BPK 241 Week 3
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
67 Terms
Skin Function
Protection (barrier from infections, UV light)
Themoregulation (open + close pores, control heartbeat, dilate and constrict blood vessels)
Sensation (feet or hands damaged when harmed)
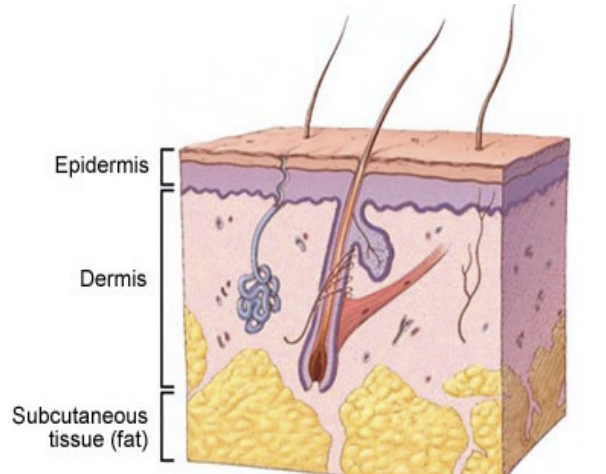
Skin Structure
Epidermis (most closest)
Basal cells
Keratinocytes/ Squames
Melanocytes
Dermis (sweat glands, hair follicle)
Subdermal adipose tissue (hypodermis) - blood vessels, fat help with temp + energy storages
Hyperhydrosis
Cause: sweating too much (exercise)
Secondary effects: most skin cause more friction, medication, low sugar
Treatment: Stay hydrated, rest breaks, prevent secondary effects, baby powders
Blisters
Shearing
Treatment: Changing socks, less friction, stay dry, prevent clot
Calluses, corn
Repeated blisters in one area
Shear or pressure
Treatment: Surgically remove it
Ingrown nails
Causes: Nail grow into nail bed laterally or medially
Secondary paronychia
Treatment: Proper trimming of nails, clippers, tweezers, ointment
Fungal Infections
Causes: Warmth, Darkness, Moisture
Contamination - direct/ indirect contact
Fungal Varieties: Tinea corporis
Body (ringworm)
Fungal Varieties: Tinea capitis
Scalp (rash & alopecia)
Fungal Varieties: Tinea Crotis
Groin
