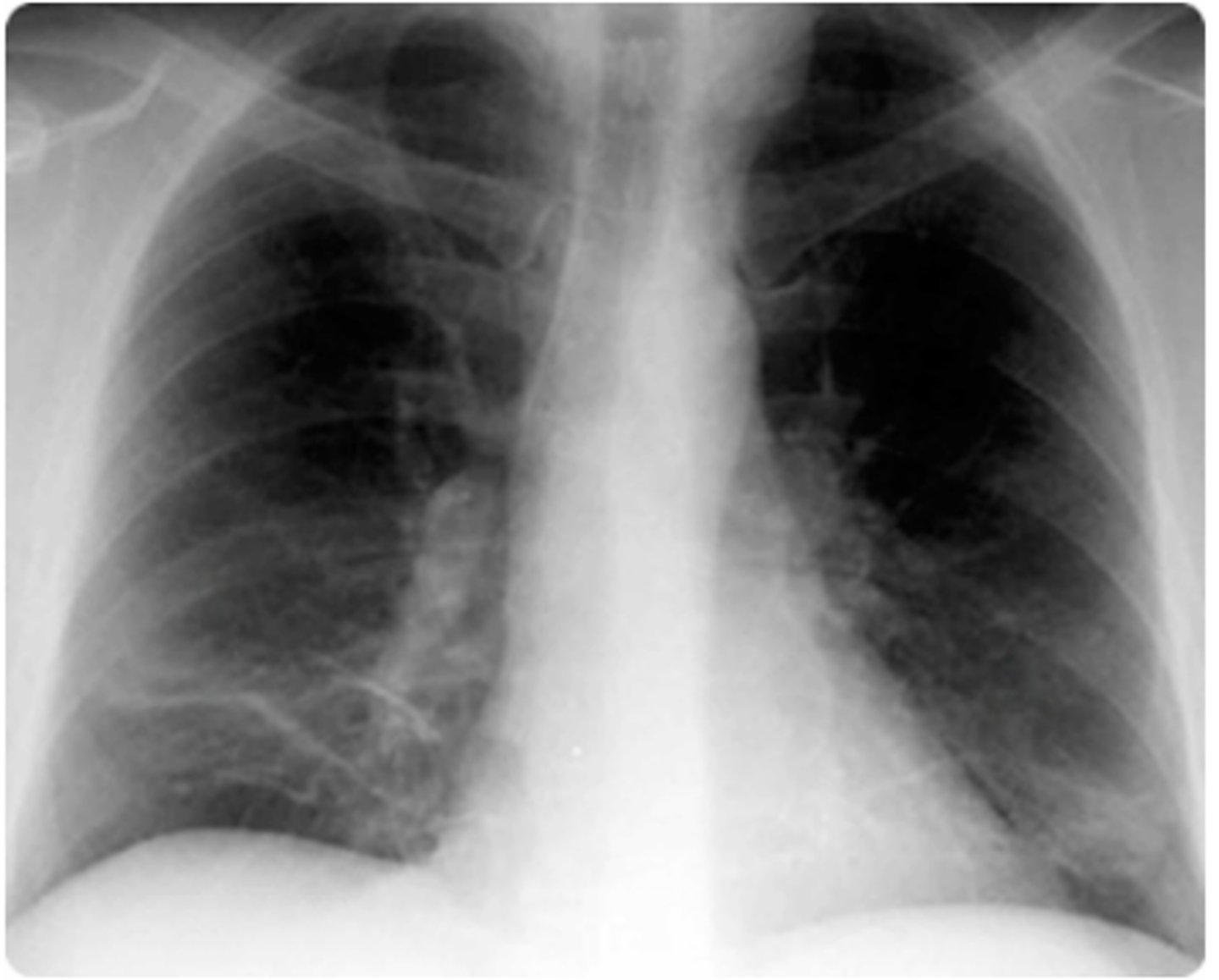
Lung Cancer Types
- Small Cell
-> Starts centrally
- Non-Small Cell
-> Adenocarcinoma: PERIPHERAL, MOST COMMON
-> Squamous Cell Carcinoma: Starts CENTRALLY, hypercalcemia
Mallory-Weiss Syndrome
RF: Alcohol Use, Hiatal Hernia, Bulimia
Dx: Suspected in patients with upper GI bleed and history of vomiting or retching
- Confirmed by upper endoscopy
PE: Acute-onset GI Bleeding (Hematemesis)
-> History of non-bloody emesis, retching, coughing prior to hematemesis
Management:
- Supportive
- Endoscopic therapy (active bleeding)
- Acid suppression (No active bleeding)
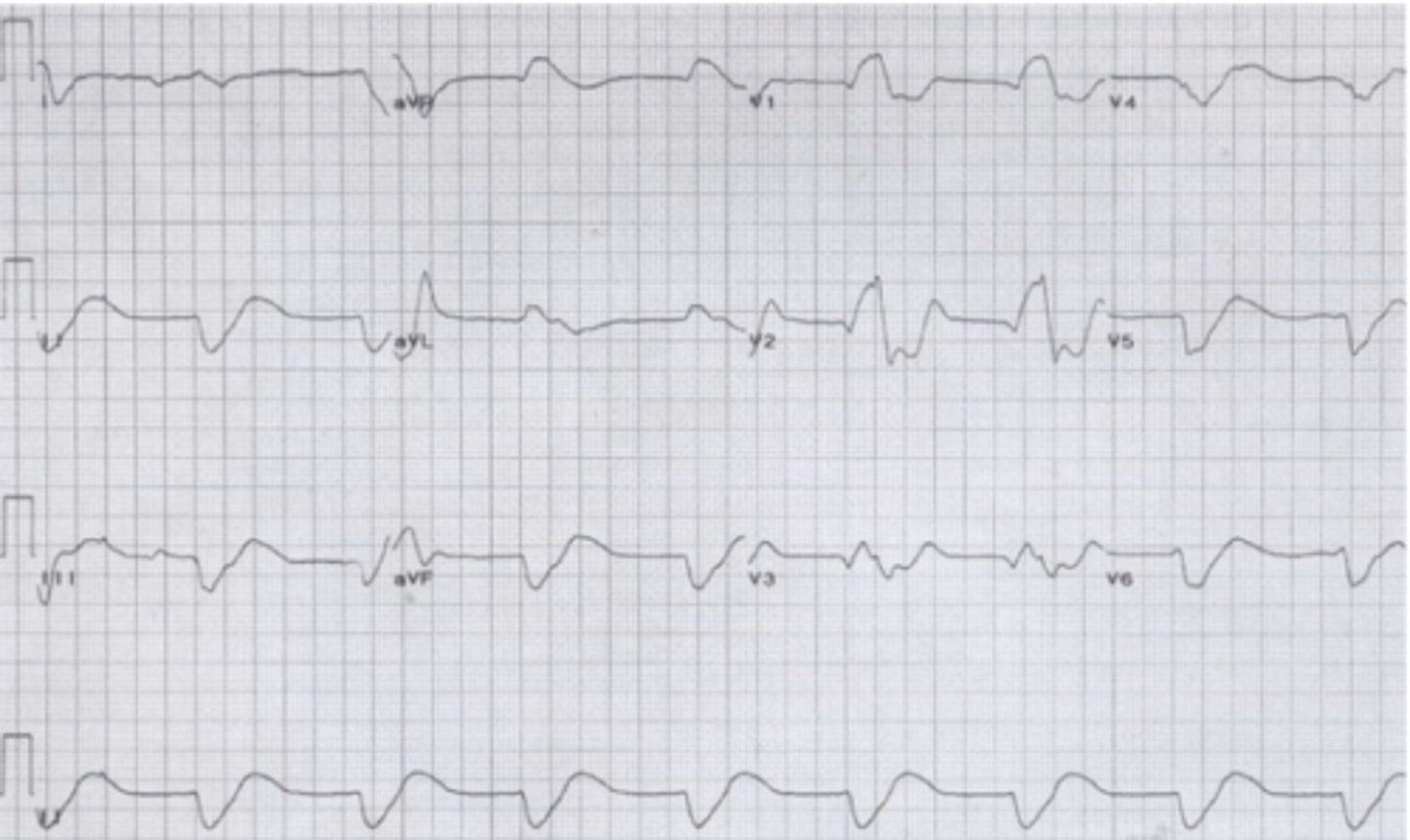
Indications for Dialysis
A: Acidosis (metabolic acidosis <7.1)
E: Electrolytes (hyperkalemia >6.5)
I: Ingestions (dialyzable drugs, such as salicylates, lithium, isopropanol, methanol, ethylene glycol)
O: Overload (Volume overload that does not respond to diuresis, especially with increased oxygen requirements)
U: Uremia (Elevated BUN with signs of uremia, such as bleeding, pericarditis, encephalopathy, neuropathy)
Vitamin B12 deficiency
- Chronic atrophic gastritis
- B12 deficiency
- Increased risk of gastric cancer
- increased risk of carcinoid tumor
- Anemia (Pernicious)
Clinical:
-> Symmetric peripheral neuropathy
-> Ataxia
-> Personality changes
-> Dementia
-> Glossitis, vaginal atrophy, malabsorption
Phyllodes Tumor of the Breast
- Leaf-Like
- Smooth, multinodular, well-defined, firm mass that is mobile and painless
- Management
-> Surgical resection
-> Radiation therapy
-> +/- Chemo
-> HRT not effective
Pancoast Tumor
- Shoulder and arm pain
- Horner syndrome
- Weakness and atrophy of the muscles of the hand
- Cough, hemoptysis, and dyspnea are uncommon
Tx
- Chemo, surgical resection
Anorectal fistula
Presentation: leakage of fecal material
Causes: Crohn disease, infection, malignancy
Dx: CT or MRI
Tx: Fistulectomy or seton placement
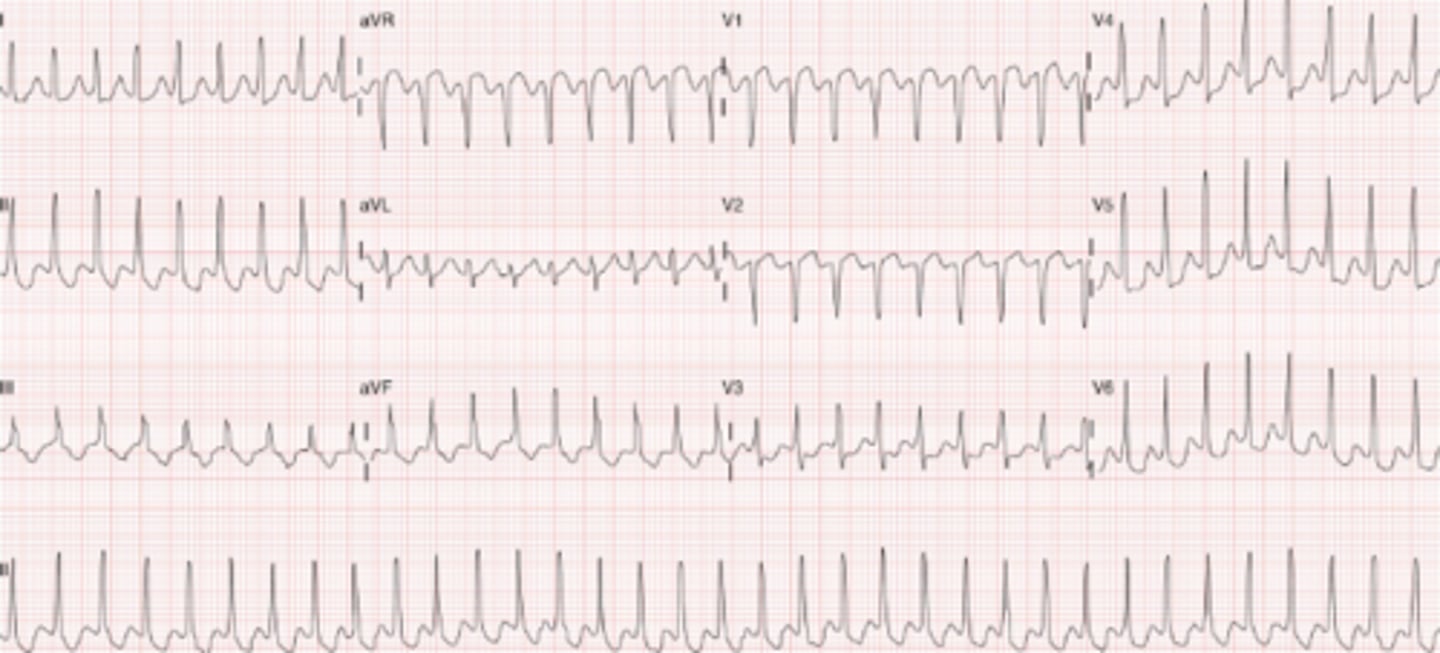
Supraventricular Tachycardia
- Regular, narrow complex tachycardia
Tx: Valsalva Maneuvers, Adenosine
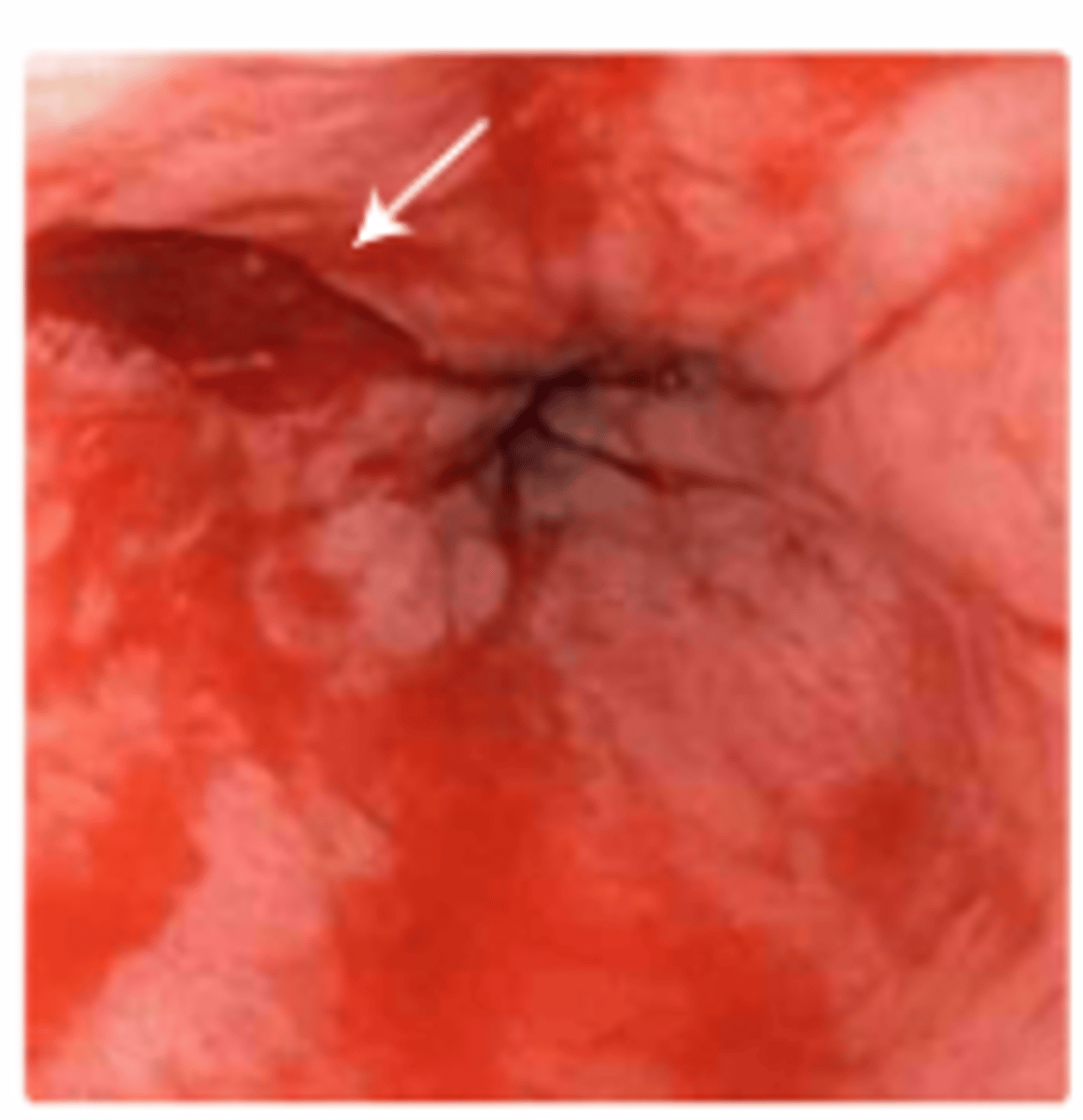
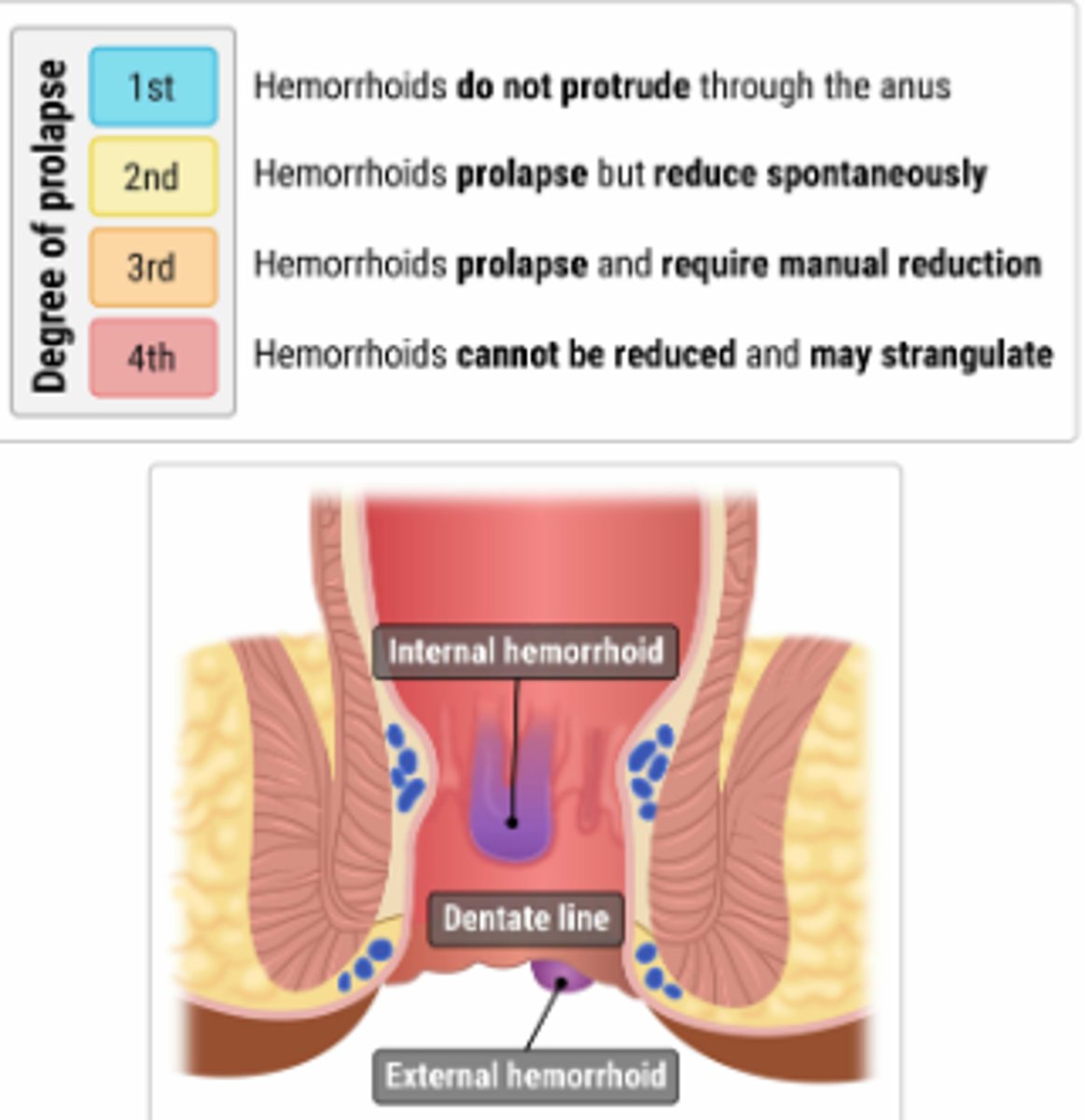
Hemorrhoids Classification
Post-op Wound Complications: Infecrtion
- Early wound infections are usually due to GAS or GBS
- Characterized by cellulitis and high fever
- Later infections are more likely to be staph aureus, E colie, proteus mirabilis, or cervicovaginal flora
