lecture 8: ribs
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
clavicles
C5 dermatome
nipples
T4 dermatome
xiphoid process
T7 dermatome
inguinal/groin regions
T12 dermatome
2-10
what is considered the typical ribs?
rib head
articulates with the corresponding vertebra and the one above.
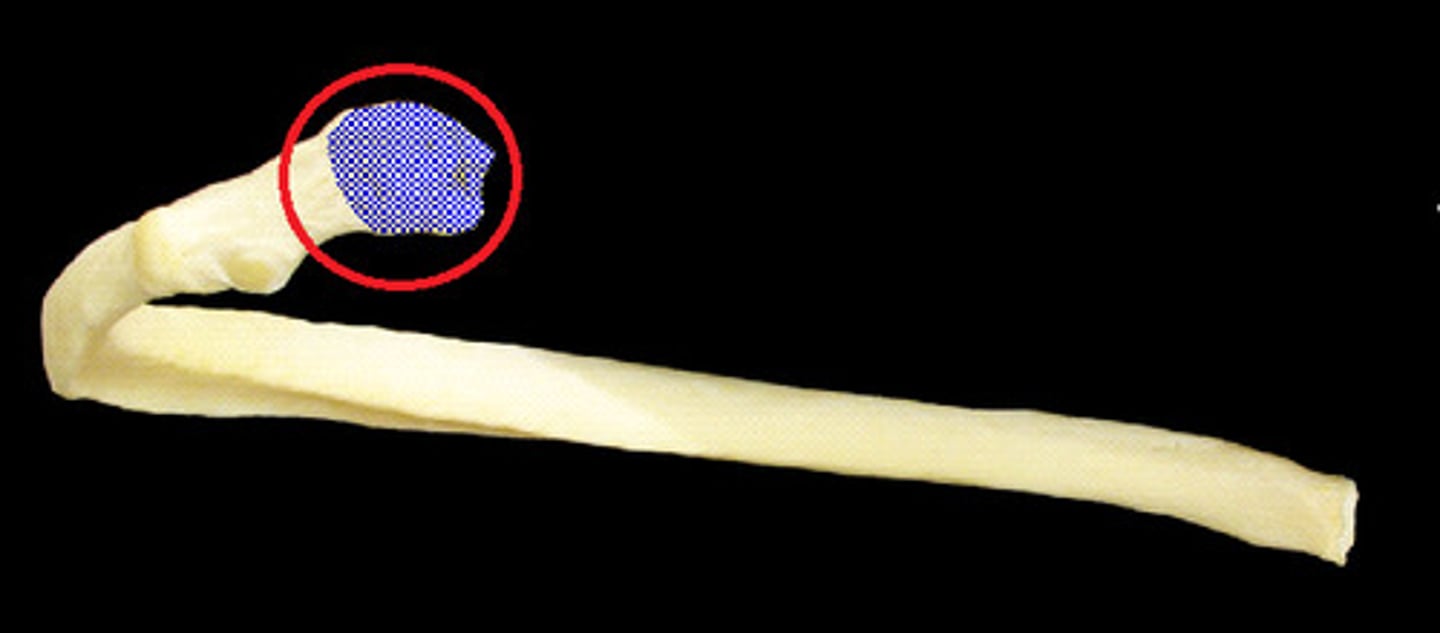
rib tubercle
articulates with corresponding transverse process

•All display both transverse axis (pump handle) and AP axis (bucket handle) motion
•Upper ribs prefer pump handle
•Lower ribs prefer bucket handle
all the typical ribs (2-10) display these motions
pump handle
upper typical ribs prefer what motion?
bucket handle
lower typical ribs prefer what motion?
ribs 1, 11-12
what are the atypical ribs?
ribs 1-7; articulate directly with sterum
what are the true ribs
ribs 8-10
-merge into a single cartilaginous mass that attaches to the sternum
what are the false ribs
11-12
what are the floating ribs?
rib 2
typical except for a large tuberosity that allows it to attach to serratus anterior
rib 11 and 12
these ribs do not have tubercles and do not attach to sternnum/costal cartilage
anterior scalene and middle scalene
muscles used to treat rib 1
posterior scalene
muscle used to treat rib 2
A/P direction
When the more superior ribs elevate, their movement expands the ribcage in what direction?