Fungal Varieties: Tinea Pedis
Feet
Fungal Varieties: Tinea ungulm
Nails and nail beds
Note responsive to tropical treatment
Bacterial Infections
Causes: Direct skin to skin contact
Indirect contact through contaminated objects ie. towels, mats, equipments
Treatments: Topical and oral antibiotics
Isolation of affected athlete from other competitors
Three Bacterial Infection Categories
Staphylococcus
Streptococcus
Bacillus
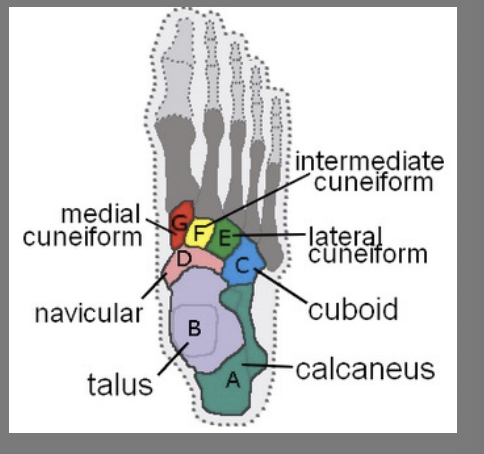
Talus
Proximal & Superior to calcaneus
Articulates with tibia and fibula
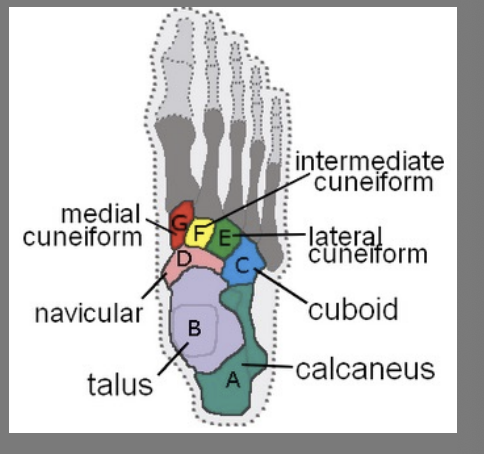
Calcaneus (heel)
Weight-bearing
Achilles tendon insertion
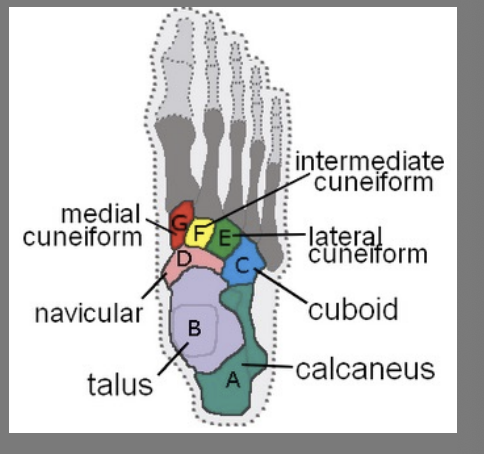
Transverse tarsal bones
Navicular (medial)
Cuboid (lateral)
Cuneiforms
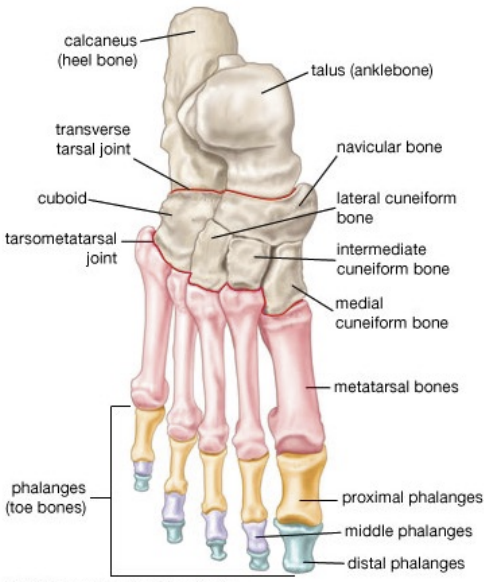
Metatarsals (MT)
I - V
I = medial (articulates with great toe)
V = lateral (articulates with pinky toe)
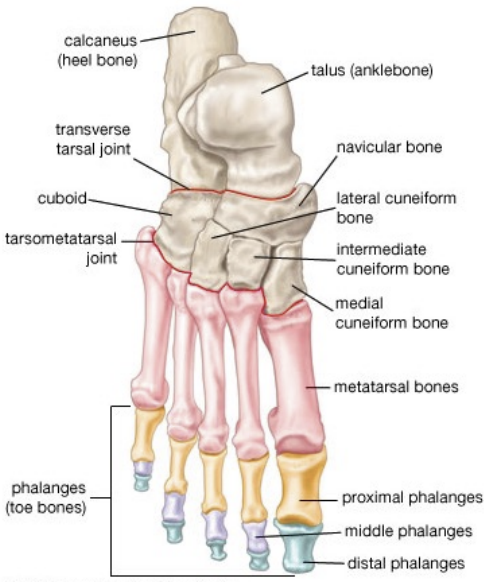
Phalanges
Phalanx = singular
Total = 14 per foot (2 in great toe, 3 in toes 2 through 5)
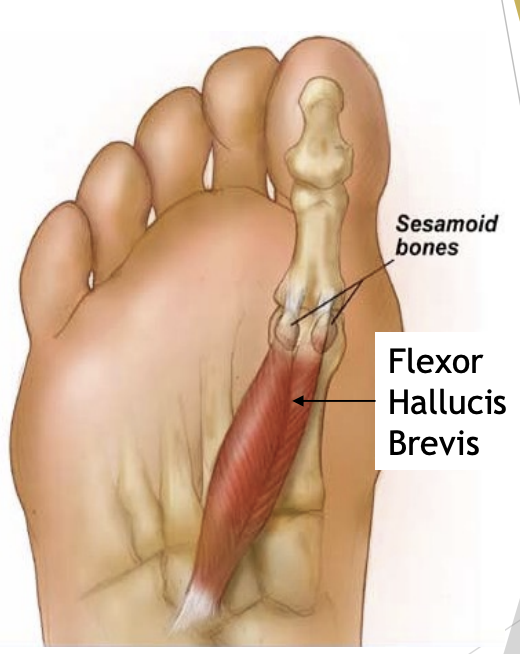
Sesamoid bones
2 (medial and lateral)
At head of 1st Metatarsal (plantar surface)
Gives greater mechanical advantage (levers)
Reinforces push or flex actions
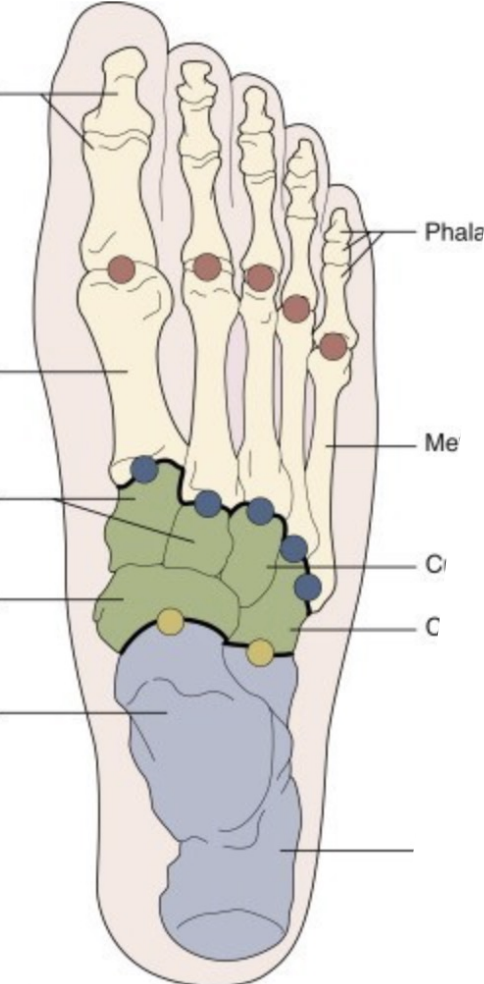
Areas of the Foot
Forefoot
Midfoot
Hindfoot/Rearfoot