- Nec fash is a rare but possible complication
Post-op Wound Complications: Hematoma and Seroma
- Collections of blood or serum
- Hematomas more common
- Usually result from failure of primary hemostasis or bleeding diathesis
- Both can cause incision to separate
- Dx clinically, confirm with CT or US
- Small can be managed expectantly, large ones should be drained
- Symptomatic hematomas should opened partially or completely under sterile conditions
- For suspected seroma, aspiration under sterile conditions mat be all that is required
Post-op Wound Complications: Wound Dehiscence
- Due to abdominal wall tension overcoming tissue or suture strength or knot security
- Can occur early or late in the post-operative period and involves a portion of the incision, or the entire incision
- When fascial disruption is suspected, wound exploration should be performed
- Complete fascial dehiscence is associated with mortality rate of 10% and is a surgical emergency.
Acute Cholangitis
- Fever, jaundice, and abdominal pain that develops as a result of stasis and infection in the biliary tract
- Management: Broad spectrum abx + endoscopic retrograde cholangiopancreatography (ERCP)
Hemorrhoids Treatment
For patients with grade I–III internal hemorrhoids who do not respond to conservative treatment, rubber band ligation is recommended. This is an office-based procedure in which small rubber bands are placed over the hemorrhoid using an anoscope. The banded hemorrhoid becomes necrotic and ischemic over 3–5 days, and healing occurs over the next several weeks. Surgical therapy is recommended for patients with grade IV hemorrhoids.
Empyema
- Analysis of the fluid will show exudative characteristics, such as a pleural fluid protein to serum protein ratio > 0.5, a pleural fluid lactate dehydrogenase (LDH) to serum LDH ratio > 0.6, or a pleural fluid LDH greater than two-thirds the normal upper limit for serum LDH. A high pleural fluid neutrophil count can distinguish empyema from chylothorax.
- Tx: Treat underlying cause, Abx, Thoracostomy
Acoustic Neuroma
- S/Sx: Hearing loss and tinnitus, Ataxia, Facial paralysis
- Treatment options for acoustic neuromas include observation, surgical removal, and radiation therapy. Observation is recommended for small, stable tumors or for patients who are asymptomatic. Surgical removal is the primary treatment option for most cases, and the timing of surgery is dependent on the size, symptoms, and age of the patient. Stereotactic radiation therapy is indicated for tumors measuring < 3 cm, patients who are poor surgical candidates, or patients who prefer to avoid surgery.