lateral direction
When the more inferior ribs elevate, their movement expands the ribcage in what direction
functional transverse axis that passes through the posterior tubercle and the head of the rib
(primarily ribs 2-5)
axis of pump handle rib motion
Anterior Rib head moves cephalad (superiorly)
Posterior rib head moves caudad (inferiorly)
motion of pump handle ribs during inhalation (2-5)
functional anteroposterior axis
-increases the transverse diameter of rib cage
bucket handle motion occurs about what axis (ribs 6-10)
•The intercostal space separates during inhalation and narrows during exhalation
motion of buckethandle ribs during respiration
caliper motion
As you inhale they move farther apart (unpinch), and as you exhale, they pinch together.
motion of ribs 11 and 12
top rib
in exhalation SD, treat this rib first
bottom rib
in inhalation somatic dysfunction, treat this rib first
pectoralis minor
muscle associated with rib 3, 4, 5 dysfunction
seratus anterior
muscle associated with rib 6-10 dysfuction
latissmus dorsi
muscle associated with rib 9-12 dysfunction
quadratus lumborum
muscle associated with rib 12 dysfunction indirectly
ribs 6-12
ribs associated with the diaphragm
•C3,4,5 (Phrenic n.)
innervation of the diaphragm
Pressure Gradients
Venous Return
Lymphatic Return
Fascial Considerations
functions of the diaphragm
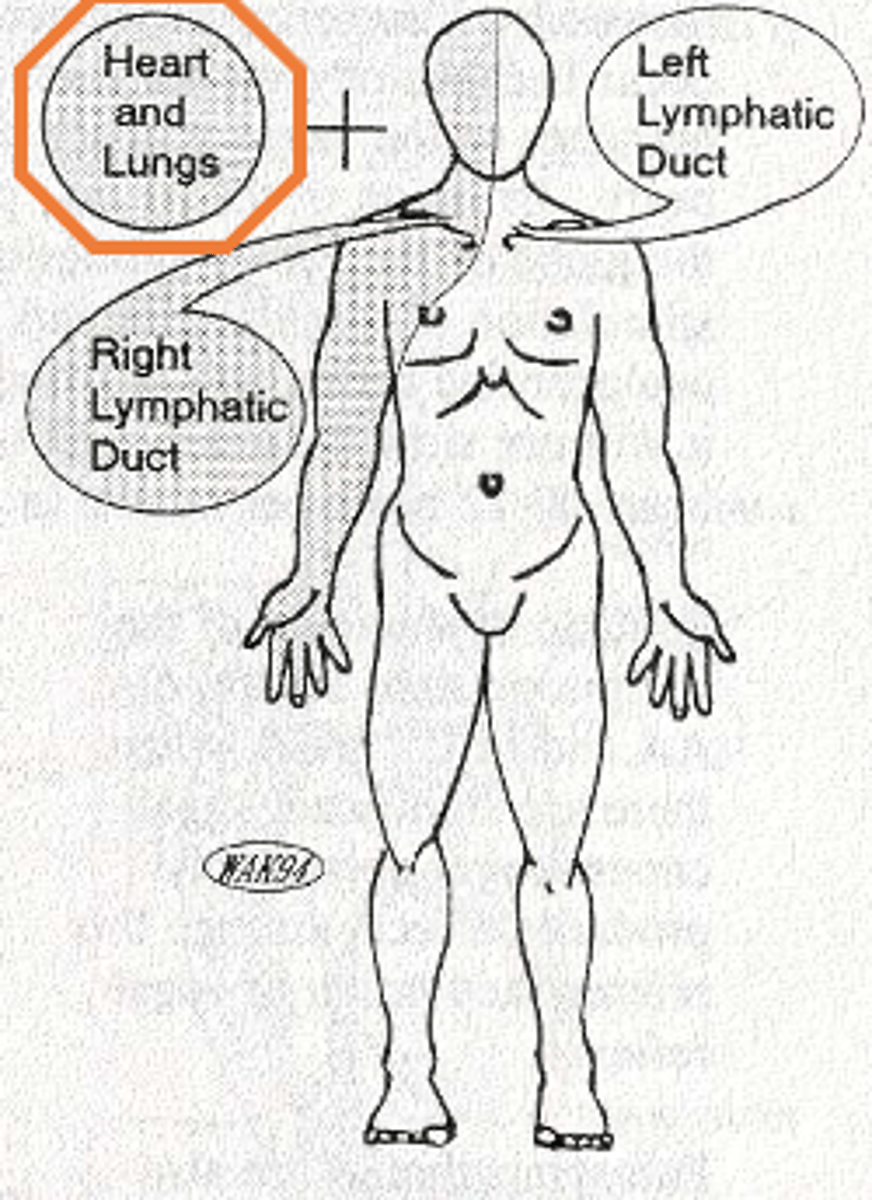
•pretracheal nodes and then to the right lymphatic duct.