Hindfoot joints
Subtalar (Inversion, eversion)
Talus & Calcaneus

Midfoot joints
Navicular with cuneiform & cuboid with cuneiform bone
Tarso-metatarsal
Cuneiforms & cuboid with MTs (Liz Frank joints)

Forefoot joints
Metatarsophalangeal (MTP)
Flexion & extension
Some abduction & adduction
Interphalangeal (IP)
Proximal and Distal (2-5 MTs)
Flexion & Extension - Hinge (Big toe)
Foot Muscle Flexors
Flexor Hallucis longus (FHL)
Flexor Hallucis brevis (FHB)
Flexor digitorum longus (FDL)
Flexor digitorum brevis (FDB)
All flex at MTP & IP joints
Also assist foot plantar flexion
Foot Muscle Extensors
Extensor Hallucis Longus (EHL)
Extensor Hallucis Brevis (EHB)
Extensor Digitorum Longus (EDL)
Extensor Digitorum Brevis (EDB)
All extend at MTP & IP
Also assist foot dorsiflexion
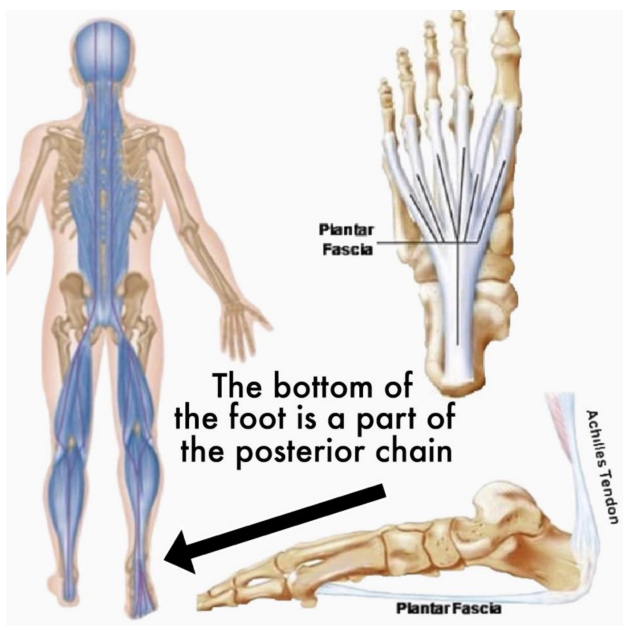
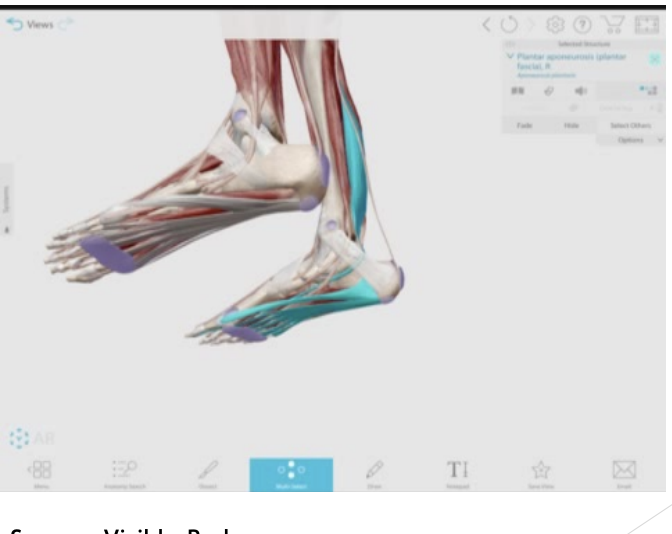
Plantar Fascia
Thick band of connective tissue at bottom of foot (calcaneus to tarsal heads)
Helps bend/arch foot
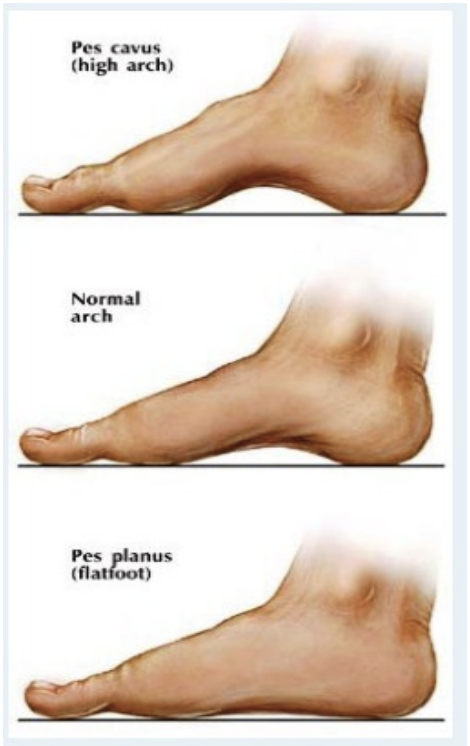
Foot posture: Pes Cavus, Neutral & Pes Planus
Looking at feet change
Looking at different degrees of arch
Symmetry? Higher or Lower? Footprints?
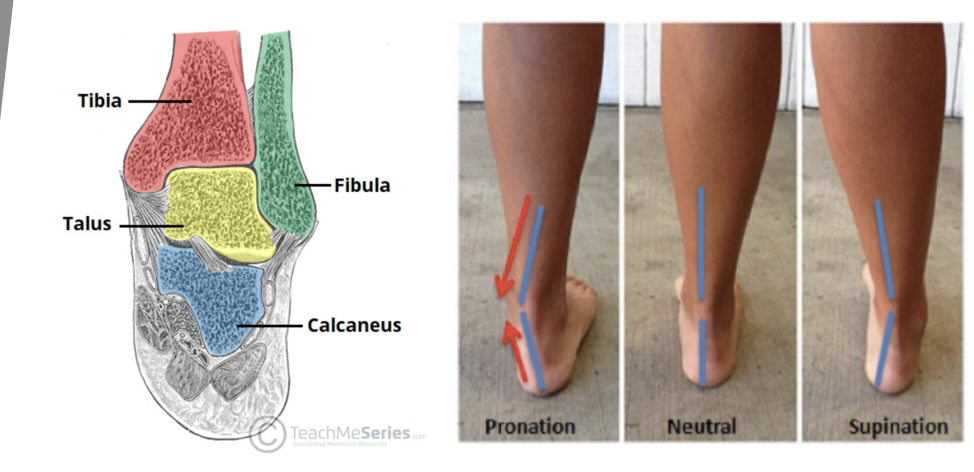
Rearfoot/Hindfoot position
Pronation & Supination
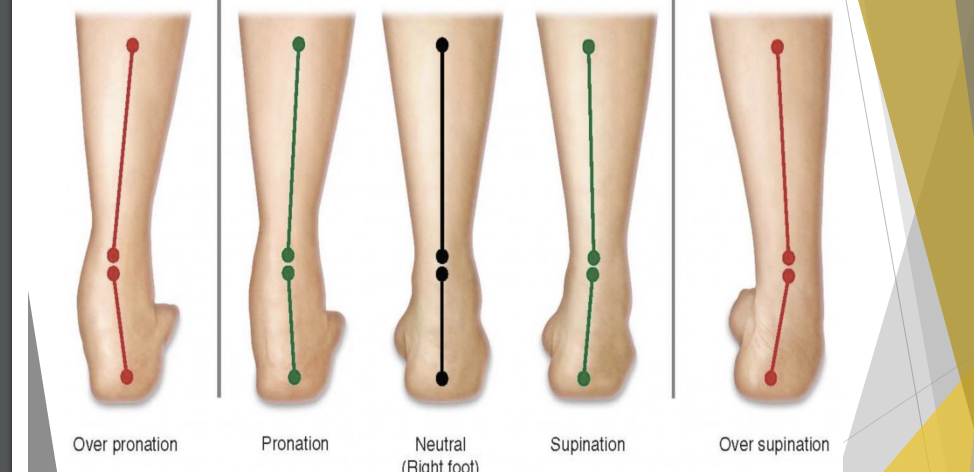
Over Pronation ←→ Over Supination
Increase pressure on soft tissue
Pronation
Medial arch collapse down a bit
Comes from mid foot joint
Allows foot to relax