Sigmoid Volvus
Dx: Plain film x-ray (low specificity): U shaped, bent inner tube
-> Abd CT scan
-> Contrast enema
RF: Long-term care facility
-> Older age
-> Bed ridden
-> Chronic constipation
Clinical: Insidious onset of abdominal pain
-> Abdominal distention
-> Nausea, Vomiting, Constipation
Management
- Flexible sigmoidectomy (to reduce volvulus)
-> Surgery (to prevent recurrence)

First-Line Surgical Pain Med
- Acetaminophen, or NSAIDs
EKG of severe Hyperkalemia
Hypertrophic Cardiomyopathy
ECG
-> Left axis deviation
-> P wave abnormalities: left or bilateral atrial enlargement
-> Abnormal Q waves in inferior and lateral leads: septal depolarization of hypertrophied tissue (mimics inferior or lateral myocardial infarction)
Clinical
-> Exertional syncope
-> Dyspnea on exertion
Management
-> Beta blockers or CCB (non-dihydropyridines)
- AVOID POSITIVE INOTROPES AND NITRATES
Cholelithiasis
Gallstones: most commonly made of cholesterol
Risk factors: female sex, age 40–50 years, pregnancy, obesity, rapid weight loss
Sx: slowly resolving right upper quadrant pain that begins suddenly after eating a fatty or large meal
Dx: RUQ ultrasound
Tx: observation or cholecystectomy
Cholecystitis
Sx: colicky, steadily increasing RUQ or epigastric pain after eating fatty foods, fever
PE: Murphy sign, Boas sign (hyperaesthesia, increased or altered sensitivity, below the right scapula)
Diagnosis Initial: U/S Gold standard: HIDA
Most commonly caused by obstruction by a gallstone
Acalculous disease can occur when critically ill
Treatment is cholecystectomy, antibiotics, and percutaneous cholecystostomy tube when critically ill or if have comorbidities and do not improve on antibiotics
Causes of post-operative fever
Opioid Receptor Activations
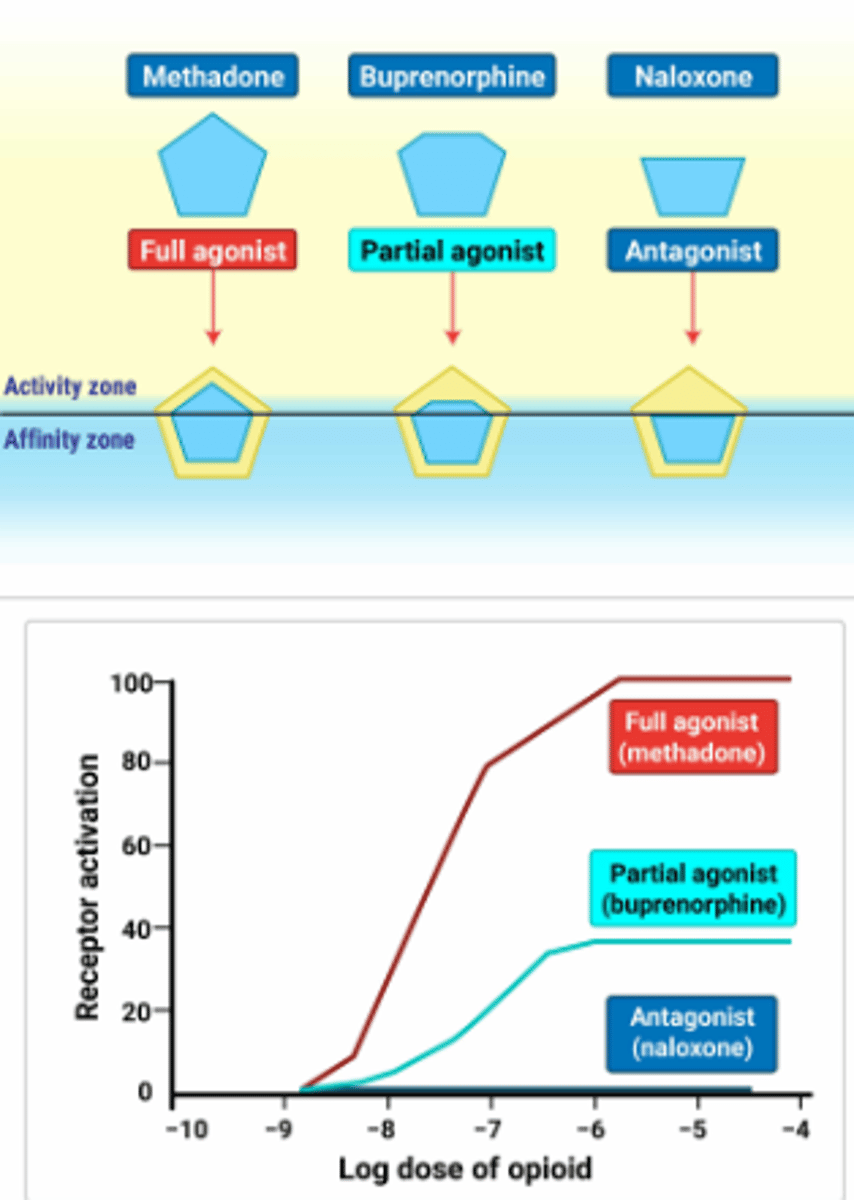
Buprenorphine
The unique pharmacokinetics of buprenorphine include a ceiling effect on its opioid agonist activity at higher doses, which further reduces the risk of overdose compared to full opioid agonists. This ceiling effect means that, above a certain dose, there will be no further increase in opioid effects such as euphoria or respiratory depression, enhancing the safety