INB 365S: Cardiac Cycle
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
diastole
the time during which cardiac muscle relaxes
systole
the time during which cardiac muscle contracts
how does contraction affect pressure?
contraction increases pressure
how does relaxation affect pressure?
relaxation decreases pressure
5 phases of the cardiac cycle
The heart at rest = late diastole
Both sets of chambers are relaxed and ventricles fill passively (80%) → blood flows by gravity from the atria into the ventricles and the relaxing ventricles expand to accommodate the entering blood
low pressure
Atrial systole
atrial contraction forces a small amount (20%) of additional blood into ventricles → pressure increases
follows the wave of depolarization that sweeps across the atria
When heart rate increases (exercise) atrial contraction plays a greater role in ventricular filling
At the end of atrial systole, the ventricles contain the largest volume = END DIASTOLIC VOLUME = EDV
S1 = BOOM (AV valves close)
Isovolumic ventricular contraction
first phase of ventricular contraction pushes AV valves closed, BUT does not create enough pressure to open semilunar valves
Ventricular ejection
as ventricular pressure rises (due to contraction) and exceeds pressure in the arteries, the semilunar valves open and blood is ejected
this pressure is the driving force for blood flow
AV valves remain closed and the atria continue to fill
the volume of blood left in the ventricle at the end of contraction = END SYSTOLIC VOLUME = ESV
S2 = BOOM (semilunar valves close)
Isovolumic ventricular relaxation
as ventricles relax, pressure in ventricles falls and blood flows back into cusps of semilunar valves
semilunar valves close
volume of blood in the ventricles is not changing
When ventricular relaxation causes ventricular pressure to become less than atrial pressure, AV valves open → blood that has been accumulating in the atria during the ventricular contraction rushes into the ventricles → the cardiac cycle begins again
how much time is spent contracting?
about 1/3 of the time
how much time is spent relaxing?
about 2/3 of the time
pressure volume curve
When the heart contracts, the pressure increases and blood flows out of the heart into areas of lower pressure.
A: the ventricle has completed a contraction and contains the minimum amount of blood that it will hold during the cycle
→ it has relaxed and pressure is at minimum value
→ blood is flowing into atrium from pulmonary veins
→ AV valve is open
A’: atrial contraction (last 20% of blood flow)
B: the ventricle contains the max volume of blood = EDV
→ ventricular contraction begins and the AV valve closes
C: semilunar valves open as ventricular presure exceeds pressure in aorta
D: semilunar valve closes = ESV
→ ESV = minimum volume of blood the ventricle contains during one cycle
D-A: isovolumic relaxation
When ventricular pressure finally falls to the point at which atrial pressure exceeds ventricular pressure, the mitral valve opens and the cycle begins again
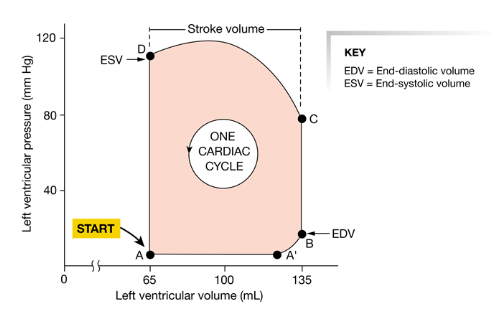
pressure volume curve: B → D
heart contraction
pressure volume curve: D → B
heart relaxing
How is pressure different for left and right sides?
volume is the same for left and right sides so flow is constant
right pressure is lower (just going to lung)
stroke volume
the amount of blood pumped by one ventricle during a contraction
Not constant → will increase as contraction force of ventricles increases (think exercise)
cardiac output
the volume of blood pumped by one ventricle in a given period of time
= stroke volume x heart rate
indicator of total blood flow through the body (not to various tissues)
Is cardiac output the same for both ventricles?
Normally - yes.