Supination
High arch
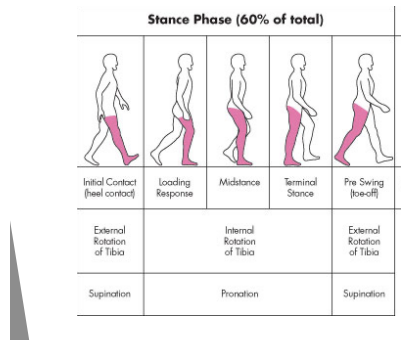
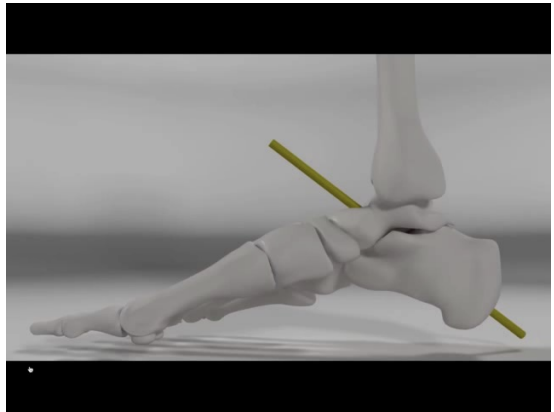
Normal Walking Gait - Stance Phase
Heel-strike occurs when landing on heel, foot should be in supination
Midstance immediately follows with foot moving into pronation
Toe-off follows midstance, foots return to supination prior to & during push off
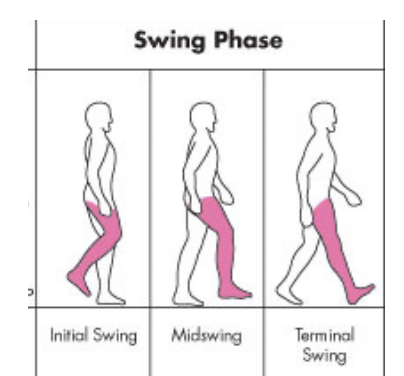
Normal Walking Gait - Swing Phase
Occurs when foot leaves ground & leg moves forward to another point of contact (40%)
Walking
Once foot is always in contact with ground
Running
Point when neither foot is in contact with ground
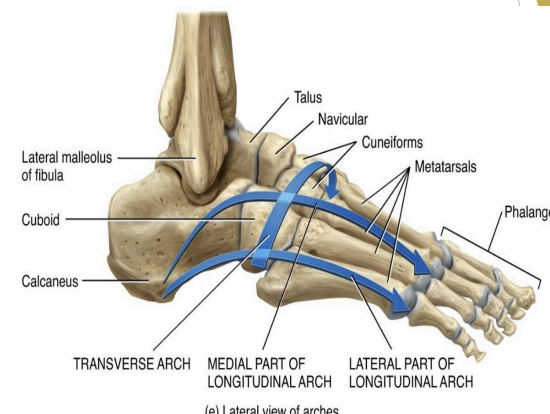
Foot Arches
Four in number
Medial longitudinal
Lateral longitudinal
Anterior metatarsal
Transverse
Foot Forms of support
Bony anatomy
Ligaments
Tendons/Plantar Fascia
Muscle Activity
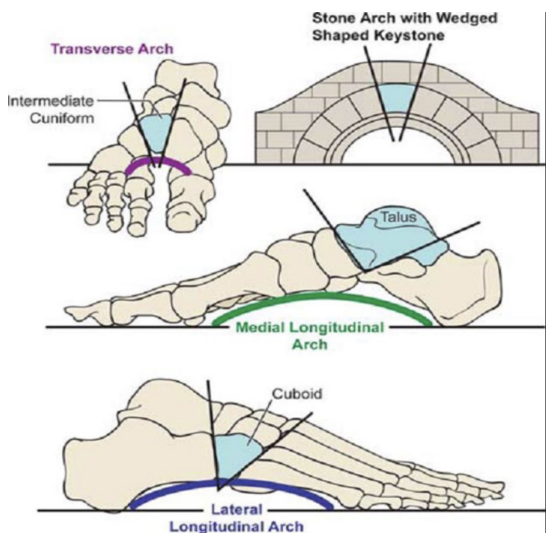
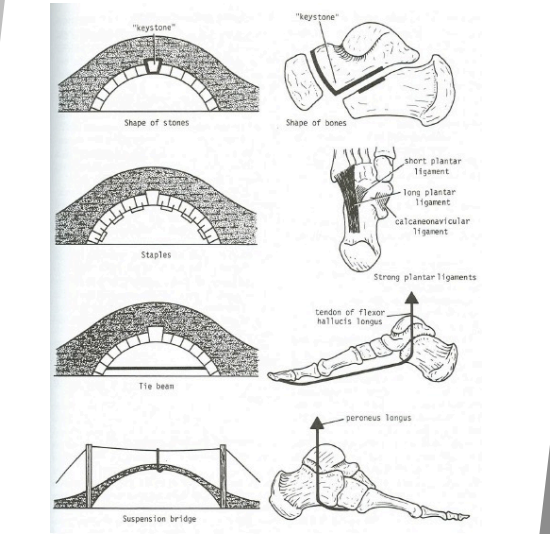
Keystone Bones
Support for arches of the foot
Either middle of highest point of arch
Integral for the structure of the bone