profile of buprenorphine for patients in treatment for OUD. Additionally, buprenorphine has a high affinity for and slow dissociation from mu-opioid receptors, which gives it the ability to displace other opioids that may be bound to these receptors for a longer period of time, thereby helping to prevent the effects of concurrent opioid use. This characteristic also contributes to buprenorphine’s effectiveness as a maintenance therapy for opioid dependence.
Buprenorphine is usually administered sublingually to optimize its bioavailability, and it is often combined with naloxone to deter intravenous misuse. Buprenorphine (or methadone) administration should be avoided until withdrawal symptoms appear.
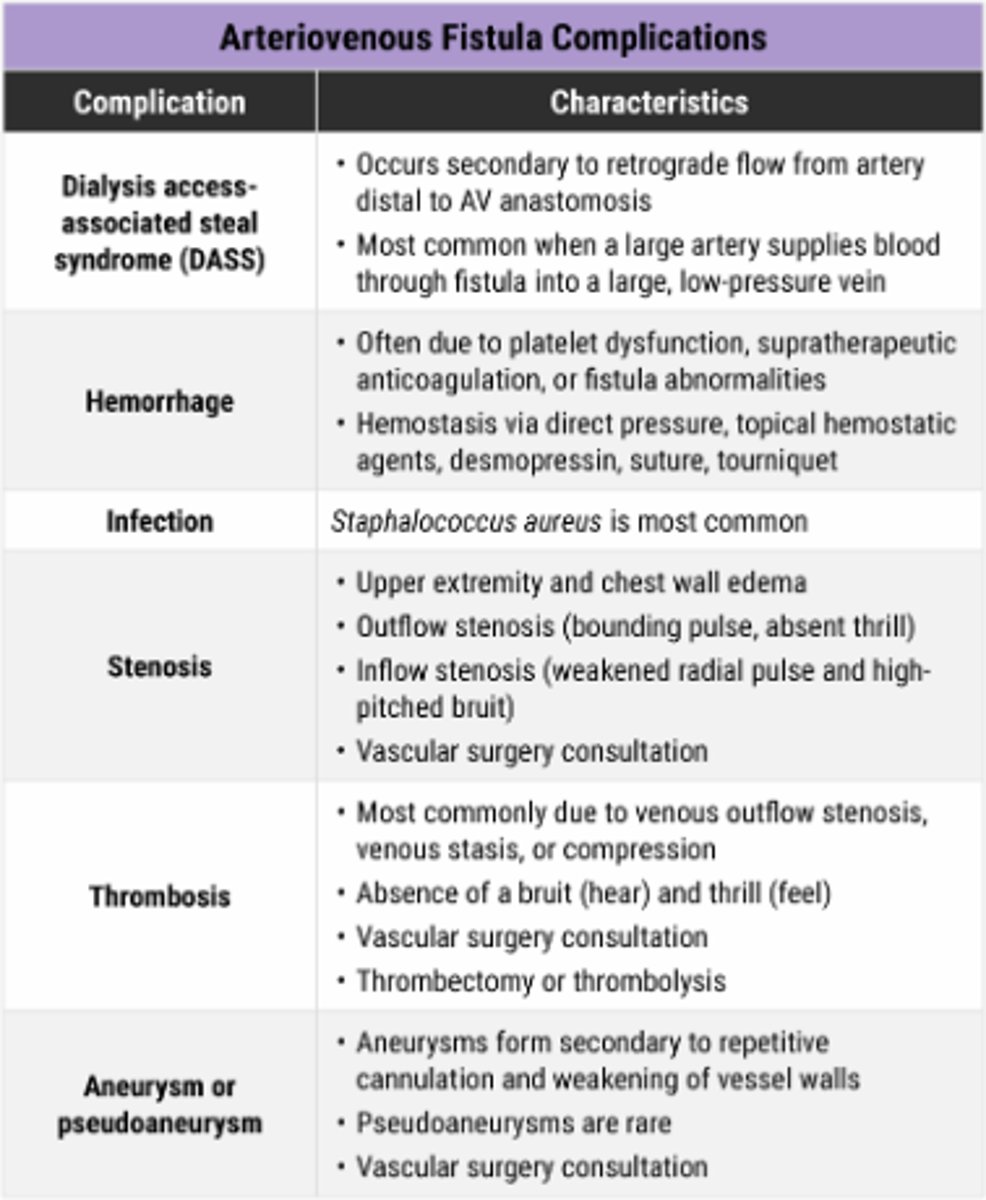
Fistula Complications
Primary Closure
- Primary Intention
-> Fastest type of closure
-> Small, clean defect
-> Blood vessels and keratinocytes migrate a small distance
Secondary Closure
- Secondary Intention
-> Wound edges cannot be approximated
-> Requires granulation tissue matrix to be built to fill the wound defect
-> More scar tissue than primary closure
Delayed Primary Closure
- Tertiary Intention
-> Wound is cleaned and observed for a few days to ensure no infection
-> Then surgically closed.
Paget Disease of the Breast
Hallmark: scaly, raw, vesicular, or ulcerated lesion that begins on the nipple and then spreads to the areola
Paget Cell: Atypical cells with large nuclei and vacuolated cytoplasm
- Pain, itching, burning, present before clinically apparent
- Dx: skin biopsy and histology, mammography, ultrasound, MRI
Tx:
-> Simple mastectomy, breast conserving treatment (often selected)
Breast Implant Monitoring for Rupture
- MRI with dedicated breast implant protocol 5 years after the implants are placed, and every 2-3 years after
- In general, can be associated with anaplastic large cell lymphoma, implant associated squamous cell carcinoma, implant associated B-Cell lymphoma
Silicone Breast Implant
- Approved by FDA in November 2006
- Gel-filled implant with silicone shell
- Natural feel and appearance, with lower chance of rippling
- If implant rupture occurs, removal of silicone gel is required
Saline Breast Implant
- Approved by the FDA in May 2000
- Saline-filled implant with a silicone shell
- Can be inserted empty, allowing for more discreet incisions
- If implant rupture occurs, saline will be absorbed by the body.