If one side of the heart begins to fall for some reason and is unable to pump efficiently, cardiac output becomes mismatched. Blood will pool in the circulation behind the weaker side of the heart
What initiates and modulates heart rate?
pacemaker cells initiate heart rate in the SA node and heart rate is modulated by neural and hormonal input
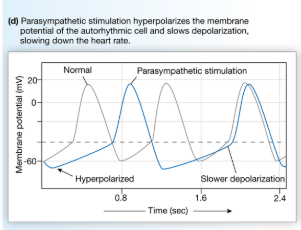
How does ACh affect heart rate?
slows heart rate (parasympathetic) by activating muscarinic cholinergic receptors that influence K+ and Ca2+ channels in pacemaker cells
→ increased K+ permeability (hyperpolarizes cell)
→ decreased Ca2+ permeability (slows rate of depolarization)
What determines heart rate?
rate of depolarization in pacemaker cells in SA node
→ can be increased or decreased due to sympathetic or parasympathetic innervation
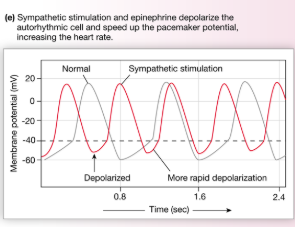
How do NE/E affect heart rate?
Increase ion flow through both funny and Ca2+ channels to speed up the rate of pacemaker depolarization
→bind to beta 1 receptors to alter transport properties of the channels
→ cAMP is the messenger for funny channels and allows them to remain open longer = increased Na+
→ cAMP as a second messenger for Ca2+ channels
2 ways heart rate can be increased
Decrease parasympathetic activity → pacemaker cells will resume their intrinsic rate of depolarization and heart rate will increase to 90-100 bpm
Sympathetic input → increases heart rate above the intrinsic rate (NE/E on beta 1 receptors)
How does ACh alter the rate of conduction?
slows the conduction of action potentials through the AV node to increase AV node delay
How do NE/E alter the rate of conduction?
enhance conduction of action potentials!
contractility
the intrinsic ability of a cardiac muscle fiber to contract at any given fiber length
function of Ca2+ interaction with contractile filaments
length-tension relationship/Starling curve
As stretch (indicated by ventricular EDV) of the ventricular wall increases, stroke volume (force) increases
= more blood to ventricle → more contractility
As additional blood enters the heart, the heart contracts more forcefully and ejects more blood
preload
GOOD
how much volume you send into the heart = EDV = the degree of myocardial stretch before contraction begins = load placed on cardiac muscles before they contract
What determines EDV?
venous return: the amount of blood that enters the heart from the venous circulation
affected by 3 factors:
contraction or compression of veins returning blood to the heart (skeletal muscle pump)
during exercise, the skeletal muscle pump helps return blood to heart
pressure changes in the abdomen and thorax during breathing (respiratory pump)
As you breathe in, low pressure decreases pressure in inferior vena cava → can draw more blood in
sympathetic constriction of veins → volume decreases → squeezes more volume out into the heart
inotropic
affecting contractility
How does Ca2+ affect contractility?
Contractility increases as the amount of Ca2+ available for contraction increases
ALSO! increasing sarcomere length makes cardiac muscle more sensitive to Ca2+
conduction vs contraction
conduction: electrical signaling
contraction: mechanical pumping
How do NE/E increase cardiac contraction?
bind to beta-1 receptors that activate cAMP second messenger systems to phosphorylate:
voltage-gated Ca2+ channels → open time increases → increased influx of Ca2+ from ECF
Phospholamban → increased activity of Ca2+-ATPase on SR
increased amount of Ca2+ stored in SR → increased amount of Ca2+ able to be released → more forceful contraction
Ca2+ is removed from cytosol faster → shortened Ca-troponin binding time → shorter duration of contraction
afterload
resistance that the left ventricle must overcome to circulate blood (semilunar valve)
not good!
pressure to prevent the blood from going out
To eject blood from the ventricle, the heart must create force to displace the blood in the aorta, pushing it farther downstream
found in pathological conditions, such as high diastolic blood pressure
3 factors affecting stroke volume
Preload/EDV (length-tension relationship) - positive effect
Contractility: increased ICF Ca2+ - positive effect
Afterload (MAP/EDV) - negative effect