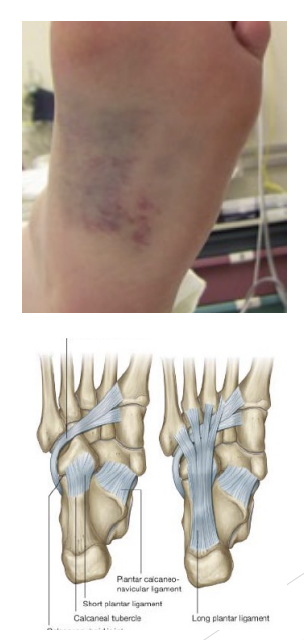
Ligament “Staple” support for arch of foot
Long plantar ligament hold’s bone together
Underside: Plantar calcaneonavicular ligament
“Tie beam/cable” support for arch of foot
Plantar fascia holding two ends of arch
Flexor Hallucis longus connecting to plantar fascia
“Suspension” support for arch of foot
Lots of suspension
Cable(muscles) attaching at the top of arch structure
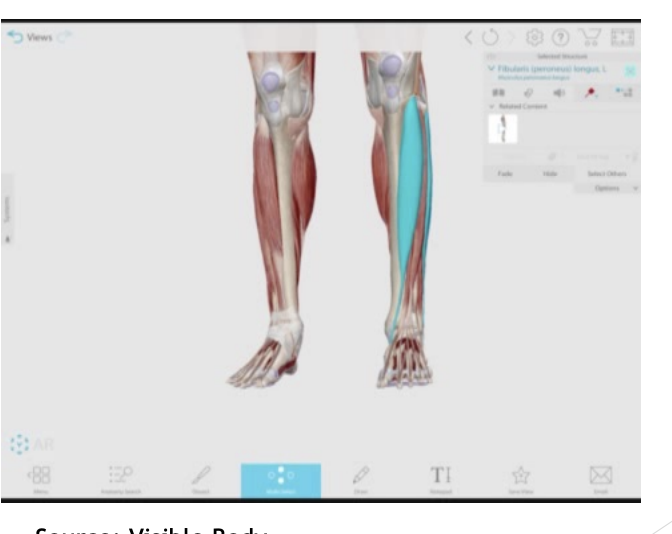
Tibialis anterior (medial longitudinal arch) and Peroneus longus (lateral longitudinal arch) are the cables of the foot
What is Windlass Mechanism?
Looks at movement of the medial longitudinal arch and how it is essential for BOTH shock absorption/ dissipation of forces AND stiff for propulsion
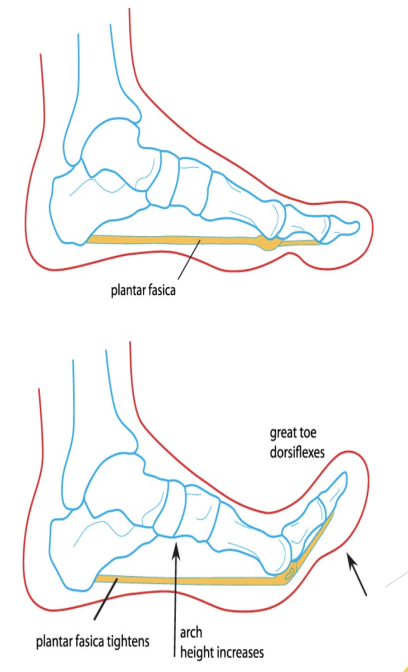
How is Windlass Mechanism accessed?
Prior to heel strike, ankle is in dorsiflexion, Plantar Fascia (PF) is taught, medial arch is high
During midstance, PF is relaxed to allow medial arch to collapse pronation for shock absorption
Prior to toe-off, first toe is in extension, PF become taught again, foot is stiff for take off, medial arch is high again
Relies on ability of 1st toe to extend normally
Published values range from 45 to 55 degrees of 1st toe extension to 60-70 degrees 1st toe extension required for normal gait
Ground Reaction Force Dissipation: Walking/ Running & Injury
Problems can arise when:
Foot too flexible & remains in pronation past midstance - soft tissue injuries
Foot is too rigid & does not pronate adequately - bony injuries

Exostoses
Causes: Excess bony growth, increase stress on the bone/joint, too much calcium around area
Obesity & abnormal weight bearing
Faulty footwear
Heredity
Mechanism: continued pull/tension, plantar flexion will respond to stress
Treatment: Correct predisposing factors, doughnut pad, may require surgery
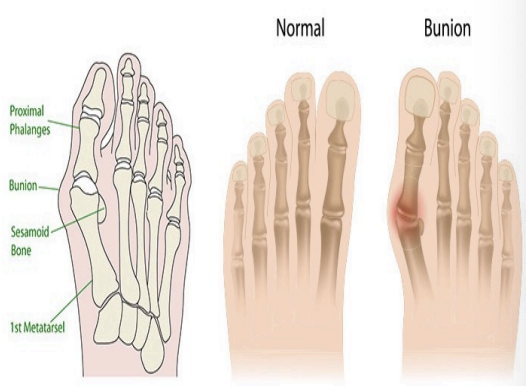
Bunion (Hallux vulgus)
Valgus deformity at MTP 1 (decrease in lateral joint angle)
Causes: Tight shoes, Heredity
Symptoms: Bone growth on medial side, increased pressure on medial metaphalanges
Treatment: Warm socks, Improved footwear +/ or orthoses, Wedge pads or taping, Surgery, try to decrease inflammation