Pneumothorax vs Tension Pneumothorax Tx
1- Chest thoracotomy
2- Needle Aspiration
Kidney Stone Treatment
An initial trial of supportive measures (e.g., pain control), urine straining, and medical expulsive therapy (e.g., tamsulosin) for 4 weeks is appropriate for stones > 5 mm and ≤ 10 mm in diameter in patients without infection or obstruction. Urologic consultation for surgical intervention, such as shock wave lithotripsy, is the most appropriate next step in management for stones that persist after 4 weeks. The size of the stone (6 mm) and its location at the ureteropelvic junction make it amenable to shock wave lithotripsy, which is a noninvasive treatment that uses shock waves to break the stone into smaller fragments that can be passed spontaneously. Shock wave lithotripsy is typically indicated for stones < 10 mm and located in the kidney or upper ureter. It is not an appropriate option for larger or more complex stones (e.g., staghorn calculi).
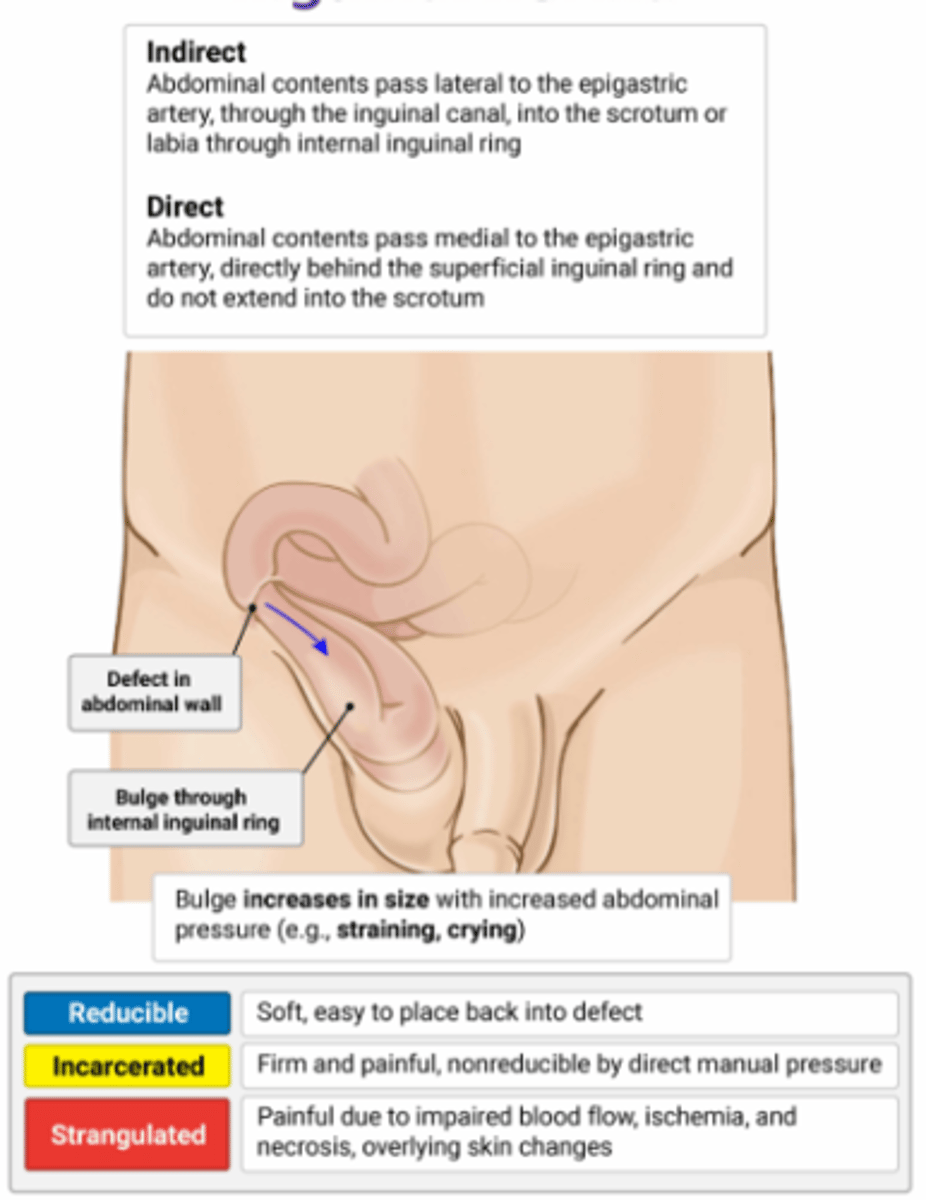
Hernias
Hemothorax
Supine CXR can show opacity
Initial treatment is tube thoracostomy
Thoracotomy indications Adults: initial chest tube output > 20 mL/kg (or 1,500 mL) or subsequent output > 200 mL/hour over 3 hours
Pediatrics: initial chest tube output > 15 mL/kg or subsequent output > 2-3 mL/kg over 3 hours
Large Bowel Obstruction
Most commonly caused by colorectal cancer
Most common location is sigmoid colon
Presentation: abdominal distension, obstipation, progressive changes in bowel habits
PE: high-pitched bowel sounds
Treatment is NGT, surgery
Goals of Perioperative Diabetes Management
- Avoid Hypoglycemia
- Prevent ketoacidosis and hyperosmolar stats
- Maintenance of fluid and electrolyte balance
- Avoidance of marked hyperglycemia
Diabetic Patient Pre-Op Work Up
- ECG to assess for asymptomatic ischemia
- Creatinine to assess for kidney injury
- Discontinue SGLT-2 3-4 days before surgery
- Other meds held day of
- Insulin can continue, assuming they don't cause any hypoglycemia
Necrotizing Fasciitis Treatment
- Surgical debridement ASAP
- Broad spectrum abx
- +/- fluids
Foreign Body Aspiration Treatment
Direct laryngoscopy with bronchoscopy
Length of time it takes vasectomy to produce sterility
- Many weeks, recommended to have semen analysis 3 months after
Light's Criteria: Transudate
- Pleural to serum protein ratio: < 0.5
- Pleural to serum LDH ratio: < 0.6
- Pleural Fluid LDH: <2/3 upper limit of normal
- Primary Causes:
-> Heart failure
-> Cirrhosis
-> Nephrotic Syndrome
-> Pulmonary Embolism
Light's Criteria: Exudative
- Pleural to serum protein ratio: >0.5
- Pleural to serum LDH ratio: >0.6
- Pleural Fluid LDH: > 2/3 ULN
- Primary Causes:
-> Malignancy
-> Bacterial or viral pneumonia
-> TB
-> PE
-> Pancreatitis
-> Esophageal Rupture
-> Collagen Vascular disease
-> Chylothorax, hemothorax
Meckel's Diverticulum
Congenital anomaly due to incomplete obliteration of the omphalomesenteric duct
Most common in children, < 5 years old
Sx: painless rectal bleeding, abdominal pain, or obstruction
Rule of 2s
2 years old
2 feet from ileocecal valve
2 inches long
2% of the population
2 epithelial types (typically gastric, intestinal, or pancreatic)
Diagnosis is made by technetium-99m pertechnetate scan (Meckel scan)
Tx: surgical resection if symptomatic
Thoracic Aneurysm X-ray
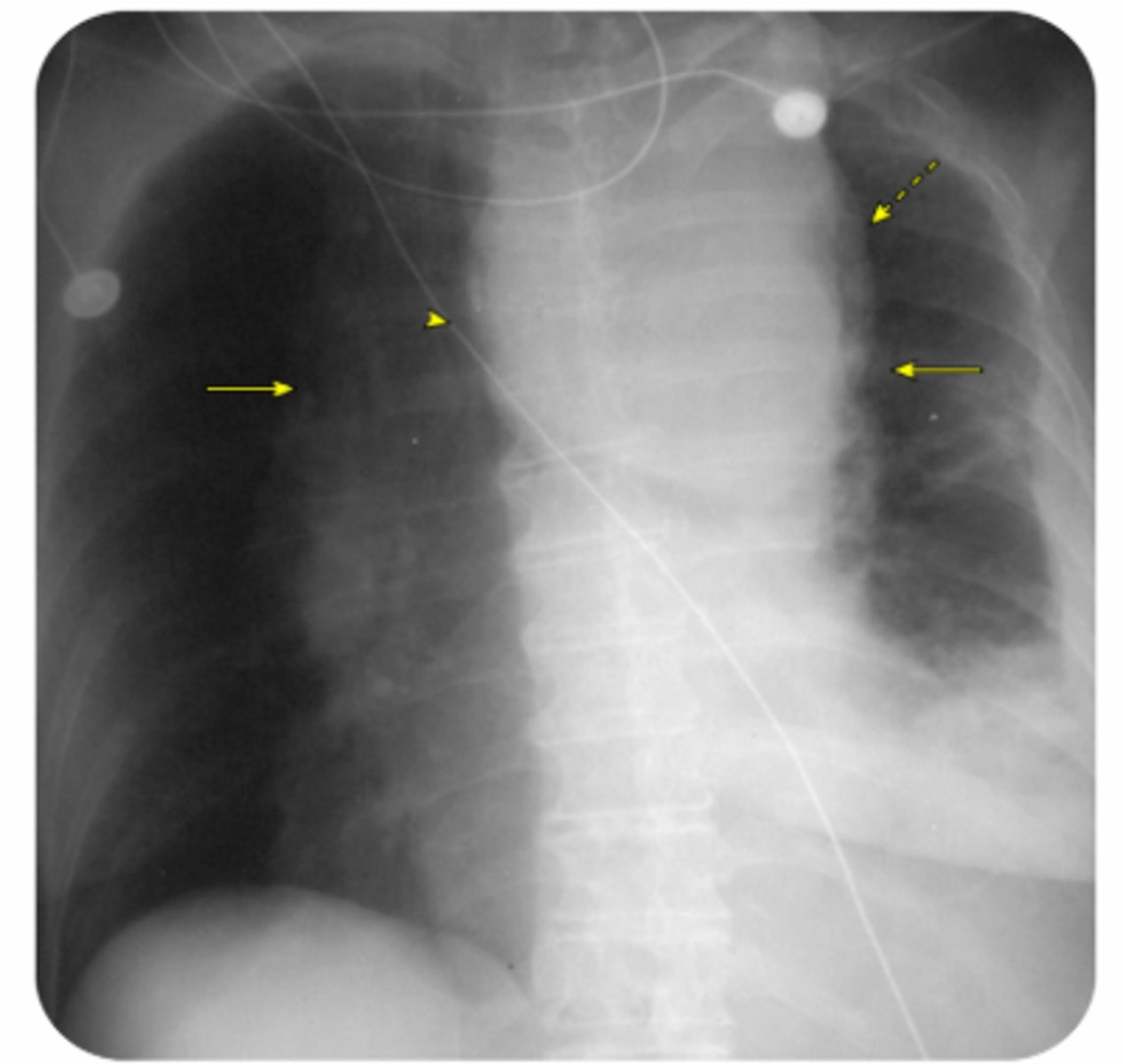
Hernia Characteristics
- Reducible: soft, easy to place back into defect
- Incarcerated: Firm and painful, non-reducible by direct manual pressure
- Strangulated: painful due to impaired blood flow, ischemia, and necrosis or overlying skin changes
Primary Hyperparathyroidism Symptoms
- Stones (kidney stones)
- Bones (bone pain)
- Groans (GI symptoms)
- Psychiatric Overtones (cognitive changes)
Esophageal Cancer
Risk factors: male sex, chronic GERD, tobacco and alcohol use, HPV infection
Sx: progressive dysphagia to solid foods, weight loss
Diagnosis is made by endoscopy with biopsy
Most common type in the US is adenocarcinoma, second is squamous cell carcinoma