pleural sac and lung tissue lymphatics drain into
anterior
the sympathetic chain ganglion lie _______ to the rib heads
•Hands or fingers lined up along costosternal joint
method of screening ribs 2-6
•Hands placed anterolateral with fingers running parallel to ribs
method of screening ribs 7-10
respiratory cooperation
-treatment technique only used for inhalation dysfunctions
-uses pt's own respirations to correct dysfunction in the ribs, utilizing the primary respiratory muscle
-contact anterior rib and accenuate exhalation while resisting inhalation
•Primarily an indirect technique
•Practiced often as a mixed technique
•Patient passive
•Uses respirations for treatment
what type of technique is Facilitated positional release?
•Goal of this technique is to reduce muscle hypertonicity (superficial and deep) and restore lost motion to a restricted articulation
what is the goal of FPR?
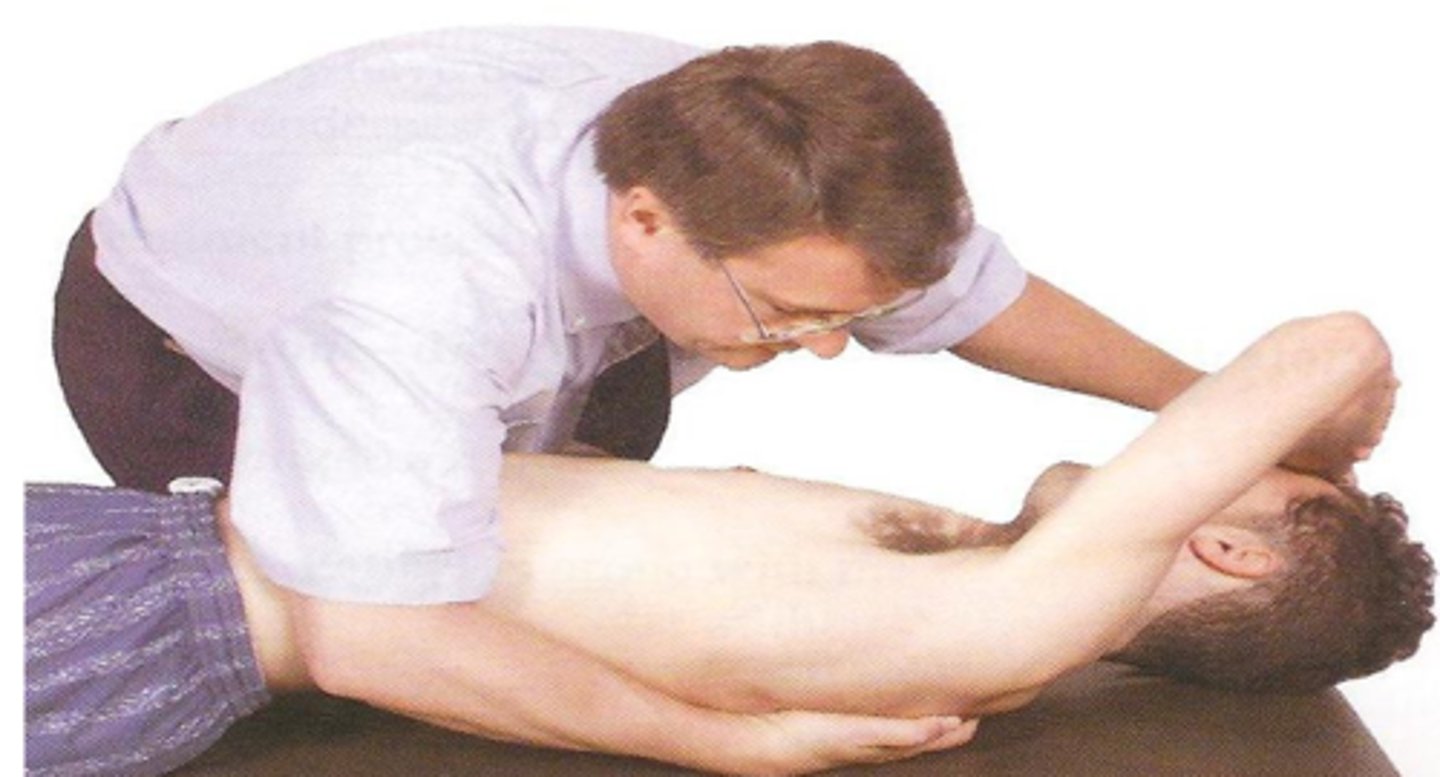
•Patient supine, dorsal aspect of ipsilateral forearm on forehead. Patient’s head turned 10-15 degrees away from dysfunctional rib in order to engage anterior and middle scalenes.