Bunion Pads/ Braces
Fixes orientations of bone

Plantar (Morton’s) Neuroma
Usually between MTs III & IV
Causes: interdigital nerve becomes entrapped between metatarsal heads, Running & pounding +/ or tight shoes, when nerves gets compressed, it gets irritated and swells up
Differential Diagnosis: Anterior arch sprain
Symtoms: Lateral forefoot pain: intermittent, Spontaneous, Reduced when barefoot, Excruciating and click & pain with MT compression.
Treatment: Surgery

Metatarsal Pad
Tries to recreate metatarsal arch
Arch Sprains
Causes: Obesity, heredity, overuse, fatigue, poor footwear, hard surfaces
Symptoms: Pain with use, more when barefoot
1st degree - slight soreness
2nd degree - inflammation, drop of arch
3rd degree - fallen arch
Treatment: If we continue to stretch, arch will drop
Heel contusion
Cause: Traumatic impact to heal
Symptoms: Difficulty weight-bearing , localized tenderness under heat
Treatment: Reduce stress (rest padding), Heel cup, taping, NSAID, Physio, X-ray all but mildest cases
Complications: Fracture (#), Chronicity or recurrence, Periostitis, exostoses
Sprain
Ligament +/ or capsule damage
Causes: Kicking, Crush, Twisting
Symptoms: Localized pain, swelling, decrease of ROM
Treatment: X-Ray most toe sprains, POLICE, Tape or cast, then rehab
Turf Toe
Sprain of 1st MTP joint ligament and capsule
Forced hyperextension of 1st MTP joint beyond 60 degrees
Incidence has increased with artificial turf
Symptoms: Pain near 1st metatarsal head, decreased ROM, difficulty running or changing directions
1st MTP is red, swollen, tender
Pain worst at end range 1st toe extension
Treatment: Supportive footwear, POLICE, lower body rehab
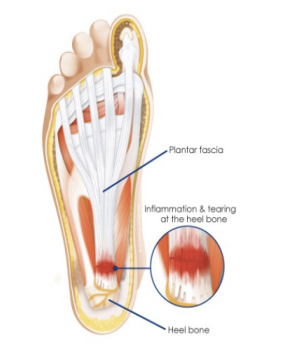
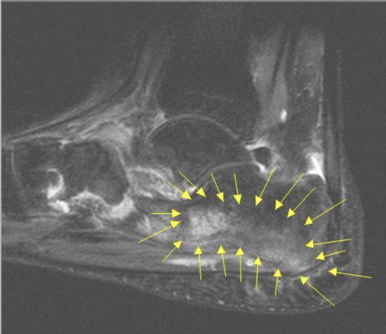
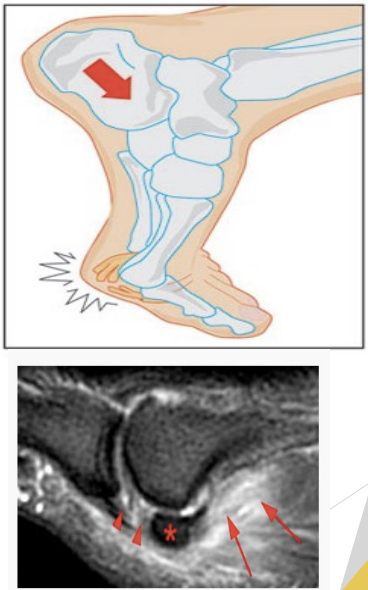
Plantar Fasciitis
Predisposing factors
Pes Cavus or Pes Planus
Running (weight on ball of foot)
Change in footwear
Signs and Symptoms
Pain in medial arch/medial distal heel
Pain worst in morning and with sitting
Swelling and tenderness, heel spur on x-ray
Treatment
Adequate rest
Stretching exercises (include Achilles tendon)
Physiotherapy with ultrasound
Soft orthotics
Gradual return to exercise, supervised

Plantar Fasciitis Treatments
Plantar fascia and Gastrocnemius/ Solues/Achilles Tendon stretching
Surgery is LAST resort
American Association of Foot & Ankle Specialists Position Statement
Don’t do surgery for Plantar Fasciitis before 6 months of conservative treatment
97% will resolve with 6 months of consistent nonoperative treatment

Fractures
General considerations
Past History, deformity, crepitus(crunchy sensation),tenderness
POLICE, splint, transport, X-Ray(Ottawa Ankle Rules)
Specific foot fractures
Ankle sprains: Talus, Fibula, Tibia
Fall or jump: Calcaneus (vertebrae?)
Crush injury: metatarsals, Phalanges
Overuse(Stress): Metatarsals, Tibia, Fibula, Calcaneus
Kicking injury: Phalanges

Navicular Stress Fracture
History: Pain, often for many months
Symptoms: Midfoot pain, worse with activity
Fracture often not evident on X-Ray = therefore delayed diagnosis, bone scan, CT scan, or MRI needed
Treatment: Non-weight bearing cast, if not healing surgery required
Foot - Rehabilitation/Reconditioning
POLICE/ Activity Modification
NSAIDS
Modalities
Footwear modification
Stretching - Early “pain free” ROM
Include proximal joints
Strengthening
Early = Toe raise(seated), ankle circumduction, towel gathering
Later = running in pool, squats, cycling, swimming
Finally = jogging, running, skipping
Taping/Orthoses
Surgery?