Adenocarcinoma usually a complication of GERD or Barrett esophagus
Post-Operative Ileus RF
- Prolonged abdominal of pelvic surgery
- Lower GI surgery
- Open Surgery
- Delayed Enteral nutrition of NG tube placement
- Intra-Abdominal Inflammation
- Peri\operative complication
- Intraoperative/Post-op bleeding
- Perioperative opioid use
Type 1 Drug Eruption
IgE Mediated
- Urticaria, angioedema, and anaphylaxis
Type 2 Drug Eruption
IgG mediated
- Drug Induced thrombocytopenia
Type 3 drug reaction
- Immune complex
- serum sickness, vasculitis, drug-induced lupus
Type 4 drug reaction
T-Cell mediated macrophage inflammation
- Morbilliform rashes (macular and papular)
- Pruritis and fever
- TB Skin test is this
- most common offending agents are aminopenicillins, cephalosporins, antibacterial sulfonamides, allopurinol, and anticonvulsant drugs
Breast Abscess Management
- Drainage (Needle aspiration 1st, then I and D)
-> I and D if necrotic tissue present
- Antibiotics (dicloxacillin, cephalexin)
-> If MRSA, then TMP-SMX, or clinda
- If breast feeding, DO NOT STOP
Pancreatic Cancer
Risk factors: history of smoking
Sx: abdominal or epigastric pain, painless jaundice, weight loss, anorexia
Labs: CA 19-9 serum marker useful in monitoring
Dx: U/S, ERCP or MRCP, CT, endoscopic ultrasound
Management: Resectable disease: Whipple procedure (pancreaticodudenectomy) + adjuvant chemo
Unresectable disease: FOLFIRINOX or gemcitabine-based chemo
Most common type is adenocarcinoma
Poor prognosis
Courvoisier Sign
An exam finding that refers to a nontender but palpable distended gallbladder at the right costal margin. It is classically associated with biliary or pancreatic cancer but is only present in about 13% of patients with pancreatic cancer.
Laparotomy vs Laparoscopy
-Otomy is 1 large incision
-Oscopy is through multiple small incisions
Achalasia Description of Barium Swallow
- Smooth tapering of the gastroesophageal segment and dilation of the proximal esophageal segment
Process of Informed Consent
- Ensuring the patient or surrogate has decision-making capability
- Discussing pertinent medical information
- Ensuring adequate understanding of the information
- Ensuring voluntaries of the patient's or surrogate's decision
- Jointly deliberating and obtaining the patient's or surrogate's agreement to a plan of care.
Simple Cellulitis Treatment
- Cephalexin, amoxicillin, dicloxacillin
Penicillin Allergic Cellulitis Treatment
- Clindamycin, erythromycin, azithromycin
MRSA Suspected Cellulitis Treatment
- TMP-SMX, Doxycycline, Clindamycin
Inpatient Treatment of Cellulitis
- Ceftriaxone, Clindamycin, Pip-Tazo, +/- vancomycin
Cellulitis
Commonly caused by group A Streptococcus or Staphylococcus aureus
Sx: pain, redness, swelling. More indolent onset than erysipelas
PE: tenderness, erythema with poorly demarcated borders, lymphedema, ± purulence
Abx selection depends on uncomplicated vs complicated cellulitis, PCN intolerance, MRSA risk factors, and purulence
Physiologic Nipple Discharge
Characteristics
- Usually bilateral
- White or clear
- May be straw colored, green, brown, gray
Common Causes
- Hyperprolactinemia
- Medications
- Neurogenic Stimulation
Pathologic Breast Discharge
Characteristics
- Usually unilateral
- Localized to single duct
- Persistent
- Spontaneous
- Serous, clear, yellow
- Sanguineous
- Seroguineous
Common Causes
- Papilloma
Testicular Cancer
Risk factors: cryptorchidism, age 15–35
Sx: testicular lump
PE: painless, hard, fixed mass
Labs: beta-hCG, AFP, or LDH may be elevated based on tumor type
Diagnosis starts with ultrasound
Tx: radical inguinal orchiectomy usually curative, radiation therapy or platinum-based chemo if metastatic
Atelectasis X-Ray
Atelectasis
- Loss of lung volume due to the collapse of lung tissue, leading to impaired gas exchange
- PE: Hypoxia
- Chest X-ray shows pulmonary opacification, displacement of intralobar fissures, and tracheal shift toward the affected side.