•Physician seated or standing facing pt with his/her hand over patient’s forearm or hand. Other hand on costotransverse junction of Rib 1-T1
•Physician requests that patient attempt to raise their head off the table as physician resists. Held for 3-5 seconds.
•During relaxation phase, engage new barrier through contact at costo-transverse junction
treatment of rib 1 (2ish) dysfunction with muscle energy
•Patient supine, dorsal aspect of ipsilateral forearm on their forehead.
•Physician standing on side to be treated, facing patient. One hand contacting anterior surface of patient’s elbow, one hand on posterior aspect of highest rib in dysfunctional group – pulling down to engage the barrier.
•Patient pulls towards chest engages the ipsilateral pectoralis muscle, pulling the anterior aspect of the ribs cephalad.
treatment of ribs 3-5 with muscle energy
•Patient supine, dorsal aspect of ipsilateral forearm on their forehead.
•Physician standing on side to be treated, facing pt. One hand contacting antero-inferior surface of patient’s elbow, one hand on posterior aspect of highest rib in dysfunctional group – pulling down to engage the barrier.
•Patient pulls towards the umbilicus engaging the ipsilateral serratus anterior muscle, pulling the anterolateral aspect of the ribs cephalad.
treatment of ribs 6-8 with muscle energy
•Physician standing on side to be treated, facing patient. One hand contacting inferior surface of patient’s elbow, one hand on posterior aspect of highest rib in dysfunctional group – pulling down to engage the barrier.
•Patient pulls down toward the hip engaging the ipsilateral latissimus dorsi muscle.
treatment of ribs 9-12 with muscle energy

Patient’s head is lifted into flexion, side bent toward the rib, and rotated away
movement of head to remove tension from scalene muscles during respiratory assist for rib 1
•Physician hand under patient at mid-scapular region contacting inferior angle of dysfunctional rib applying superior pressure
•Support patient’s head with forearm
•Other hand contact superior aspect of dysfunctional rib anteriorly
•Flex head and thorax to restrictive barrier
•Patient takes a deep breath and with exhalation the physician’s anterior hand moves the dysfunctional rib inferior with continued superior pressure on the posterior rib, moving it to a new restrictive barrier
technique of respiratory assist of ribs 2-6
•Patient side bent to the dysfunctional side until local tissue relaxation is felt
•One hand contacts the posterior inferior aspect of the dysfunctional rib
•Other hand thumb and index finger contacts superior aspect of shaft of dysfunctional rib at mid-axillary line
•Physician resists motion with inhalation and follows motion inferior with exhalation to new barrier
respiratory assist technique of ribs 7-10
•Arm on the dysfunction side is up toward patient’s head
•Patient’s lower extremities are moved toward the physician to place traction on the quadratus lumborum of dysfunctional side
•Physician contacts the dysfunctional 11th or 12th rib at the costovertebral joint
•Physician grasps the ASIS of the dysfunctional side and rotates the pelvis posteriorly
•Patient breathes in and out deeply while the physician maintains tension at the pelvis and stabilizes the costovertebral junction
•On exhalation the physician lifts the ASIS further into the new barrier
treatment of ribs 11-12 using respiratory assist
•One hand contacts posterior rib just medial to rib angle, with other hand contact anterior end of same rib at the costosternal joint
•Slight compression between front and back hands
•While maintaining compression at position of ease you will then apply slight “vector” of either traction or compression to disengage the rib or ribs
•While maintaining compression between front and back of rib, follow inhalation or exhalation to position of ease
•After 3-5 seconds allow rib to come back to neutral
technique of treating a typical rib with FPR
•Patient supine and physician on the dysfunctional side
•Place one hand palm up with fingers around contouring the angle of rib cage posteriorly
•Other hand placed down with fingers around rib cage anteriorly
•Hands pressure is adjusted toward the ease of movement of the ribs and underlying tissue until a balance of tension is achieved.
technique of treating exhalation dysfunction with BLT