POLICE/ Activity Modification
Avoid aggravating activities
Take few days off running or prolonged standing
Ice packs for pain, helpful with acute conditions
NSAIDs - Anti-inflammatory medications (if signs of inflammation present)

Rehabilitation/Reconditioning
Modalities
Contrast bath
Ultrasound
Shockwave Therapy
Laser Therapy
Electrical stim
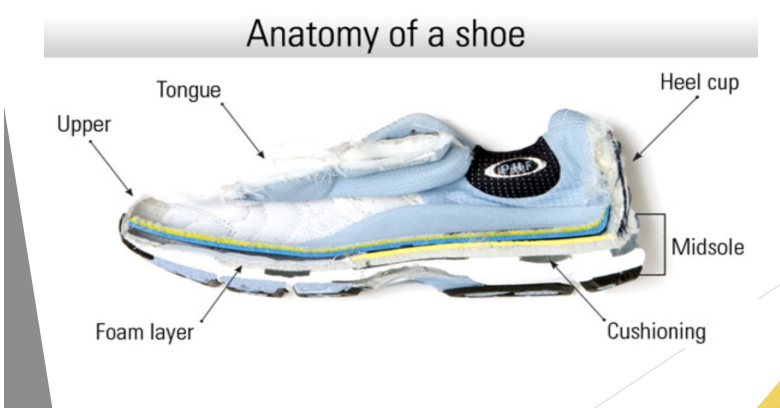
Footwear Modification
Proper fitting footwear
Proper shock absorption AND/OR arch support
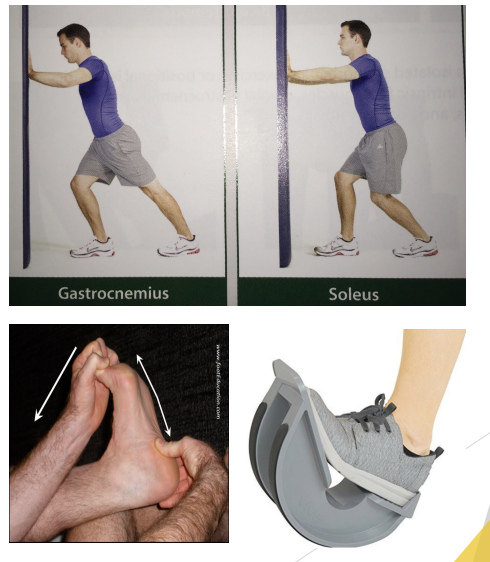
Stretching
Gastrocnemius and Soleus Stretching
Plantar Fascia

Strengthening Exercises
Towel Scrunches
Marble pick ups
Short foot exercises

TAPING/Orthoses
Low dye arch tape job
Calcaneal fat pad tape job
Orthotics
Heel Cup
Night splint
Surgery
Indicated in long term cases when conservative treatment fails
Plantar fascia release - increase its length
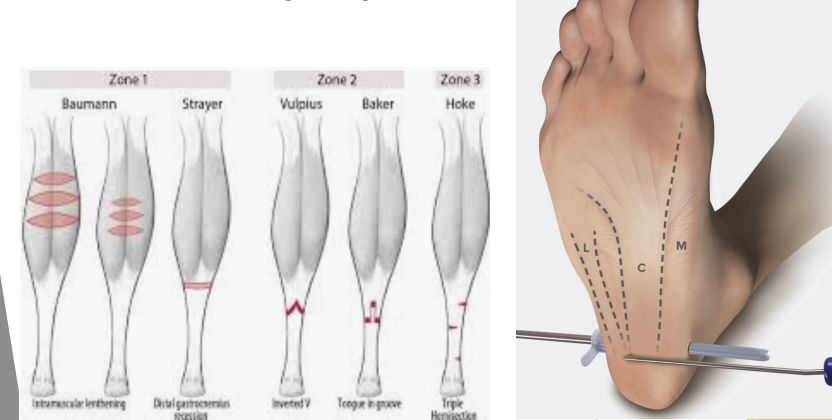
Gastrocnemius lengthening
Ankle Rehab
Activity Modification/Controlled Weight Bearing
Strengthening
Balance/ Proprioception
Running Progression
Return to Sport