Ethical Principles of Consent
Autonomy
- To respect the patient's right to make their own decisions about their medical care
Beneficence
- To take actions that are expected to provide benefit to the patient
Nonmaleficence
- To refrain from actions that may cause harm to the patient
Justice
- To provide equitable care to all patients regardless of age, sex, race, socioeconomic class, and other characteristics
Veracity
- To tell the truth
- To provide informed consent so the patient can exercise autonomy
Fidelity
- To do what one has promised regarding care
Confidentiality
- TO protect the patient's privacy
Professionalism
- Respect patient boundaries and guard against violations
- Maintain competence in the practice of medicine with continuing education
- To interact respectfully with patient's families, staff, colleagues, other professionals
- To guard against actions that may result in impairment and seek help if needed
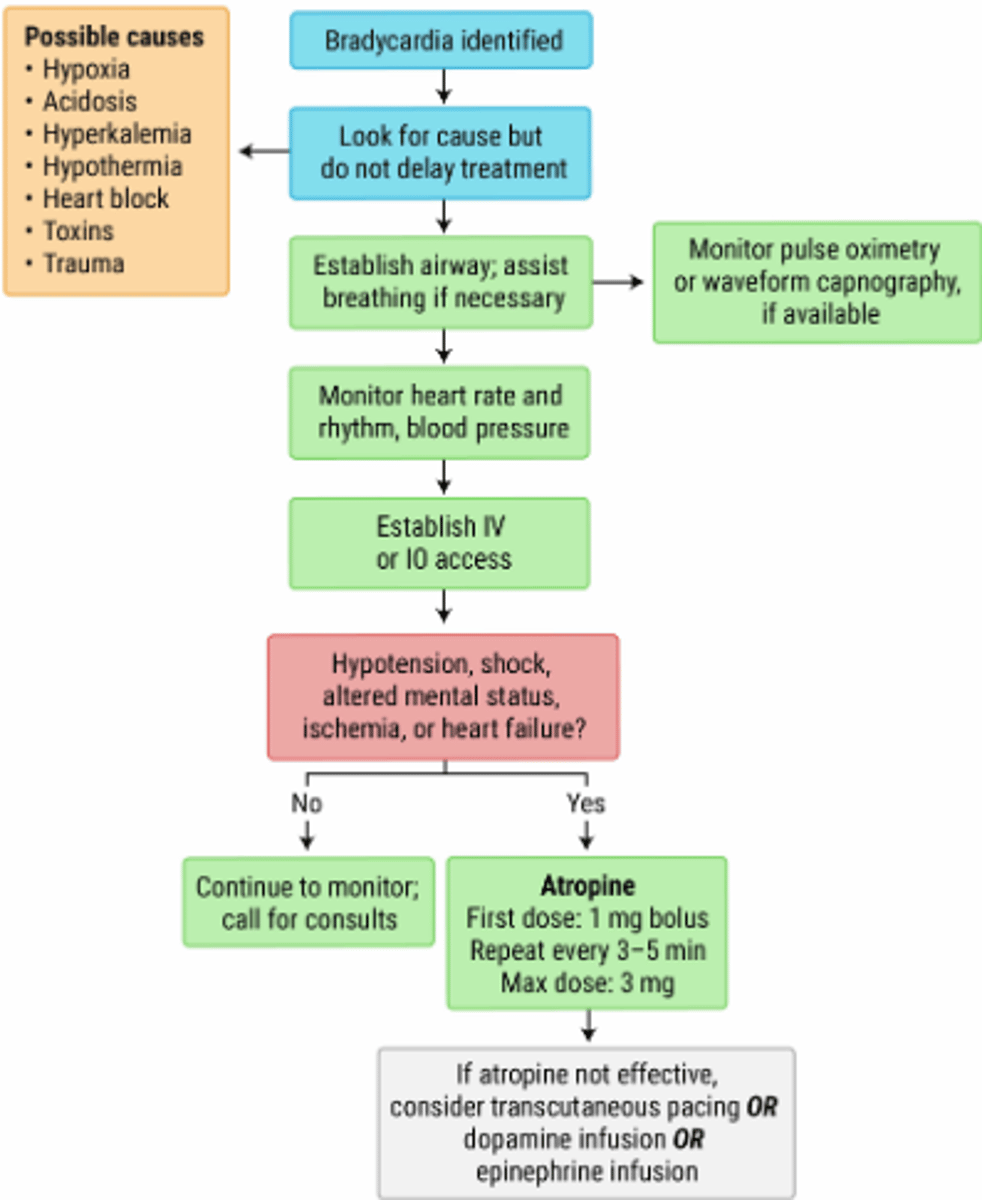
ACLS Bradycardia Algorithm
Cecal Volvulus
Congenital defect in peritoneum resulting in twisting of mobile segment of cecum
More common in younger individuals compared with sigmoid volvulus
Sx: abdominal pain, distension, vomiting, obstipation
Imaging X-ray: coffee bean or comma appearance
CT: mesenteric whirl sign
Tx: surgery
- second most common site of volvulus (after sigmoid)
Cecal Volvulus X-Ray

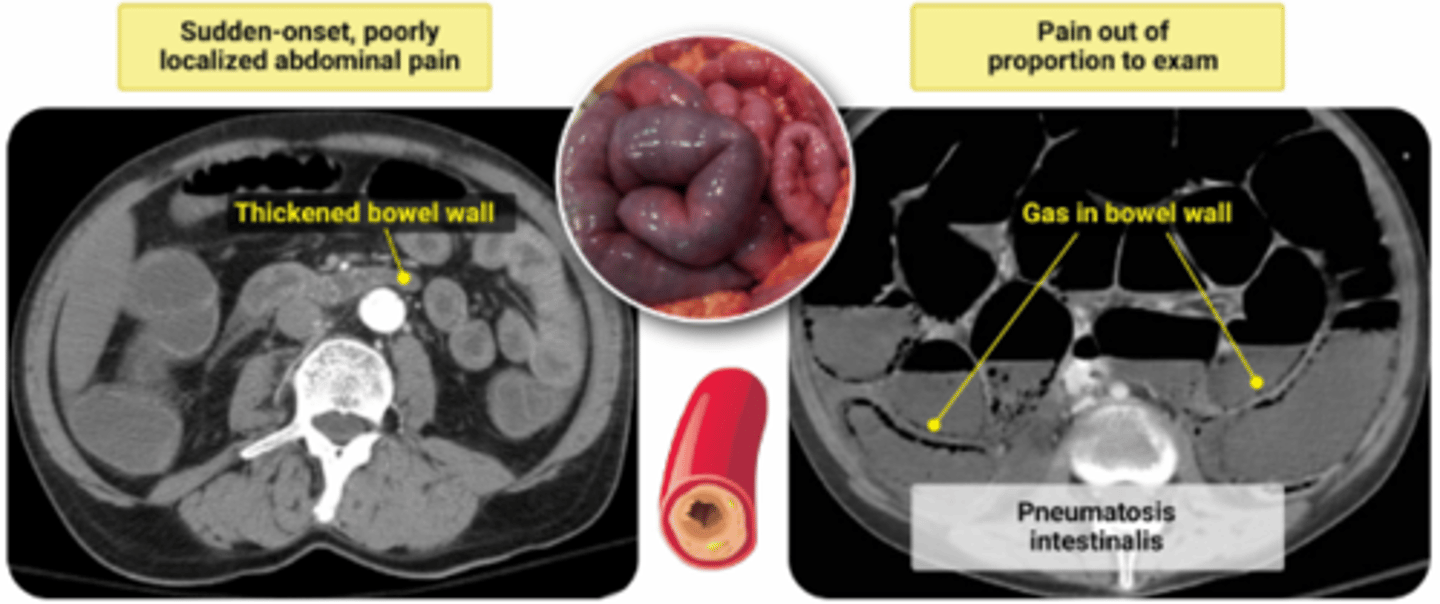
Acute Mesenteric Ischemia
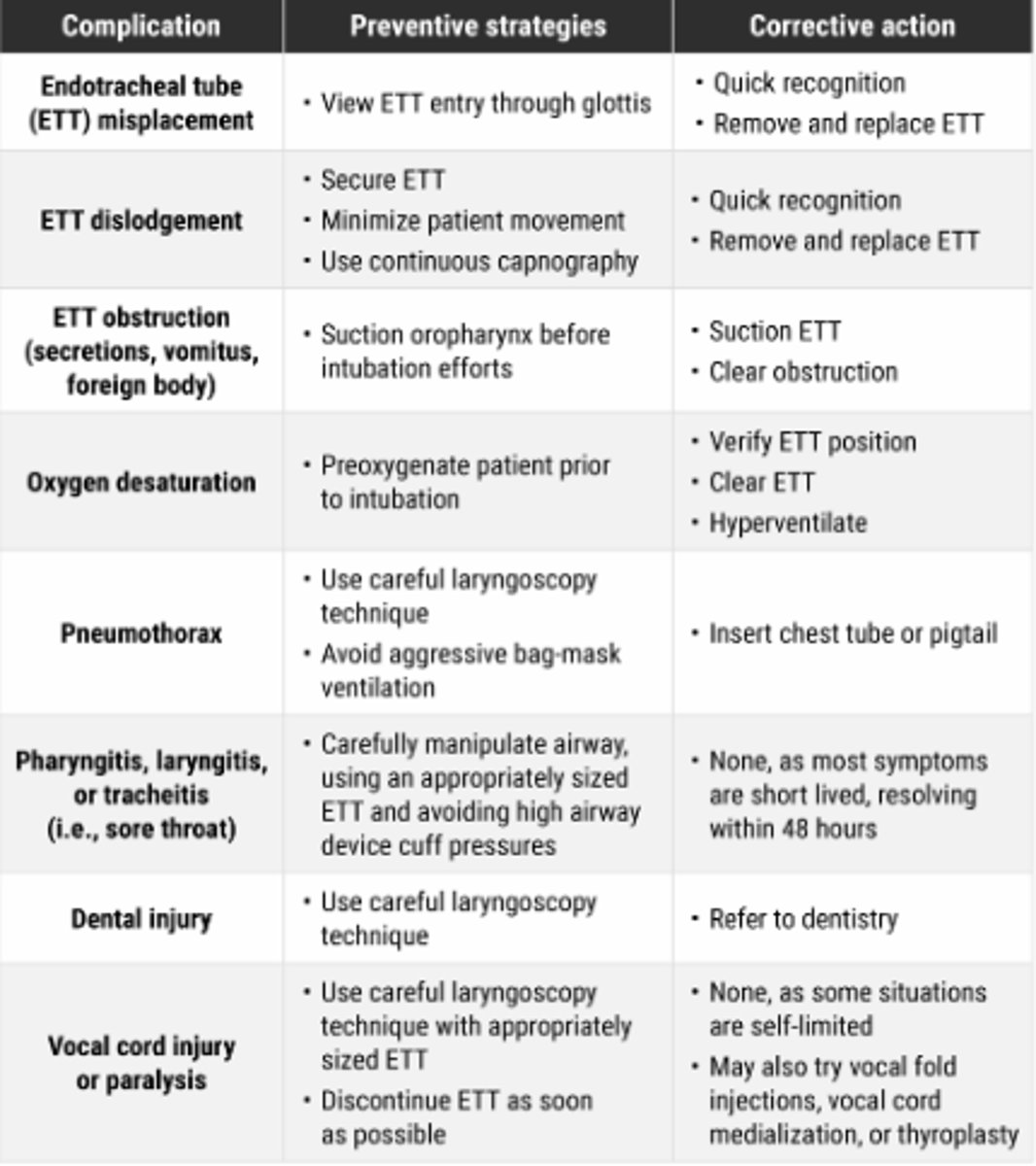
ET Tube Complications
Internal Jugular Central Venous Access
Location: anterior and lateral to carotid artery
Trendelenburg
Anterior approach: medial to SCM, aiming toward ipsilateral nipple
Posterior: lateral to SCM, aiming toward sternoclavicular notch
Central: between sternal and clavicular heads of the SCM, aiming toward ipsilateral nipple
Right side preferred
Complications: carotid artery puncture, bleeding, hematomas → airway compression
Dysrhythmias: heart wall irritation, withdraw until cessation
Pulsatile flow: arterial puncture
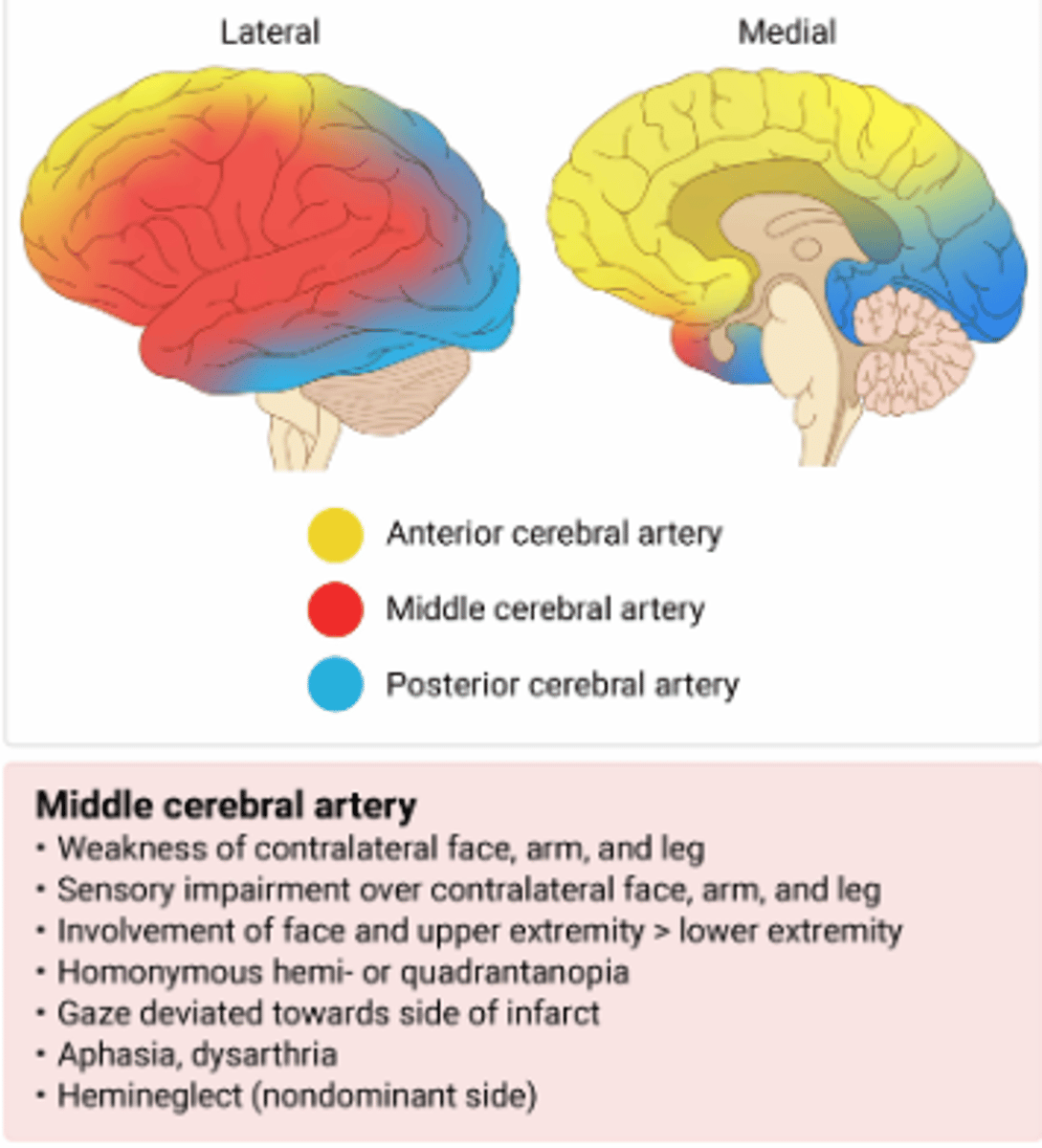
Stroke Distribution
Vitamin B12 Deficiency
Risk factors: vegan diet, metformin use, gastrectomy
Sx: fatigue, weakness, and peripheral neuropathy
PE: pallor and glossitis
Lab results: MCV > 100 fL, hypersegmented neutrophils, elevated homocysteine, elevated methylmalonic acid
Tx: parenteral vitamin B12, oral considered if no neurologic Sx or malabsorption
Neuropathy is more common with vitamin B12 deficiency (as opposed to folate deficiency)
Pernicious anemia: autoimmune destruction of cells that produce intrinsic factor, resulting in vitamin B12 deficiency
Choledocolithiasis
Presence of gallstones within the common bile duct
Sx: RUQ or epigastric pain, nausea, vomiting
Lab results: elevated LFTs in a primarily cholestatic pattern
Dx: transabdominal ultrasound
Complications: acute cholangitis, acute pancreatitis
Tx based on the likelihood of choledocholithiasis (options include ERCP with stone removal, cholecystectomy)
Diverticulitis
Sx: abdominal pain localized to the left lower quadrant, fever, nausea, vomiting, and a change in bowel habits
PE: localized guarding, rigidity, and rebound tenderness
Diagnosis is confirmed by CT with IV contrast: thickened bowel wall, fat stranding
May show complications (bowel perforation, abscess, fistula, obstruction)
Consider treatment with supportive care or antibiotics based on risk factors and presentation
Antibiotics to cover gram-negative and anaerobic bacteria, bowel rest, and surgery (in severe cases)
High-fiber diet can help in prevention
Complicated Forms of Diverticulitis (Hospital)
Abscess formation, bowel obstruction, fistula formation, and bowel perforation.
Aortic Dissection
Risks: advancing age, male sex, HTN, Marfan syndrome
Sx: acute onset of ripping or tearing chest pain or back pain
PE: asymmetric pulses or SBP difference > 20 mm Hg
CXR: widened mediastinum
Dx: CT angiography or transesophageal echocardiogram (TEE)
Treatment: reduce BP and HR (beta-blockers), pain control, emergency surgery (type A dissection)
Type A: involves ascending aorta
Type B: involves only descending aorta
Aortic Stenosis
Risk factors: advancing age, diabetes, hypertension
Sx: dyspnea, chest pain, syncope
PE: crescendo-decrescendo systolic murmur that radiates to the carotids, paradoxically split S2, S4 gallop
Murmur decreases with Valsalva
Most commonly caused by degenerative calcification
Treatment: aortic valve replacement